
Use of Inhaled Corticosteroids and Risk of Acquiring Haemophilus influenzae in Patients with Chronic Obstructive Pulmonary Disease

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
- I
- The Danish Register of Chronic Obstructive Pulmonary Disease (DrCOPD), which is a national register established in 2008. It contains information about the quality of treatment of COPD patients from all over Denmark. Data are extracted from inpatient and outpatient pulmonary clinic visits. The following variables were used: age, forced expiratory volume in 1 s (FEV1), smoking status (i.e., active, former, never), BMI, dyspnoea registered using the Medical Research Council (MRC) Dyspnoea Scale [14].
- II
- The Danish National Patient Registry (DNPR), which is used to determine the comorbidities in the study population. It contains records from all Danish hospitals since 1977 and all hospital outpatient visits since 1995 [15].
- III
- The Danish National Database of Reimbursed Prescriptions (DNDRP), which is used to assess exposure to ICS. It contains records of all prescribed and reimbursed medications obtained in the Danish community and hospital-based pharmacies since 2004. Drugs are coded according to Anatomical Therapeutic Chemical (ATC) classification [16].
- IV
- Microbiological data, which were obtained from the Clinical Microbiology Departments in Eastern Denmark (i.e., Zealand and Capital Regions) to retrieve H. influenzae culture results.
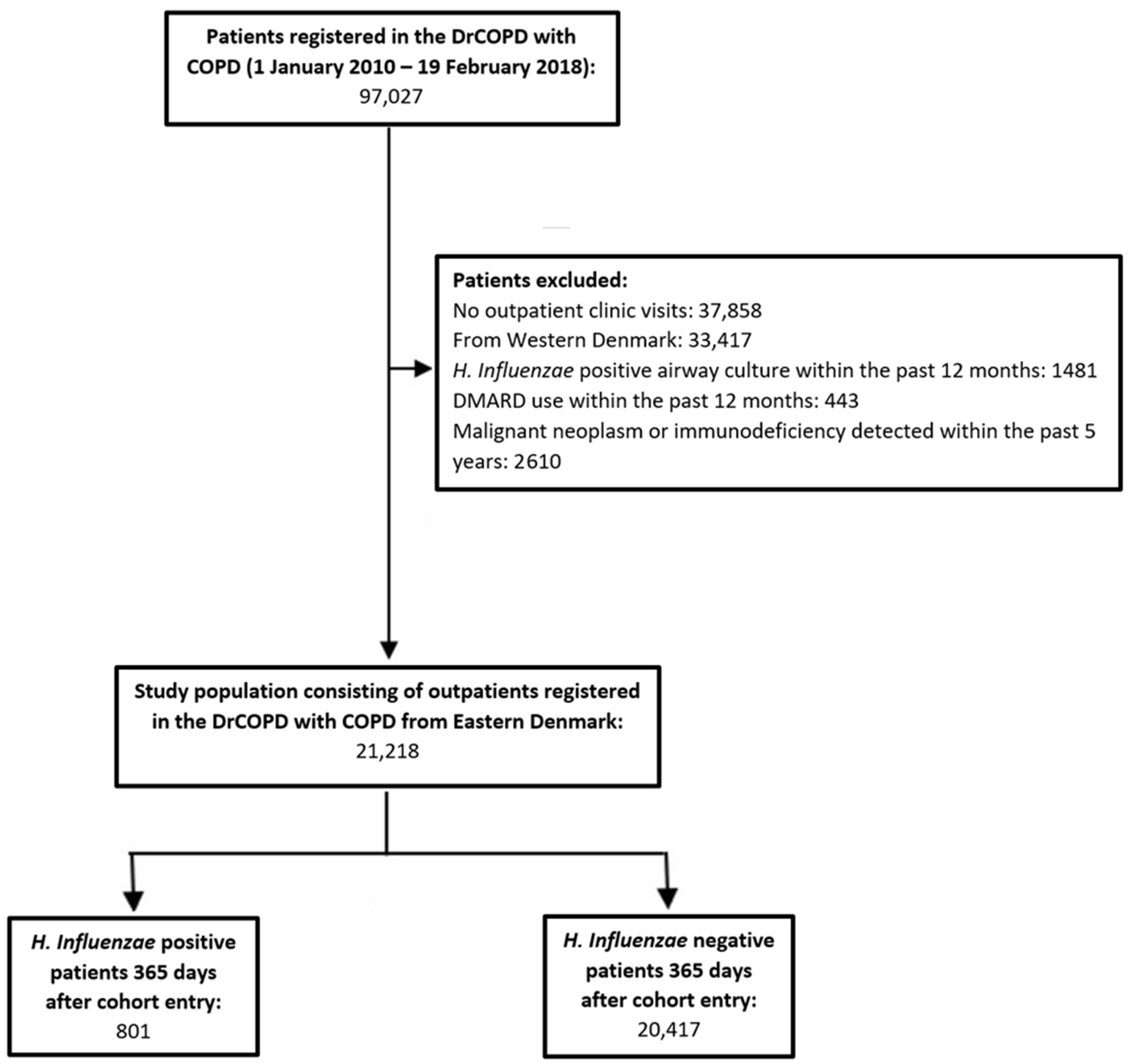
2.2. Study Population
2.3. Exposure to ICS
2.4. Outcome
2.5. Statistical Analysis
2.6. Sensitivity Analyses
3. Results
3.1. Outcome
3.2. Sensitivity Analyses
4. Discussion
4.1. Strengths of Current Study
4.2. Limitations of Current Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agusti, A.; Fabbri, L.M.; Singh, D.; Vestbo, J.; Celli, B.; Franssen, F.M.E.; Rabe, K.F.; Papi, A. Inhaled corticosteroids in COPD: Friend or foe? Eur. Respir. J. 2018, 52, 1801219. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Sin, D.D. Inhaled corticosteroids in COPD: The final verdict is. Eur. Respir. J. 2018, 52, 1801940. [Google Scholar] [CrossRef] [PubMed]
- Watz, H.; Tetzlaff, K.; Wouters, E.F.; Kirsten, A.; Magnussen, H.; Rodriguez-Roisin, R.; Vogelmeier, C.; Fabbri, L.M.; Chanez, P.; Dahl, R.; et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: A post-hoc analysis of the WISDOM trial. Lancet Respir. Med. 2016, 4, 390–398. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Singh, D.; Vestbo, J.; Paggiaro, P.L.; Jones, P.W.; Bonnet-Gonod, F.; Cohuet, G.; Corradi, M.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine beclomethasone/formoterol in severe COPD patients with history of exacerbations. Respir. Med. 2014, 108, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Kew, K.M.; Seniukovich, A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, CD010115. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Patenaude, V.; Lapi, F.; Ernst, P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax 2013, 68, 1029–1036. [Google Scholar] [CrossRef]
- Suissa, S. Mortality in IMPACT: Confounded by Asthma? Am. J. Respir. Crit. Care Med. 2020, 202, 772–773. [Google Scholar] [CrossRef]
- Calzetta, L.; Ritondo, B.L.; de Marco, P.; Cazzola, M.; Rogliani, P. Evaluating triple ICS/LABA/LAMA therapies for COPD patients: A network meta-analysis of ETHOS, KRONOS, IMPACT, and TRILOGY studies. Expert Rev. Respir. Med. 2021, 15, 143–152. [Google Scholar] [CrossRef]
- Calverley, P.M.; Anderson, J.A.; Celli, B.; Ferguson, G.T.; Jenkins, C.; Jones, P.W.; Yates, J.C.; Vestbo, J. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 2007, 356, 775–789. [Google Scholar] [CrossRef]
- Vestbo, J.; Anderson, J.A.; Brook, R.D.; Calverley, P.M.; Celli, B.R.; Crim, C.; Martinez, F.; Yates, J.; Newby, D.E.; Investigators, S. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): A double-blind randomised controlled trial. Lancet 2016, 387, 1817–1826. [Google Scholar] [CrossRef]
- Vestbo, J.; Fabbri, L.; Papi, A.; Petruzzelli, S.; Scuri, M.; Guasconi, A.; Vezzoli, S.; Singh, D. Inhaled corticosteroid containing combinations and mortality in COPD. Eur. Respir. J. 2018, 52, 1801230. [Google Scholar] [CrossRef] [PubMed]
- Desai, H.; Eschberger, K.; Wrona, C.; Grove, L.; Agrawal, A.; Grant, B.; Yin, J.; Parameswaran, G.I.; Murphy, T.; Sethi, S. Bacterial colonization increases daily symptoms in patients with chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 2014, 11, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Anzueto, A. Impact of exacerbations on COPD. Eur. Respir. Rev. 2010, 19, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Lange, P.; Tottenborg, S.S.; Sorknaes, A.D.; Andersen, J.S.; Sogaard, M.; Nielsen, H.; Thomsen, R.W.; Nielsen, K.A. Danish Register of chronic obstructive pulmonary disease. Clin. Epidemiol. 2016, 8, 673–678. [Google Scholar] [CrossRef]
- Schmidt, M.; Schmidt, S.A.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sorensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef]
- Johannesdottir, S.A.; Horvath-Puho, E.; Ehrenstein, V.; Schmidt, M.; Pedersen, L.; Sorensen, H.T. Existing data sources for clinical epidemiology: The Danish National Database of Reimbursed Prescriptions. Clin. Epidemiol. 2012, 4, 303–313. [Google Scholar] [CrossRef]
- Schmidt, M.; Pedersen, L.; Sorensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef]
- Sivapalan, P.; Ingebrigtsen, T.S.; Rasmussen, D.B.; Sørensen, R.; Rasmussen, C.M.; Jensen, C.B.; Allin, K.H.; Eklöf, J.; Seersholm, N.; Vestbo, J.; et al. COPD exacerbations: The impact of long versus short courses of oral corticosteroids on mortality and pneumonia: Nationwide data on 67,000 patients with COPD followed for 12 months. BMJ Open Respir. Res. 2019, 6, e000407. [Google Scholar] [CrossRef]
- Gensler, L.S. Glucocorticoids. Neurohospitalist 2013, 3, 92–97. [Google Scholar] [CrossRef]
- Sullivan, P.W.; Ghushchyan, V.H.; Globe, G.; Schatz, M. Oral corticosteroid exposure and adverse effects in asthmatic patients. J. Allergy Clin. Immunol. 2018, 141, 110–116. [Google Scholar] [CrossRef]
- Altman, D.G.; Andersen, P.K. Calculating the number needed to treat for trials where the outcome is time to an event. BMJ 1999, 319, 1492–1495. [Google Scholar] [CrossRef] [PubMed]
- Biomedical Statistics and Informatics Software Packages. Available online: http://bioinformaticstools.mayo.edu/research/gmatch/ (accessed on 4 January 2021).
- Andrejak, C.; Nielsen, R.; Thomsen, V.O.; Duhaut, P.; Sorensen, H.T.; Thomsen, R.W. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax 2013, 68, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Ernst, P.; Gonzalez, A.V.; Brassard, P.; Suissa, S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am. J. Respir. Crit. Care Med. 2007, 176, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Castellana, G.; Castellana, M.; Castellana, C.; Castellana, G.; Resta, E.; Carone, M.; Resta, O. Inhaled Corticosteroids and Risk of Tuberculosis in Patients with Obstructive Lung Diseases: A Systematic Review and Meta-Analysis of Non-randomized Studies. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2219–2227. [Google Scholar] [CrossRef]
- Brode, S.K.; Campitelli, M.A.; Kwong, J.C.; Lu, H.; Marchand-Austin, A.; Gershon, A.S.; Jamieson, F.B.; Marras, T.K. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur. Respir. J. 2017, 50, 1700037. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Machin, M.; Russell, K.E.; Pavlidis, S.; Zhu, J.; Barnes, P.J.; Chung, K.F.; Adcock, I.M.; Durham, A.L. Corticosteroid modulation of immunoglobulin expression and B-cell function in COPD. FASEB J. 2016, 30, 2014–2026. [Google Scholar] [CrossRef] [PubMed]
- van de Garde, M.D.; Martinez, F.O.; Melgert, B.N.; Hylkema, M.N.; Jonkers, R.E.; Hamann, J. Chronic exposure to glucocorticoids shapes gene expression and modulates innate and adaptive activation pathways in macrophages with distinct changes in leukocyte attraction. J. Immunol. 2014, 192, 1196–1208. [Google Scholar] [CrossRef]
- Contoli, M.; Pauletti, A.; Rossi, M.R.; Spanevello, A.; Casolari, P.; Marcellini, A.; Forini, G.; Gnesini, G.; Marku, B.; Barnes, N.; et al. Long-term effects of inhaled corticosteroids on sputum bacterial and viral loads in COPD. Eur. Respir. J. 2017, 50, 1700451. [Google Scholar] [CrossRef]
- Baindara, P. Host-directed therapies to combat tuberculosis and associated non-communicable diseases. Microb. Pathog. 2019, 130, 156–168. [Google Scholar] [CrossRef]
- Behrouzi, A.; Vaziri, F.; Rahimi-Jamnani, F.; Afrough, P.; Rahbar, M.; Satarian, F.; Siadat, S.D. Vaccine Candidates against Nontypeable Haemophilus influenzae: A Review. Iran. Biomed. J. 2017, 21, 69–76. [Google Scholar] [CrossRef]
- Sethi, S.; Murphy, T.F. Bacterial Infection in Chronic Obstructive Pulmonary Disease in 2000: A State-of-the-Art Review. Clin. Microbiol. Rev. 2001, 14, 336–363. [Google Scholar] [CrossRef] [PubMed]
- Smit, J.; Kaasch, A.J.; Sogaard, M.; Thomsen, R.W.; Nielsen, H.; Froslev, T.; Schonheyder, H.C. Use of Glucocorticoids and Risk of Community-Acquired Staphylococcus aureus Bacteremia: A Population-Based Case-Control Study. Mayo Clin. Proc. 2016, 91, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Matkovic, Z.; Miravitlles, M. Chronic bronchial infection in COPD. Is there an infective phenotype? Respir. Med. 2013, 107, 10–22. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | H. influenzae Positive Patients | H. influenzae Negative Patients | p Value | |
|---|---|---|---|---|
| Number of patients | 21,218 (100) | 801 (3.8) | 20,417 (96.2) | |
| Demographics | ||||
| Age (year), median (IQR) | 70 (62–77) | 68 (62–75) | 70 (62–77) | 0.01 |
| Age class | 0.0006 | |||
| Age < 62 | 5379 (25.4) | 206 (25.7) | 5173 (25.3) | |
| Age 62–69 | 5511 (26.0) | 254 (31.7) | 5257 (25.8) | |
| Age 70–77 | 5632 (26.5) | 191 (23.9) | 5441 (26.7) | |
| Age > 77 | 4696 (22.1) | 150 (18.7) | 4546 (22.3) | |
| Male | 9954 (46.9) | 403 (50.3) | 9551 (46.7) | 0.05 |
| BMI, median (IQR) | 25 (21–29) | 24 (20–28) | 25 (21–29) | <0.0001 |
| Unknown BMI | 2520 (11.9) | 49 (6.1) | 2471 (12.1) | |
| BMI class | <0.0001 | |||
| <18.5 | 1787 (8.4) | 115 (14.4) | 1672 (8.2) | |
| 18.5–24.9 | 7152 (33.7) | 293 (36.6) | 6859 (33.6) | |
| 25–29.9 | 5587 (26.3) | 211 (26.3) | 5376 (26.3) | |
| 30–34.9 | 2735 (12.9) | 90 (11.3) | 2645 (13.0) | |
| ≥35 | 1437 (6.8) | 43 (6.1) | 1394 (6.8) | |
| Pulmonary parameters | ||||
| MRC, median (IQR) | 3 (2–4) | 3 (3–4) | 3 (2–4) | <0.0001 |
| Unknown MRC | 2631 (12.4) | 56 (7.0) | 2575 (12.6) | |
| FEV1% predicted, median (IQR) | 49 (36–63) | 38 (29–50) | 50 (37–64) | <0.0001 |
| Unknown FEV1% | 2429 (11.5) | 51 (6.4) | 2378 (11.7) | |
| FEV1% predicted, severity of obstruction | <0.0001 | |||
| ≥80 | 1430 (6.01) | 19 (2.84) | 1411 (6.10) | |
| 79–50 | 9038 (37.99) | 155 (23.13) | 8883 (38.42) | |
| 49–30 | 9868 (41.48) | 306 (45.67) | 9562 (41.36) | |
| <30 | 3453 (14.52) | 190 (28.36) | 3263 (14.11) | |
| Smoking status | 0.004 | |||
| Active | 7187 (33.9) | 326 (40.7) | 6861 (33.6) | |
| Former | 11,043 (52.1) | 409 (51.1) | 10,634 (52.1) | |
| Never | 666 (3.1) | 18 (2.3) | 648 (3.2) | |
| Unknown | 2322 (10.9) | 48 (6.0) | 2274 (11.1) | |
| Hospital requiring COPD exacerbation 12 months prior to cohort entry | <0.0001 | |||
| 0 | 10,474 (49.4) | 309 (38.6) | 10,165 (49.8) | |
| 1 | 2903 (13.7) | 130 (16.2) | 2773 (13.6) | |
| ≥2 | 7841 (37.0) | 362 (45.2) | 7479 (36.6) | |
| All-cause hospitalisation 12 months prior to cohort entry | 18,313 (86.3) | 738 (92.1) | 17,575 (86.1) | <0.001 |
| Number of pulmonary microbial cultures in the preceding year a | 0 (0–2) | 1 (0–2) | 0 (0–2) | <0.0001 |
| All Patients | H. influenzae Positive Patients | H. influenzae Negative Patients | p Value | |
|---|---|---|---|---|
| Patients with ICS use | 14,142 (66.7) | 657 (82.0) | 13,485 (66.0) | <0.0001 |
| Accumulated ICS dose in ICS users a | <0.001 | |||
| Low | 4819 (34.1) | 143 (21.8) | 4676 (34.7) | |
| Moderate | 4559 (32.2) | 219 (33.3) | 4340 (32.2) | |
| High | 4764 (33.7) | 295 (44.9) | 4469 (33.1) | |
| Median accumulated ICS dose, mg (IQR) | 202 (96–367) | 269 (139–510) | 195 (96–360) | |
| Daily mean ICS dose, ug b | 763 | 984 | 752 | <0.0001 |
| Number of prescriptions, median (IQR) | 5 (2–8) | 6 (3–9) | 5 (2–8) | <0.001 |
| Number of prescriptions by ICS type c | ||||
| Beclomethasone | 765 (1.0) | 99 (2.2) | 666 (0.88) | |
| Budesonid | 51,871 (64.6) | 2584 (58.4) | 49,287 (64.9) | |
| Fluticasone | 27,266 (33.9) | 1679 (37.9) | 25,587 (33.7) | |
| Ciclesonide | 106 (0.13) | 21 (0.47) | 84 (0.11) | |
| Momethasone | 322 (0.40) | 45 (1.0) | 277 (0.36) | |
| H. influenzae | Unadjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | HR after Matching (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Accumulated ICS dose 365 days prior cohort entry, mg a | ||||||
| Low <120 | 1.37 (1.21–1.73) | 0.008 | 1.21 (0.95–1.53) | 0.1 | 1.32 (1.00–1.74) | 0.05 |
| Moderate 120–300 | 2.27 (1.84–2.81) | <0.0001 | 1.69 (1.35–2.12) | <0.0001 | 1.61 (1.24–2.09) | 0.0004 |
| High > 300 | 2.92 (2.39–3.57) | <0.0001 | 1.90 (1.52–2.38) | <0.0001 | 1.98 (1.54–2.56) | <0.0001 |
| ICS use without division into categories | 2.18 (1.82–2.62) | <0.0001 | 1.56 (1.29–1.89) | <0.0001 | ||
| Accumulated OCS dose 365 days prior to cohort entry, mg b | ||||||
| Low ≤750 | 1.89 (1.58–2.26) | <0.0001 | 1.57 (1.31–1.89) | <0.0001 | ||
| High >750 | 2.67 (2.28–3.14) | <0.0001 | 1.99 (1.67–2.37) | <0.0001 | ||
| Active smoking c | 1.32 (1.14–1.53) | 0.0003 | 1.33 (1.15–1.54) | 0.0002 | ||
| Age class | ||||||
| Age <62 | Reference | Reference | ||||
| Age 62–69 | 1.23 (1.02–1.48) | 0.03 | 1.11(0.92–1.34) | 0.3 | ||
| Age 70–77 | 0.89(0.73–1.08) | 0.2 | 0.83 (0.68–1.02) | 0.08 | ||
| Age >77 | 0.84 (0.68–1.04) | 0.1 | 0.84 (0.67–1.05) | 0.1 | ||
| Male | 1.17 (1.02–1.35) | 0.02 | 1.20 (1.04–1.38) | 0.01 | ||
| BMI class d | ||||||
| <18.5 | 1.84 (1.49–2.28) | <0.0001 | 1.38 (1.10–1.73) | 0.005 | ||
| 18.5–24.9 | Reference | Reference | ||||
| 25–29.9 | 1.07 (0.9–1.3) | 0.4 | 1.04 (0.88–1.24) | 0.6 | ||
| 30–34.9 | 0.94 (0.75–1.19) | 0.6 | 0.93 (0.74–1.18) | 0.5 | ||
| ≥35 | 0.87 (0.63–1.19) | 0.4 | 0.86 (0.62–1.18) | 0.3 | ||
| GOLD stage e | ||||||
| Stage 1: FEV1% ≥ 80 | Reference | Reference | ||||
| Stage 2: FEV1%= 79–50 | 1.38(0.88–2.16) | 0.2 | 1.21 (0.77–1.90) | 0.4 | ||
| Stage 3: FEV1% = 49–30 | 3.22(2.07–5.01) | <0.0001 | 2.29 (1.46–3.58) | 0.0003 | ||
| Stage 4: FEV1% < 30 | 5.05 (3.22–7.90) | <0.0001 | 2.81 (1.76–4.48) | <0.0001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohsin, R.U.; Heerfordt, C.K.; Eklöf, J.; Sivapalan, P.; Saeed, M.I.; Ingebrigtsen, T.S.; Nielsen, S.D.; Harboe, Z.B.; Iversen, K.K.; Bangsborg, J.; et al. Use of Inhaled Corticosteroids and Risk of Acquiring Haemophilus influenzae in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2022, 11, 3539. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123539
Mohsin RU, Heerfordt CK, Eklöf J, Sivapalan P, Saeed MI, Ingebrigtsen TS, Nielsen SD, Harboe ZB, Iversen KK, Bangsborg J, et al. Use of Inhaled Corticosteroids and Risk of Acquiring Haemophilus influenzae in Patients with Chronic Obstructive Pulmonary Disease. Journal of Clinical Medicine. 2022; 11(12):3539. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123539
Chicago/Turabian StyleMohsin, Raza Ul, Christian Kjer Heerfordt, Josefin Eklöf, Pradeesh Sivapalan, Mohamad Isam Saeed, Truls Sylvan Ingebrigtsen, Susanne Dam Nielsen, Zitta Barrella Harboe, Kasper Karmark Iversen, Jette Bangsborg, and et al. 2022. "Use of Inhaled Corticosteroids and Risk of Acquiring Haemophilus influenzae in Patients with Chronic Obstructive Pulmonary Disease" Journal of Clinical Medicine 11, no. 12: 3539. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11123539