
A Radiographic Analysis of Proximal Humeral Anatomy in Patients with Primary Glenohumeral Arthritis and Implications for Press-Fit Stem Length


Abstract
:1. Introduction
2. Materials and Methods
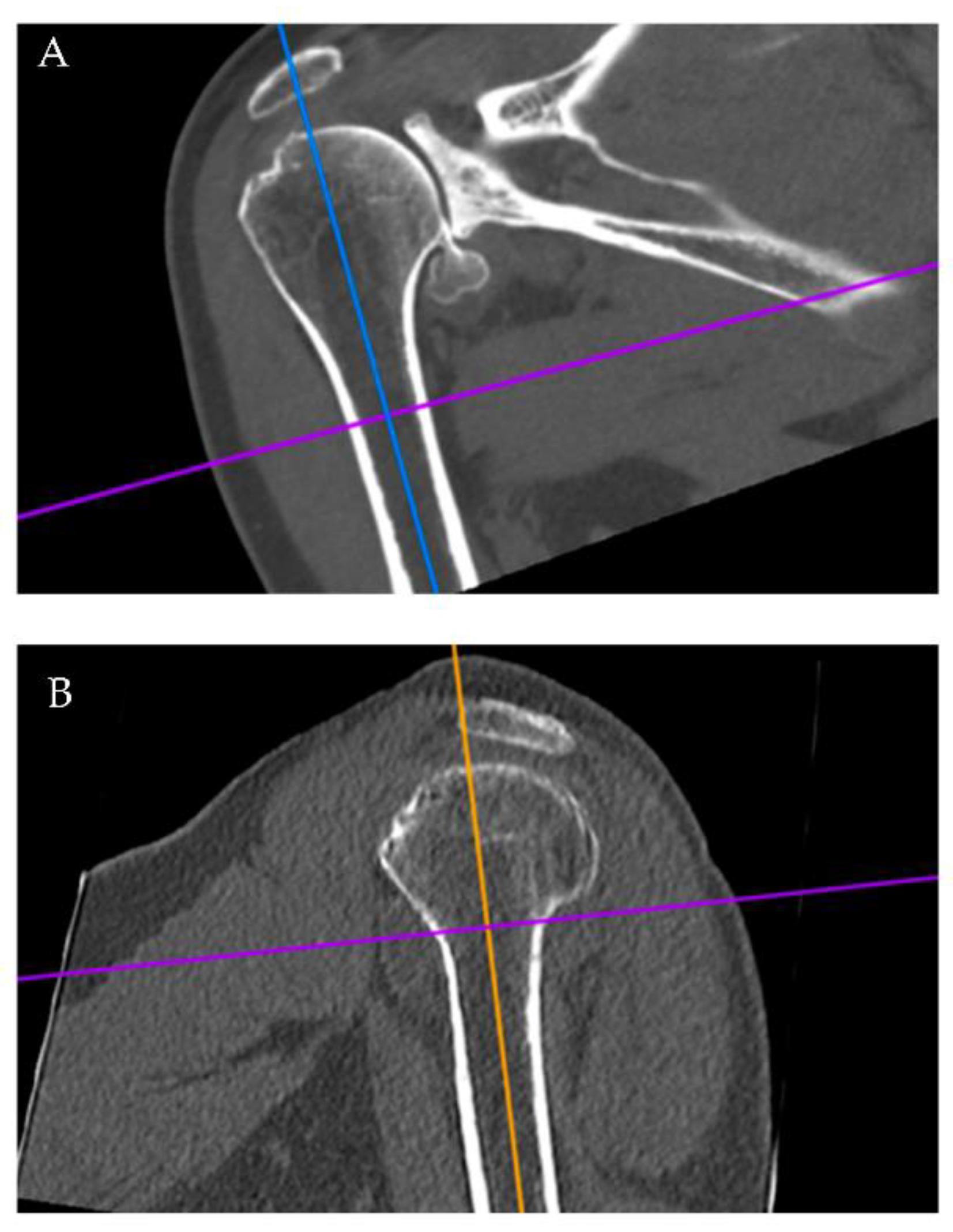
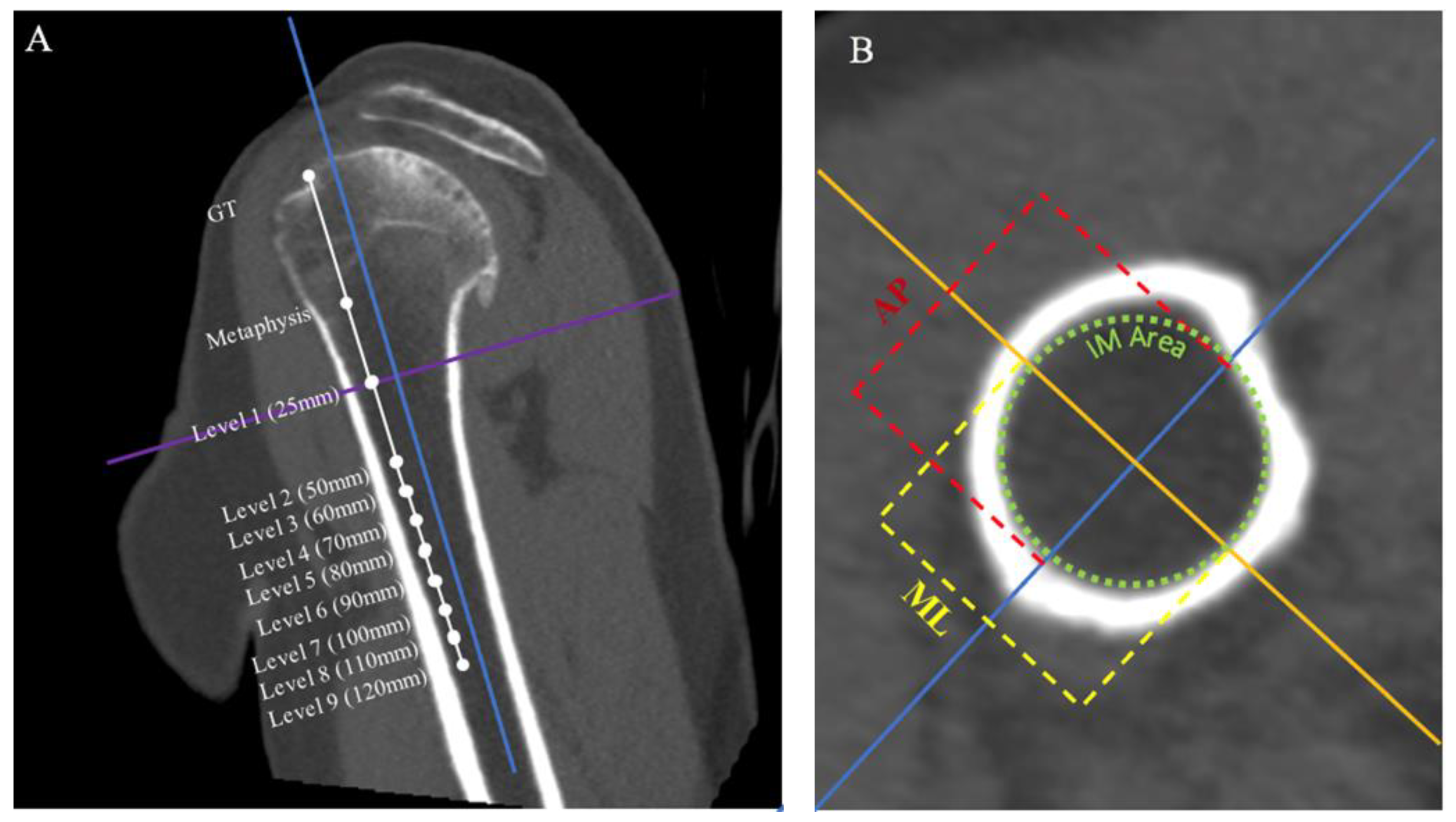
2.1. Radiographic Evaluation
2.2. Statistical Analysis
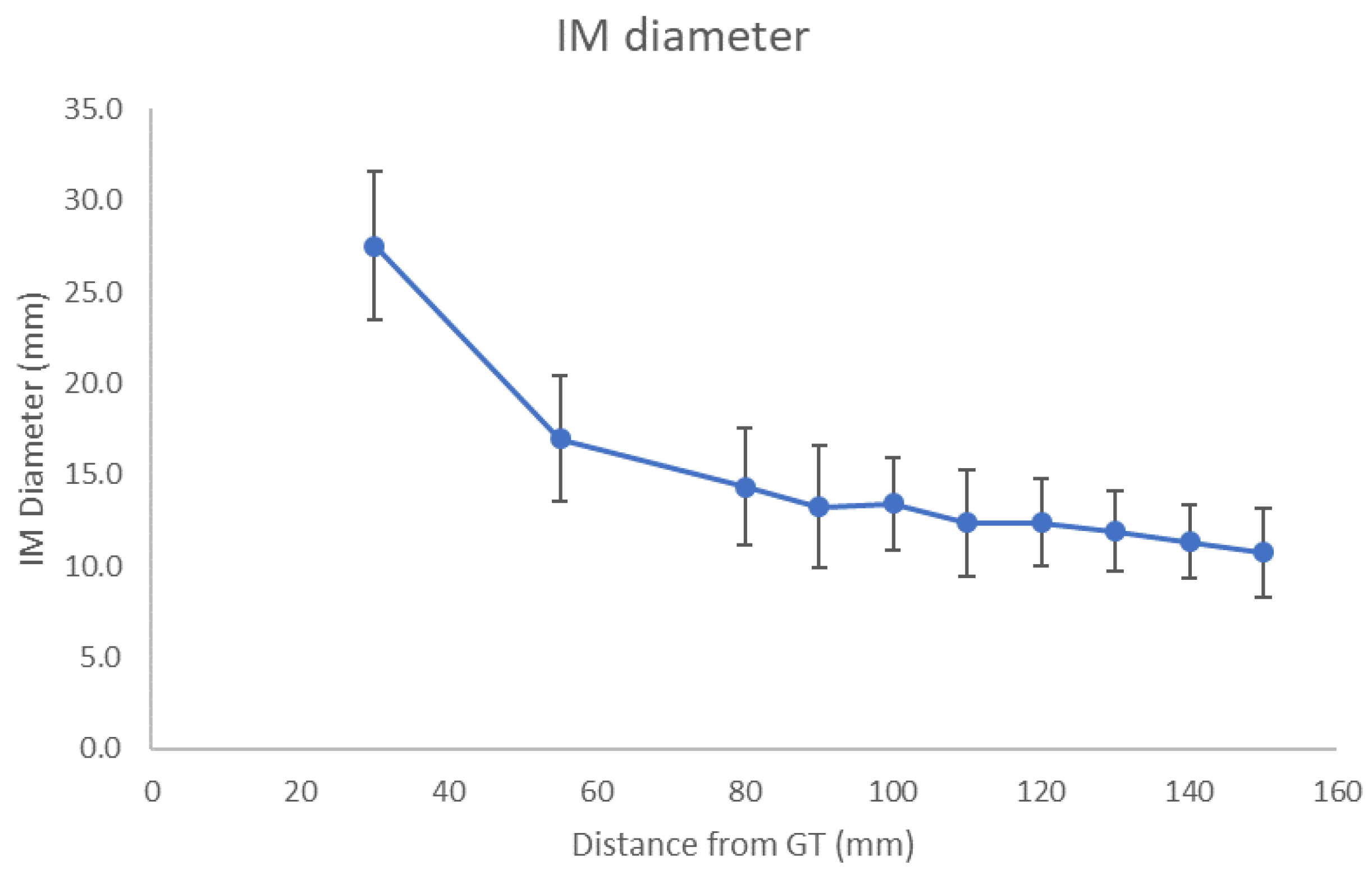
3. Results
3.1. Male vs Female
3.2. Stem Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deshmukh, A.V.; Koris, M.; Zurakowski, D.; Thornhill, T.S. Total Shoulder Arthroplasty: Long-Term Survivorship, Functional Outcome, and Quality of Life. J. Shoulder Elb. Surg. 2005, 14, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Mansat, P.; Mansat, M.; Bellumore, Y.; Rongières, M.; Bonnevialle, P. Mid-term results of shoulder arthroplasty for primary osteoarthritis. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2002, 88, 544–552. [Google Scholar] [PubMed]
- Torchia, M.E.; Cofield, R.H.; Settergren, C.R. Total Shoulder Arthroplasty with the Neer Prosthesis: Long-Term Results. J. Shoulder Elb. Surg. 1997, 6, 495–505. [Google Scholar] [CrossRef]
- Best, M.J.; Aziz, K.T.; Wilckens, J.H.; McFarland, E.G.; Srikumaran, U. Increasing Incidence of Primary Reverse and Anatomic Total Shoulder Arthroplasty in the United States. J. Shoulder Elb. Surg. 2021, 30, 1159–1166. [Google Scholar] [CrossRef]
- Ravi, V.; Murphy, R.J.; Moverley, R.; Derias, M.; Phadnis, J. Outcome and Complications Following Revision Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. Bone Jt. Open 2021, 2, 618–630. [Google Scholar] [CrossRef]
- Denard, P.J.; Raiss, P.; Gobezie, R.; Edwards, T.B.; Lederman, E. Stress Shielding of the Humerus in Press-Fit Anatomic Shoulder Arthroplasty: Review and Recommendations for Evaluation. J. Shoulder Elb. Surg. 2018, 27, 1139–1147. [Google Scholar] [CrossRef]
- Bauer, T.W.; Schils, J. The Pathology of Total Joint Arthroplasty. Skelet. Radiol. 1999, 28, 483–497. [Google Scholar] [CrossRef]
- Dujovne, A.R.; Bobyn, J.D.; Krygier, J.J.; Miller, J.E.; Brooks, C.E. Mechanical Compatibility of Noncemented Hip Prostheses with the Human Femur. J. Arthroplast. 1993, 8, 7–22. [Google Scholar] [CrossRef]
- Engh, C.; Bobyn, J.; Glassman, A. Porous-Coated Hip Replacement. The Factors Governing Bone Ingrowth, Stress Shielding, and Clinical Results. J. Bone Jt. Surgery. Br. Vol. 1987, 69-B, 45–55. [Google Scholar] [CrossRef]
- Nagels, J.; Stokdijk, M.; Rozing, P.M. Stress Shielding and Bone Resorption in Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2003, 12, 35–39. [Google Scholar] [CrossRef]
- Oh, H.K.; Lim, T.K. Short Humeral Stems in Shoulder Arthroplasty. Clin Shoulder Elb. 2018, 21, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tracy, S.T.; Werner, B.C.; Steinbeck, J.; Smith, M.J.; Lin, A.; Sears, B.W.; Hatzidakis, A.M.; Cohen, B.S.; Lichtenberg, S.; Lederman, E.S.; et al. Revision to Reverse Total Shoulder Arthroplasty: Do Short Stem and Stemless Implants Reduce the Operative Burden Compared to Convertible Stems? Semin. Arthroplast. JSES 2021, 31, 248–254. [Google Scholar] [CrossRef]
- Abdic, S.; Athwal, G.S.; Wittmann, T.; Walch, G.; Raiss, P. Short Stem Humeral Components in Reverse Shoulder Arthroplasty: Stem Alignment Influences the Neck-Shaft Angle. Arch. Orthop. Trauma Surg. 2021, 141, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Ascione, F.; Bugelli, G.; Domos, P.; Neyton, L.; Godeneche, A.; Bercik, M.J.; Walch, G. Reverse Shoulder Arthroplasty with a New Convertible Short Stem: Preliminary 2- to 4-Year Follow-up Results. J. Shoulder Elb. Arthroplast. 2017, 1, 247154921774627. [Google Scholar] [CrossRef] [Green Version]
- Casagrande, D.J.; Parks, D.L.; Torngren, T.; Schrumpf, M.A.; Harmsen, S.M.; Norris, T.R.; Kelly, J.D. Radiographic Evaluation of Short-Stem Press-Fit Total Shoulder Arthroplasty: Short-Term Follow-Up. J. Shoulder Elb. Surg. 2016, 25, 1163–1169. [Google Scholar] [CrossRef]
- Denard, P.J.; Noyes, M.P.; Walker, J.B.; Shishani, Y.; Gobezie, R.; Romeo, A.A.; Lederman, E. Radiographic Changes Differ between Two Different Short Press-Fit Humeral Stem Designs in Total Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 217–223. [Google Scholar] [CrossRef]
- Godenèche, A.; Garret, J.; Barth, J.; Michelet, A.; Geais, L.; Shoulder Friends Institute. Comparison of Revision Rates and Radiographic Observations of Long and Short, Uncoated and Coated Humeral Stem Designs in Total Shoulder Arthroplasty. EFORT Open Rev. 2019, 4, 70–76. [Google Scholar] [CrossRef]
- Jost, P.W.; Dines, J.S.; Griffith, M.H.; Angel, M.; Altchek, D.W.; Dines, D.M. Total Shoulder Arthroplasty Utilizing Mini-Stem Humeral Components: Technique and Short-Term Results. HSS J. 2011, 7, 213–217. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Sperling, J.W.; Haidukewych, G.H.; Cofield, R.H. Periprosthetic Humeral Fractures after Shoulder Arthroplasty. J. Bone Jt. Surg.-Am. Vol. 2004, 86, 680–689. [Google Scholar] [CrossRef]
- Lädermann, A.; Chiu, J.C.-H.; Cunningham, G.; Hervé, A.; Piotton, S.; Bothorel, H.; Collin, P. Do Short Stems Influence the Cervico-Diaphyseal Angle and the Medullary Filling after Reverse Shoulder Arthroplasties? Orthop. Traumatol. Surg. Res. 2020, 106, 241–246. [Google Scholar] [CrossRef]
- Morwood, M.P.; Johnston, P.S.; Garrigues, G.E. Proximal Ingrowth Coating Decreases Risk of Loosening Following Uncemented Shoulder Arthroplasty Using Mini-Stem Humeral Components and Lesser Tuberosity Osteotomy. J. Shoulder Elb. Surg. 2017, 26, 1246–1252. [Google Scholar] [CrossRef] [PubMed]
- Raiss, P.; Schnetzke, M.; Wittmann, T.; Kilian, C.M.; Edwards, T.B.; Denard, P.J.; Neyton, L.; Godenèche, A.; Walch, G. Postoperative Radiographic Findings of an Uncemented Convertible Short Stem for Anatomic and Reverse Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2019, 28, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Romeo, A.A.; Thorsness, R.J.; Sumner, S.A.; Gobezie, R.; Lederman, E.S.; Denard, P.J. Short-Term Clinical Outcome of an Anatomic Short-Stem Humeral Component in Total Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 70–74. [Google Scholar] [CrossRef]
- Schnetzke, M.; Loew, M.; Raiss, P.; Walch, G. Short-Stem Anatomical Shoulder Replacement—a Systematic Review. Obere Extrem. 2019, 14, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Zmistowski, B.; Carpenter, D.P.; Chalmers, P.N.; Smith, M.J.; Keener, J.D. Symptomatic Aseptic Loosening of a Short Humeral Stem Following Anatomic Total Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2021, 30, 2738–2744. [Google Scholar] [CrossRef]
- Denard, P.J.; Werner, B.C.; Gobezie, R.; Cohen, B.S.; Lederman, E. Cause for Revision Differs between a Short and Standard Length Stem at 5 Year Follow-Up. Semin. Arthroplast. JSES 2021, 31, 836–841. [Google Scholar] [CrossRef]
- Goetzmann, T.; Molé, D.; Aisene, B.; Neyton, L.; Godeneche, A.; Walch, G.; Sirveaux, F.; Jacquot, A. A Short and Convertible Humeral Stem for Shoulder Arthroplasty: Preliminary Results. J. Shoulder Elb. Arthroplast. 2017, 1, 247154921772272. [Google Scholar] [CrossRef]
- Denard, P.J.; Noyes, M.P.; Walker, J.B.; Shishani, Y.; Gobezie, R.; Romeo, A.A.; Lederman, E. Proximal Stress Shielding Is Decreased with a Short Stem Compared with a Traditional-Length Stem in Total Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 53–58. [Google Scholar] [CrossRef]
- Razfar, N.; Reeves, J.M.; Langohr, D.G.; Willing, R.; Athwal, G.S.; Johnson, J.A. Comparison of Proximal Humeral Bone Stresses between Stemless, Short Stem, and Standard Stem Length: A Finite Element Analysis. J. Shoulder Elb. Surg. 2016, 25, 1076–1083. [Google Scholar] [CrossRef]
- Diaz, M.A.; Gorman, R.A.; Mahendraraj, K.A.; Paredes, L.A.; Brewley, E.E.; Jawa, A. The Effect of Stem Length on Reverse Total Shoulder Humeral Fixation. Semin. Arthroplast. JSES 2021, 31, 139–146. [Google Scholar] [CrossRef]
- Kassi, J.-P.; Heller, M.O.; Stoeckle, U.; Perka, C.; Duda, G.N. Stair Climbing Is More Critical than Walking in Pre-Clinical Assessment of Primary Stability in Cementless THA in Vitro. J. Biomech. 2004, 38, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Reimeringer, M.; Nuño, N.; Desmarais-Trépanier, C.; Lavigne, M.; Vendittoli, P.A. The Influence of Uncemented Femoral Stem Length and Design on Its Primary Stability: A Finite Element Analysis. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 1221–1231. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | ||||||
|---|---|---|---|---|---|---|
| Total Distance From GT | ML (mm) | p-Value vs. Level above | AP (mm) | p-Value vs. Level above | IM Diameter (mm) | p-Value vs. Level above |
| Metaphysis | 34.7 | 30.7 | 27.5 | |||
| Level 1 | 19.1 | <0.001 | 18.4 | <0.001 | 16.9 | <0.001 |
| Level 2 | 15.8 | <0.001 | 15.5 | <0.001 | 14.3 | <0.001 |
| Level 3 | 15.0 | 0.058 | 14.8 | 0.075 | 13.2 | 0.018 |
| Level 4 | 14.4 | 0.140 | 14.3 | 0.178 | 13.4 | 0.631 |
| Level 5 | 13.6 | >0.05 | 13.7 | >0.05 | 12.4 | >0.05 |
| Level 6 | 13.6 | >0.05 | 13.5 | >0.05 | 12.3 | >0.05 |
| Level 7 | 12.9 | >0.05 | 13.1 | >0.05 | 11.9 | >0.05 |
| Level 8 | 12.4 | >0.05 | 12.5 | >0.05 | 11.3 | >0.05 |
| Level 9 | 12.2 | >0.05 | 12.5 | >0.05 | 10.7 | >0.05 |
| Males | ||||||
|---|---|---|---|---|---|---|
| Total Distance From GT | ML (mm) | p-Value vs. Level above | AP (mm) | p-Value vs. Level above | IM Diameter (mm) | p-Value vs. Level above |
| Metaphysis | 36.5 | 32.0 | 29.1 | |||
| Level 1 | 20.5 | <0.001 | 19.7 | <0.001 | 18.1 | <0.001 |
| Level 2 | 17.1 | <0.001 | 16.6 | <0.001 | 15.8 | <0.001 |
| Level 3 | 16.2 | 0.065 | 15.7 | 0.070 | 14.3 | 0.005 |
| Level 4 | 15.5 | 0.142 | 15.1 | >0.05 | 14.3 | >0.05 |
| Level 5 | 14.4 | >0.05 | 14.4 | >0.05 | 13.1 | >0.05 |
| Level 6 | 14.4 | >0.05 | 13.8 | >0.05 | 13.0 | >0.05 |
| Level 7 | 13.5 | >0.05 | 13.5 | >0.05 | 12.5 | >0.05 |
| Level 8 | 13.0 | >0.05 | 13.0 | >0.05 | 11.9 | >0.05 |
| Level 9 | 12.7 | >0.05 | 12.9 | >0.05 | 11.4 | >0.05 |
| Females | ||||||
|---|---|---|---|---|---|---|
| Total Distance From GT | ML (mm) | p-Value vs. Level above | AP (mm) | p-Value vs. Level above | IM Diameter (mm) | p-Value vs. Level above |
| Metaphysis | 32.1 | 29.0 | 25.3 | |||
| Level 1 | 17.0 | <0.001 | 16.5 | <0.001 | 15.3 | <0.001 |
| Level 2 | 13.9 | <0.001 | 14.0 | <0.001 | 12.3 | <0.001 |
| Level 3 | 13.3 | 0.281 | 13.6 | 0.435 | 11.7 | 0.361 |
| Level 4 | 12.7 | >0.05 | 13.0 | >0.05 | 11.9 | >0.05 |
| Level 5 | 12.3 | >0.05 | 12.6 | >0.05 | 11.2 | >0.05 |
| Level 6 | 12.2 | >0.05 | 12.8 | >0.05 | 11.2 | >0.05 |
| Level 7 | 11.7 | >0.05 | 12.1 | >0.05 | 10.7 | >0.05 |
| Level 8 | 10.8 | >0.05 | 11.1 | >0.05 | 9.9 | >0.05 |
| Level 9 | 10.6 | >0.05 | 11.4 | >0.05 | 8.8 | >0.05 |
| Diameter | ||||
|---|---|---|---|---|
| Total Distance from GT | Male (mm) | Female (mm) | Mean Diff (mm) | p |
| Metaphysis | 29.1 | 25.3 | 3.8 | <0.001 |
| Level 1 | 18.1 | 15.3 | 2.9 | <0.001 |
| Level 2 | 15.8 | 12.3 | 3.6 | <0.001 |
| Level 3 | 14.3 | 11.7 | 2.6 | <0.001 |
| Level 4 | 14.3 | 11.9 | 2.4 | <0.001 |
| Level 5 | 13.1 | 11.2 | 1.8 | 0.004 |
| Level 6 | 13.0 | 11.2 | 1.8 | 0.001 |
| Level 7 | 12.5 | 10.7 | 1.8 | 0.002 |
| Level 8 | 11.9 | 9.9 | 2.0 | 0.002 |
| Level 9 | 11.4 | 8.8 | 2.6 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bents, E.J.; Werner, B.C.; Griffin, J.W.; Raiss, P.; Denard, P.J. A Radiographic Analysis of Proximal Humeral Anatomy in Patients with Primary Glenohumeral Arthritis and Implications for Press-Fit Stem Length. J. Clin. Med. 2022, 11, 2867. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102867
Bents EJ, Werner BC, Griffin JW, Raiss P, Denard PJ. A Radiographic Analysis of Proximal Humeral Anatomy in Patients with Primary Glenohumeral Arthritis and Implications for Press-Fit Stem Length. Journal of Clinical Medicine. 2022; 11(10):2867. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102867
Chicago/Turabian StyleBents, Easton J., Brian C. Werner, Justin W. Griffin, Patric Raiss, and Patrick J. Denard. 2022. "A Radiographic Analysis of Proximal Humeral Anatomy in Patients with Primary Glenohumeral Arthritis and Implications for Press-Fit Stem Length" Journal of Clinical Medicine 11, no. 10: 2867. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102867