
Caries Experience and Increment in Children Attending Kindergartens with an Early Childhood Caries Preventive Program Compared to Basic Prophylaxis Measures—A Retrospective Cohort Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria and Dental Examination
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Long–Term Data concerning Caries Experience
3.2. Characteristics of the Intervention and Control Group for Caries Increment Analysis
3.3. Examination Period between 300 and 550 Days
3.4. Examination Period More Than 550 Days
4. Discussion
4.1. Results of the Evaluation in Context with Other Studies
- Compared to permanent dentition, caries progresses faster in primary teeth. The period of amelogenesis is shorter in the primary dentition, leading to a very thin enamel layer and a less organized microstructure [49]. As a result, the enamel of primary teeth is more susceptible to acidic demineralization [50,51].
- Although parental control should still be present, schoolchildren become more and more responsible for their nutritional and dental health care behavior with increasing age and can be motivated to adopt tooth-healthy behavior. At kindergarten age, parents are fully responsible for the nutritional and toothbrushing behavior of their children. Phillips et al. [52] showed an association between unhealthy maternal behavior and the caries experience of the child. Therefore, the mothers/caregivers need to be trained. This training was not within the scope of the ECC preventive program under investigation.
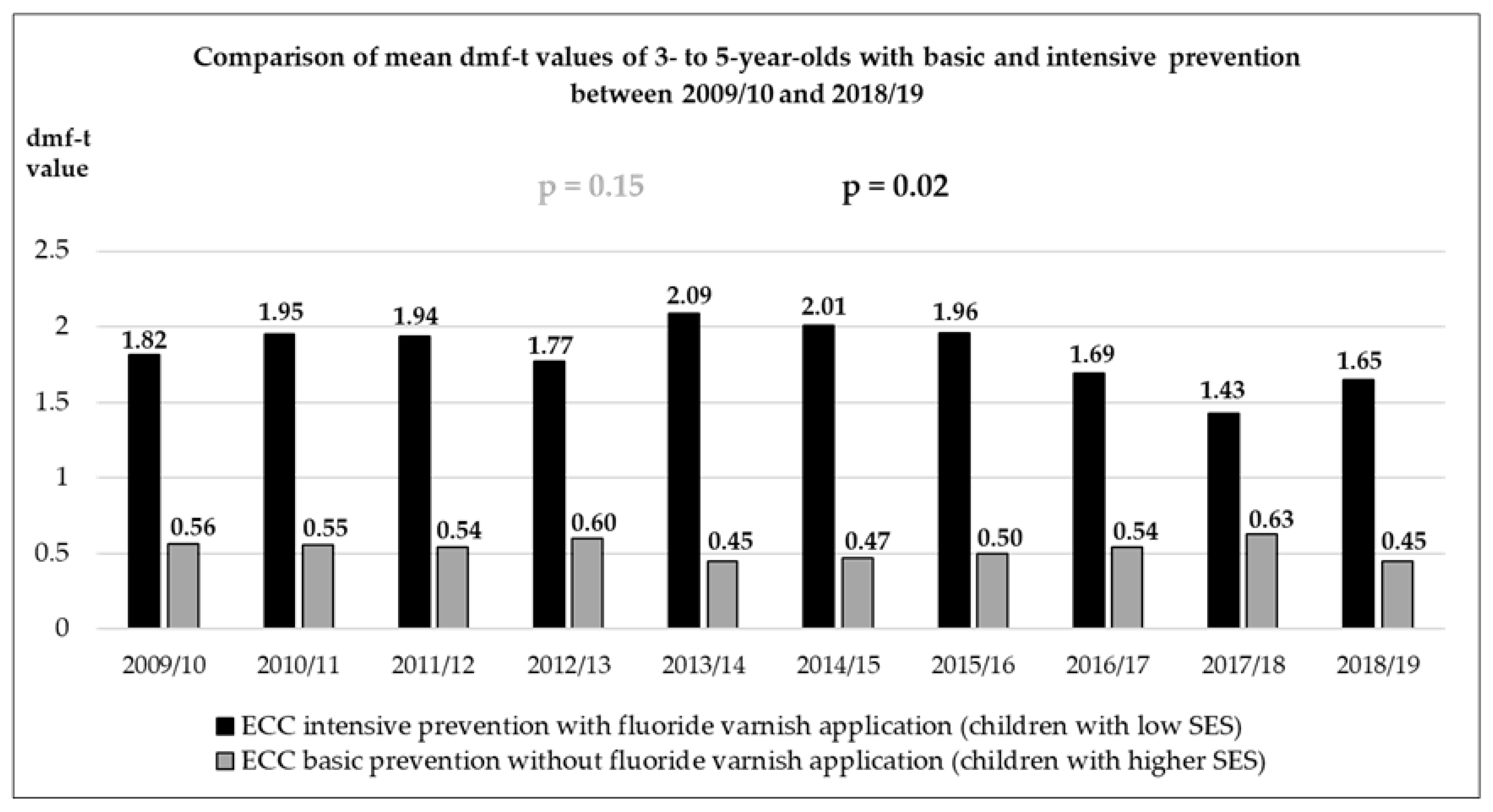
- While a relatively constant and low mean dmf–t value was found when comparing the representative long-term data on the caries experience of 3–5-year-old kindergarten children with basic prophylaxis measures, a significant decline in caries was seen in the kindergarten children from socially deprived areas. This decline in caries may possibly be attributed to regular fluoride varnish applications, where children at the age of five received up to six fluoride varnish applications. The gap between children with and without fluoride varnish application in kindergartens has narrowed slightly over 10 years. Therefore, the null hypothesis—there is no difference between the two groups in regards to long-term caries experience (2009–2019)—must be rejected.
- In both observation periods (300 to 550 and more than 550 days), the mean level of oral rehabilitation improved more in the intervention group than in the control group. This was also shown in an evaluation of an interdisciplinary ECC preventive program in Dormagen, Germany, and was explained by the interprofessional referral system of midwives, pediatricians, social workers, and dentists of the public health service [53]. For the present study, such a referral system existed between the dental public health service and the dentist in dental practice. However, the children were only referred once a year after the dental examination. Both the screening examination (basic prevention) and the examination with fluoride varnish application, as well as the second fluoride varnish application per year (intensive prevention), were written to the parents. Thus, parents whose children attended kindergartens with the ECC preventive program were confronted with the topic of “dentist” once more per year. Possibly, in the case of untreated ECC, the letter appealed to the conscience of the caregivers and led to a treatment appointment.
4.2. Strengths and Limitations
5. Perspectives and Conclusions
- The children with low SES and fluoride varnish application showed positive long-term effects regarding the reduction in caries. However, the decline in caries cannot be explained by the fluoride varnish application alone, as it may have been influenced by confounding factors that were not collected in the study. By implementing the intensive preventive program, the staff of the dental public health service expected a greater decline in caries. Despite the fact that fluoride varnish applications were not capable of preventing carious lesion formation over a short-term period, it would certainly be a valuable add-on to other long-term preventive programs that provide early and low-threshold information [82] and motivation for parents to adopt tooth-healthy dietary and dental hygiene behaviors [83]. Against this background, the well-implemented fluoride varnish application for kindergarten children from socially underprivileged areas should be maintained and supplemented by another interdisciplinary prevention concept involving gynecologists, social workers, pediatricians, and dentists.
- After the implementation of further ECC prevention elements, the complete concept should be evaluated prospectively with appropriate parent questionnaires to survey home nutrition and dental care behavior, dental visits, sociodemographic data, etc.
- The interdisciplinary prevention concept described under point one and used in the Dormagen study [45] should be utilized for all children in the region. For the evaluation of the program, it is important that the respective intervention and the control group do not show any differences during the first dental examination regarding age distribution, mean caries experience, the proportion of children with naturally healthy dentition, and SES.
- Since the likelihood of the reduction in caries is greatest where a large caries experience is found, future studies should include children attending kindergartens in social hotspots. A kindergarten group, used as a historical comparison, could serve as a control group [45]. The children of the control group should not take part in the interdisciplinary program. Better still would be a comparison with a control group from another region without a preventive program and based on matched pairs [47] in terms of age, SES, and caries experience at the first dental examination.
- For such a prospective study, it would already be a success if kindergarten children with a low SES were at the same level of caries increment as kindergarten children with a higher SES. In the present population, this would mean a 0.3 dmf–t lower increase in caries for an observation period of about 550 days. Under these conditions, a sample size calculation was carried out and showed that a group sample size of 450 (intervention group) and 450 (control group) achieved a 90% power to detect a difference of 0.3 using a one-sided Mann–Whitney U when the significance level (alpha) of the test is 0.05, and the standard deviation is 1.5 in both groups.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schroth, R.J.; Levi, J.; Kliewer, E.; Friel, J.; Moffatt, M.E. Association between iron status, iron deficiency anaemia, and severe early childhood caries: A case-control study. BMC Pediatr. 2013, 13, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaoul, R.; Gaitini, L.; Kharouba, J.; Darawshi, G.; Maor, I.; Somri, M. The association of childhood iron deficiency anaemia with severe dental caries. Acta Paediatr. 2012, 101, e76–e79. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.S.; Huang, M.C.; Huang, S.T. Relationship between dental caries status and anemia in children with severe early childhood caries. Kaohsiung J. Med. Sci. 2013, 29, 330–336. [Google Scholar] [CrossRef] [Green Version]
- Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bonecker, M.; Raggio, D.P. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent. Oral Epidemiol. 2011, 39, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Robke, F.J. Effects of nursing bottle misuse on oral health. Prevalence of caries, tooth malalignments and malocclusions in North-German preschool children. J. Orofac. Orthop. 2008, 69, 5–19. [Google Scholar] [CrossRef] [PubMed]
- GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990-2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- ADA. ADA Position on Early Childhood Caries: Prevention and Control of Early Childhood Caries. Available online: https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/caries-risk-assessment-and-management (accessed on 3 May 2022).
- Colak, H.; Dülgergil, C.T.; Dalli, M.; Hamidi, M.M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Meyer, F.; Karch, A.; Schlinkmann, K.M.; Dreesman, J.; Horn, J.; Rübsamen, N.; Sudradjat, H.; Schubert, R.; Mikolajczyk, R. Sociodemographic determinants of spatial disparities in early childhood caries: An ecological analysis in Braunschweig, Germany. Community Dent. Oral Epidemiol. 2017, 45, 442–448. [Google Scholar] [CrossRef]
- Pitts, N.B.; Baez, R.J.; Diaz-Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Seow, W.K.; Sharkov, N.; Songpaisan, Y.; et al. Early Childhood Caries: IAPD Bangkok Declaration. Int. J. Paediatr. Dent. 2019, 29, 384–386. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.; Nicoll, A.D.; Adair, P.M.; Pine, C.M. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar] [PubMed]
- Paglia, L.; Scaglioni, S.; Torchia, V.; De Cosmi, V.; Moretti, M.; Marzo, G.; Giuca, M.R. Familial and dietary risk factors in Early Childhood Caries. Eur. J. Paediatr. Dent. 2016, 17, 93–99. [Google Scholar] [PubMed]
- Dos Santos, A.P.; Nadanovsky, P.; de Oliveira, B.H. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.P.; Oliveira, B.H.; Nadanovsky, P. Effects of low and standard fluoride toothpastes on caries and fluorosis: Systematic review and meta-analysis. Caries Res. 2013, 47, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.T.; Crall, J.J.; Fontana, M.; Gillette, E.J.; Novy, B.B.; Dhar, V.; Donly, K.; Hewlett, E.R.; Quinonez, R.B.; Chaffin, J.; et al. Evidence-based clinical practice guideline for the use of pit-and-fissure sealants: A report of the American Dental Association and the American Academy of Pediatric Dentistry. J. Am. Dent. Assoc. 2016, 147, 672–682.e12. [Google Scholar] [CrossRef] [Green Version]
- Kim Seow, W. Environmental, maternal, and child factors which contribute to early childhood caries: A unifying conceptual model. Int. J. Paediatr. Dent. 2012, 22, 157–168. [Google Scholar] [CrossRef]
- Folayan, M.O.; El Tantawi, M.; Oginni, A.B.; Alade, M.; Adeniyi, A.; Finlayson, T.L. Malnutrition, enamel defects, and early childhood caries in preschool children in a sub-urban Nigeria population. PLoS ONE 2020, 15, e0232998. [Google Scholar] [CrossRef]
- Janakiram, C.; Antony, B.; Joseph, J. Association of Undernutrition and Early Childhood Dental Caries. Indian Pediatr. 2018, 55, 683–685. [Google Scholar] [CrossRef]
- Hart, T.C.; Corby, P.M.; Hauskrecht, M.; Hee Ryu, O.; Pelikan, R.; Valko, M.; Oliveira, M.B.; Hoehn, G.T.; Bretz, W.A. Identification of microbial and proteomic biomarkers in early childhood caries. Int. J. Dent. 2011, 2011, 196721. [Google Scholar] [CrossRef] [Green Version]
- Seow, W.K.; Clifford, H.; Battistutta, D.; Morawska, A.; Holcombe, T. Case-control study of early childhood caries in Australia. Caries Res. 2009, 43, 25–35. [Google Scholar] [CrossRef]
- Tham, R.; Bowatte, G.; Dharmage, S.C.; Tan, D.J.; Lau, M.X.; Dai, X.; Allen, K.J.; Lodge, C.J. Breastfeeding and the risk of dental caries: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 62–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhalla, S.; Tandon, S.; Satyamoorthy, K. Salivary proteins and early childhood caries: A gel electrophoretic analysis. Contemp. Clin. Dent. 2010, 1, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Hemadi, A.S.; Huang, R.; Zhou, Y.; Zou, J. Salivary proteins and microbiota as biomarkers for early childhood caries risk assessment. Int. J. Oral Sci. 2017, 9, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef]
- Corrêa-Faria, P.; Viana, K.A.; Raggio, D.P.; Hosey, M.T.; Costa, L.R. Recommended procedures for the management of early childhood caries lesions—A scoping review by the Children Experiencing Dental Anxiety: Collaboration on Research and Education (CEDACORE). BMC Oral Health 2020, 20, 75. [Google Scholar] [CrossRef]
- Ludovichetti, F.S.; Stellini, E.; Signoriello, A.G.; Di Fiore, A.; Gracco, A.; Mazzoleni, S. Zirconia vs. stainless steel pediatric crowns: A literature review. Minerva Dent. Oral Sci. 2021, 70, 112–118. [Google Scholar] [CrossRef]
- Innes, N.P.; Ricketts, D.; Chong, L.Y.; Keightley, A.J.; Lamont, T.; Santamaria, R.M. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst. Rev. 2015, 2015, Cd005512. [Google Scholar] [CrossRef]
- Alrashdi, M.; Ardoin, J.; Liu, J.A. Zirconia crowns for children: A systematic review. Int. J. Paediatr. Dent. 2022, 32, 66–81. [Google Scholar] [CrossRef]
- Chisini, L.A.; Collares, K.; Cademartori, M.G.; de Oliveira, L.J.C.; Conde, M.C.M.; Demarco, F.F.; Correa, M.B. Restorations in primary teeth: A systematic review on survival and reasons for failures. Int. J. Paediatr. Dent. 2018, 28, 123–139. [Google Scholar] [CrossRef]
- Krämer, N.; Lohbauer, U.; Frankenberger, R. Restorative materials in the primary dentition of poli-caries patients. Eur. Arch. Paediatr. Dent. 2007, 8, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, T.; Born, C. Das Marburger Modell, Ein Konzept zur Gruppen-und Intensivprophylaxe von den Anfängen bis hin zu den neuesten Entwicklungen. Zahnärztl Gesundheitsdienst 2005, 1, 6–8. [Google Scholar]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HGöGD. Hessisches Gesetz über den Öffentlichen Gesundheitsdienst vom 28. September 2007 in der Fassung vom 15. October 2014. Available online: https://www.rv.hessenrecht.hessen.de/bshe/document/jlr-GesDGHEV5P11 (accessed on 3 May 2022).
- Pieper, K. Epidemiologische Begleituntersuchungen zur Gruppenprophylaxe 2004. Gutachten; DAJ: Bonn, Germany, 2005. [Google Scholar]
- DAJ. Epidemiologische Begleituntersuchungen zur Gruppenprophylaxe 2016. Gutachten; DAJ: Bonn, Germany, 2017. [Google Scholar]
- Petersen, P.E.; Baez, R.J.; WHO. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/97035 (accessed on 3 May 2022).
- DAJ. Grundsätze für Maßnahmen zur Förderung der Mundgesundheit. Available online: https://www.daj.de/fileadmin/user_upload/PDF_Downloads/grundsaetze.pdf (accessed on 3 May 2022).
- Meier, M. Sozialbericht der Universitätsstadt Marburg—2013. Available online: https://www.marburg.de/portal/seiten/sozialberichterstattung-daten-fuer-taten-900001172-23001.html (accessed on 1 April 2022).
- Bencze, Z.; Mahrouseh, N.; Andrade, C.A.S.; Kovács, N.; Varga, O. The Burden of Early Childhood Caries in Children under 5 Years Old in the European Union and Associated Risk Factors: An Ecological Study. Nutrients 2021, 13, 455. [Google Scholar] [CrossRef]
- Baggio, S.; Abarca, M.; Bodenmann, P.; Gehri, M.; Madrid, C. Early childhood caries in Switzerland: A marker of social inequalities. BMC Oral Health 2015, 15, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieper, K.; Dressler, S.; Heinzel-Gutenbrunner, M.; Neuhäuser, A.; Krecker, M.; Wunderlich, K.; Jablonski-Momeni, A. The influence of social status on pre-school children’s eating habits, caries experience and caries prevention behavior. Int. J. Public Health 2012, 57, 207–215. [Google Scholar] [CrossRef]
- Winter, J.; Glaser, M.; Heinzel-Gutenbrunner, M.; Pieper, K. Association of caries increment in preschool children with nutritional and preventive variables. Clin. Oral Investig. 2015, 19, 1913–1919. [Google Scholar] [CrossRef]
- Winter, J.; Bartsch, B.; Schutz, C.; Jablonski-Momeni, A.; Pieper, K. Implementation and evaluation of an interdisciplinary preventive program to prevent early childhood caries. Clin. Oral Investig. 2019, 23, 187–197. [Google Scholar] [CrossRef]
- Schiffner, U. 11 Krankheits- und Versorgungsprävalenzen bei Kindern (12-Jährige) 11.1 Karies, Erosionen, Molaren-Inzisiven-Hypomineralisationen. In Fünfte Deutsche Mundgesundheitsstudie DMS V; Jordan, A., Micheelis, W., Eds.; Deutscher Ärzte Verlag: Köln, Germany, 2016; pp. 231–268. [Google Scholar]
- Pieper, K.; Weber, K.; Margraf-Stiksrud, J.; Heinzel-Gutenbrunner, M.; Stein, S.; Jablonski-Momeni, A. Evaluation of a preventive program aiming at children with increased caries risk using ICDAS II criteria. Clin. Oral Investig. 2013, 17, 2049–2055. [Google Scholar] [CrossRef]
- Winter, J.; Weber, K.; Martin, K.; Heinzel-Gutenbrunner, M.; Pieper, K. Evaluation of an intensified prevention program for 4th graders with increased caries risk using ICDAS. Int. J. Paediatr. Dent. 2016, 26, 250–258. [Google Scholar] [CrossRef]
- De Menezes Oliveira, M.A.; Torres, C.P.; Gomes-Silva, J.M.; Chinelatti, M.A.; De Menezes, F.C.; Palma-Dibb, R.G.; Borsatto, M.C. Microstructure and mineral composition of dental enamel of permanent and deciduous teeth. Microsc. Res. Tech. 2010, 73, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.R.; Beynon, A.D. Mineralization differences between human deciduous and permanent enamel measured by quantitative microradiography. Arch. Oral Biol. 1989, 34, 85–88. [Google Scholar] [CrossRef]
- Zamudio-Ortega, C.M.; Contreras-Bulnes, R.; Scougall-Vilchis, R.J.; Morales-Luckie, R.A.; Olea-Mejía, O.F.; Rodríguez-Vilchis, L.E. Morphological, chemical and structural characterisation of deciduous enamel: SEM, EDS, XRD, FTIR and XPS analysis. Eur. J. Paediatr. Dent. 2014, 15, 275–280. [Google Scholar]
- Phillips, M.; Masterson, E.; Sabbah, W. Association between child caries and maternal health-related behaviours. Community Dent. Health 2016, 33, 133–137. [Google Scholar] [CrossRef]
- Schütz, C.; Bartsch, B.; Winter, J.; Jablonski-Momeni, A.; Pieper, K. Gemeinsam gegen Karies. Oralprophylaxe Kinderzahnheilkd 2018, 40, 179–186. [Google Scholar] [CrossRef]
- Hallett, K.B.; O’Rourke, P.K. Pattern and severity of early childhood caries. Community Dent. Oral Epidemiol. 2006, 34, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Van den Branden, S.; Van den Broucke, S.; Leroy, R.; Declerck, D.; Hoppenbrouwers, K. Oral health and oral health-related behaviour in preschool children: Evidence for a social gradient. Eur. J. Pediatr. 2013, 172, 231–237. [Google Scholar] [CrossRef]
- Marinho, V.C.; Worthington, H.V.; Walsh, T.; Clarkson, J.E. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2013, Cd002279. [Google Scholar] [CrossRef]
- Mishra, P.; Fareed, N.; Battur, H.; Khanagar, S.; Bhat, M.A.; Palaniswamy, J. Role of fluoride varnish in preventing early childhood caries: A systematic review. Dent. Res. J. 2017, 14, 169–176. [Google Scholar] [CrossRef]
- De Sousa, F.S.O.; Dos Santos, A.P.P.; Nadanovsky, P.; Hujoel, P.; Cunha-Cruz, J.; de Oliveira, B.H. Fluoride Varnish and Dental Caries in Preschoolers: A Systematic Review and Meta-Analysis. Caries Res. 2019, 53, 502–513. [Google Scholar] [CrossRef]
- Schmoeckel, J.; Gorseta, K.; Splieth, C.H.; Juric, H. How to Intervene in the Caries Process: Early Childhood Caries—A Systematic Review. Caries Res. 2020, 54, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Agouropoulos, A.; Twetman, S.; Pandis, N.; Kavvadia, K.; Papagiannoulis, L. Caries-preventive effectiveness of fluoride varnish as adjunct to oral health promotion and supervised tooth brushing in preschool children: A double-blind randomized controlled trial. J. Dent. 2014, 42, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Pieper, K.; Winter, J.; Krutisch, M.; Volkner-Stetefeld, P.; Jablonski-Momeni, A. Prevention in kindergartens with 500 ppm fluoride toothpaste-a randomized clinical trial. Clin. Oral Investig. 2016, 20, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, 3, Cd007868. [Google Scholar] [CrossRef]
- Lussi, A.; Buzalaf, M.A.R.; Duangthip, D.; Anttonen, V.; Ganss, C.; João-Souza, S.H.; Baumann, T.; Carvalho, T.S. The use of fluoride for the prevention of dental erosion and erosive tooth wear in children and adolescents. Eur. Arch. Paediatr. Dent. 2019, 20, 517–527. [Google Scholar] [CrossRef]
- García-Pola, M.; González-Díaz, A.; García-Martín, J.M. Effect of a Preventive Oral Health Program Starting during Pregnancy: A Case-Control Study Comparing Immigrant and Native Women and Their Children. Int. J. Environ. Res. Public Health 2021, 18, 4096. [Google Scholar] [CrossRef]
- Wagner, Y.; Heinrich-Weltzien, R. Evaluation of an interdisciplinary preventive programme for early childhood caries: Findings of a regional German birth cohort study. Clin. Oral Investig. 2016, 20, 1943–1952. [Google Scholar] [CrossRef]
- Colvara, B.C.; Faustino-Silva, D.D.; Meyer, E.; Hugo, F.N.; Celeste, R.K.; Hilgert, J.B. Motivational interviewing for preventing early childhood caries: A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2021, 49, 10–16. [Google Scholar] [CrossRef]
- Weinstein, P.; Harrison, R.; Benton, T. Motivating mothers to prevent caries: Confirming the beneficial effect of counseling. J. Am. Dent. Assoc. 2006, 137, 789–793. [Google Scholar] [CrossRef]
- Wennhall, I.; Martensson, E.M.; Sjunnesson, I.; Matsson, L.; Schroder, U.; Twetman, S. Caries-preventive effect of an oral health program for preschool children in a low socio-economic, multicultural area in Sweden: Results after one year. Acta Odontol. Scand. 2005, 63, 163–167. [Google Scholar] [CrossRef]
- Schmidt, H.F.M.; Grundmann, T.; Dietze, L.; Zingg, B. Marburger Modell: F-Lackapplikation in Grundschulen. Zahnärztl Mitt 1986, 76, 2587–2592. [Google Scholar] [PubMed]
- Schulte, A.; Born, C.; Stoll, R.; Pieper, K. Die Auswirkung eines Fluoridlack-Programms auf den Kariesbefall 12-Jähriger Schüler in Marburg. Dtsch Zahnärztl Z 1993, 48, 548–550. [Google Scholar]
- Pieper, K.; Born, C.; Hartmann, T.; Heinzel-Gutenbrunner, M.; Jablonski-Momeni, A. Association of preventive measures with caries experience expressed by outcome variables. Schweiz Mon. Zahnmed 2007, 117, 1038–1044. [Google Scholar]
- Talari, K.; Goyal, M. Retrospective studies—Utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef]
- Euser, A.M.; Zoccali, C.; Jager, K.J.; Dekker, F.W. Cohort studies: Prospective versus retrospective. Nephron Clin. Pract. 2009, 113, c214–c217. [Google Scholar] [CrossRef] [Green Version]
- Hess, D.R. Retrospective studies and chart reviews. Respir. Care 2004, 49, 1171–1174. [Google Scholar]
- Manja, V.; Lakshminrusimha, S. Epidemiology and Clinical Research Design, Part 1: Study Types. Neoreviews 2014, 15, e558–e569. [Google Scholar] [CrossRef] [Green Version]
- Tofthagen, C. Threats to validity in retrospective studies. J. Adv. Pract. Oncol. 2012, 3, 181–183. [Google Scholar]
- Jablonski-Momeni, A.; Winter, J.; Petrakakis, P.; Schmidt-Schafer, S. Caries prevalence (ICDAS) in 12-year-olds from low caries prevalence areas and association with independent variables. Int. J. Paediatr. Dent. 2014, 24, 90–97. [Google Scholar] [CrossRef]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Uebereck, C.; Kühnisch, J.; Michael, R.; Taschner, M.; Frankenberger, R.; Krämer, N. Zahngesundheit bayerischer Schulkinder 2015/16. Oralprophylaxe Kinderzahnheilkd 2017, 39, 161–171. [Google Scholar] [CrossRef]
- Knoblauch, U.; Ritschel, G.; Weidner, K.; Mogwitz, S.; Hannig, C.; Viergutz, G.; Lenk, M. The association between socioeconomic status, psychopathological symptom burden in mothers, and early childhood caries of their children. PLoS ONE 2019, 14, e0224509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigel, J.; Forster, J.; Berner, R.; Puppe, W.; Neumann-Häfelin, D.; Meyer, C.; Zepp, F.; Schmitt, H.J. Virale Atemwegsinfektionen mit saisonaler Häufung bei Kindern Eine Übersicht mit Schwerpunkt auf Daten aus Deutschland. Bundesgesundheitsbl-Gesundheitsforsch-Gesundheitsschutz 2003, 46, 9–19. [Google Scholar] [CrossRef]
- Splieth, C.H.; Banerjee, A.; Bottenberg, P.; Breschi, L.; Campus, G.; Ekstrand, K.R.; Giacaman, R.A.; Haak, R.; Hannig, M.; Hickel, R.; et al. How to Intervene in the Caries Process in Children: A Joint ORCA and EFCD Expert Delphi Consensus Statement. Caries Res. 2020, 54, 297–305. [Google Scholar] [CrossRef]
- Colvara, B.C.; Faustino-Silva, D.D.; Meyer, E.; Hugo, F.N.; Hilgert, J.B.; Celeste, R.K. Motivational Interviewing in Preventing Early Childhood Caries in Primary Healthcare: A Community-based Randomized Cluster Trial. J. Pediatr. 2018, 201, 190–195. [Google Scholar] [CrossRef]


{kind=link}
| Year | 2009/10 | 2010/11 | 2011/12 | 2012/13 | 2013/14 | 2014/15 | 2015/16 | 2016/17 | 2017/18 | 2018/19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of children | TG | 1201 | 1233 | 1389 | 1276 | 1414 | 1392 | 1440 | 1454 | 1430 | 1526 |
| CG | 1026 | 1009 | 1200 | 1056 | 1203 | 1181 | 1223 | 1246 | 1224 | 1294 | |
| IG | 175 | 224 | 189 | 220 | 211 | 211 | 217 | 208 | 206 | 232 | |
| Mean dmf–t value [mean ± SD] | TG | 0.75 ± 2.00 | 0.81 ± 2.12 | 0.73 ± 2.04 | 0.80 ± 2.06 | 0.68 ± 1.95 | 0.78 ± 2.00 | 0.72 ± 2.01 | 0.71 ± 1.98 | 0.75 ± 2.11 | 0.64 ± 1.80 |
| Number of children with dmf–t = 0 [n (% of group)] | TG | 955 (79.52) | 974 (78.99) | 1124 (80.92) | 1003 (78.61) | 1156 (81.75) | 1139 (81.82) | 1178 (81.81) | 1197 (82.32) | 1170 (81.82) | 1253 (82.11) |
| CG | 855 (83.33) | 856 (84.84) | 1011 (84.25) | 874 (82.77) | 1033 (85.87) | 1011 (85.61) | 1052 (86.02) | 1067 (85.63) | 1039 (84.89) | 1123 (86.79) | |
| IG | 100 (57.14) | 118 (52.68) | 113 (59.79) | 129 (58.64) | 123 (58.29) | 128 (60.66) | 126 (58.06) | 130 (62.50) | 131 (63.59) | 130 (56.03) | |
| Number of children with dmf–t > 0 [n (% of group)] | TG | 246 (20.48) | 259 (21.01) | 265 (19.08) | 273 (21.39) | 258 (18.25) | 253 (18.18) | 262 (18.19) | 257 (17.68) | 260 (18.18) | 273 (17.89) |
| CG | 171 (16.7) | 153 (15.16) | 189 (15.75) | 182 (17.23) | 170 (14.13) | 170 (14.39) | 171 (13.98) | 179 (14.37) | 185 (15.11) | 171 (13.21) | |
| IG | 75 (42.86) | 106 (47.32) | 76 (40.21) | 91 (41.36) | 88 (41.71) | 83 (39.34) | 91 (41.94) | 78 (37.50) | 75 (36.41) | 102 (43.97) | |
| Mean dmf–t value of children with caries experience total group [mean ± SD (minimum–maximum)] | TG | 3.64 ± 2.99 (1–14) | 3.85 ± 3.13 (1–15) | 3.85 ± 3.13 (1–16) | 3.74 ± 2.97 (1–15) | 3.80 ± 3.20 (1–18) | 3.89 ± 3.12 (1–18) | 3.94 ± 3.08 (1–16) | 4.00 ± 3.02 (1–17) | 4.1 ± 3.27 (1–19) | 3.56 ± 2.78 (1–14) |
| CG | 3.38 ± 2.79 (1–14) | 3.65 ± 3.13 (1–15) | 3.46 ± 3.05 (1–16) | 3.48 ± 2.88 (1–14) | 3.18 ± 2.51 (1–12) | 3.29 ± 2.75 (1–18) | 3.55 ± 2.76 (1–13) | 3.77 ± 2.82 (1–16) | 4.15 ± 3.49 (1–19) | 3.42 ± 2.72 (1–14) | |
| IG | 4.24 ± 3.36 (1–14) | 4.12 ± 3.13 (1–14) | 4.82 ± 3.12 (1–14) | 4.27 ± 3.07 (1–15) | 5.00 ± 3.98 (1–18) | 5.11 ± 3.44 (1–14) | 4.67 ± 3.50 (1–16) | 4.51 ± 3.40 (1–17) | 3.96 ± 2.67 (1–12) | 3.75 ± 2.86 (1–12) | |
| Observation Period | 300 to 550 Days | More Than 550 Days | |||
|---|---|---|---|---|---|
| Groups | IG N = 122 | CG N = 91 | IG N = 57 | CG N = 46 | |
| dmf–t = 0 and no initial carious lesions present [n (%)] | FDE | 80 (65.57) | 67 (73.63) | 40 (70.18) | 42 (91.3) |
| SDE | 68 (55.74) | 50 (54.95) | 31 (54.39) | 36 (78.26) | |
| dmf–t = 0 and initial carious lesions present [n (%)] | FDE | 9 (7.38) | 10 (10.99) | 5 (8.77) | 2 (4.35) |
| SDE | 4 (3.28) | 9 (9.89) | 4 (7.08) | 1 (2.17) | |
| dmf–t > 0 [n (%)] | FDE | 33 (27.05) | 14 (15.38) | 12 (21.05) | 2 (4.35) |
| SDE | 50 (40.98) | 32 (35.16) | 22 (38.6) | 9 (19.57) | |
| Increased caries risk according to DAJ criteria [n (%)] | FDE | 27 (22.13) | 13 (14.29) | 8 (14.04) | 2 (4.35) |
| SDE | 25 (20.49) | 13 (14.29) | 8 (14.04) | 2 (4.35) | |
| Mean dmf–t [mean ± SD (minimum–maximum)] | FDE | 0.96 ± 2.14 (0–12) | 0.75 ± 2.14 (0–12) | 0.54 ± 1.27 (0–6) | 0.13 ± 0.65 (0–4) |
| SDE | 1.73 ± 2.87 (0–13) | 1.34 ± 2.80 (0–14) | 1.88 ± 3.04 (0–11) | 0.57 ± 1.57 (0–8) | |
| Mean level of oral rehabilitation [%] | FDE | 20.32 | 35.91 | 16.67 | 25 |
| SDE | 41.71 | 38.49 | 50.67 | 29.63 | |
| Caries increment between FDE and SDE [n (%)] | 40 (32.79) | 24 (26.37) | 21 (36.84) | 8 (17.39) | |
| Caries increment [mean ± SD (minimum–maximum)] | 0.80 ± 1.48 (0–7) | 0.59 ± 1.13 (0–5) | 1.33 ± 2.33 (0–11) | 0.43 ± 1.05 (0–4) | |
| Caries increment among children with a high caries risk [mean ± SD (minimum–maximum)] | 2.52 ± 2.06 (0–7) | 2.46 ± 1.51 (0–5) | 5.5 ± 3.12 (1–11) | 4 ± 0.00 (4–4) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amend, S.; Hartmann, T.; Heinzel-Gutenbrunner, M.; Frankenberger, R.; Krämer, N.; Winter, J. Caries Experience and Increment in Children Attending Kindergartens with an Early Childhood Caries Preventive Program Compared to Basic Prophylaxis Measures—A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 2864. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102864
Amend S, Hartmann T, Heinzel-Gutenbrunner M, Frankenberger R, Krämer N, Winter J. Caries Experience and Increment in Children Attending Kindergartens with an Early Childhood Caries Preventive Program Compared to Basic Prophylaxis Measures—A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(10):2864. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102864
Chicago/Turabian StyleAmend, Stefanie, Thea Hartmann, Monika Heinzel-Gutenbrunner, Roland Frankenberger, Norbert Krämer, and Julia Winter. 2022. "Caries Experience and Increment in Children Attending Kindergartens with an Early Childhood Caries Preventive Program Compared to Basic Prophylaxis Measures—A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 10: 2864. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102864