
Clinical Characteristics, Outcomes, and Risk Factors for Mortality in Patients with Stenotrophomonas maltophilia Bacteremia

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
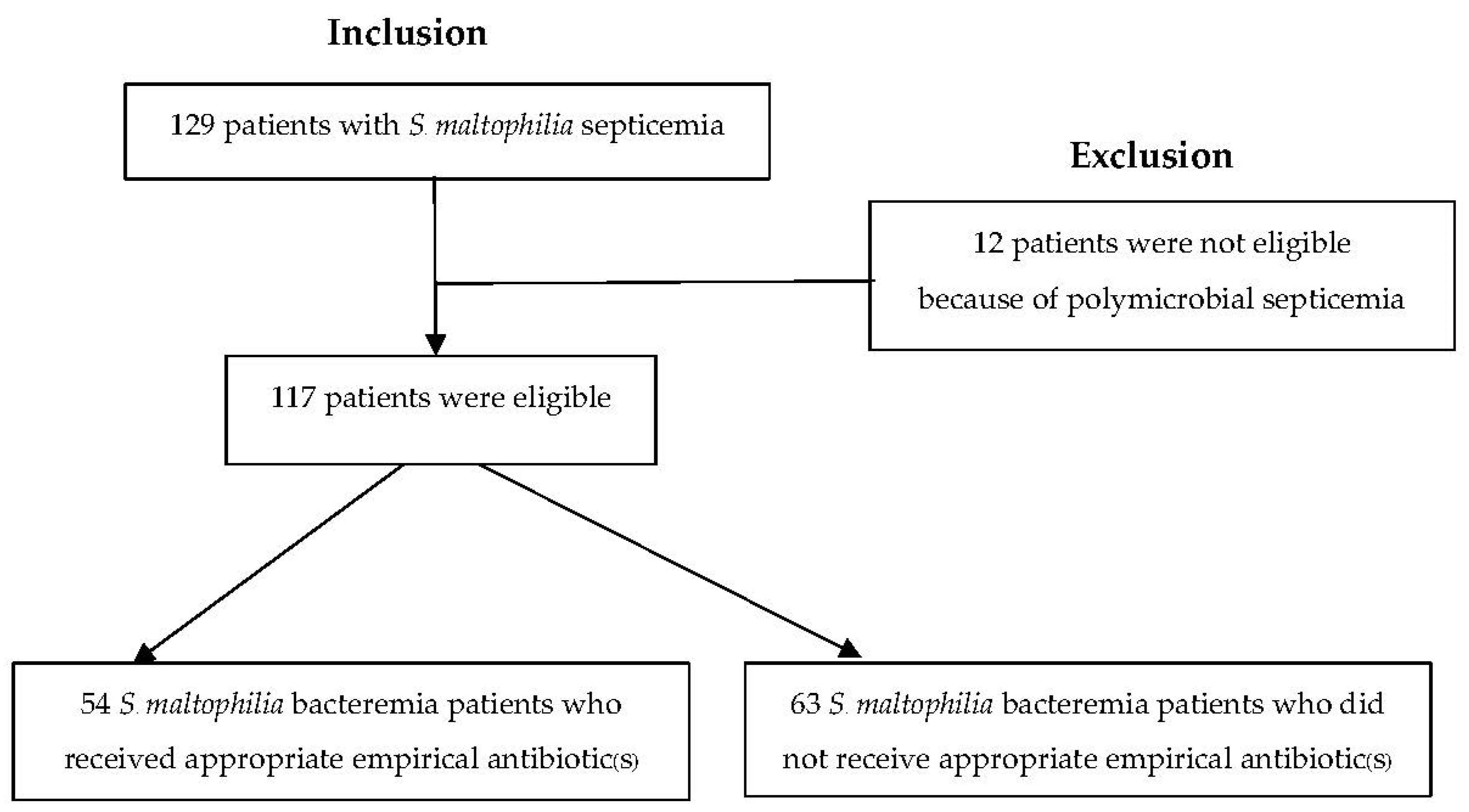
2.1. Patients and Setting
2.2. Bacterial Identification and Antimicrobial Susceptibility
2.3. Study Design and Data Collection
Data Retrieval
2.4. Statistical Analysis
2.5. Ethical Statement
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, Y.; Suo, J.; Du, M.; Chen, L.; Liu, Y.; Wang, L.; Liang, Z. Clinical features, outcomes, and risk factors of bloodstream infections due to Stenotrophomonas maltophilia in a tertiary-care hospital of China: A retrospective analysis. Biomed Res. Int. 2019, 2019, 4931501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looney, W.J.; Narita, M.; Mühlemann, K. Stenotrophomonas maltophilia: An emerging opportunist human pathogen. Lancet Infect. Dis. 2009, 9, 312–323. [Google Scholar] [CrossRef]
- Wang, W.-S.; Liu, C.-P.; Lee, C.-M.; Huang, F.-Y. Stenotrophomonas maltophilia bacteremia in adults: Four years’ experience in a medical center in northern Taiwan. J. Microbiol. Immunol. Infect. 2004, 37, 359–365. [Google Scholar] [PubMed]
- Victor, M.A.; Arpi, M.; Bruun, B.; Jønsson, V.; Hansen, M.M. Xanthomonas maltophilia bacteremia in immunocompromised hematological patients. Scand. J. Infect. Dis. 1994, 26, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Labarca, J.A.; Leber, A.L.; Kern, V.L.; Territo, M.C.; Brankovic, L.E.; Bruckner, D.A.; Pegues, D.A. Outbreak of Stenotrophomonas maltophilia bacteremia in allogenic bone marrow transplant patients: Role of severe neutropenia and mucositis. Clin. Infect. Dis. 2000, 30, 195–197. [Google Scholar] [CrossRef] [Green Version]
- Micozzi, A.; Venditti, M.; Monaco, M.; Friedrich, A.; Taglietti, F.; Santilli, S.; Martino, P. Bacteremia due to Stenotrophomonas maltophilia in patients with hematologic malignancies. Clin. Infect. Dis. 2000, 31, 705–711. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kastoris, A.C.; Vouloumanou, E.K.; Rafailidis, P.I.; Kapaskelis, A.M.; Dimopoulos, G. Attributable mortality of Stenotrophomonas maltophilia infections: A systematic review of the literature. Future Microbiol. 2009, 4, 1103–1109. [Google Scholar] [CrossRef]
- Demiraslan, H.; Sevim, M.; Pala, Ç.; Durmaz, S.; Berk, V.; Kaynar, L.; Metan, G. Risk factors influencing mortality related to Stenotrophomonas maltophilia infection in hematology–oncology patients. Int. J. Hematol. 2013, 97, 414–420. [Google Scholar] [CrossRef]
- Garcia Paez, J.; Tengan, F.; Barone, A.; Levin, A.; Costa, S. Factors associated with mortality in patients with bloodstream infection and pneumonia due to Stenotrophomonas maltophilia. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 901–906. [Google Scholar] [CrossRef]
- Alonso, A.; Martinez, J.L. Multiple antibiotic resistance in Stenotrophomonas maltophilia. Antimicrob. Agents Chemother. 1997, 41, 1140–1142. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Li, X.-Z.; Poole, K. Multiple antibiotic resistance in Stenotrophomonas maltophilia: Involvement of a multidrug efflux system. Antimicrob. Agents Chemother. 2000, 44, 287–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Insuwanno, W.; Kiratisin, P.; Jitmuang, A. Stenotrophomonas maltophilia infections: Clinical characteristics and factors associated with mortality of hospitalized patients. Infect. Drug Resist. 2020, 13, 1559. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kang, C.-I.; Kim, J.; Ha, Y.E.; Chung, D.R.; Lee, N.Y.; Peck, K.R.; Song, J.-H. Can levofloxacin be a useful alternative to trimethoprim-sulfamethoxazole for treating Stenotrophomonas maltophilia bacteremia? Antimicrob. Agents Chemother. 2014, 58, 581–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.-S.; Hong, S.G.; Kim, Y.R.; Shin, K.S.; Whang, D.H.; Ahn, J.Y.; Park, Y.-J.; Uh, Y.; Chang, C.L.; Shin, J.H. Antimicrobial susceptibility of Stenotrophomonas maltophilia isolates from Korea, and the activity of antimicrobial combinations against the isolates. J. Korean Med. Sci. 2013, 28, 62–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.T.; Lin, C.Y.; Lu, P.L.; Lai, C.C.; Chen, T.C.; Chen, C.Y.; Wu, D.C.; Wang, T.P.; Lin, C.M.; Lin, W.R. Stenotrophomonas maltophilia bloodstream infection: Comparison between community-onset and hospital-acquired infections. J. Microbiol. Immunol. Infect. 2014, 47, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.L.; Scipione, M.R.; Dubrovskaya, Y.; Papadopoulos, J. Monotherapy with fluoroquinolone or trimethoprim-sulfamethoxazole for treatment of Stenotrophomonas maltophilia infections. Antimicrob. Agents Chemother. 2014, 58, 176–182. [Google Scholar] [CrossRef] [Green Version]
- Bonfiglio, G.; Cascone, C.; Azzarelli, C.; Cafiso, V.; Marchetti, F.; Stefani, S. Levofloxacin in vitro activity and time–kill evaluation of Stenotrophomonas maltophilia clinical isolates. J. Antimicrob. Chemother. 2000, 45, 115–117. [Google Scholar] [CrossRef]
- Paez, J.G.; Costa, S. Risk factors associated with mortality of infections caused by Stenotrophomonas maltophilia: A systematic review. J. Hosp. Infect. 2008, 70, 101–108. [Google Scholar] [CrossRef]
- Xun, M.; Zhang, Y.; Li, B.-L.; Wu, M.; Zong, Y.; Yin, Y.-M. Clinical characteristics and risk factors of infections caused by Stenotrophomonas maltophilia in a hospital in northwest China. J. Infect. Dev. Ctries. 2014, 8, 1000–1005. [Google Scholar] [CrossRef] [Green Version]
- Jeon, Y.D.; Jeong, W.Y.; Kim, M.H.; Jung, I.Y.; Ahn, M.Y.; Ann, H.W.; Ahn, J.Y.; Han, S.H.; Choi, J.Y.; Song, Y.G. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia. Medicine 2016, 95, e4375. [Google Scholar] [CrossRef]
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Disk Susceptibility Tests. In CLSI Standard MO2, 13th ed.; Clinical and Laboratory Standards Institute: Malvern, PA, USA, 2018. [Google Scholar]
- National Committee for Clinical Laboratory Standards. MD2 Disk Diffusion Reading Guide. In CLSI Quick Guide MO2QG, 1st ed.; Clinical and Laboratory Standards Institute: Malvern, PA, USA, 2018. [Google Scholar]
- Matuschek, E.; Ahman, J.; Webster, C.; Kahlmeter, G. Antimicrobial susceptibility testing of colistin-evaluation of seven commercial MIC products against standard broth microdilution for Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter spp. Clin. Microbiol. Infect. 2018, 24, 865–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of AmpC β-Lactamaseproducing Enterobacterales, Carbapenem-Resistant Acinetobacter Baumannii, and Stenotrophomonas Maltophilia Infections. Version 2.0. Available online: https://www.idsociety.org/practice-guideline/amr-guidance-2.0/ (accessed on 16 May 2022).
- Ontong, J.C.; Ozioma, N.F.; Voravuthikunchai, S.P.; Chusri, S. Synergistic antibacterial effects of colistin in combination with aminoglycoside, carbapenems, cephalosporins, fluoroquinolones, tetracyclines, fosfomycin, and piperacillin on multidrug resistant Klebsiella pneumoniae isolates. PLoS ONE 2021, 16, e0244673. [Google Scholar]
- Del Toro, M.D.; Rodriguez-Bano, J.; Herrero, M.; Rivero, A.; Garcia-Ordonez, M.A.; Corzo, J.; Perez-Cano, R. Clinical epidemiology of Stenotrophomonas maltophilia colonization and infection: A multicenter study. Medicine 2002, 81, 228–239. [Google Scholar] [CrossRef]
- Aisenberg, G.; Rolston, K.; Dickey, B.; Kontoyiannis, D.; Raad, I.; Safdar, A. Stenotrophomonas maltophilia pneumonia in cancer patients without traditional risk factors for infection, 1997–2004. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 13–20. [Google Scholar] [CrossRef]
- Friedman, N.; Korman, T.; Fairley, C.; Franklin, J.; Spelman, D. Bacteraemia due to Stenotrophomonas maltophilia: An analysis of 45 episodes. J. Infect. 2002, 45, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Samonis, G.; Karageorgopoulos, D.E.; Maraki, S.; Levis, P.; Dimopoulou, D.; Spernovasilis, N.A.; Kofteridis, D.P.; Falagas, M.E. Stenotrophomonas maltophilia infections in a general hospital: Patient characteristics, antimicrobial susceptibility, and treatment outcome. PLoS ONE 2012, 7, e37375. [Google Scholar] [CrossRef]
- Kilic, A.U.; Unuvar, G.K.; Cevahir, F.; Alp, E. Economic Burden of Multidrug-Resistant Gram-Negative Infections in a Developing Country. Erciyes Med. J. 2019, 41, 312–316. [Google Scholar]



{kind=link}
{kind=link}
| Parameter | S. maltophilia Bacteremia Patients (n = 117) | S. maltophilia Bacteremia Patients Receiving Appropriate Empirical Antibiotics (n = 54) | S. maltophilia Bacteremia Patients Not Receiving Appropriate Empirical Antibiotics (n = 63) | p-Value A |
|---|---|---|---|---|
| Demographics | ||||
| Age, median (IQR) | 45 (40, 51) | 45 (36, 51) | 45 (41, 51) | 0.974 |
| Male sex | 77 (70) | 40 (74) | 37 (59) | 0.121 |
| Comorbidities | 105 (90) | 51 (94) | 54 (86) | 0.213 |
| Immunocompromised status | 6 (5) | 3 (6) | 3 (5) | 0.997 |
| Obesity | 83 (70) | 36 (67) | 47 (75) | 0.460 |
| Previous exposure to antibiotics | ||||
| Carbapenem | 112 (96) | 50 (93) | 62 (98) | 0.158 |
| Cephalosporin | 85 (73) | 41 (76) | 44 (69) | 0.462 |
| Fluoroquinolone | 72 (62) | 32 (59) | 40 (63) | 0.639 |
| β-lactam/β-lactamase inhibitor | 69 (59) | 36 (67) | 33 (52) | 0.119 |
| Aminoglycoside | 40 (34) | 18 (33) | 22 (35) | 0.857 |
| Clinical characteristics | ||||
| Initial ICU admission | 54 (46) | 32 (59) | 22 (35) | 0.014 |
| APACHE II score, median (IQR) | 19 (15, 23) | 20 (13, 22) | 16 (14, 18) | 0.021 |
| Pneumonia | 55 (47) | 26 (48) | 29 (46) | 0.966 |
| Invasive medical devices | ||||
| Mechanical ventilator | 95 (81) | 48 (89) | 47 (74) | 0.054 |
| Intra-vascular device | 73 (62) | 39 (72) | 34 (54) | 0.044 |
| Urinary catheterization | 101 (86) | 52 (96) | 49 (78) | 0.008 |
| Treatment Empirical treatment including | ||||
| Carbapenem(s) | 110 (94) | 50 (93) | 60 (94) | 0.551 |
| Colistin | 40 (34) | 30 (56) | 10 (15) | <0.001 |
| TMP-SMX | 30 (25) | 30 (56) | 0 (0) | <0.001 |
| Fluoroquinolone(s) | 31 (26) | 28 (52) | 3 (5) | <0.001 |
| Duration of empirical treatment | 3 (3, 4) | 3 (3, 4) | 3 (3, 4) | 0.996 |
| Antibiotics | No. of Resistant Isolates (%) |
|---|---|
| Chloramphenicol | 21 (18) |
| Colistin | 41 (35) |
| Levofloxacin | 14 (12) |
| TMP-SMX | 8 (7) |
| Ceftazidime | 76 (65) |
| Outcomes | S. maltophilia Bacteremia Patients Who Received Appropriate Empirical Antibiotic(s) (n = 54) | S. maltophilia Bacteremia Patients Who Did Not Receive Appropriate Empirical Antibiotic(s) (n = 63) | p-Value A |
|---|---|---|---|
| Clinical outcomes | |||
| Mortality | |||
| 14-day | 4 (7) | 21 (33) | 0.001 |
| 30-day | 4 (7) | 30 (48) | <0.001 |
| In-hospital | 5 (9) | 32 (51) | <0.001 |
| Non-clinical outcomes | |||
| Length of hospital stay (days) [median (IQR)] | 21 (15, 31) | 34 (29, 50) | <0.001 |
| Cost (baht) [median(IQR)] | |||
| Total hospital | 142,463 (125,008–212,389) | 185,663 (159,223–200,685) | 0.002 |
| Antimicrobial | 30,854 (26,447–33,321) | 31,854 (29,606–34,014) | 0.031 |
| Non-antimicrobial | 118,007 (97,245–175,004) | 146,897 (131,488–190,884) | <0.001 |
| Variables | Values | Crude OR (95% CI) | Adjusted OR (95% CI) | p-Value A | |
|---|---|---|---|---|---|
| Survivors (n = 83) | Non-Survivors (n = 34) | ||||
| Age (years) [median (IQR)] | 45 (42, 67) | 47 (36, 73) | 1.01 (0.99, 1.03) | 1.01 (0.96, 1.02) | 0.386 |
| Male sex | 57 (69) | 20 (59) | 0.65 (0.28, 1.49) | 0.53 (0.25, 2.15) | 0.567 |
| Underlying disease(s) | 76 (92) | 29 (85) | 0.53 (0.16, 1.81) | 0.3 (0.10, 1.05) | 0.615 |
| Immunocompromised status | 5 (6) | 1 (3) | 0.45 (0.05, 4.12) | 0.41 (0.08, 3.71) | 0.738 |
| Obesity | 58 (70) | 25 (74) | 1.19 (0.49, 2.04) | 1.06 (0.35, 2.00) | 0.905 |
| APACHE II score [median (IQR)] | 16 (13, 21) | 18 (15, 21) | 1.05 (1.01, 1.15) | 1.19 (1.04, 1.35) | 0.012 |
| Pneumonia | 40 (48) | 15 (44) | 0.84 (0.53, 2.63) | 0.72 (0.50, 2.46) | 0.546 |
| Initial intensive care unit admission | 38 (46) | 16 (47) | 1.05 (0.47, 2.32) | 1.03 (0.25, 1.54) | 0.131 |
| Appropriate empirical antibiotic(s) | 50 (60) | 4 (12) | 0.09 (0.03, 0.27) | 0.04 (0.01, 0.16) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanchanasuwan, S.; Rongmuang, J.; Siripaitoon, P.; Kositpantawong, N.; Charoenmak, B.; Hortiwakul, T.; Nwabor, O.F.; Chusri, S. Clinical Characteristics, Outcomes, and Risk Factors for Mortality in Patients with Stenotrophomonas maltophilia Bacteremia. J. Clin. Med. 2022, 11, 3085. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11113085
Kanchanasuwan S, Rongmuang J, Siripaitoon P, Kositpantawong N, Charoenmak B, Hortiwakul T, Nwabor OF, Chusri S. Clinical Characteristics, Outcomes, and Risk Factors for Mortality in Patients with Stenotrophomonas maltophilia Bacteremia. Journal of Clinical Medicine. 2022; 11(11):3085. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11113085
Chicago/Turabian StyleKanchanasuwan, Siripen, Jakkapan Rongmuang, Pisud Siripaitoon, Narongdet Kositpantawong, Boonsri Charoenmak, Thanaporn Hortiwakul, Ozioma Forstinus Nwabor, and Sarunyou Chusri. 2022. "Clinical Characteristics, Outcomes, and Risk Factors for Mortality in Patients with Stenotrophomonas maltophilia Bacteremia" Journal of Clinical Medicine 11, no. 11: 3085. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11113085