
Endogenous Pain Modulation in Response to a Single Session of Percutaneous Electrolysis in Healthy Population: A Double-Blinded Randomized Clinical Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants Recruitment and Eligibility Criteria
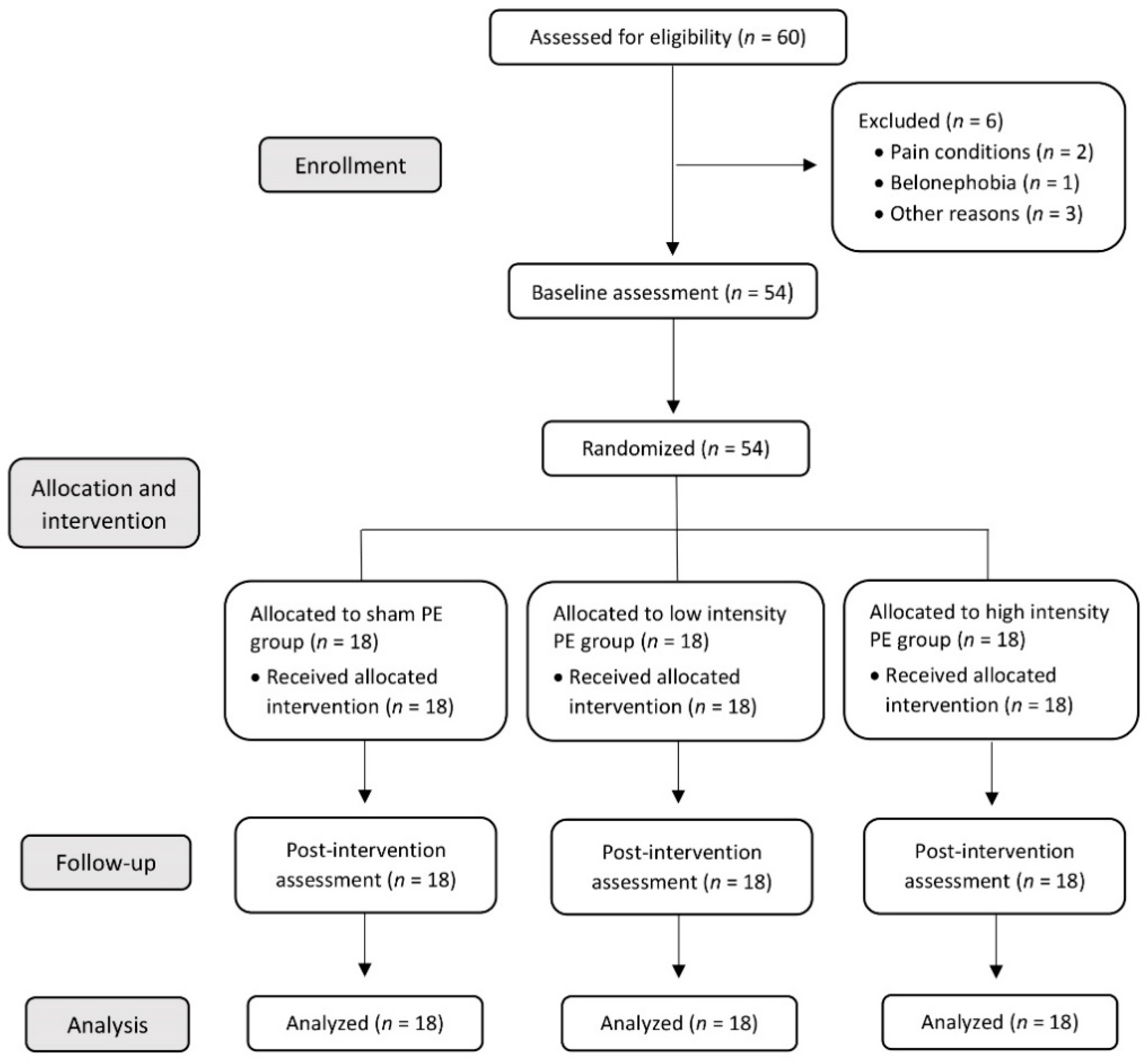
2.3. Allocation and Randomization
2.4. Blinding
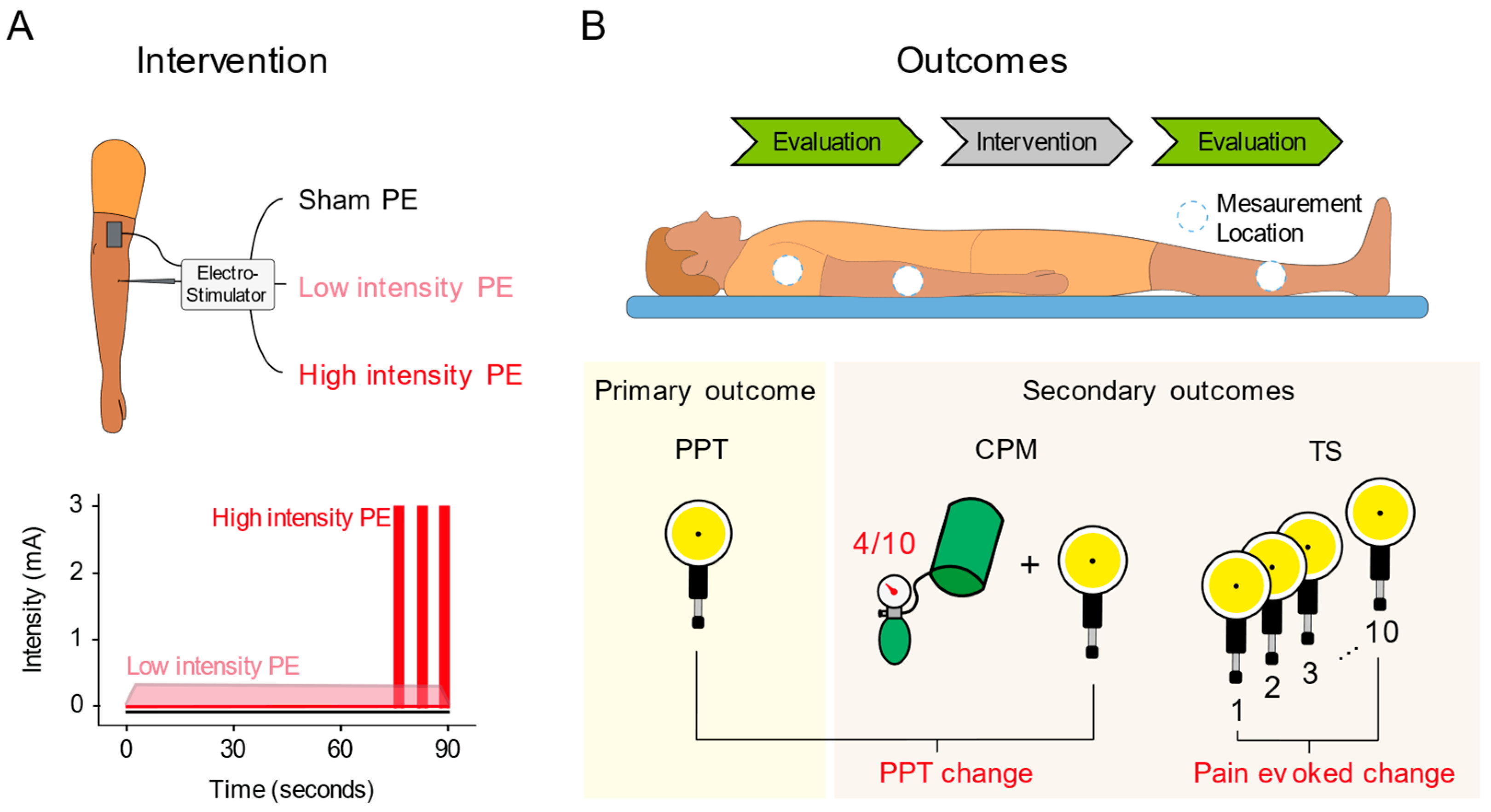
2.5. Interventions
2.6. Outcomes
2.6.1. Primary Outcome
2.6.2. Secondary Outcomes
2.7. Sample Size Calculation
2.8. Statistical Analysis
3. Results
3.1. Sample Characteristics
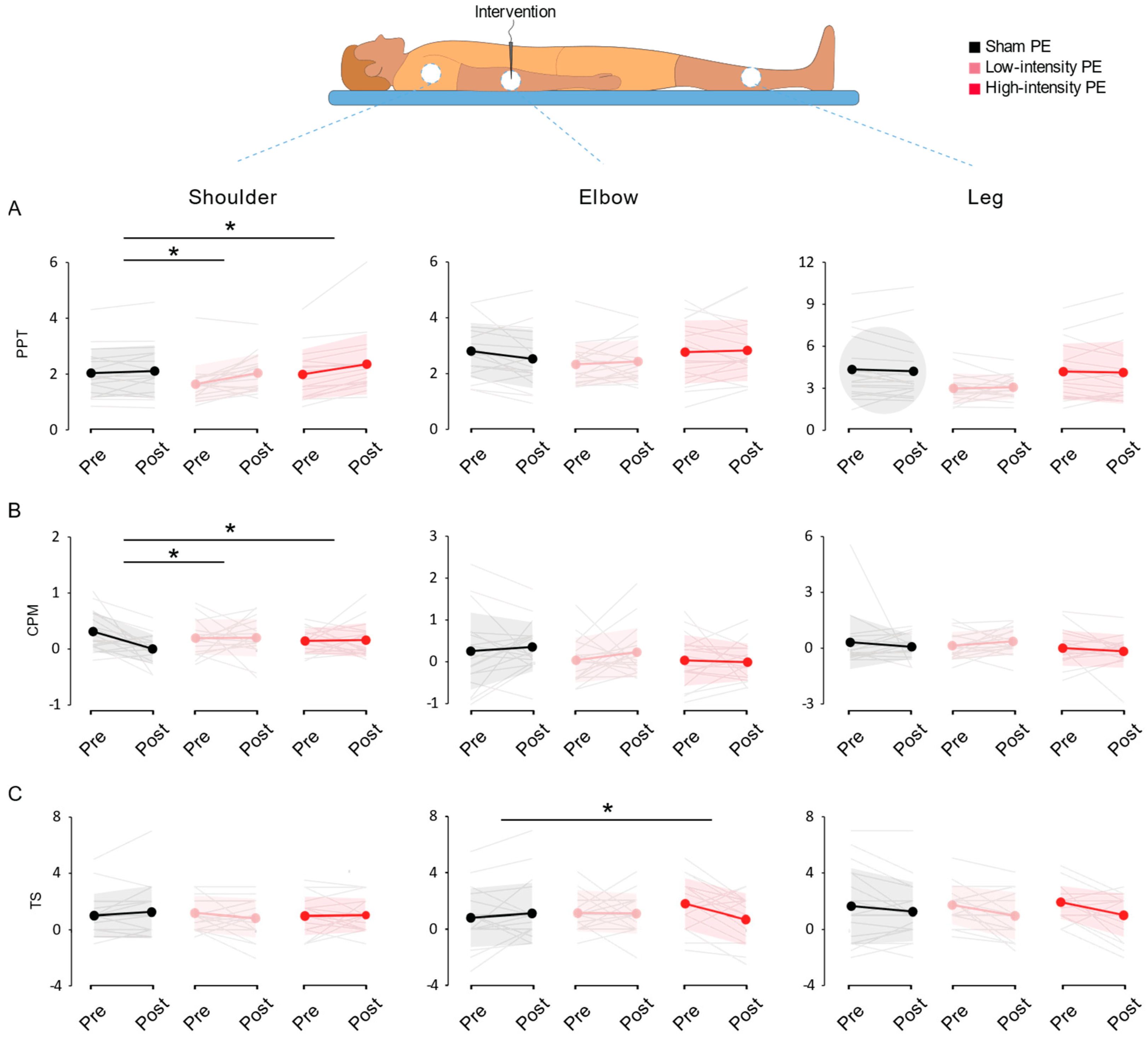
3.2. Widespread Sensitivity
3.3. Conditioned Pain Modulation
3.4. Temporal Summation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abat, F.; Sanchez-Sanchez, J.L.; Martin-Nogueras, A.M.; Calvo-Arenillas, J.I.; Yajeya, J.; Mendez-Sanchez, R.; Monllau, J.C.; Gelber, P.E. Randomized Controlled Trial Comparing the Effectiveness of the Ultrasound-Guided Galvanic Electrolysis Technique (USGET) Versus Conventional Electro-Physiotherapeutic Treatment on Patellar Tendinopathy. J. Exp. Orthop. 2016, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valera-Garrido, F.; Minaya-Muñoz, F. Electrólisis Percutánea Musculoesquelética. In Fisioterapia Invasiva; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, Spain, 2016; pp. 387–451. [Google Scholar]
- Moreno, C.; Mattiussi, G.; Núñez, F.J.; Messina, G.; Rejc, E. Intratissue Percutaneous Electolysis Combined with Active Physical Therapy for the Treatment of Adductor Longus Enthesopathy-Related Groin Pain: A Randomized Trial. J. Sports Med. Phys. Fitness 2017, 57, 1318–1329. [Google Scholar] [CrossRef] [PubMed]
- Abat, F.; Gelber, P.E.; Polidori, F.; Monllau, J.C.; Sanchez-Ibañez, J.M. Clinical Results After Ultrasound-Guided Intratissue Percutaneous Electrolysis (EPI®) And Eccentric Exercise In the Treatment Of Patellar Tendinopathy. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Abat, F.; Valles, S.L.; Gelber, P.E.; Polidori, F.; Stitik, T.P.; García-Herreros, S.; Monllau, J.C.; Sanchez-Ibánez, J.M. Mecanismos Moleculares De Reparación Mediante La Técnica Electrólisis Percutánea Intratisular En La Tendinosis Rotuliana. Rev. Esp. Cir. Ortop. Traumatol. 2014, 58, 201–205. [Google Scholar] [CrossRef]
- García-Naranjo, J.; Barroso-Rosa, S.; Loro-Ferrer, J.F.; Limiñana-Cañal, J.M.; Suarez-Hernández, E. A Novel Approach In the Treatment of Acute Whiplash Syndrome: Ultrasound-Guided Needle Percutaneous Electrolysis. A Randomized Controlled Trial. Orthop. Traumatol. Surg. Res. 2017, 103, 1229–1234. [Google Scholar] [CrossRef]
- Varela-Rodríguez, S.; Cáceres-Pajuelo, J.E.; Sánchez-Sánchez, J.L. Percutaneous Electrolysis In Patients with Musculoskeletal Disorders: A Systematic Review. J. Mol. Genet. Med. 2021, 15, 476. [Google Scholar]
- Gómez-Chiguano, G.F.; Navarro-Santana, M.J.; Cleland, J.A.; Arias-Buría, J.L.; Fernández-de-las-Peñas, C.; Ortega-Santiago, R.; Plaza-Manzano, G. Effectiveness of Ultrasound-Guided Percutaneous Electrolysis for Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Pain Med. 2021, 22, 1055–1071. [Google Scholar] [CrossRef]
- De-Miguel-Valtierra, L.; Salom-Moreno, J.; Fernández-de-las-Peñas, C.; Cleland, J.A.; Arias-Buría, J.L. Ultrasound-Guided Application of Percutaneous Electrolysis as An Adjunct to Exercise and Manual Therapy for Subacromial Pain Syndrome: A Randomized Clinical Trial. J. Pain 2018, 19, 1201–1210. [Google Scholar] [CrossRef]
- Arias-Buría, J.L.; Truyols-Domínguez, S.; Valero-Alcaide, R.; Salom-Moreno, J.; Atín-Arratibel, M.A.; Fernández-De-Las-Peñas, C. Ultrasound-Guided Percutaneous Electrolysis and Eccentric Exercises for Subacromial Pain Syndrome: A Randomized Clinical Trial. Evid. Based Complement. Altern. Med. 2015, 2015, 315219. [Google Scholar] [CrossRef]
- López-Martos, R.; González-Pérez, L.M.; Ruiz-Canela-Méndez, P.; Urresti-López, F.J.; Gutiérrez-Perez, J.L.; Infante-Cossio, P. Randomized, Double-Blind Study Comparing Percutaneous Electrolysis and Dry Needling for the Management Of Temporomandibular Myofascial Pain. Med. Oral Patol. Oral Y Cir. Bucal 2018, 23, e454–e462. [Google Scholar] [CrossRef]
- González-Pérez, L.M.; Canivell-Zabaleta, M.; Rodríguez-Posada, F.; Caro-Jiménez, M.J.; López-Martos, R.; Infante-Cossio, P.; Gutiérrez-Pérez, J.L. Study Comparing Intratissue Percutaneous Electrolysis, Deep Dry Needling and Botulinum Toxin for the Management of Temporomandibular Myofascial Pain. Int. J. Oral Maxillofac. Surg. 2019, 48, 280. [Google Scholar] [CrossRef]
- Rodríguez-Huguet, M.; Góngora-Rodríguez, J.; Lomas-Vega, R.; Martín-Valero, R.; Díaz-Fernández, Á.; Obrero-Gaitán, E.; Ibáñez-Vera, A.J.; Rodríguez-Almagro, D. Percutaneous Electrolysis in the Treatment of Lateral Epicondylalgia: A Single-Blind Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2068. [Google Scholar] [CrossRef] [PubMed]
- García-Bermejo, P.; De-La-Cruz-Torres, B.; Naranjo-Orellana, J.; Albornoz-Cabello, M. Autonomic Responses to Ultrasound-Guided Percutaneous Needle Electrolysis: Effect of Needle Puncture or Electrical Current? J. Altern. Complement. Med. 2018, 24, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Abat, F.; Diesel, W.-J.; Gelber, P.-E.; Polidori, F.; Monllau, J.-C.; Sanchez-Ibanez, J.-M. Effectiveness of the Intratissue Percutaneous Electrolysis (EPI®) Technique and Isoinertial Eccentric Exercise in the Treatment of Patellar Tendinopathy At Two Years Follow-Up. Muscles. Ligaments Tendons J. 2014, 4, 188–193. [Google Scholar] [CrossRef]
- Mattiussi, G.; Moreno, C. Treatment of Proximal Hamstring Tendinopathyrelated Sciatic Nerve Entrapment: Presentation of A n Ultrasound-Guided “Intratissue Percutaneous Electrolysis” Application. Muscles Ligaments Tendons J. 2016, 6, 248–252. [Google Scholar] [CrossRef]
- Rodríguez-Huguet, M.; Góngora-Rodríguez, J.; Rodríguez-Huguet, P.; Ibañez-Vera, A.J.; Rodríguez-Almagro, D.; Martín-Valero, R.; Díaz-Fernández, Á.; Lomas-Vega, R. Effectiveness of Percutaneous Electrolysis In Supraspinatus Tendinopathy: A Single-Blinded Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1837. [Google Scholar] [CrossRef]
- Abat, F.; Valles, S.-L.; Gelber, P.-E.; Polidori, F.; Jorda, A.; García-Herreros, S.; Monllau, J.-C.; Sanchez-Ibáñez, J.-M. An Experimental Study of Muscular Injury Repair In A Mouse Model Of Notexin-Induced Lesion with EPI® Technique. BMC Sports Sci. Med. Rehabil. 2015, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Sánchez, J.L.; Calderón-Díez, L.; Herrero-Turrión, J.; Méndez-Sánchez, R.; Arias-Buría, J.L.; Fernández-de-las-Peñas, C. Changes In Gene Expression Associated with Collagen Regeneration and Remodeling of Extracellular Matrix after Percutaneous Electrolysis on Collagenase-Induced Achilles Tendinopathy in an Experimental Animal Model: A Pilot Study. J. Clin. Med. 2020, 9, 3316. [Google Scholar] [CrossRef]
- Chou, L.W.; Kao, M.J.; Lin, J.G. Probable Mechanisms of Needling Therapies for Myofascial Pain Control. Evidence Based Complement. Altern. Med. 2012, 2012, 705327. [Google Scholar] [CrossRef]
- Cagnie, B.; Dewitte, V.; Barbe, T.; Timmermans, F.; Delrue, N.; Meeus, M. Physiologic Effects of Dry Needling. Curr. Pain Headache Rep. 2013, 17, 348. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Nijs, J. Trigger Point Dry Needling for the Treatment of Myofascial Pain Syndrome: Current Perspectives within A Pain Neuroscience Paradigm. J. Pain Res. 2019, 12, 1899–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butts, R.; Dunning, J.; Perreault, T.; Mourad, F.; Grubb, M. Peripheral And Spinal Mechanisms of Pain And Dry Needling Mediated Analgesia: A Clinical Resource Guide For Health Care Professionals. Am. J. Phys. Med. Rehabil. 2016, 4, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Lv, Q.; Wu, F.; Gan, X.; Yang, X.; Zhou, L.; Chen, J.; He, Y.; Zhang, R.; Zhu, B.; Liu, L. The Involvement of Descending Pain Inhibitory System in Electroacupuncture-Induced Analgesia. Front. Integr. Neurosci. 2019, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Moana-Filho, E.J.; Babiloni, A.H.; Theis-Mahon, N.R. Endogenous Pain Modulation In Chronic Orofacial Pain: A Systematic Review And Meta-Analysis. Pain 2018, 159, 1441–1455. [Google Scholar] [CrossRef]
- Staud, R. Abnormal Endogenous Pain Modulation Is A Shared Characteristic Of Many Chronic Pain Conditions. Expert Rev. Neurother. 2012, 12, 577–585. [Google Scholar] [CrossRef]
- Chen, Q.L.; Heinricher, M.M. Descending Control Mechanisms and Chronic Pain. Curr. Rheumatol. Rep. 2019, 21, 13. [Google Scholar] [CrossRef]
- De-La-Cruz-Torres, B.; Albornoz-Cabello, M.; García-Bermejo, P.; Naranjo-Orellana, J. Autonomic Responses To Ultrasoundguided Percutaneous Needle Electrolysis Of The Patellar Tendon In Healthy Male Footballers. Acupunct. Med. 2016, 34, 275–279. [Google Scholar] [CrossRef]
- García-Bermejo, P.; De-la-Cruz-Torres, B.; Naranjo-Orellana, J.; Albornoz-Cabello, M. Autonomic Activity In Women During Percutaneous Needle Electrolysis. Eur. J. Integr. Med. 2017, 11, 53–58. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, T.; Fernández-Rolle, Á.; Truyols-Domínguez, S.; Benítez-Martínez, J.C.; Casaña-Granell, J. Prospective Randomized Trial of Electrolysis for Chronic Plantar Heel Pain. Foot Ankle Int. Am. Orthop. Foot Ankle Soc. Swiss Foot Ankle Soc. 2018, 39, 1039–1046. [Google Scholar] [CrossRef]
- Bumgarner, J.R.; Walker, W.H., 2nd; Nelson, R.J. Circadian Rhythms And Pain. Neurosci. Biobehav. Rev. 2021, 129, 296–306. [Google Scholar] [CrossRef]
- Flood, A.; Waddington, G.; Cathcart, S. High-Definition Transcranial Direct Current Stimulation Enhances Conditioned Pain Modulation In Healthy Volunteers: A Randomized Trial. J. Pain 2016, 17, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Tobbackx, Y.; Meeus, M.; Wauters, L.; De Vilder, P.; Roose, J.; Verhaeghe, T.; Nijs, J. Does Acupuncture Activate Endogenous Analgesia In Chronic Whiplash-Associated Disorders? A Randomized Crossover Trial. Eur. J. Pain 2013, 17, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Nie, H.; Arendt-Nielsen, L.; Andersen, H.; Graven-Nielsen, T. Temporal Summation Of Pain Evoked By Mechanical Stimulation In Deep And Superficial Tissue. J. Pain 2005, 6, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Nir, R.R.; Yarnitsky, D. Conditioned Pain Modulation. Curr. Opin. Support. Palliat. Care 2015, 9, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Yarnitsky, D.; Bouhassira, D.; Drewes, A.M.; Fillingim, R.B.; Granot, M.; Hansson, P.; Landau, R.; Marchand, S.; Matre, D.; Nilsen, K.B.; et al. Recommendations On Practice Of Conditioned Pain Modulation (CPM) Testing. Eur. J. Pain 2015, 19, 805–806. [Google Scholar] [CrossRef] [PubMed]
- Meeus, M.; Hermans, L.; Ickmans, K.; Struyf, F.; Van Cauwenbergh, D.; Bronckaerts, L.; De Clerck, L.S.; Moorken, G.; Hans, G.; Grosemans, S.; et al. Endogenous Pain Modulation In Response To Exercise In Patients With Rheumatoid Arthritis, Patients With Chronic Fatigue Syndrome And Comorbid Fibromyalgia, And Healthy Controls: A Double-Blind Randomized Controlled Trial. Pain Pract. 2015, 15, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, S.L.; Jacques, A.; Leboeuf-Yde, C.; Etherington, S.J.; Walker, B.F. No Difference In Pressure Pain Threshold And Temporal Summation After Lumbar Spinal Manipulation Compared To Sham: A Randomised Controlled Trial In Adults With Low Back Pain. Musculoskelet. Sci. Pract. 2019, 43, 18–25. [Google Scholar] [CrossRef]
- Leite, P.M.S.; Mendonça, A.R.C.; Maciel, L.Y.S.; Poderoso-Neto, M.L.; Araujo, C.C.A.; Góis, H.C.J.; Souza, J.H.S.; DeSantana, J.M. Does Electroacupuncture Treatment Reduce Pain And Change Quantitative Sensory Testing Responses In Patients With Chronic Nonspecific Low Back Pain? A Randomized Controlled Clinical Trial. Evid. Based. Complement. Alternat. Med. 2018, 2018, 8586746. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical Power Analyses Using G*Power 3.1: Tests For Correlation And Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-T.; Hsieh, L.-F.; Kuan, T.-S.; Kao, M.-J.; Chou, L.-W.; Hong, C.-Z. Remote Effects Of Dry Needling On The Irritability Of The Myofascial Trigger Point In The Upper Trapezius Muscle. Am. J. Phys. Med. Rehabil. 2010, 89, 133–140. [Google Scholar] [CrossRef]
- Schliessbach, J.; van der Klift, E.; Siegenthaler, A.; Arendt-Nielsen, L.; Curatolo, M.; Streitberger, K. Does Acupuncture Needling Induce Analgesic Effects Comparable To Diffuse Noxious Inhibitory Controls? Evid. Based. Complement. Alternat. Med. 2012, 2012, 785613. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.T.; Shen, L.L.; Zhu, B.; Zhang, Z.Q.; Ma, C.Y.; Huang, G.F.; Yin, J.; Yu, L.L.; Yu, S.Y.; Ding, M.Q.; et al. Effects Of Intensity Of Electroacupuncture On Chronic Pain In Patients With Knee Osteoarthritis: A Randomized Controlled Trial. Arthritis Res. Ther. 2019, 21, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Feng, S.J.Q.; da Costa, C.; Li, C.G.; Lu, D.; Xue, C.C. Acupuncture Analgesia For Temporal Summation Of Experimental Pain: A Randomised Controlled Study. Eur. J. Pain 2010, 14, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Valera-Calero, J.A.; Sánchez-Mayoral-Martín, A.; Varol, U. Short-Term Effectiveness Of High- And Low-Intensity Percutaneous Electrolysis In Patients With Patellofemoral Pain Syndrome: A Pilot Study. World J. Orthop. 2021, 12, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Margalef, R.; Bosque, M.; Monclús, P.; Flores, P.; Minaya-Muñoz, F.; Valera-Garrido, F.; Santafé, M.M. Percutaneous Application of Galvanic Current in Rodents Reverses Signs of Myofascial Trigger Points. Evidence Based Complement. Altern. Med. 2020, 2020, 4173218. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 54) | Sham (n = 18) | Low-Intensity (n = 18) | High-Intensity (n = 18) | p |
|---|---|---|---|---|---|
| Demographic | |||||
| Age (years) | 22.96 (3.63) | 23.50 (3.09) | 23.33 (4.47) | 22.06 (3.19) | 0.26 |
| Weight (kg) | 67.17 (10.45) | 67.93 (11.38) | 66.66 (11.19) | 66.92 (9.22) | 0.55 |
| Height (m) | 1.73 (0.08) | 1.74 (0.07) | 1.76 (0.09) | 1.74 (0.95) | 0.75 |
| BMI (kg/m2) | 22.23 (2.21) | 22.31 (3.07) | 22.46 (1.92) | 21.91 (1.43) | 0.43 |
| IPAQ-SF (METs-min-week) | 2668 (2687) | 3249 (3446) | 2709 (2572) | 2045 (1804) | 0.54 |
| Gender (male) | 34 (63.0) | 12 (66.6) | 9 (50.0) | 13 (72.2) | 0.36 |
| Smoking (yes) | 8 (14.8) | 3 (16.7) | 2 (11.1) | 3 (16.7) | 0.86 |
| Baseline Outcomes | |||||
| PPT elbow (kg/cm2) | 2.62 (0.97) | 2.81 (0.96) | 2.32 (0.77) | 2.74 (1.12) | 0.30 |
| PPT shoulder (kg/cm2) | 1.88 (0.81) | 2.04 (0.86) | 1.62 (0.66) | 1.97 (0.88) | 0.18 |
| PPT leg (kg/cm2) | 3.82 (1.88) | 4.35 (2.20) | 2.96 (1.07) | 4.14 (1.96) | 0.08 |
| CPM elbow (kg/cm2) | 0.11 (0.69) | 0.26 (0.92) | 0.03 (0.51) | 0.03 (0.60) | 0.56 |
| CPM shoulder (kg/cm2) | 0.22 (0.30) | 0.31 (0.35) | 0.19 (0.30) | 0.15 (0.22) | 0.22 |
| CPM leg (kg/cm2) | 0.21 (0.30) | 0.32 (1.44) | 0.13 (0.72) | 0.01 (0.94) | 0.85 |
| TS elbow (0–10) | 1.23 (1.76) | 0.81 (2.07) | 1.11 (1.23) | 1.78 (1.82) | 0.24 |
| TS shoulder (0–10) | 1.04 (1.33) | 1.00 (1.53) | 1.17 (1.15) | 0.97 (1.36) | 0.82 |
| TS leg (0–10) | 1.75 (1.83) | 1.64 (2.69) | 1.69 (1.33) | 1.92 (1.15) | 0.89 |
| Measure | Group | Pre | Post | Intra-Group Differences | Between-Group Differences |
|---|---|---|---|---|---|
| Pressure Pain Threshold (PPT) | |||||
| PPT elbow (kg/cm2) | Sham | 2.81 (0.96) | 2.53 (1.05) | −0.28 (−0.58 to 0.03); d = 0.28 | Sham vs. Low −0.38 (−0.91 to 0.15); d = 0.60 |
| Low | 2.32 (0.77) | 2.42 (0.75) | 0.10 (−0.22 to 0.42); d = 0.13 | Sham vs. High −0.34 (−0.86 to 0.19); d = 0.52 | |
| High | 2.74 (1.12) | 2.80 (1.08) | 0.06 (−0.27 to 0.39); d = 0.05 | Low vs. High 0.04 (−0.49 to 0.57); d = 0.06 | |
| PPT shoulder (kg/cm2) | Sham | 2.04 (0.86) | 2.11 (0.67) | 0.07 (−0.08 to 0.23); d = 0.08 | Sham vs. Low −0.32 (−0.67 to 0.03); d = 0.74 * |
| Low | 1.62 (0.66) | 2.01 (0.67) | 0.39 (0.13 to 0.66); d = 0.59 ** | Sham vs. High −0.29 (−0.64 to 0.06); d = 0.80 * | |
| High | 1.97 (0.88) | 2.33 (1.08) | 0.36 (0.16 to 0.56); d = 0.37 ** | Low vs. High 0.03 (−0.32 to 0.38); d = 0.07 | |
| PPT leg (kg/cm2) | Sham | 4.35 (2.20) | 4.22 (2.20) | −0.13 (−0.50 to 0.24); d = 0.06 | Sham vs. Low −0.20 (−0.49 to 0.90); d = 0.25 |
| Low | 2.96 (1.07) | 3.03 (0.84) | 0.07 (−0.38 to 0.54); d = 0.08 | Sham vs. High −0.06 (−0.63 to 0.76); d = 0.09 | |
| High | 4.14 (1.96) | 4.07 (2.19) | −0.07 (−0.48 to 0.36); d = 0.03 | Low vs. High 0.14 (−0.56 to 0.83); d = 0.16 | |
| Conditioned Pain Modulation (CPM) | |||||
| CPM elbow (kg/cm2) | Sham | 0.25 (0.92) | 0.35 (0.59) | 0.10 (−0.29 to 0.49); d = 0.13 | Sham vs. Low −0.09 (−0.70 to 0.52); d = 0.12 |
| Low | 0.03 (0.51) | 0.22 (0.58) | 0.19 (−0.18 to 0.56); d = 0.35 | Sham vs. High 0.14 (−0.47 to 0.75); d = 0.19 | |
| High | 0.03 (0.60) | −0.01 (0.44) | −0.04 (−0.38 to 0.30); d = 0.08 | Low vs. High 0.23 (−0.38 to 0.84); d = 0.33 | |
| CPM shoulder (kg/cm2) | Sham | 0.31 (0.35) | 0.00 (0.26) | −0.31 (−0.52 to −0.10); d = 1.00 ** | Sham vs. Low −0.32 (−0.66 to 0.03) d = 0.72 * |
| Low | 0.19 (0.30) | 0.20 (0.33) | 0.01 (−0.22 to 0.24); d = 0.02 | Sham vs. High −0.32 (−0.67 to 0.02); d = 0.82 * | |
| High | 0.15 (0.22) | 0.16 (0.01) | 0.01 (−0.17 to 0.20); d = 0.05 | Low vs. High 0.00 (−0.35 to −0.34); d = 0.13 | |
| CPM leg (kg/cm2) | Sham | 0.32 (1.44) | 0.08 (0.64) | −0.24 (−1.10 to 0.61); d = 0.22 | Sham vs. Low −0.47 (−1.51 to 0.57); d = 0.35 |
| Low | 0.13 (0.72) | 0.36 (0.69) | 0.23 (−0.19 to 0.64); d = 0.32 | Sham vs. High −0.07 (−1.12 to 0.97); d = 0.05 | |
| High | 0.01 (0.94) | −0.16 (0.87) | −0.17 (−0.70 to 0.36); d = 0.19 | Low vs. High 0.40 (−0.65 to 1.44); d = 0.41 | |
| Temporal Summation (TS) | |||||
| TS elbow(0–10) | Sham | 0.81 (2.07) | 1.11 (2.17) | 0.30 (−0.48 to 1.09); d = 0.14 | Sham vs. Low 0.33 (−1.02 to 1.69); d = 0.21 |
| Low | 1.11 (1.23) | 1.08 (1.37) | −0.03 (−0.86 to 0.80); d = 0.02 | Sham vs. High 1.41 (0.06 to 2.77); d = 0.87 * | |
| High | 1.78 (1.82) | 0.67 (1.83) | −1.11 (−1.94 to −0.28); d = 0.61 * | Low vs. High 1.08 (−0.28 to −0.06); d = 0.65 | |
| TS shoulder (0–10) | Sham | 1.00 (1.53) | 1.25 (1.86) | 0.25 (−0.16 to 0.66); d = 0.15 | Sham vs. Low 0.61 (−0.37 to 1.59); d = 0.54 |
| Low | 1.17 (1.15) | 0.81 (1.35) | −0.36 (−1.05 to 0.33); d = 0.29 | Sham vs. High 0.19 (−0.78 to 1.17); d = 0.18 | |
| High | 0.97 (1.36) | 1.03 (1.17) | 0.06 (−0.58 to 0.69); d = 0.04 | Low vs. High −0.42 (−1.39 to 0.56); d = 0.31 | |
| TS leg(0–10) | Sham | 1.64 (2.69) | 1.25 (2.09) | −0.39 (−1.04 to 0.26); d = 0.16 | Sham vs. Low 0.36 (−0.79 to 1.51); d = 0.27 |
| Low | 1.69 (1.33) | 0.94 (1.65) | −0.75 (−1.44 to −0.06); d = 0.50 * | Sham vs. High 0.53 (−0.62 to 1.67); d = 0.38 | |
| High | 1.92 (1.15) | 1.00 (1.51) | −0.92 (−1.65 to −0.19); d = 0.68 * | Low vs. High 0.17 (−0.98 to 1.31); d = 0.12 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varela-Rodríguez, S.; Sánchez-Sánchez, J.L.; Velasco, E.; Delicado-Miralles, M.; Sánchez-González, J.L. Endogenous Pain Modulation in Response to a Single Session of Percutaneous Electrolysis in Healthy Population: A Double-Blinded Randomized Clinical Trial. J. Clin. Med. 2022, 11, 2889. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102889
Varela-Rodríguez S, Sánchez-Sánchez JL, Velasco E, Delicado-Miralles M, Sánchez-González JL. Endogenous Pain Modulation in Response to a Single Session of Percutaneous Electrolysis in Healthy Population: A Double-Blinded Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(10):2889. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102889
Chicago/Turabian StyleVarela-Rodríguez, Sergio, José Luis Sánchez-Sánchez, Enrique Velasco, Miguel Delicado-Miralles, and Juan Luis Sánchez-González. 2022. "Endogenous Pain Modulation in Response to a Single Session of Percutaneous Electrolysis in Healthy Population: A Double-Blinded Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 10: 2889. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102889