
Mechanical Fatigue Performance of Patient-Specific Polymer Plates in Oncologic Mandible Reconstruction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Test Specimens
2.2. Plates and Screws
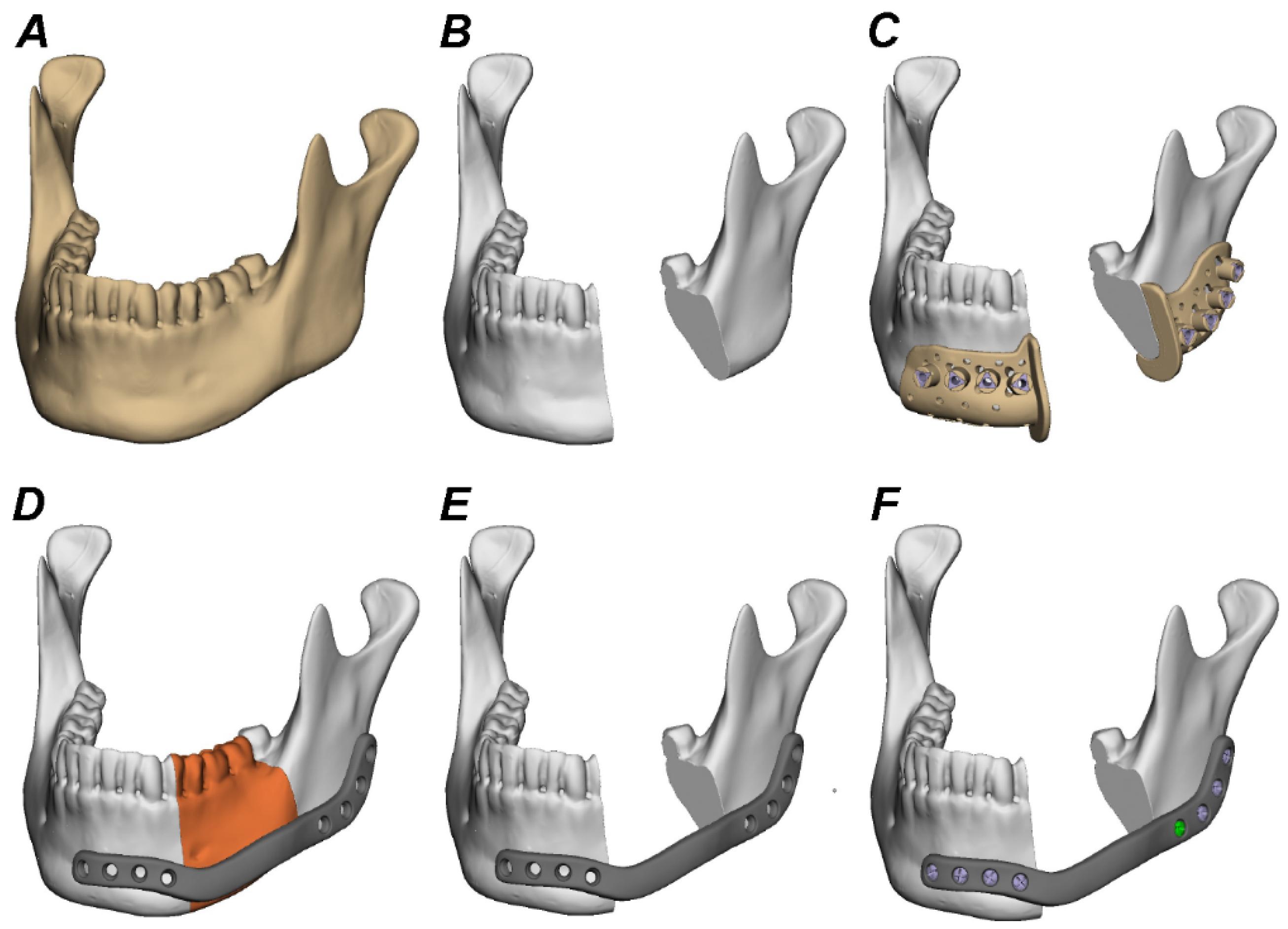
2.3. Virtual Planning, Shaping, and Manufacturing of Reconstruction Plates
2.4. Plate Fixation to Test Specimens
2.5. Mechanical Testing
2.6. Statistical Analysis
3. Results
3.1. Fatigue Test
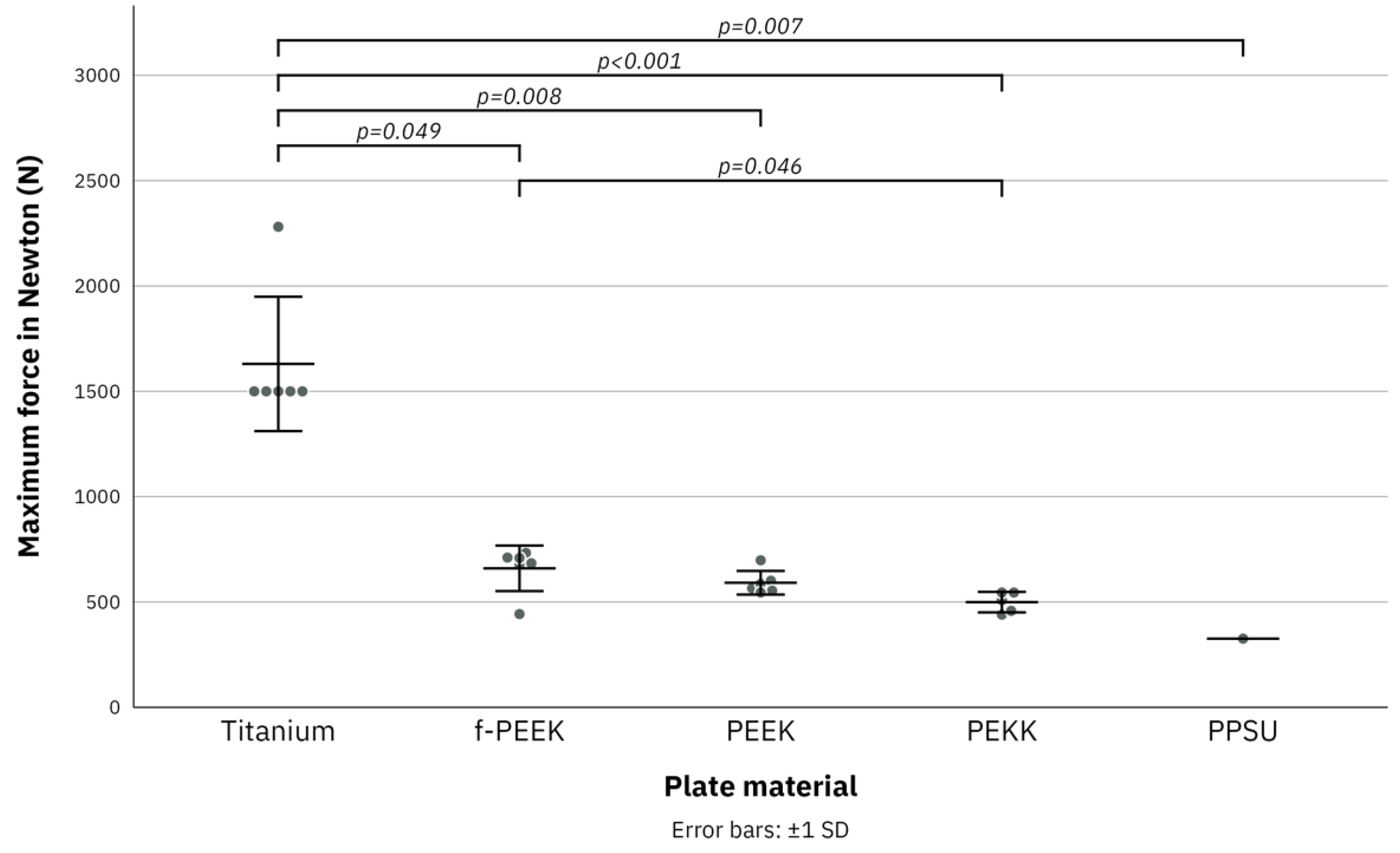
3.2. Load to Failure Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sproll, C.K.; Holtmann, H.; Schorn, L.K.; Jansen, T.M.; Reifenberger, J.; Boeck, I.; Rana, M.; Kübler, N.R.; Lommen, J. Mandible handling in the surgical treatment of oral squamous cell carcinoma: Lessons from clinical results after marginal and segmental mandibulectomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Möllmann, H.L.; Apeltrath, L.; Karnatz, N.; Wilkat, M.; Riedel, E.; Singh, D.D.; Rana, M. Comparison of the Accuracy and Clinical Parameters of Patient-Specific and Conventionally Bended Plates for Mandibular Reconstruction. Front. Oncol. 2021, 11, 719028. [Google Scholar] [CrossRef] [PubMed]
- Vignesh, U.; Mehrotra, D.; Howlader, D.; Singh, P.K.; Gupta, S. Patient Specific Three-Dimensional Implant for Reconstruction of Complex Mandibular Defect. J. Craniofacial Surg. 2019, 30, e308–e311. [Google Scholar]
- Toto, J.M.; Chang, E.I.; Agag, R.; Devarajan, K.; Patel, S.A.; Topham, N.S. Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck 2015, 37, 1660–1664. [Google Scholar] [CrossRef] [PubMed]
- Lommen, J.; Schorn, L.; Sproll, C.; Haussmann, J.; Kübler, N.R.; Budach, W.; Rana, M.; Tamaskovics, B. Reduction of CT Artifacts Using Polyetheretherketone (PEEK), Polyetherketoneketone (PEKK), Polyphenylsulfone (PPSU), and Polyethylene (PE) Reconstruction Plates in Oral Oncology. J. Oral Maxillofac. Surg. 2022, in press. [Google Scholar] [CrossRef]
- Bojechko, C.; Hua, P.; Sumner, W.; Guram, K.; Atwood, T.; Sharabi, A. Adaptive replanning using cone beam CT for deformation of original CT simulation. J. Med. Radiat. Sci. 2021, 69, 267–272. [Google Scholar] [CrossRef]
- Friedrich, R.E.; Todorovic, M.; Heiland, M.; Scheuer, H.A.; Krüll, A. Scattering effects of irradiation on surroundings calculated for a small dental implant. Anticancer Res. 2012, 32, 2043–2046. [Google Scholar]
- Maurer, P.; Pistner, H.; Schubert, J. Computer assisted chewing power in patients with segmental resection of the mandible. Mund Kiefer Gesichtschir. 2006, 10, 37–41. [Google Scholar] [CrossRef]
- Rendenbach, C.; Steffen, C.; Sellenschloh, K.; Heyland, M.; Morlock, M.M.; Toivonen, J.; Moritz, N.; Smeets, R.; Heiland, M.; Vallittu, P.K.; et al. Patient specific glass fiber reinforced composite versus titanium plate: A comparative biomechanical analysis under cyclic dynamic loading. J. Mech. Behav. Biomed. Mater. 2019, 91, 212–219. [Google Scholar] [CrossRef]
- Zhang, J.; Tian, W.; Chen, J.; Yu, J.; Zhang, J.; Chen, J. The application of polyetheretherketone (PEEK) implants in cranioplasty. Brain Res. Bull. 2019, 153, 143–149. [Google Scholar] [CrossRef]
- Panayotov, I.V.; Orti, V.; Cuisinier, F.; Yachouh, J. Polyetheretherketone (PEEK) for medical applications. J. Mater. Sci. Mater. Med. 2016, 27, 118. [Google Scholar] [CrossRef] [PubMed]
- Alqurashi, H.; Khurshid, Z.; Syed, A.U.Y.; Rashid Habib, S.; Rokaya, D.; Zafar, M.S. Polyetherketoneketone (PEKK): An emerging biomaterial for oral implants and dental prostheses. J. Adv. Res. 2021, 28, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Díez-Pascual, A.M.; Díez-Vicente, A.L. Effect of TiO(2) nanoparticles on the performance of polyphenylsulfone biomaterial for orthopaedic implants. J. Mater. Chem. B 2014, 2, 7502–7514. [Google Scholar] [CrossRef] [PubMed]
- Rendenbach, C.; Sellenschloh, K.; Gerbig, L.; Morlock, M.M.; Beck-Broichsitter, B.; Smeets, R.; Heiland, M.; Huber, G.; Hanken, H. CAD-CAM plates versus conventional fixation plates for primary mandibular reconstruction: A biomechanical in vitro analysis. J. Craniomaxillofac. Surg. 2017, 45, 1878–1883. [Google Scholar] [CrossRef]
- Steiner, T.; Raith, S.; Scherer, E.; Mücke, T.; Torsiglieri, T.; Rohleder, N.H.; Eder, M.; Grohmann, I.; Kesting, M.; Bier, H.; et al. Which kind of frontal mandibulotomy is the smartest? A biomechanical study. J. Craniomaxillofac. Surg. 2015, 43, 199–203. [Google Scholar] [CrossRef]
- Schupp, W.; Arzdorf, M.; Linke, B.; Gutwald, R. Biomechanical testing of different osteosynthesis systems for segmental resection of the mandible. J. Oral Maxillofac. Surg. 2007, 65, 924–930. [Google Scholar] [CrossRef]
- Slagter, A.P.; Bosman, F.; van der Glas, H.W.; van der Bilt, A. Human jaw-elevator muscle activity and food comminution in the dentate and edentulous state. Arch. Oral Biol. 1993, 38, 195–205. [Google Scholar] [CrossRef]
- Nicolini, L.F.; Kobbe, P.; Seggewiß, J.; Greven, J.; Ribeiro, M.; Beckmann, A.; Da Paz, S.; Eschweiler, J.; Prescher, A.; Markert, B.; et al. Motion preservation surgery for scoliosis with a vertebral body tethering system: A biomechanical study. Eur. Spine J. 2022, 31, 1013–1021. [Google Scholar] [CrossRef]
- Brandes, L.L.; Nicolini, L.F.; Greven, J.; Lichte, P.; Stopinski, T.T.; Sattler, M.; Hildebrand, F.; Pishnamaz, M. Biomechanical Performance of BoneHelix(®) Compared with Elastic Stable Intramedullary Nailing (ESIN) in a Pediatric Tibia Fracture Model. Life 2021, 11, 1189. [Google Scholar] [CrossRef]
- Radzi, S.; Cowin, G.; Robinson, M.; Pratap, J.; Volp, A.; Schuetz, M.A.; Schmutz, B. Metal artifacts from titanium and steel screws in CT, 1.5T and 3T MR images of the tibial Pilon: A quantitative assessment in 3D. Quant. Imaging Med. Surg. 2014, 4, 163–172. [Google Scholar]
- Kovacs, D.G.; Rechner, L.A.; Appelt, A.L.; Berthelsen, A.K.; Costa, J.C.; Friborg, J.; Persson, G.F.; Bangsgaard, J.P.; Specht, L.; Aznar, M.C. Metal artefact reduction for accurate tumour delineation in radiotherapy. Radiother. Oncol. 2018, 126, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Tao, S.; Tan, J.; Hu, X.; Liu, H.; Li, Z. Long-term follow-up of fibular graft for the reconstruction of bone defects. Medicine 2018, 97, e12605. [Google Scholar] [CrossRef] [PubMed]
- Bates, J.F.; Stafford, G.D.; Harrison, A. Masticatory function-a review of the literature: (II) Speed of movement of the mandible, rate of chewing and forces developed in chewing. J. Oral Rehabil. 1975, 2, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Takaki, P.; Vieira, M.; Bommarito, S. Maximum bite force analysis in different age groups. Int. Arch. Otorhinolaryngol. 2014, 18, 272–276. [Google Scholar] [PubMed] [Green Version]
- Franco, R.; de Matos, L.L.; Kulcsar, M.A.V.; de Castro-Júnior, G.; Marta, G.N. Influence of time between surgery and postoperative radiation therapy and total treatment time in locoregional control of patients with head and neck cancer: A single center experience. Clinics 2020, 75, e1615. [Google Scholar] [CrossRef]
- Henschel, J.; Tsai, S.; Fitzpatrick, D.C.; Marsh, J.L.; Madey, S.M.; Bottlang, M. Comparison of 4 Methods for Dynamization of Locking Plates: Differences in the Amount and Type of Fracture Motion. J. Orthop. Trauma 2017, 31, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Trainotti, S.; Raith, S.; Kesting, M.; Eichhorn, S.; Bauer, F.; Kolk, A.; Lethaus, B.; Hölzle, F.; Steiner, T. Locking versus nonlocking plates in mandibular reconstruction with fibular graft--a biomechanical ex vivo study. Clin. Oral Investig. 2014, 18, 1291–1298. [Google Scholar] [CrossRef]
- Park, S.M.; Lee, J.W.; Noh, G. Which plate results in better stability after segmental mandibular resection and fibula free flap reconstruction? Biomechanical analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 380–389. [Google Scholar] [CrossRef]
- Brown, J.S.; Lowe, D.; Kanatas, A.; Schache, A. Mandibular reconstruction with vascularised bone flaps: A systematic review over 25 years. Br. J. Oral Maxillofac. Surg. 2017, 55, 113–126. [Google Scholar] [CrossRef]
- Okuyama, K.; Michi, Y.; Mizutani, M.; Yamashiro, M.; Kaida, A.; Harada, K. Clinical study on mandibular fracture after marginal resection of the mandible. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 461–467. [Google Scholar] [CrossRef]
- Vallittu, P.K.; Närhi, T.O.; Hupa, L. Fiber glass-bioactive glass composite for bone replacing and bone anchoring implants. Dent. Mater. 2015, 31, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Seto, I.; Marukawa, E.; Asahina, I. Mandibular reconstruction using a combination graft of rhBMP-2 with bone marrow cells expanded in vitro. Plast. Reconstr. Surg. 2006, 117, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Boyne, P.J. Reconstruction of mandibular continuity defects with bone morphogenetic protein-2 (rhBMP-2). J. Oral Maxillofac. Surg. 2008, 66, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Lommen, J.; Schorn, L.; Landers, A.; Holtmann, H.; Berr, K.; Kübler, N.R.; Sproll, C.; Rana, M.; Depprich, R. Release kinetics of the model protein FITC-BSA from different polymer-coated bovine bone substitutes. Head Face Med. 2019, 15, 27. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Screw Type | Position | Screw Length (mm) |
|---|---|---|
| Ø 2.7 mm, locking (bicortical) | 1 | 17 |
| Ø 2.7 mm, locking (bicortical) | 2 | 17 |
| Ø 2.7 mm, locking (bicortical) | 3 | 15 |
| Ø 2.7 mm, locking (bicortical) | 4 | 17 |
| Ø 2.7 mm, locking (bicortical) | 5 | 13 |
| Ø 2.7 mm, locking (bicortical) | 6 | 11 |
| Ø 2.7 mm, locking (bicortical) | 7 | 11 |
| Ø 2.7 mm, locking (bicortical) | 8 | 9 |
| Plate Number | Plate Material | Number of Cycles | Plate Failure | Screw Failure |
|---|---|---|---|---|
| 1 | Titanium | 250,000 | No | No |
| 2 | Titanium | 250,000 | No | No |
| 3 | Titanium | 250,000 | No | No |
| 4 | Titanium | 250,000 | No | No |
| 5 | Titanium | 250,000 | No | No |
| 6 | Titanium | 250,000 | No | No |
| 1 | f-PEEK | 250,000 | No | No |
| 2 | f-PEEK | 250,000 | No | No |
| 3 | f-PEEK | 250,000 | No | No |
| 4 | f-PEEK | 250,000 | No | No |
| 5 | f-PEEK | 250,000 | No | No |
| 6 | f-PEEK | 250,000 | No | No |
| 1 | PEEK | 250,000 | No | No |
| 2 | PEEK | 250,000 | No | No |
| 3 | PEEK | 250,000 | No | No |
| 4 | PEEK | 250,000 | No | No |
| 5 | PEEK | 250,000 | No | No |
| 6 | PEEK | 250,000 | No | No |
| 1 | PEKK | 250,000 | No | No |
| 2 | PEKK | 25,701 | Yes | No |
| 3 | PEKK | 250,000 | No | No |
| 4 | PEKK | 250,000 | No | No |
| 5 | PEKK | 250,000 | No | No |
| 6 | PEKK | 250,000 | No | No |
| 1 | PPSU | 285 | Yes | No |
| 2 | PPSU | 6 | Yes | No |
| 3 | PPSU | 19,011 | Yes | No |
| 4 | PPSU | 63,075 | Yes | No |
| 5 | PPSU | 110,997 | Yes | No |
| 6 | PPSU | N/A | N/A | N/A |
| Plate Number | Plate Material | Maximum Force (N) |
|---|---|---|
| 1 | Titanium * | 2281 |
| 2 | Titanium ** | 1500 |
| 3 | Titanium ** | 1500 |
| 4 | Titanium ** | 1500 |
| 5 | Titanium ** | 1500 |
| 6 | Titanium ** | 1500 |
| 1 | f-PEEK | 443 |
| 2 | f-PEEK | 711 |
| 3 | f-PEEK | 733 |
| 4 | f-PEEK | 679 |
| 5 | f-PEEK | 684 |
| 6 | f-PEEK | 709 |
| 1 | PEEK | 698 |
| 2 | PEEK | 565 |
| 3 | PEEK | 586 |
| 4 | PEEK | 601 |
| 5 | PEEK | 554 |
| 6 | PEEK | 545 |
| 1 | PEKK | 440 |
| 2 | PEKK | N/A |
| 3 | PEKK | 509 |
| 4 | PEKK | 545 |
| 5 | PEKK | 545 |
| 6 | PEKK | 458 |
| 1 | PPSU | N/A |
| 2 | PPSU | N/A |
| 3 | PPSU | N/A |
| 4 | PPSU | N/A |
| 5 | PPSU | N/A |
| 6 | PPSU | 326 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lommen, J.; Schorn, L.; Sproll, C.; Kübler, N.R.; Nicolini, L.F.; Merfort, R.; Dilimulati, A.; Hildebrand, F.; Rana, M.; Greven, J. Mechanical Fatigue Performance of Patient-Specific Polymer Plates in Oncologic Mandible Reconstruction. J. Clin. Med. 2022, 11, 3308. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123308
Lommen J, Schorn L, Sproll C, Kübler NR, Nicolini LF, Merfort R, Dilimulati A, Hildebrand F, Rana M, Greven J. Mechanical Fatigue Performance of Patient-Specific Polymer Plates in Oncologic Mandible Reconstruction. Journal of Clinical Medicine. 2022; 11(12):3308. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123308
Chicago/Turabian StyleLommen, Julian, Lara Schorn, Christoph Sproll, Norbert R. Kübler, Luis Fernando Nicolini, Ricarda Merfort, Ayimire Dilimulati, Frank Hildebrand, Majeed Rana, and Johannes Greven. 2022. "Mechanical Fatigue Performance of Patient-Specific Polymer Plates in Oncologic Mandible Reconstruction" Journal of Clinical Medicine 11, no. 12: 3308. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123308