
The Impact of Postoperative Radiotherapy on Dietary Function of Head and Neck Cancer Patients after Pharyngoesophageal Reconstruction with Free Jejunal Flap

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. General Characterictics
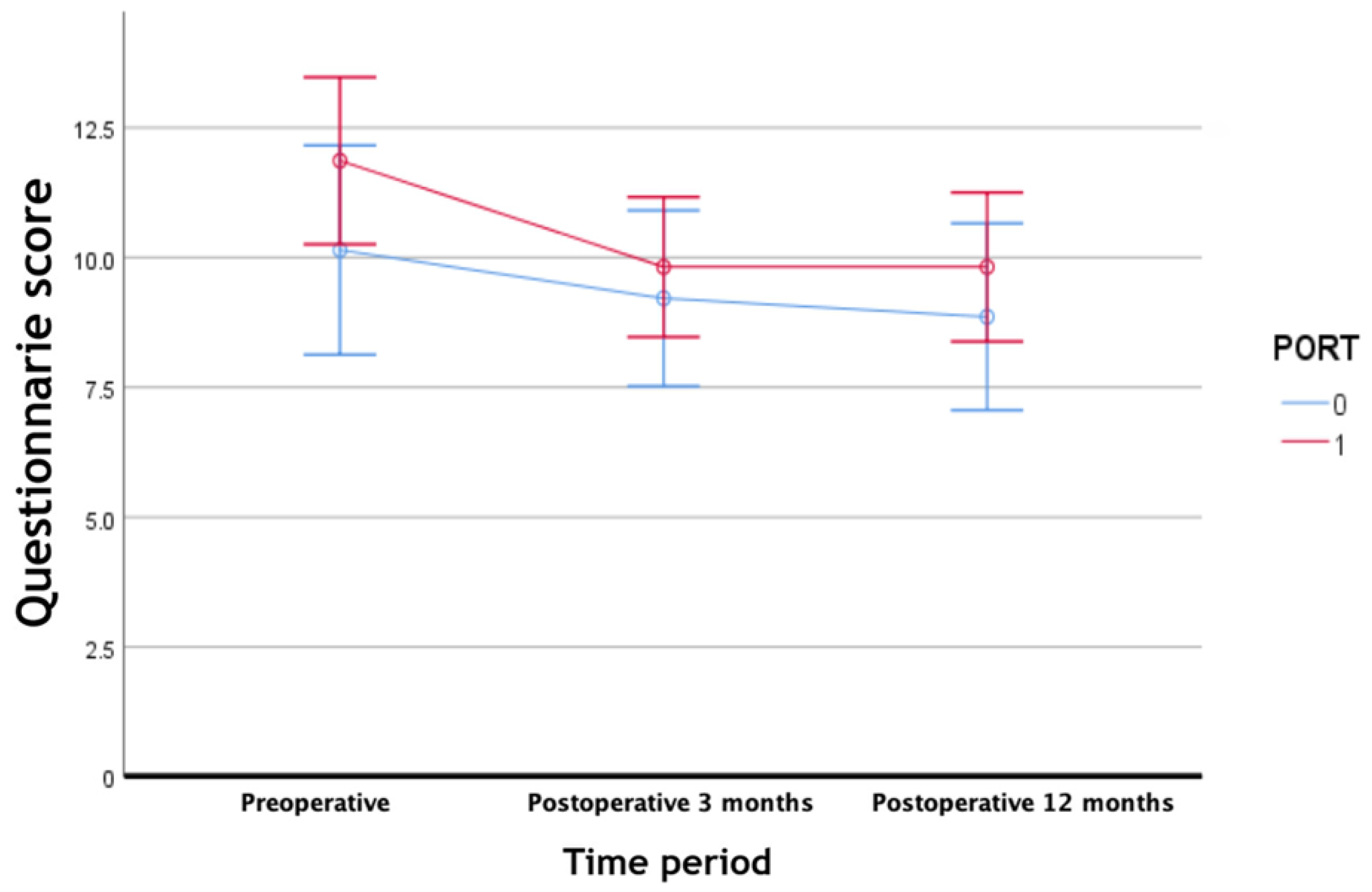
3.2. Questionnaire
3.3. Risk Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, Y.-W.; Ng, R.W.M.; Liu, L.H.L.; Chung, H.P.; Wei, W.I. Reconstruction of circumferential pharyngeal defects after tumour resection: Reference or preference. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Neligan, P.C.; Rodriguez, E.D.; Beek, A.L.V.; Losee, J.E. Craniofacial, head and neck surgery, pediatric plastic surgery. In Plastic Surgery, 3rd ed.; Elsevier/Saunders: London, UK, 2013; pp. 107–108. [Google Scholar]
- Yu, P.; Lewin, J.S.; Reece, G.P.; Robb, G.L. Comparison of clinical and functional outcomes and hospital costs following pharyngoesophageal reconstruction with the anterolateral thigh free flap versus the jejunal flap. Plast. Reconstr. Surg. 2006, 117, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.J.; Goepfert, H.; Ang, K.K.; Byers, R.M.; Maor, M.H.; Guillamondegui, O.; Morrison, W.H.; Weber, R.S.; Garden, A.S.; Frankenthaler, R.A. Evaluation of the dose for postoperative radiation therapy of head and neck cancer: First report of a prospective randomized trial. Int. J. Radiat. Oncol. Biol. Phys. 1993, 26, 3–11. [Google Scholar] [CrossRef]
- Baglan, K.L.; Frazier, R.C.; Yan, D.; Huang, R.R.; Martinez, A.A.; Robertson, J.M. The dose-volume relationship of acute small bowel toxicity from concurrent 5-FU-based chemotherapy and radiation therapy for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 176–183. [Google Scholar] [CrossRef]
- Bjordal, K.; de Graeff, A.; Fayers, P.M.; Hammerlid, E.; van Pottelsberghe, C.; Curran, D.; Ahlner-Elmqvist, M.; Maher, E.J.; Meyza, J.W.; Bredart, A.; et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur. J. Cancer 2000, 36, 1796–1807. [Google Scholar] [CrossRef]
- El-Sabawi, B.; Sosin, M.; Carey, J.N.; Nahabedian, M.Y.; Patel, K.M. Breast reconstruction and adjuvant therapy: A systematic review of surgical outcomes. J. Surg. Oncol. 2015, 112, 458–464. [Google Scholar] [CrossRef]
- Peled, A.W.; Sears, M.; Wang, F.; Foster, R.D.; Alvarado, M.; Wong, J.; Ewing, C.A.; Sbitany, H.; Esserman, L.J.; Fowble, B. Complications After Total Skin-Sparing Mastectomy and Expander-Implant Reconstruction: Effects of Radiation Therapy on the Stages of Reconstruction. Ann. Plast. Surg. 2018, 80, 10–13. [Google Scholar] [CrossRef]
- Wang, F.; Peled, A.W.; Chin, R.; Fowble, B.; Alvarado, M.; Ewing, C.; Esserman, L.; Foster, R.; Sbitany, H. The Impact of Radiation Therapy, Lymph Node Dissection, and Hormonal Therapy on Outcomes of Tissue Expander-Implant Exchange in Prosthetic Breast Reconstruction. Plast. Reconstr. Surg. 2016, 137, 1–9. [Google Scholar] [CrossRef]
- Gazyakan, E.; Wu, C.W.; Huang, J.J.; Engel, H.; Valerio, I.L.; Cheng, M.H. Minimizing osteoradionecrosis after mandibular reconstruction and radiation in advanced head and neck cancer patients. J. Surg. Oncol. 2016, 114, 399–404. [Google Scholar] [CrossRef]
- Chang, T.-Y.; Hsiao, J.-R.; Lee, W.-T.; Ou, C.-Y.; Yen, Y.-T.; Tseng, Y.-L.; Pan, S.-C.; Shieh, S.-J.; Lee, Y.-C. Esophageal reconstruction after oncological total laryngopharyngoesophagectomy: Algorithmic approach. Microsurgery 2018, 39, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Disa, J.J.; Pusic, A.L.; Hidalgo, D.A.; Cordeiro, P.G. Microvascular reconstruction of the hypopharynx: Defect classification, treatment algorithm, and functional outcome based on 165 consecutive cases. Plast. Reconstr. Surg. 2003, 111, 652–660; discussion 653–661. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.S.; Kwon, J.G.; Jeong, W.S.; Nam, S.Y.; Choi, S.H.; Choi, J.W. A flag-shaped anterolateral thigh free flap for complete circumferential hypopharyngeal reconstruction with dead space obliteration and monitoring flap inset. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Robb, G.L. Pharyngoesophageal Reconstruction with the Anterolateral Thigh Flap: A Clinical and Functional Outcomes Study. Plast. Reconstr. Surg. 2005, 116, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Anthony, J.P.; Singer, M.I.; Mathes, S.J. Pharyngoesophageal reconstruction using the tubed free radial forearm flap. Clin. Plast. Surg. 1994, 21, 137–147. [Google Scholar] [CrossRef]
- Kountouras, J.; Zavos, C. Recent advances in the management of radiation colitis. World J. Gastroenterol. 2008, 14, 7289–7301. [Google Scholar] [CrossRef]
- Chan, J.Y.; Chow, V.L.; Chan, R.C.; Lau, G.I. Oncological outcome after free jejunal flap reconstruction for carcinoma of the hypopharynx. Eur. Arch. Otorhinolaryngol. 2012, 269, 1827–1832. [Google Scholar] [CrossRef] [Green Version]
- Perez-Smith, D.; Wagels, M.; Theile, D.R. Jejunal free flap reconstruction of the pharyngolaryngectomy defect: 368 Consecutive cases. J. Plast. Reconstr. Aesthetic Surg. 2013, 66, 9–15. [Google Scholar] [CrossRef]
- Agarwal, J.; Dutta, D.; Palwe, V.; Gupta, T.; Laskar, S.G.; Budrukkar, A.; Murthy, V.; Chaturvedi, P.; Pai, P.; Chaukar, D.; et al. Prospective subjective evaluation of swallowing function and dietary pattern in head and neck cancers treated with concomitant chemo-radiation. J. Cancer Res. Ther. 2010, 6, 15–21. [Google Scholar] [CrossRef]
- Pauloski, B.R.; Rademaker, A.W.; Logemann, J.A.; Lazarus, C.L.; Newman, L.; Hamner, A.; MacCracken, E.; Gaziano, J.; Stachowiak, L. Swallow function and perception of dysphagia in patients with head and neck cancer. Head Neck 2002, 24, 555–565. [Google Scholar] [CrossRef]
- List, M.A.; D’Antonio, L.L.; Cella, D.F.; Siston, A.; Mumby, P.; Haraf, D.; Vokes, E. The Performance Status Scale for Head and Neck Cancer Patients and the Functional Assessment of Cancer Therapy-Head and Neck Scale. A study of utility and validity. Cancer 1996, 77, 2294–2301. [Google Scholar] [CrossRef]
- List, M.A.; Ritter-Sterr, C.; Lansky, S.B. A performance status scale for head and neck cancer patients. Cancer 1990, 66, 564–569. [Google Scholar] [CrossRef]
- Russi, E.G.; Corvo, R.; Merlotti, A.; Alterio, D.; Franco, P.; Pergolizzi, S.; De Sanctis, V.; Redda, R.M.G.; Ricardi, U.; Paiar, F.; et al. Swallowing dysfunction in head and neck cancer patients treated by radiotherapy: Review and recommendations of the supportive task group of the Italian Association of Radiation Oncology. Cancer Treat. Rev. 2012, 38, 1033–1049. [Google Scholar] [CrossRef] [PubMed]
- Starmer, H.M.; Quon, H.; Kumar, R.; Alcorn, S.; Murano, E.; Jones, B.; Humbert, I. The Effect of Radiation Dose on Swallowing: Evaluation of Aspiration and Kinematics. Dysphagia 2015, 30, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Teguh, D.N.; Levendag, P.C.; Sewnaik, A.; Hakkesteegt, M.M.; Noever, I.; Voet, P.; van der Est, H.; Sipkema, D.; van Rooij, P.; de Jong, R.J.B.; et al. Results of fiberoptic endoscopic evaluation of swallowing vs. radiation dose in the swallowing muscles after radiotherapy of cancer in the oropharynx. Radiother. Oncol. 2008, 89, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, L.; Heemsbergen, W.D.; de Jong, R.; van Rossum, M.A.; Smeele, L.E.; Rasch, C.R.; Hilgers, F.J. Dysphagia and trismus after concomitant chemo-Intensity-Modulated Radiation Therapy (chemo-IMRT) in advanced head and neck cancer; dose-effect relationships for swallowing and mastication structures. Radiother. Oncol. 2013, 106, 364–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Daele, D.J.; Langmore, S.E.; Krisciunas, G.P.; Lazarus, C.L.; Pauloski, B.R.; McCulloch, T.M.; Gramigna, G.D.; Messing, B.P.; Wagner, C.W.; Mott, S.L. The impact of time after radiation treatment on dysphagia in patients with head and neck cancer enrolled in a swallowing therapy program. Head Neck 2019, 41, 606–614. [Google Scholar] [CrossRef]
- Hu, H.T.; Shin, J.H.; Kim, J.H.; Park, J.H.; Sung, K.B.; Song, H.Y. Fluoroscopically guided balloon dilation for pharyngoesophageal stricture after radiation therapy in patients with head and neck cancer. AJR Am. J. Roentgenol. 2010, 194, 1131–1136. [Google Scholar] [CrossRef]


{kind=link}
| During the Past Week | Not at All | A Little | Quite a Bit | Very Much |
|---|---|---|---|---|
| Have you had a painful throat? | 1 | 2 | 3 | 4 |
| Have you had problems swallowing liquids? | 1 | 2 | 3 | 4 |
| Have you had problems swallowing pureed food? | 1 | 2 | 3 | 4 |
| Have you had problems swallowing solid food? | 1 | 2 | 3 | 4 |
| Have you had trouble eating? | 1 | 2 | 3 | 4 |
| Baseline Characteristics | Value | PORT+ | PORT− | p-Value |
|---|---|---|---|---|
| Number | 36 | 22 (61.1) | 14 (38.9) | |
| Age at op (yr) | 55.22 ± 9.97 | 54.91 ± 10.94 | 55.71 ± 8.60 | 0.817 |
| Sex | 0.511 | |||
| Male | 34 (94.4) | 20 (90.9) | 14 (100) | |
| Female | 2 (5.5) | 2 (9.1) | 0 (0) | |
| Follow-up period (mo) | 49.47 ± 28.65 | |||
| Cancer type | 0.754 | |||
| Hypopharyngeal cancer | 28 (77.8) | 17 (77.3) | 11 (78.6) | |
| Upper esophageal cancer | 4 (11.1) | 2 (9.1) | 2 (14.3) | |
| Laryngeal cancer | 4 (11.1) | 3 (13.6) | 1 (7.1) | |
| Primary or Recurred | 0.067 | |||
| Primary | 25 (69.4) | 18 (81.8) | 7 (50.0) | |
| Recurred | 11 (30.6) | 4 (18.2) | 7 (50.0) | |
| Neoadjuvant CTx | 11 (30.6) | 8 (36.4) | 3 (21.4) | 0.467 |
| Adjuvant CTx | 18 (50.0) | 16 (72.7) | 2 (14.3) | 0.001 |
| Previous RTx | 11 (30.6) | 5 (22.7) | 6 (42.9) | 0.273 |
| T stage | 0.105 | |||
| T1 | 1 (2.8) | 0 (0) | 1 (7.1) | |
| T2 | 5 (13.9) | 1 (4.5) | 4 (28.6) | |
| T3 | 7 (11.1) | 6 (27.3) | 1 (7.1) | |
| T4 | 23 (8.3) | 15 (68.2) | 8 (57.1) | |
| N stage | 0.216 | |||
| N0 | 18 (50.0) | 8 (36.4) | 10 (71.4) | |
| N1 | 11 (30.6) | 9 (40.9) | 2 (14.3) | |
| N2 | 4 (11.1) | 3 (13.6) | 1 (7.1) | |
| N3 | 3 (8.3) | 2 (9.1) | 1 (7.1) |
| Operation Related | Value | PORT+ | PORT− | p-Value |
|---|---|---|---|---|
| Neck dissection | 0.04 | |||
| MRND | 18 (50) | 14 (63.6) | 4 (28.6) | |
| Selective neck dissection | 10 (27.8) | 6 (27.3) | 4 (28.6) | |
| Extended neck dissection | 3 (8.3) | 2 (9.1) | 1 (7.1) | |
| Other | 2 (5.5) | 0 (0) | 2 (14.3) | |
| None | 3 (8.3) | 0 (0) | 3 (21.4) | |
| Concomitant Thyroidectomy | 15 (41.7) | 8 (36.4) | 7 (50.0) | 0.499 |
| Length of jejunal FF | 15.58 ± 3.11 | 15.45 ± 2.79 | 15.79 ± 3.66 | 0.761 |
| Recipient artery | 1.000 | |||
| Sup. Thyroid artery | 32 (88.9) | 19 (86.4) | 13 (92.9) | |
| Other | 4 (11.1) | 3 (13.6) | 1 (7.1) | |
| Recipient vein | 1.000 | |||
| Ext. jugular vein | 25 (69.4) | 15 (68.2) | 10 (71.4) | |
| Branch of internal jugular vein | 8 (22.2) | 5 (22.7) | 3 (21.4) | |
| Vena comitantes of sup. thyroid artery | 3 (8.3) | 2 (9.1) | 1 (7.1) |
| Variables | Value | PORT+ | PORT− | p-Value |
|---|---|---|---|---|
| Esophagography (days) | 18.81 ± 2.90 | 19.05 ± 3.06 | 18.43 ± 2.68 | 0.761 |
| Oral intake start (days) | 20.56 ± 4.63 | 21.05 ± 5.47 | 19.79 ± 2.89 | 1.000 |
| Early Complication | 1.000 | |||
| Leakage | 3 (7.5) | 2 (9.1) | 1 (7.1) | |
| Hematoma | 1 (2.5) | 0 (0) | 1 (7.1) | |
| Flap failure | 1 (2.5) | 1 (4.5) | 0 (0) | |
| Late complication | 1.000 | |||
| PEG insertion due to swallowing difficulty | 3 (7.5) | 2 (9.1) | 1 (7.1) | |
| Focal stenosis | 1 (2.5) | 0 (0) | 1 (7.1) | |
| Donor site complication | 1.000 | |||
| Wound dehiscence | 2 (5) | 1 (4.5) | 1 (7.1) | |
| Intussusception | 1 (2.5) | 0 (0) | 1 (7.1) |
| Variables | PORT− | PORT+ | Overall |
|---|---|---|---|
| Questionnaire score | |||
| Preop | 10.14 ± 3.21 | 11.86 ± 3.99 | 11.19 ± 3.76 |
| Postop 3 months | 9.21 ± 2.94 | 9.82 ± 3.22 | 9.58 ± 3.01 |
| Postop 12 months | 8.86 ± 3.35 | 9.82 ± 3.29 | 9.44 ± 3.30 |
| p-value | 0.310 † <0.0001 † | ||
| Differences within groups with time (p-value) | |||
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| Age | 0.021 | 0.715 | −0.015 | 0.728 |
| Sex | 1.647 | 0.170 | 2.7764 | 0.170 |
| Cancer type | −0.155 | 0.959 | 0.074 | |
| Hypopharyngeal cancer | Ref | Ref | ||
| Upper esophageal cancer | 0 | 1 | −1.594 | 0.259 |
| Laryngeal cancer | −0.5 | 0.773 | −2.8434 | 0.081 |
| Recurred cancer | −1.033 | 0.395 | ||
| Length of jejunal FF | 0.223 | 0.218 | ||
| Neoadjuvant CTx | −0.407 | 0.738 | −2.9493 | 0.006 † |
| Previous RTx | 1.978 | 0.098 | 3.4673 | 0.002 † |
| Adjuvant CTx | 0.0111 | 0.405 | ||
| Postop RTx | 0.961 | 0.212 | 0.0648 | 0.962 |
| Early complication | −0.531 | 0.577 | ||
| Neck dissection | 0.623 | 0.069 | <0.001 | |
| None | Ref | Ref | ||
| MRND | 4.778 | 0.009 | 7.640 | <0.001 † |
| Selective neck dissection | 3.867 | 0.004 | 6.448 | 0.001 |
| Extended neck dissection | 3.333 | 0.162 | 2.934 | 0.182 |
| Other | 6.667 | 0.012 | 8.174 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, L.S.; Wang, H.; Ahn, H.C.; Lee, T.H.; Tae, K.; Park, S.O. The Impact of Postoperative Radiotherapy on Dietary Function of Head and Neck Cancer Patients after Pharyngoesophageal Reconstruction with Free Jejunal Flap. J. Clin. Med. 2022, 11, 2860. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102860
Chang LS, Wang H, Ahn HC, Lee TH, Tae K, Park SO. The Impact of Postoperative Radiotherapy on Dietary Function of Head and Neck Cancer Patients after Pharyngoesophageal Reconstruction with Free Jejunal Flap. Journal of Clinical Medicine. 2022; 11(10):2860. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102860
Chicago/Turabian StyleChang, Lan Sook, Hyun Wang, Hee Chang Ahn, Tae Hyeon Lee, Kyung Tae, and Seong Oh Park. 2022. "The Impact of Postoperative Radiotherapy on Dietary Function of Head and Neck Cancer Patients after Pharyngoesophageal Reconstruction with Free Jejunal Flap" Journal of Clinical Medicine 11, no. 10: 2860. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102860