
Effect of Combined Intraosseous and Intraarticular Infiltrations of Autologous Platelet-Rich Plasma on Subchondral Bone Marrow Mesenchymal Stromal Cells from Patients with Hip Osteoarthritis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PRP Preparation and Administration Procedure
2.3. Bone Marrow Aspirate Sample Processing and the Establishment of MSC Cultures
2.4. Colony-Forming Unit-Fibroblast (CFU-F) Assay and Colony Analysis
2.5. Senescence Assay
2.6. Gene Expression
2.7. Statistical Analysis
3. Results
3.1. Patients Characteristics and Response to Treatment
3.2. Platelet-Rich Plasma Characterization
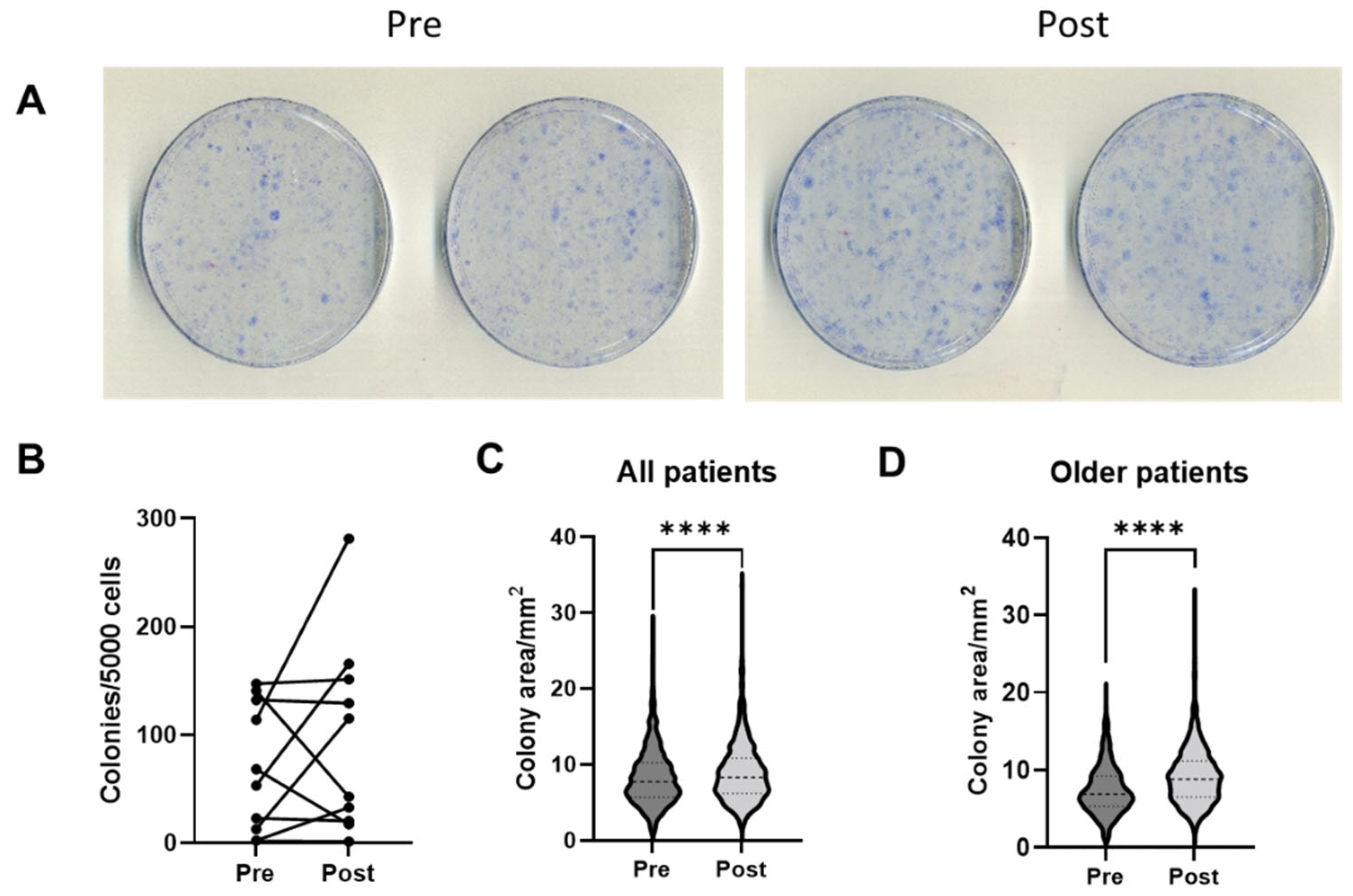
3.3. Colony Numbers and Characteristics
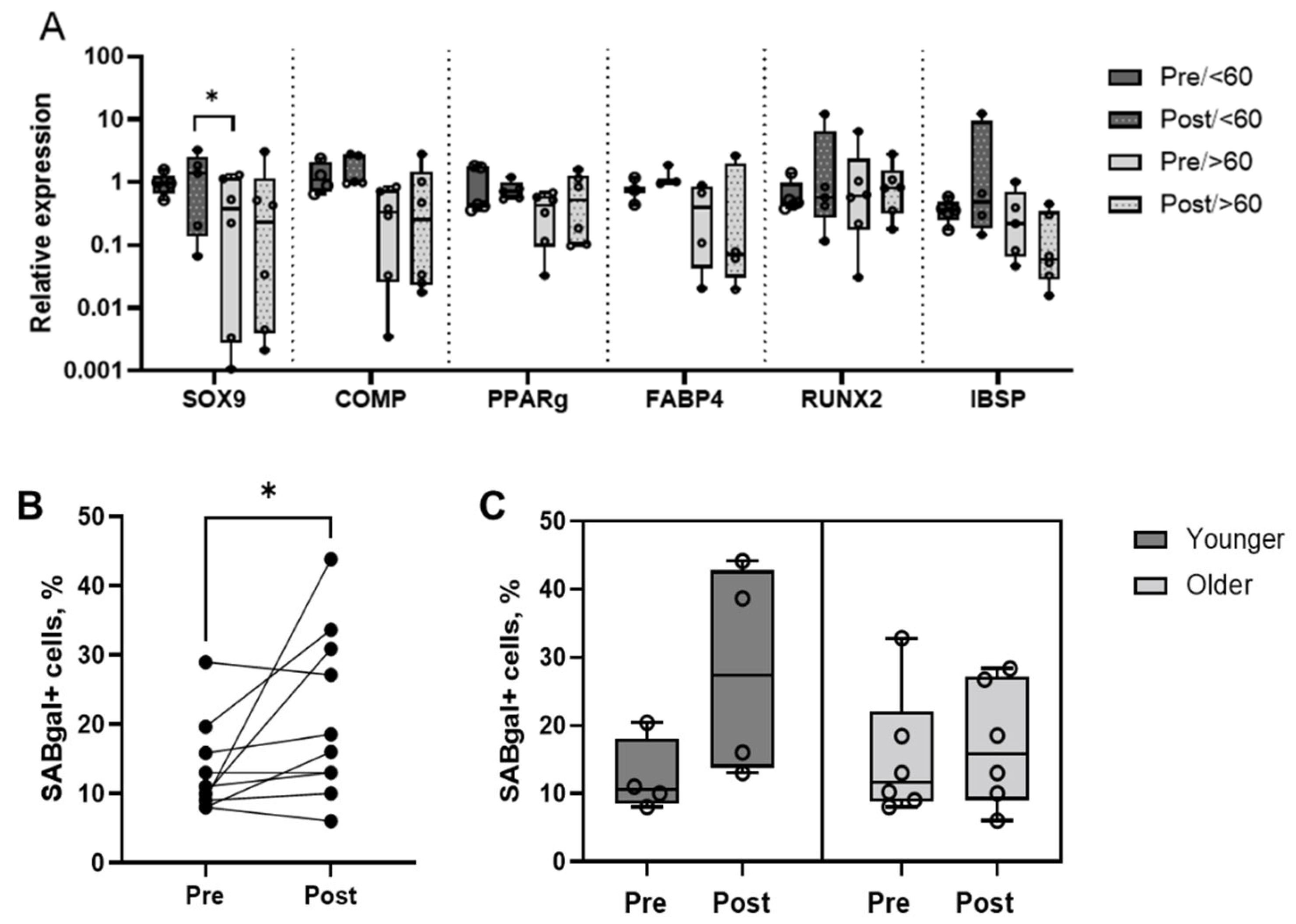
3.4. MSC Multipotentiality Marker Expression and Proportion of Senescent Cells
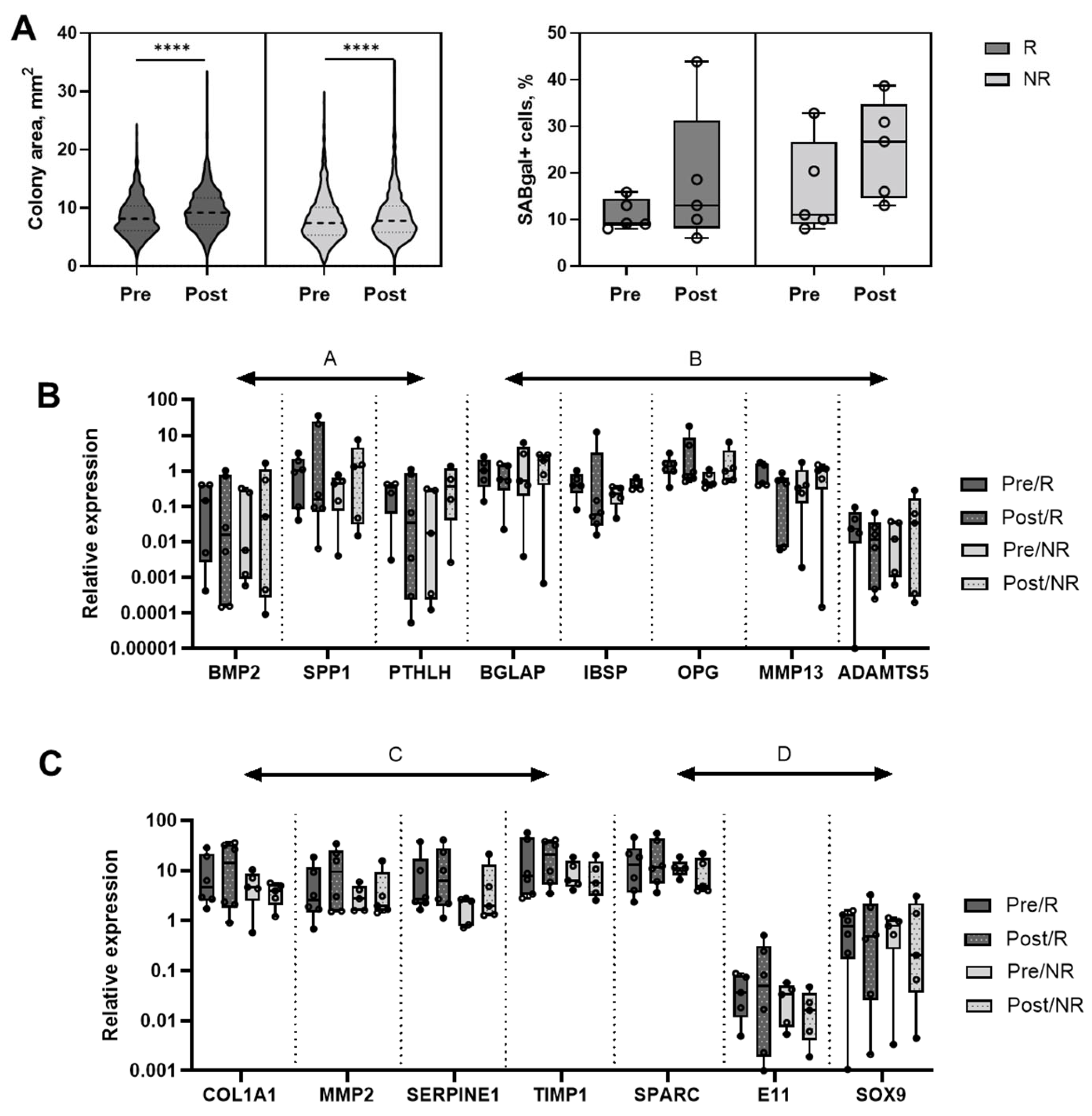
3.5. MSC Changes in Relation to Treatment Response
4. Discussion
5. Conclusions, Limitations and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sánchez, M.; Fiz, N.; Azofra, J.; Usabiaga, J.; Recalde, E.A.; Gutierrez, A.G.; Albillos, J.; Gárate, R.; Aguirre, J.J.; Padilla, S.; et al. A randomized clinical trial evaluating plasma rich in growth factors (PRGF-Endoret) versus hyaluronic acid in the short-term treatment of symptomatic knee osteoarthritis. Arthroscopy 2012, 28, 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.J.; Karas, V.; Hussey, K.; Merkow, D.B.; Pilz, K.; Fortier, L.A. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double-Blind Randomized Controlled Trial Comparing Clinical Outcomes and Effects on Intra-articular Biology for the Treatment of Knee Osteoarthritis. Am. J. Sports Med. 2017, 45, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Anitua, E.; Delgado, D.; Sanchez, P.; Prado, R.; Goiriena, J.J.; Prosper, F.; Orive, G.; Padilla, S. A new strategy to tackle severe knee osteoarthritis: Combination of intra-articular and intraosseous injections of Platelet Rich Plasma. Expert Opin. Biol. Ther. 2016, 16, 627–643. [Google Scholar] [CrossRef] [PubMed]
- Kon, E.; Di Matteo, B.; Delgado, D.; Cole, B.J.; Dorotei, A.; Dragoo, J.L.; Filardo, G.; Fortier, L.A.; Giuffrida, A.; Jo, C.H.; et al. Platelet-rich plasma for the treatment of knee osteoarthritis: An expert opinion and proposal for a novel classification and coding system. Expert Opin. Biol. Ther. 2020, 20, 1447–1460. [Google Scholar] [CrossRef]
- Goldring, S.R.; Goldring, M.B. Changes in the osteochondral unit during osteoarthritis: Structure, function and cartilage-bone crosstalk. Nat. Rev. Rheumatol. 2016, 12, 632–644. [Google Scholar] [CrossRef]
- Yuan, X.; Meng, H.; Wang, Y.; Peng, J.; Guo, Q.; Wang, A.; Lu, S. Bone-cartilage interface crosstalk in osteoarthritis: Potential pathways and future therapeutic strategies. Osteoarthr. Cartil. 2014, 22, 1077–1089. [Google Scholar] [CrossRef] [Green Version]
- Ilas, D.C.; Churchman, S.M.; McGonagle, D.; Jones, E. Targeting subchondral bone mesenchymal stem cell activities for intrinsic joint repair in osteoarthritis. Future Sci. OA 2017, 3, FSO228. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, M.; Delgado, D.; Sánchez, P.; Muiños-López, E.; Paiva, B.; Granero-Moltó, F.; Prósper, F.; Pompei, O.; Perez, J.C.; Azofra, J.; et al. Combination of Intra-Articular and Intraosseous Injections of Platelet Rich Plasma for Severe Knee Osteoarthritis: A Pilot Study. BioMed Res. Int. 2016, 2016, 4868613. [Google Scholar] [CrossRef]
- Muiños-López, E.; Delgado, D.; Sánchez, P.; Paiva, B.; Anitua, E.; Fiz, N.; Aizpurua, B.; Guadilla, J.; Padilla, S.; Granero-Moltó, F.; et al. Modulation of Synovial Fluid-Derived Mesenchymal Stem Cells by Intra-Articular and Intraosseous Platelet Rich Plasma Administration. Stem Cells Int. 2016, 2016, 1247950. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, M.; Delgado, D.; Pompei, O.; Pérez, J.C.; Sánchez, P.; Garate, A.; Bilbao, A.M.; Fiz, N.; Padilla, S. Treating Severe Knee Osteoarthritis with Combination of Intra-Osseous and Intra-Articular Infiltrations of Platelet-Rich Plasma: An Observational Study. Cartilage 2019, 10, 245–253. [Google Scholar] [CrossRef]
- Fiz, N.; Pérez, J.C.; Guadilla, J.; Garate, A.; Sánchez, P.; Padilla, S.; Delgado, D.; Sánchez, M. Intraosseous Infiltration of Platelet-Rich Plasma for Severe Hip Osteoarthritis. Arthrosc. Tech. 2017, 6, e821–e825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, K.; Bai, Y.; Wang, J.; Zhang, H.; Liu, H.; Ma, S. Comparison of hyaluronic acid and PRP intra-articular injection with combined intra-articular and intraosseous PRP injections to treat patients with knee osteoarthritis. Clin. Rheumatol. 2018, 37, 1341–1350. [Google Scholar] [CrossRef]
- Zhen, G.; Wen, C.; Jia, X.; Li, Y.; Crane, J.; Mears, S.C.; Askin, F.B.; Frassica, F.J.; Chang, W.; Yao, J.; et al. Inhibition of TGF-β signaling in mesenchymal stem cells of subchondral bone attenuates osteoarthritis. Nat. Med. 2013, 19, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.M.; Dixon, K.; Beck, S.; Fabian, D.; Feldman, A.; Barry, F. Reduced chondrogenic and adipogenic activity of mesenchymal stem cells from patients with advanced osteoarthritis. Arthritis Rheum. 2002, 46, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Campbell, T.M.; Churchman, S.M.; Gomez, A.; McGonagle, D.; Conaghan, P.G.; Ponchel, F.; Jones, E. Mesenchymal Stem Cell Alterations in Bone Marrow Lesions in Patients With Hip Osteoarthritis. Arthritis Rheumatol. 2016, 68, 1648–1659. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.G.; El-Jawhari, J.J.; Brockett, C.L.; Koria, L.; Ktistakis, I.; Jones, E. Multipotential stromal cells in the talus and distal tibia in ankle osteoarthritis—Presence, potency and relationships to subchondral bone changes. J. Cell. Mol. Med. 2021, 25, 259–271. [Google Scholar] [CrossRef]
- Coryell, P.R.; Diekman, B.O.; Loeser, R.F. Mechanisms and therapeutic implications of cellular senescence in osteoarthritis. Nat. Rev. Rheumatol. 2021, 17, 47–57. [Google Scholar] [CrossRef]
- Jeon, O.H.; Kim, C.; Laberge, R.-M.; DeMaria, M.; Rathod, S.; Vasserot, A.P.; Chung, J.W.; Kim, D.H.; Poon, Y.; David, N.; et al. Local clearance of senescent cells attenuates the development of post-traumatic osteoarthritis and creates a pro-regenerative environment. Nat. Med. 2017, 23, 775–781. [Google Scholar] [CrossRef]
- Kovalenko, B.; Bremjit, P.; Fernando, N. Classifications in Brief: Tönnis Classification of Hip Osteoarthritis. Clin. Orthop. Relat. Res. 2018, 476, 1680–1684. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Fragkakis, E.M.; El-Jawhari, J.J.; Dunsmuir, R.A.; Millner, P.A.; Rao, A.S.; Henshaw, K.T.; Pountos, I.; Jones, E.; Giannoudis, P.V. Vertebral body versus iliac crest bone marrow as a source of multipotential stromal cells: Comparison of processing techniques, tri-lineage differentiation and application on a scaffold for spine fusion. PLoS ONE 2018, 13, e0197969. [Google Scholar] [CrossRef] [PubMed]
- El-Jawhari, J.J.; Kleftouris, G.; El-Sherbiny, Y.; Saleeb, H.; West, R.M.; Jones, E.; Giannoudis, P.V. Defective Proliferation and Osteogenic Potential with Altered Immunoregulatory phenotype of Native Bone marrow-Multipotential Stromal Cells in Atrophic Fracture Non-Union. Sci. Rep. 2019, 9, 17340. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, P.; El-Jawhari, J.J.; Burska, A.N.; Ponchel, F.; Giannoudis, P.V.; Jones, E.A. The Analysis of In Vivo Aging in Human Bone Marrow Mesenchymal Stromal Cells Using Colony-Forming Unit-Fibroblast Assay and the CD45 low CD271 + Phenotype. Stem Cells Int. 2019, 2019, 5197983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churchman, S.M.; Boxall, S.A.; McGonagle, D.; Jones, E.A. Predicting the Remaining Lifespan and Cultivation-Related Loss of Osteogenic Capacity of Bone Marrow Multipotential Stromal Cells Applicable across a Broad Donor Age Range. Stem Cells Int. 2017, 2017, 6129596. [Google Scholar] [CrossRef] [PubMed]
- Gothard, D.; Dawson, J.I.; Oreffo, R.O.C. Assessing the potential of colony morphology for dissecting the CFU-F population from human bone marrow stromal cells. Cell Tissue Res. 2013, 352, 237–247. [Google Scholar] [CrossRef]
- Sanjurjo-Rodriguez, C.; Altaie, A.; Mastbergen, S.; Baboolal, T.; Welting, T.; Lafeber, F.; Pandit, H.; McGonagle, D.; Jones, E. Gene Expression Signatures of Synovial Fluid Multipotent Stromal Cells in Advanced Knee Osteoarthritis and Following Knee Joint Distraction. Front. Bioeng. Biotechnol. 2020, 8, 579751. [Google Scholar] [CrossRef] [PubMed]
- Zhai, W.; Tan, J.; Russell, T.; Chen, S.; McGonagle, D.; Naing, M.W.; Yong, D.; Jones, E. Multi-pronged approach to human mesenchymal stromal cells senescence quantification with a focus on label-free methods. Sci. Rep. 2021, 11, 1054. [Google Scholar] [CrossRef]
- Ganguly, P.; Burska, A.N.; Davis, C.L.; El-Jawhari, J.J.; Giannoudis, P.V.; Jones, E.A. Intrinsic Type 1 Interferon (IFN1) Profile of Uncultured Human Bone Marrow CD45 low CD271 + Multipotential Stromal Cells (BM-MSCs): The Impact of Donor Age, Culture Expansion and IFNα and IFNβ Stimulation. Biomedicines 2020, 8, 214. [Google Scholar] [CrossRef]
- Churchman, S.; Ponchel, F.; Boxall, S.A.; Cuthbert, R.; Kouroupis, D.; Roshdy, T.; Giannoudis, P.V.; Emery, P.; McGonagle, D.; Jones, E.A. Transcriptional profile of native CD271+ multipotential stromal cells: Evidence for multiple fates, with prominent osteogenic and Wnt pathway signaling activity. Arthritis Rheum. 2012, 64, 2632–2643. [Google Scholar] [CrossRef]
- Farr, J.N.; Khosla, S. Cellular senescence in bone. Bone 2019, 121, 121–133. [Google Scholar] [CrossRef]
- Marie, P.J. Bone cell senescence: Mechanisms and perspectives. J. Bone Miner. Res. 2014, 29, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Sanjurjo-Rodriguez, C.; Baboolal, T.G.; Burska, A.N.; Ponchel, F.; El-Jawhari, J.; Pandit, H.; McGonagle, D.; Jones, E. Gene expression and functional comparison between multipotential stromal cells from lateral and medial condyles of knee osteoarthritis patients. Sci. Rep. 2019, 9, 9321. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee osteoarthritis: A review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes 2020, 11, 854. [Google Scholar] [CrossRef] [PubMed]
- Zahir, H.; Dehghani, B.; Yuan, X.; Chinenov, Y.; Kim, C.; Burge, A.; Bandhari, R.; Nemirov, D.; Fava, P.; Moley, P.; et al. In vitro responses to platelet-rich-plasma are associated with variable clinical outcomes in patients with knee osteoarthritis. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Andia, I.; Atilano, L.; Maffulli, N. Moving toward targeting the right phenotype with the right platelet-rich plasma (PRP) formulation for knee osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211004336. [Google Scholar] [CrossRef]
- Paterson, K.L.; Hunter, D.J.; Metcalf, B.R.; Eyles, J.; Duong, V.; Kazsa, J.; Wang, Y.; Buchbinder, R.; Cicuttini, F.; Forbes, A.; et al. Efficacy of intra-articular injections of platelet-rich plasma as a symptom- and disease-modifying treatment for knee osteoarthritis—the RESTORE trial protocol. BMC Musculoskelet. Disord. 2018, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, P.; El-Jawhari, J.J.; Giannoudis, P.V.; Burska, A.N.; Ponchel, F.; Jones, E.A. Age-related Changes in Bone Marrow Mesenchymal Stromal Cells: A Potential Impact on Osteoporosis and Osteoarthritis Development. Cell Transplant. 2017, 26, 1520–1529. [Google Scholar] [CrossRef] [Green Version]
- Philippart, P.; Meuleman, N.; Stamatopoulos, B.; Najar, M.; Pieters, K.; De Bruyn, C.; Bron, D.; Lagneaux, L. In vivo production of mesenchymal stromal cells after injection of autologous platelet-rich plasma activated by recombinant human soluble tissue factor in the bone marrow of healthy volunteers. Tissue Eng. Part A 2014, 20, 160–170. [Google Scholar] [CrossRef]
- Watt, F.; Hamid, B.; Garriga, C.; Judge, A.; Hrusecka, R.; Custers, R.; Jansen, M.; Lafeber, F.; Mastbergen, S.; Vincent, T. The molecular profile of synovial fluid changes upon joint distraction and is associated with clinical response in knee osteoarthritis. Osteoarthr. Cartil. 2020, 28, 324–333. [Google Scholar] [CrossRef] [Green Version]
- Delgado, D.; Garate, A.; Sánchez, P.; Bilbao, A.M.; del Caño, G.G.; Salles, J.; Sánchez, M. Biological and structural effects after intraosseous infiltrations of age-dependent platelet-rich plasma: An in vivo study. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2020, 38, 1931–1941. [Google Scholar] [CrossRef]
- Bolia, I.K.; Bougioukli, S.; Hill, W.J.; Trasolini, N.A.; Petrigliano, F.A.; Lieberman, J.R.; Weber, A.E. Clinical Efficacy of Bone Marrow Aspirate Concentrate Versus Stromal Vascular Fraction Injection in Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2022, 50, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- El-Kadiry, A.E.-H.; Rafei, M.; Shammaa, R. Cell Therapy: Types, Regulation, and Clinical Benefits. Front. Med. 2021, 8, 756029. [Google Scholar] [CrossRef] [PubMed]
- Ghasroldasht, M.M.; Seok, J.; Park, H.-S.; Ali, F.B.L.; Al-Hendy, A. Stem Cell Therapy: From Idea to Clinical Practice. Int. J. Mol. Sci. 2022, 23, 2850. [Google Scholar] [CrossRef] [PubMed]
- Shirokova, L.; Noskov, S.; Gorokhova, M.V.; Reinecke, J.A.; Shirokova, K. Intra-Articular Injections of a Whole Blood Clot Secretome, Autologous Conditioned Serum, Have Superior Clinical and Biochemical Efficacy Over Platelet-Rich Plasma and Induce Rejuvenation-Associated Changes of Joint Metabolism: A Prospective, Controlled Open-Label Clinical Study in Chronic Knee Osteoarthritis. Rejuvenation Res. 2020, 23, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-Y.; Huang, C.-F.; Lin, T.-C.; Tsai, C.-Y.; Chen, S.-Y.T.; Liu, A.; Chen, W.-H.; Wei, H.-J.; Wang, M.-F.; Williams, D.F.; et al. Delayed animal aging through the recovery of stem cell senescence by platelet rich plasma. Biomaterials 2014, 35, 9767–9776. [Google Scholar] [CrossRef]
- Görmeli, G.; Görmeli, C.A.; Ataoglu, B.; Çolak, C.; Aslantürk, O.; Ertem, K. Multiple PRP injections are more effective than single injections and hyaluronic acid in knees with early osteoarthritis: A randomized, double-blind, placebo-controlled trial. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2017, 25, 958–965. [Google Scholar] [CrossRef]
- Ganguly, P.; Toghill, B.; Pathak, S. Aging, Bone Marrow and Next-Generation Sequencing (NGS): Recent Advances and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 12225. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Gender | Age, Years | Response | Tönnis | Medications |
|---|---|---|---|---|
| M | 58 | Positive | 3 | Unspecified treatment for arterial hypertension |
| F | 61 | Positive | 2 | None |
| F | 56 | Negative | 3 | Unspecified treatment for arterial hypertension |
| F | 54 | Negative | 3 | None |
| F | 61 | Positive | 2 | None |
| F | 70 | Positive | 2 | Thyroxine |
| M | 61 | Negative | 2 | Antihypertensives; Statins |
| M | 40 | Negative | 2 | None |
| F | 55 | Positive | 3 | None |
| F | 64 | Positive | 3 | None |
| M | 56 | Positive | 3 | Leflunomide |
| F | 86 | Negative | 3 | Escitalopram; Paracetamol |
| PRP Preparation | |
| Blood volume taken | 72 mL |
| Anticoagulant | Sodium citrate 3.8% (w/v) |
| System | Close |
| Centrifugation | Once, 580 g/8 min |
| Final PRP volume | 10 mL (IO) plus 8 mL (IA) |
| PRP Characteristics | |
| PRP Type | 13-00-11 |
| MPV | 10.1 fL (CI: 9.30–10.50) |
| Red Blood Cells | <0.01 × 106/μL |
| White Blood Cells | <0.05 × 106/μL |
| Activation | CaCl2 10% (w/v) |
| Application Characteristics | |
| Formulation type | Liquid |
| Administration route | IO plus IA |
| Dosage | 2 infiltrations at two weeks interval |
| Volume | IO: 10 mL (5 mL acetabulum + 5 mL femoral head) IA injection: 8 mL |
| Dose (range of platelets) | IO injection: 2.76 × 109–3.98 × 109 IA injection: 2.21 × 109–3.18 × 109 |
| Tissue | Cartilage, synovium, subchondral bone |
| Pathology | Hip osteoarthritis |
| Genes | Median Relative Expression Values | Fold Differences, Post/Pre | ||||
|---|---|---|---|---|---|---|
| Pre/R | Post/R | Pre/NR | Post/NR | R | NR | |
| RUNX2 | 0.5016 | 0.6905 | 0.5779 | 0.8294 | 1.376595 | 1.435196 |
| ALP | 0.5477 | 0.9033 | 0.3409 | 0.5918 | 1.649261 | 1.735993 |
| IBSP | 0.3944 | 0.05968 | 0.22 | 0.3793 | 0.151318 | 1.724091 |
| COL1A1 | 4.653 | 14.38 | 4.677 | 3.967 | 3.090479 | 0.848193 |
| BGLAP | 1.02 | 0.57 | 0.5216 | 1.952 | 0.558824 | 3.742331 |
| SPP1 | 1.001 | 0.1541 | 0.4335 | 1.323 | 0.153946 | 3.051903 |
| SPARC | 12.91 | 11.64 | 11.16 | 4.895 | 0.901627 | 0.43862 |
| OPG | 1.34 | 0.8102 | 0.4803 | 0.9831 | 0.604627 | 2.046846 |
| ANKH | 0.4462 | 0.5939 | 0.5231 | 0.5771 | 1.331017 | 1.103231 |
| GREM1 | 0.555 | 0.9183 | 0.3949 | 1.152 | 1.654595 | 2.917194 |
| E11 | 0.03657 | 0.04949 | 0.03373 | 0.01627 | 1.353295 | 0.48236 |
| BMP2 | 0.1449 | 0.01558 | 0.005887 | 0.05139 | 0.107522 | 8.729404 |
| PTHLH | 0.3283 | 0.03508 | 0.01772 | 0.3664 | 0.106853 | 20.6772 |
| SOX9 | 0.7716 | 0.4732 | 0.7836 | 0.2052 | 0.613271 | 0.261868 |
| COMP | 0.6122 | 0.7304 | 0.6867 | 1.027 | 1.193074 | 1.495558 |
| ACAN | 0.9876 | 1.029 | 0.6267 | 1.112 | 1.04192 | 1.774374 |
| MMP1 | 0.1341 | 0.4476 | 0.06261 | 0.1486 | 3.337808 | 2.373423 |
| MMP2 | 2.528 | 9.414 | 2.76 | 1.982 | 3.723892 | 0.718116 |
| MMP13 | 0.4501 | 0.4859 | 0.3275 | 1.014 | 1.079538 | 3.096183 |
| ADAMTS4 | 0.02331 | 0.01155 | 0.01217 | 0.03424 | 0.495495 | 2.813476 |
| SERPINE1 | 2.658 | 6.356 | 2.449 | 1.942 | 2.391272 | 0.792977 |
| TIMP1 | 7.729 | 20.88 | 6.346 | 5.652 | 2.701514 | 0.89064 |
| TIMP2 | 2.32 | 3.828 | 2.023 | 2.37 | 1.65 | 1.171527 |
| TIMP3 | 4.378 | 7.125 | 2.982 | 1.84 | 1.627455 | 0.617036 |
| PTGS2 | 1.096 | 0.8219 | 1.066 | 1.071 | 0.749909 | 1.00469 |
| PPAR-ɣ | 0.431 | 0.6278 | 0.5237 | 0.7886 | 1.456613 | 1.505824 |
| CXCL12 | 1.246 | 1.911 | 1.721 | 2.398 | 1.533708 | 1.393376 |
| VEGFA | 1.099 | 2.048 | 1.109 | 1.403 | 1.863512 | 1.265104 |
| VEGFC | 6.912 | 8.79 | 7.783 | 8.161 | 1.271701 | 1.048567 |
| PDGFRB | 1.009 | 1.253 | 0.6647 | 0.9144 | 1.241824 | 1.375658 |
| EGFR | 0.06623 | 0.08422 | 0.03631 | 0.1435 | 1.271629 | 3.952079 |
| FGFR1 | 0.387 | 0.571 | 0.2379 | 0.4063 | 1.475452 | 1.70786 |
| FGFR2 | 0.2632 | 0.1553 | 0.3359 | 0.3029 | 0.590046 | 0.901756 |
| TGFBR2 | 0.4042 | 0.8372 | 0.3433 | 0.4072 | 2.071252 | 1.186135 |
| PTPRC | 0.6435 | 1.469 | 0.5147 | 0.6744 | 2.282828 | 1.310278 |
| NT5E | 1.536 | 1.891 | 1.718 | 2.714 | 1.23112 | 1.579744 |
| Thy1 | 1.97 | 1.764 | 1.33 | 1.625 | 0.895431 | 1.221805 |
| P21 | 1.215 | 1.097 | 1.091 | 0.9113 | 0.902881 | 0.835289 |
| P53 | 0.646 | 0.6835 | 0.5047 | 0.5311 | 1.05805 | 1.052308 |
| P16 | 1.705 | 1.359 | 1.483 | 2.114 | 0.797067 | 1.425489 |
| HPRT1 | 1 | 1 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganguly, P.; Fiz, N.; Beitia, M.; Owston, H.E.; Delgado, D.; Jones, E.; Sánchez, M. Effect of Combined Intraosseous and Intraarticular Infiltrations of Autologous Platelet-Rich Plasma on Subchondral Bone Marrow Mesenchymal Stromal Cells from Patients with Hip Osteoarthritis. J. Clin. Med. 2022, 11, 3891. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133891
Ganguly P, Fiz N, Beitia M, Owston HE, Delgado D, Jones E, Sánchez M. Effect of Combined Intraosseous and Intraarticular Infiltrations of Autologous Platelet-Rich Plasma on Subchondral Bone Marrow Mesenchymal Stromal Cells from Patients with Hip Osteoarthritis. Journal of Clinical Medicine. 2022; 11(13):3891. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133891
Chicago/Turabian StyleGanguly, Payal, Nicolás Fiz, Maider Beitia, Heather E. Owston, Diego Delgado, Elena Jones, and Mikel Sánchez. 2022. "Effect of Combined Intraosseous and Intraarticular Infiltrations of Autologous Platelet-Rich Plasma on Subchondral Bone Marrow Mesenchymal Stromal Cells from Patients with Hip Osteoarthritis" Journal of Clinical Medicine 11, no. 13: 3891. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11133891