
Autism Spectrum Disorders and Malocclusions: Systematic Review and Meta-Analyses

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focused Question and Eligibility Criteria
2.3. Search Strategy and Study Selection
2.4. Data Extraction Process and Data Items
2.5. Risk of Bias (RoB) Assessment
2.6. Summary Measures and Synthesis of Results
3. Results
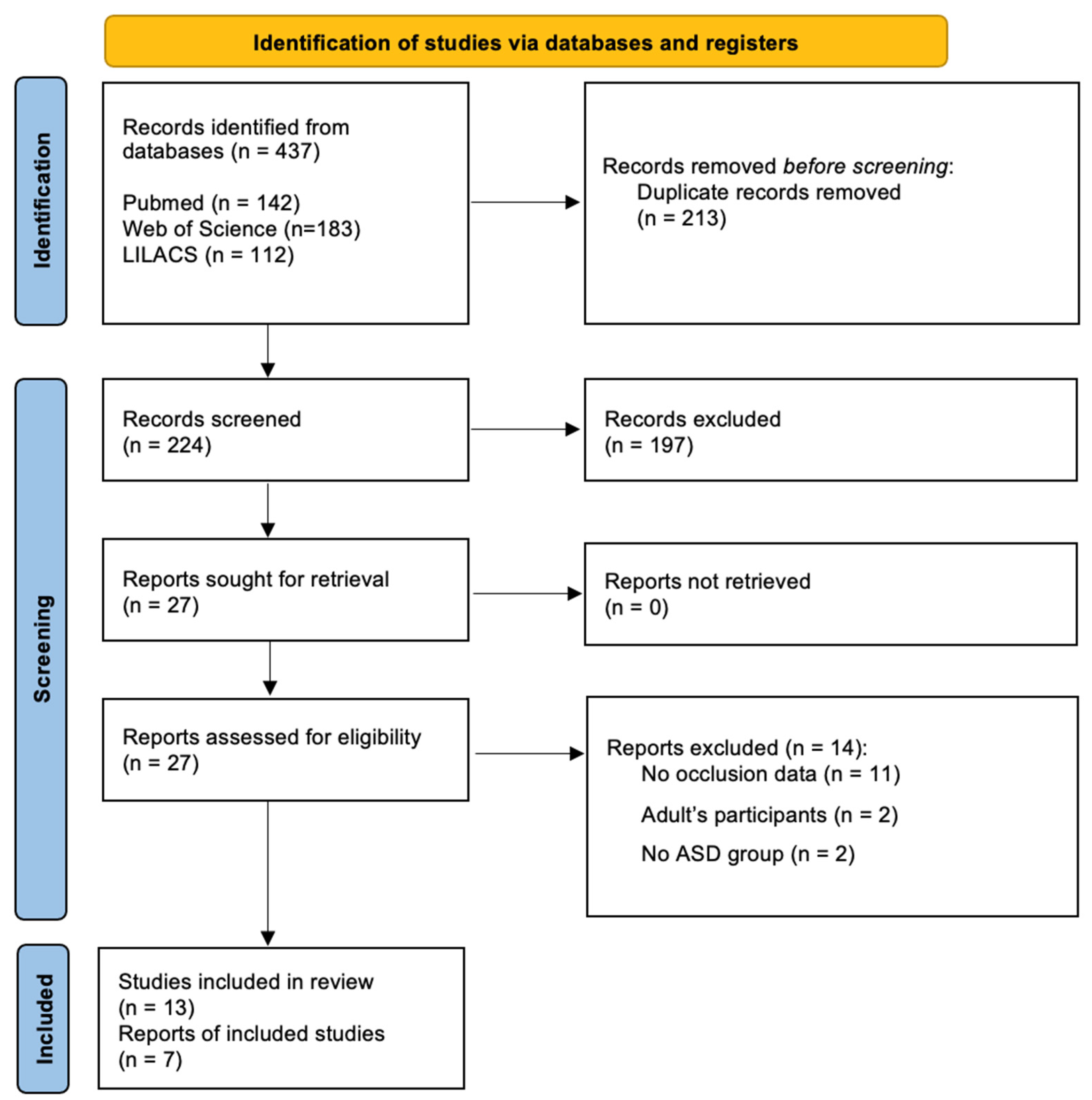
3.1. Study Selection
3.2. Studies Characteristics
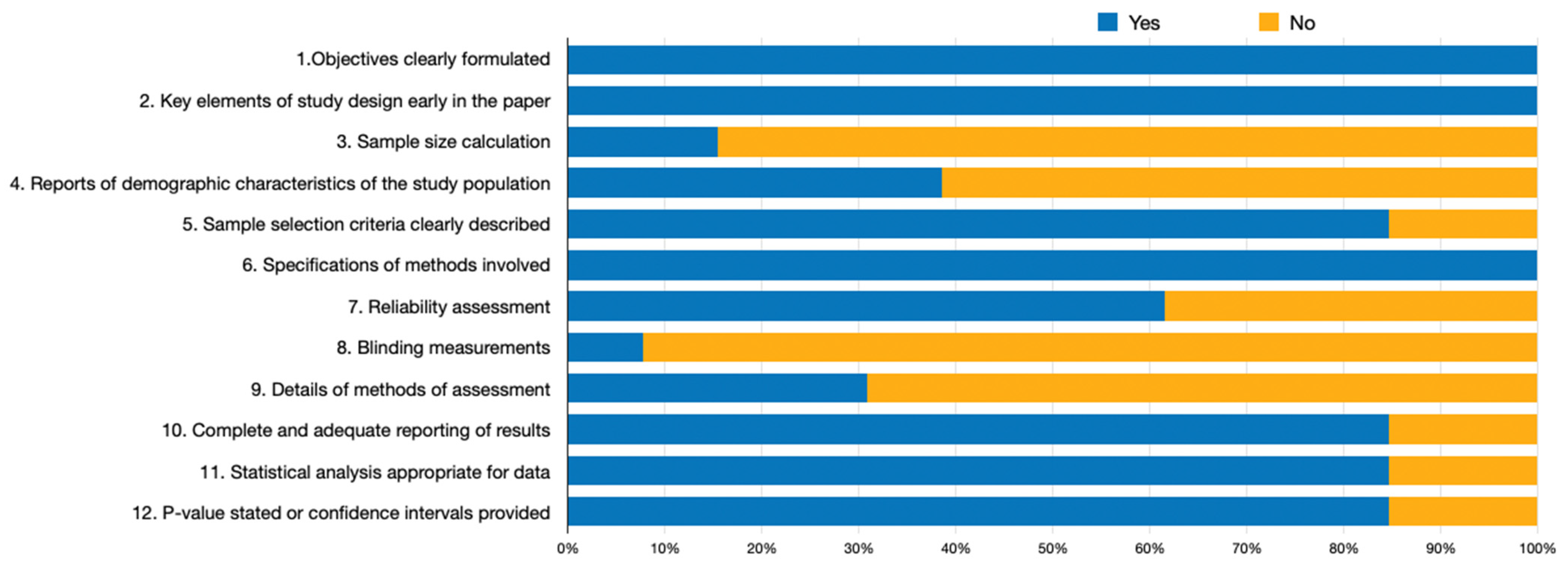
3.3. Methodological Quality of the Included Studies
3.4. Outcomes Measures
3.4.1. Malocclusion Class (Primary Outcome)
3.4.2. Secondary Outcomes
4. Discussion
4.1. Summary of Main Findings
4.2. Implications for Practice and Research
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Bartolome-Villar, B.; Mourelle-Martinez, M.; Dieguez-Perez, M.; de Nova-Garcia, M. Incidence of Oral Health in Paediatric Patients with Disabilities: Sensory Disorders and Autism Spectrum Disorder. Systematic Review II. J. Clin. Exp. Dent. 2016, 8, 344. [Google Scholar] [CrossRef] [PubMed]
- Önol, S.; Kırzıoğlu, Z. Evaluation of Oral Health Status and Influential Factors in Children with Autism. Niger. J. Clin. Pract. 2018, 21, 429–435. [Google Scholar] [PubMed]
- Leiva-García, B.; Planells, E.; Planells del Pozo, P.; Molina-López, J. Association Between Feeding Problems and Oral Health Status in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 49, 4997–5008. [Google Scholar] [CrossRef] [PubMed]
- Kuter, B.; Uzel, I. Evaluation of Oral Health Status and Oral Disorders of Children with Autism Spectrum Disorders by Gender. Arch. Pédiatrie 2021, 28, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Fontaine-Sylvestre, C.; Roy, A.; Rizkallah, J.; Dabbagh, B.; Ferraz dos Santos, B. Prevalence of Malocclusion in Canadian Children with Autism Spectrum Disorder. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 38–41. [Google Scholar] [CrossRef]
- Bagattoni, S.; Lardani, L.; D’Alessandro, G.; Piana, G. Oral Health Status of Italian Children with Autism Spectrum Disorder. Eur. J. Paediatr. Dent. 2021, 22, 243–247. [Google Scholar] [CrossRef]
- Farmani, S.; Ajami, S.; Babanouri, N. Prevalence of Malocclusion and Occlusal Traits in Children with Autism Spectrum Disorders. CCIDE 2020, 12, 343–349. [Google Scholar] [CrossRef]
- Koskela, A.; Neittaanmäki, A.; Rönnberg, K.; Palotie, A.; Ripatti, S.; Palotie, T. The Relation of Severe Malocclusion to Patients’ Mental and Behavioral Disorders, Growth, and Speech Problems. Eur. J. Orthod. 2021, 43, 159–164. [Google Scholar] [CrossRef]
- Büyükbayraktar, Z.Ç.; Doruk, C. Orthodontic Approach to Patients with Autism: A Review. Turk. J. Orthod. 2019, 32, 172–175. [Google Scholar] [CrossRef]
- Du, R.Y.; Yiu, C.K.; King, N.M.; Wong, V.C.; McGrath, C.P. Oral Health among Preschool Children with Autism Spectrum Disorders: A Case-Control Study. Autism 2015, 19, 746–751. [Google Scholar] [CrossRef]
- Kuter, B. Caries Experience, Oral Disorders, Oral Hygiene Practices and Sociodemographic Characteristics of Autistic Children. Eur. J. Paediatr. Dent. 2019, 20, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joanna Briggs Institute. The Systematic Review of Prevalence and Incidence Data; The Joanna Briggs Institute: Adelaide, Australia, 2014. [Google Scholar]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Use R! Springer International Publishing: Cham, Switzerland, 2015; ISBN 978-3-319-21415-3. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Soft. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; Wiley: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53662-8. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirtala-Orellana, L.; Silvestre, F.; Martinez-Sanchis, S.; Martinez-Mihi, V.; Bautista, D. Oral Manifestations in a Group of Adults with Autism Spectrum Disorder. Med. Oral 2012, 17, e415–e419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomqvist, M.; Bejerot, S.; Dahllöf, G. A Cross-Sectional Study on Oral Health and Dental Care in Intellectually Able Adults with Autism Spectrum Disorder. BMC Oral Health 2015, 15, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossù, M.; Trottini, M.; Corridore, D.; Di Giorgio, G.; Sfasciotti, G.L.; Palaia, G.; Ottolenghi, L.; Polimeni, A.; Di Carlo, S. Oral Health Status of Children with Autism in Central Italy. Appl. Sci. 2020, 10, 2247. [Google Scholar] [CrossRef] [Green Version]
- Morais Junior, R.C.; Rangel, M.d.L.; de Carvalho, L.G.A.; Figueiredo, S.C.; Ribeiro, I.L.A.; de Castro, R.D. Social, Educational and Dental Profiles of Brazilian Patients with Special Needs Attended at a Center for Dental Specialties. Pesqui. Bras. Odontopediatria Clín. Integr. 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Makkar, A.; Indushekar, K.R.; Saraf, B.G.; Sardana, D.; Sheoran, N. A Cross Sectional Study to Evaluate the Oral Health Status of Children with Intellectual Disabilities in the National Capital Region of India (Delhi-NCR). J. Intellect. Disabil. Res. 2019, 63, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Suhaib, F.; Saeed, A.; Gul, H.; Kaleem, M. Oral Assessment of Children with Autism Spectrum Disorder in Rawalpindi, Pakistan. Autism 2019, 23, 81–86. [Google Scholar] [CrossRef]
- Naidoo, M.; Singh, S. The Oral Health Status of Children with Autism Spectrum Disorder in KwaZulu-Nata, South Africa. BMC Oral Health 2018, 18, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, R.; Simões, P.W.; Pires, P.D.S.; Rosso, M.L.P. Prevalência de Alterações Bucais Em Pessoas Com Deficiência Na Clínica Da Universidade Do Extremo Sul Catarinense. Rev. De Odontol. Da Univ. Cid. De São Paulo 2017, 29, 118–128. [Google Scholar] [CrossRef] [Green Version]
- El Khatib, A.A.; El Tekeya, M.M.; El Tantawi, M.A.; Omar, T. Oral Health Status and Behaviours of Children with Autism Spectrum Disorder: A Case-Control Study. Int. J. Paediatr. Dent. 2014, 24, 314–323. [Google Scholar] [CrossRef]
- Jaber, M.A. Dental Caries Experience, Oral Health Status and Treatment Needs of Dental Patients with Autism. J. Appl. Oral Sci. 2011, 19, 212–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaber, M.A.; Sayyab, M.; Abu Fanas, S.H. Oral Health Status and Dental Needs of Autistic Children and Young Adults: Oral Health Status of Autistic Patients. J. Investig. Clin. Dent. 2011, 2, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Fahlvik-Planefeldt, C.; Herrström, P. Dental Care of Autistic Children within the Non-Specialized Public Dental Service. Swed. Dent. J. 2001, 25, 113–118. [Google Scholar]
- Vellappally, S.; Gardens, S.J.; Al Kheraif, A.-A.A.; Krishna, M.; Babu, S.; Hashem, M.; Jacob, V.; Anil, S. The Prevalence of Malocclusion and Its Association with Dental Caries among 12-18-Year-Old Disabled Adolescents. BMC Oral Health 2014, 14, 123. [Google Scholar] [CrossRef] [Green Version]
- DeMattei, R.; Cuvo, A.; Maurizio, S. Oral Assessment of Children with an Autism Spectrum Disorder. J. Dent. Hyg. 2007, 81, 65. [Google Scholar]
- Alkhabuli, J.O.S.; Essa, E.Z.; Al-Zuhair, A.M.; Jaber, A.A. Oral Health Status and Treatment Needs for Children with Special Needs: A Cross-Sectional Study. Pesqui. Bras. Odontopediatria Clín. Integr. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Rekha, C.V.; Arangannal, P.; Shahed, H. Oral Health Status of Children with Autistic Disorder in Chennai. Eur. Arch. Paediatr. Dent. 2012, 13, 126–131. [Google Scholar] [CrossRef]
- Alkhadra, T. Characteristic of Malocclusion among Saudi Special Need Group Children. J. Contemp. Dent. Pract. 2017, 18, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Luppanapornlarp, S.; Leelataweewud, P.; Putongkam, P.; Ketanont, S. Periodontal Status and Orthodontic Treatment Need of Autistic Children. World J. Orthod. 2010, 11, 256–261. [Google Scholar] [PubMed]
- Corridore, D.; Zumbo, G.; Corvino, I. Prevalence of Oral Disease and Treatment Types Proposed To children Affected by Autistic Spectrum Disorder in Pediatric Dentistry: A Systematic Review. Clin. Ter. 2020, 171, 275–282. [Google Scholar] [CrossRef]
- AlOtaibi, A.; Ben Shaber, S.; AlBatli, A.; AlGhamdi, T.; Murshid, E. A Systematic Review of Population-Based Gingival Health Studies among Children and Adolescents with Autism Spectrum Disorder. Saudi Dent. J. 2021, 33, 370–374. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year (Country) | Funding | Search Period | ASD/Non-ASD Participants (N Total [Male/Female]) | Age Range (Years) (ASD/Non-ASD) | Occlusion ASD Participants (n [%]) | Occlusion Non-ASD Participants (n [%]) | Main Results |
|---|---|---|---|---|---|---|---|
| Bagattoni et al. 2021 (Italy) [7] | NR | January 2015 to March 2018 | 64 (42/22)/ 64 (37/27) | 9.0 ± 2.9/8.4 ± 3.0 | Class I—34 (70.0%); Class II—13 (26.0%); Class III—2 (4.0%); Posterior crossbite—9 (14.0%); Overbite Anterior open bite—12 (19.0%); Deep bite—9 (14.0%). | Class I—38 (76.0%); Class II—9 (18.0%); Class III—3 (6.0%); Posterior crossbite—10 (17.0%); Overbite Anterior open bite—3 (5.0%); Deep bite—10 (17.0%). | The difference between the two groups was not statistically significant in the overall analysis (p > 0.05), except on the anterior open bite (p = 0.013) |
| Farmani et al. 2020 (Iran) [8] | Vice Chancellery of Shiraz University of Medical Sciences, Shiraz, Iran (grant number: 16499). | June 2018 to October 2018 | 47 (36/11)/ 49 (28/27) | 10.7 ± 2.1/9.5 ± 1.3 | Malocclusion—35 (76.1%); Class I—20 (55.6%); Class II—16 (44.4%); Class III—7 (25.9%); Overjet Normal—20 (55.6); Increased—16 (44.4%); Decreased—7 (25.9%); Overbite Normal—24 (66.7%); Increased—12 (33.3%); Decreased—7 (22.6%); Crossbite Anterior and posterior—3 (6.4%) | Malocclusion—38 (79.2%); Class I—30 (88.2%); Class II—4 (11.8%); Class III—13 (30.2%); Overjet Normal—30 (88.2%); Increased—4 (11.8%); Decreased—13 (30.2%); Overbite Normal—24 (75.0%); Increased—8 (25.0%); Decreased—13 (35.1%); Crossbite Anterior and posterior—7 (14.3%) | Increased overjet and Class II molar relationship were the most prevalent malocclusions in the ASD group compared with control group (p = 0.03). ASD children were 6 times more likely to have increased overjet than those in the control group (OR: 6.0; 95% CI: 1.7–20.6). There was no statistically significant difference between the two groups in terms of crossbite and overbite. |
| Alkhabuli et al. 2019 (United Arab Emirates) [33] | None | NR | 9 (NR/NR)/Not Present | NR/Not Present | Class II—38.0%; Class III—25.0%; Class II/III—38.0% | Not Present | Class II and Class III malocclusions among ASD patients are frequent |
| Kuter 2019 (Turkey) [12] | NR | NR | 285 (NR/NR)/ 122 (NR/NR) | range 12–16 years | Open bite—16 (5.7%) | Open bite—6 (4.9%) | No significant difference in the proportion of open bite was identified (p > 0.05) |
| Leiva-García et al. 2019 (Spain) [4] | Mutua Madrileña Research Foundation. | January 2016 to December 2017 | 51 (37/13)/ 93 (50/43) | 12.8 ± 3.7/12.8 ± 3.7 | No malocclusion—12 (24.0%); Class I crowding—20 (40.0%); Class II—6 (10.0%); Class III—3 (6.0%); Open bite—9 (18.0%); Crossbite—1 (2.0%) | No malocclusion—46 (49.5%); Class I crowding—8 (8.6%); Class II—12 (12.9%); Class III—8 (8.6%); Open bite—4 (4.3%); Crossbite −8 (8.6%) | Malocclusion and open bite were more prevalent in the ASD group than in the control group (p = 0.000). |
| Orellana et al. 2019 (Chile) [19] | Comisión Nacional de Investigación Científica y Tecnológica, Chile. Proyecto FONIS SA15I20110. | 2016–2017 | 123 (102/21)/ Not Present | 9.4 ± 4.3/Not Present | Deep/ogival palate—64 (52.0%); Anterior open bite—7 (5.7%); Crossbite Anterior—10 (8.1%); Posterior—4 (3.3%). | Not Present | A high percentage of deep/ogival palate was found in this population |
| Önol & Kurzioğlu 2018 (Turkey) [3] | None | March to July 2016. | 33 (NR/NR)/ 33 (NR/NR) | 10.5 ± 2.9/10.2 ± 2.5 | Class I—23 (69.8%); Class II division I—6 (20.6%); Class II division II—2 (4.8%); Class III—2 (4.8%); Cross bite—0 (0.0%); Open bite—1(1.6%); Deep bite—0 (0.0%); High arch palate—2 (6.3%) | Class I—29 (86.5%); Class II division I—3 (8.1%); Class II division II—1 (3.6%); Class III—1 (1.8%); Cross bite—1 (3.0%); Open bite—1 (1.8%); Deep bite—2(5.4%); High arch palate—1(0.9%) | Crossbite and deep bite were more prevalent in the non-ASD group than in the ASD group (p = 0.013). No significant differences were found in Angle’s molar relationship. |
| Alkhadra 2017 (Saudi Arabia) [35] | None | NR | 100 (65/35)/ Not Present | NR/Not Present | Crossbite—10 (10.0%) Overjet Normal—84 (84.0%); Increased—16 (16.0%); Overbite Normal—55 (55.0%); Increased—4 (4.0%); Permanent dentition Right/Left Class I—40/41 (40.0%/41.0%); Right/Left Class II—16/13 (16.0%/13.0%); Right/Left Class III—3/5 (3.0%/5.0%); | Not Present | ASD children exhibited more of class I malocclusion. |
| DeMattei et al. 2017 (United Arab Emirates) [32] | The Autism Project. | NR | 39 (NR/NR)/ Not Present | NR/Not Present | Class I—18 (46.2%); Class II—14 (35.9%); Class III—7 (17.9%); Cross bite—5 (12.8%); Crowding—1 (2.6%) | Not Present | No significant difference in the oral health status of children with an ASD when comparing younger children to older children or when comparing children with an ASD who resided with their parents to those who lived at the residential school |
| Fontaine-Sylvestre et al. 2017 (Canada) [6] | NR | January 2013 to August 2015 | 99 (78/21)/ 101 (83/18) | 11.0 ± 3.7/11.0 ± 3.8 | Class I—37 (42.5%); Class II—37 (42.5%); Class III—13 (14.9%); Midline deviation (>4 mm)—35 (38.9%); Midline deviation (<4 mm)—55 (61.1%). Crossbite Anterior—8 (8.1%); Posterior—13 (13.1%); Overbite Anterior Open bite—8 (8.1%); Posterior Open bite—3 (3.0%); Normal—67 (77.0%); Increased (>65%)—12 (13.8%); Decreased (≤0%)—8 (9.2%); Overjet Normal—49 (54.4%); Increased (>4 mm)—35 (38.9%); Decreased (<1 mm)—6 (6.7%); Crowding Minimal Maxillary—29 (29.3%); Moderate Maxillary—4 (4.0%); Severe Maxillary—5 (5.1%); Minimal Mandibular—36 (36.4%); Moderate Mandibular—8 (8.1%); Severe Mandibular—4 (4.0%) | Class I—51 (56.0%); Class II—30 (33.0%); Class III—10 (11.0%); Midline deviation (<4 mm)—69 (68.3%); Midline deviation (>4 mm)—32 (31.7%). Crossbite Anterior—6 (5.9%); Posterior—5 (4.9%); Overbite Anterior open bite—6 (3.9%); Normal– 79 (79.0%); Increased (>65%)—15 (15.0%); Decreased (≤0%)—6 (6.0%); Overjet Normal—85 (85.1%); Increased (>4 mm)—11 (10.9%); Decreased (<1 mm)—4 (4.0%); Crowding Minimal Maxillary—20 (19.8%); Moderate Maxillary—17 (16.8%); Severe Maxillary—1 (1.0%); Minimal Mandibular—23 (22.8%); Moderate Mandibular—25 (14.9%); Severe Mandibular—3 (3.0%) | Midline deviation (33.5%) was the most common trait in this population. Children with ASD had a significantly higher prevalence of posterior crossbite (p = 0.03), increased overjet (p < 0.001), and severe maxillary crowding (p = 0.006) |
| Du et al. 2015 (Hong Kong) [11] | General Research Fund (17116014) of the Research Grant Council of Hong Kong. | NR | 257 (217/40)/ 258 (218/40) | 4.9 ± 0.8/NR | Overbite Deep bite—95 (37.0%); Anterior open bite—6 (2.3%); Overjet Increased—48 (18.7%); Crossbite Anterior—36 (14.0%); Posterior—0 (0.0%) | Overbite Deep bite—80 (31.1%); Anterior open bite—10 (3.9%); Overjet Increased Overjet—38 (14.8%); Crossbite Anterior—28 (10.90%); Posterior—1 (0.4%) | No statistically significant difference was found between the two groups (p > 0.05) |
| Rekha et al. 2012 (India) [34] | NR | NR | 483 (363/120)/ Not Present | NR/Not Present | Primary dentition Crowding—0 (0.0%); Proinclination—3 (0.6%); Anterior open bite—0 (0.0%); Rotation—0 (0.0%); Mixed dentition Crowding—21 (4.34%); Proinclination—15 (3.1%); Anterior open bite—3 (0.6%); Rotation—3 (0.6%); Permanent dentition Crowding—51 (10.5%); Proinclination—42 (8.6%); Anterior open bite—0 (0.0%); Rotation—6 (1.2%) | Not Present | Children with permanent dentition had more malocclusion (71.15%) |
| Luppanapornlarp et al. 2010 (Tailand) [36] | NR | NR | 32 (25/7)/ 48 (19/29) | 9.7 ± 1.2/9.9 ± 1.1 | DAI score ≤ 25—12 (37.5%); DAI score 26–30—8 (25.0%); DAI score 31–35—7 (22.0%); DAI ≥ 36—5 (15.5%) | DAI score ≤ 25—14 (29.0%); DAI score 26–30—14 (29.0%); DAI score 31–35—13 (27.0%); DAI ≥ 36—7 (15.0%) | In ASD children, malocclusion symptoms such as missing teeth, spacing, diastemas, reverse overjet, open bite, and Class II molar relationship tendency were found at a higher percentage than in the control group |
| Variable | N Studies | N of Participants (ASD/Controls) | OR | 95% CI | p-Value | I2 (%) |
|---|---|---|---|---|---|---|
| Malocclusion | 3 | 197/243 | 0.90 | 0.24; 3.38 | 0.8703 | 89.5 |
| Class I | 5 | 275/324 | 1.47 | 0.47; 4.59 | 0.5101 | 87.4 |
| Class II | 5 | 275/324 | 1.78 | 0.97; 3.24 | 0.0619 | 46.6 |
| Class III | 5 | 275/324 | 0.87 | 0.50; 1.52 | 0.6346 | 0.0 |
| Crossbite | ||||||
| Anterior Crossbite | 3 | 420/423 | 1.72 | 0.90; 3.28 | 0.1028 | 34.4 |
| Posterior Crossbite | 3 | 405/409 | 1.38 | 0.50; 3.81 | 0.5374 | 39.2 |
| Anterior + Posterior Crossbite | 3 | 131/175 | 0.33 | 0.11; 1.00 | 0.0508 | 0.0 |
| Overbite | ||||||
| Deep bite or increased overbite | 5 | 496; 501 | 1.19 | 0.88; 1.60 | 0.2649 | 0.0 |
| Open bite or decreased overbite | 6 | 768; 652 | 1.19 | 0.58; 2.43 | 0.6413 | 52.0 |
| Overjet | ||||||
| Increased overjet | 3 | 399; 406 | 3.07 | 1.10; 8.57 | 0.0043 | 81.7 |
| Normal overjet | 2 | 142; 148 | 0.28 | 0.10; 0.79 | 0.0164 | 72.9 |
| Decreased overjet | 2 | 142; 148 | 0.83 | 0.28; 2.48 | 0.7388 | 43.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barros, A.; Mascarenhas, P.; Botelho, J.; Machado, V.; Balixa, G.; Bandeira Lopes, L. Autism Spectrum Disorders and Malocclusions: Systematic Review and Meta-Analyses. J. Clin. Med. 2022, 11, 2727. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102727
Barros A, Mascarenhas P, Botelho J, Machado V, Balixa G, Bandeira Lopes L. Autism Spectrum Disorders and Malocclusions: Systematic Review and Meta-Analyses. Journal of Clinical Medicine. 2022; 11(10):2727. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102727
Chicago/Turabian StyleBarros, Aline, Paulo Mascarenhas, João Botelho, Vanessa Machado, Gabriela Balixa, and Luísa Bandeira Lopes. 2022. "Autism Spectrum Disorders and Malocclusions: Systematic Review and Meta-Analyses" Journal of Clinical Medicine 11, no. 10: 2727. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102727