
Late Dialysis Modality Education Could Negatively Predict Peritoneal Dialysis Selection

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
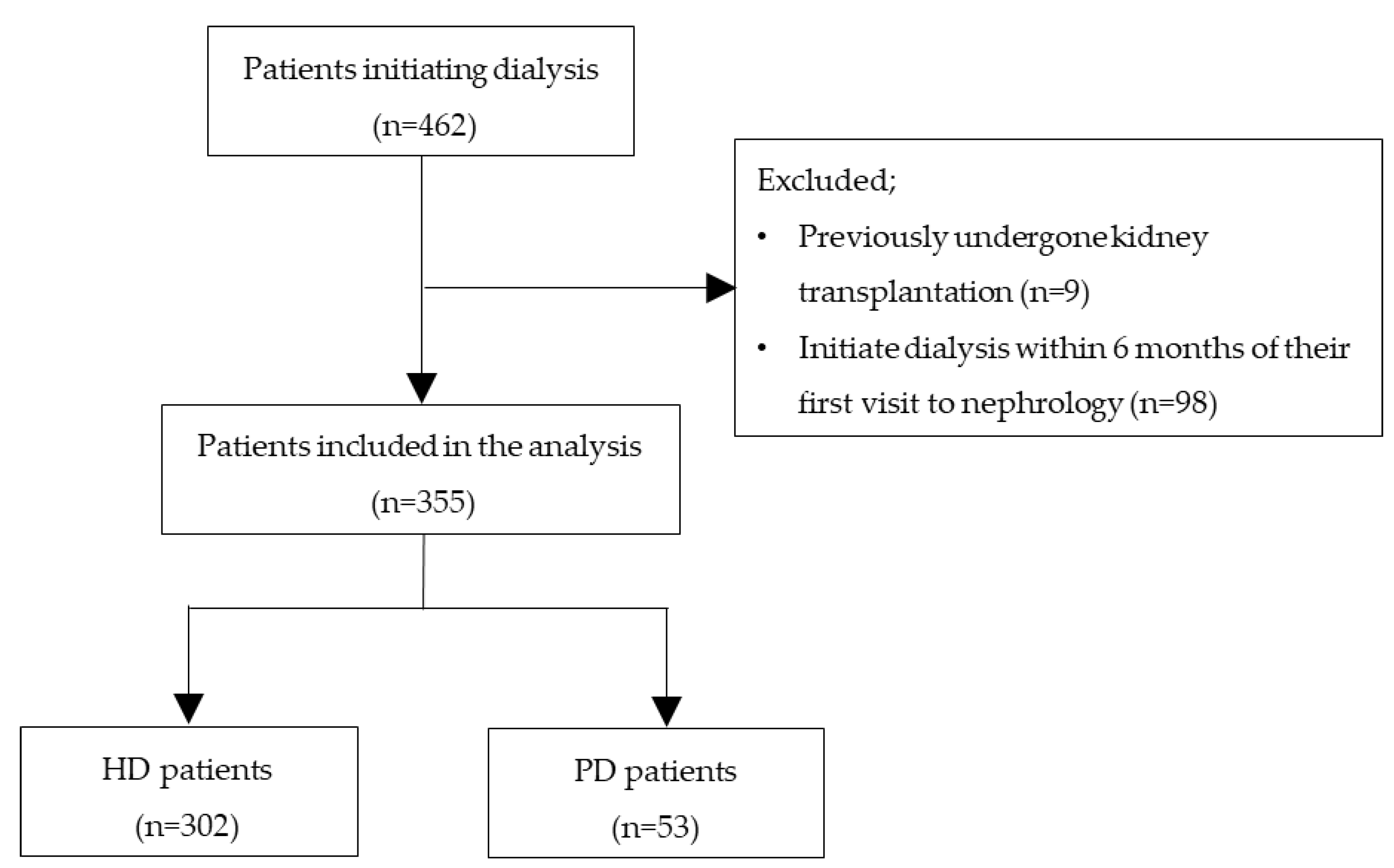
2.1. Study Population
2.2. Data Collection and Participant Evaluation
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Biochemical Data
3.3. Timing of Education
3.4. Influence of the Timing of RRT Education on Dialysis Modality Selection
3.5. Dialysis Modality Selection and Timing of Patient Education for Each Attending Doctor
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Karopadi, A.N.; Mason, G.; Rettore, E.; Ronco, C. Cost of peritoneal dialysis and hemodialysis across the world. Nephrol. Dial Transpl. 2013, 28, 2553–2569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sens, F.; Schott-Pethelaz, A.M.; Labeeuw, M.; Colin, C.; Villar, E. Survival advantage of hemodialysis relative to peritoneal dialysis in patients with end-stage renal disease and congestive heart failure. Kidney Int. 2011, 80, 970–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, M.; Nakano, H.; Nakayama, M. Novel therapeutic option for refractory heart failure in elderly patients with chronic kidney disease by incremental peritoneal dialysis. J. Cardiol. 2010, 55, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Jansen, M.A.; Hart, A.A.; Korevaar, J.C.; Dekker, F.W.; Boeschoten, E.W.; Krediet, R.T. Predictors of the rate of decline of residual renal function in incident dialysis patients. Kidney Int. 2002, 62, 1046–1053. [Google Scholar] [CrossRef] [Green Version]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef]
- Rubin, H.R.; Fink, N.E.; Plantinga, L.C.; Sadler, J.H.; Kliger, A.S.; Powe, N.R. Patient ratings of dialysis care with peritoneal dialysis vs hemodialysis. JAMA 2004, 291, 697–703. [Google Scholar] [CrossRef] [Green Version]
- Fadem, S.Z.; Walker, D.R.; Abbott, G.; Friedman, A.L.; Goldman, R.; Sexton, S.; Peters, T.G. Satisfaction with renal replacement therapy and education: The American Association of Kidney Patients survey. Clin. J. Am. Soc. Nephrol. 2011, 6, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Li, P.K.; Chow, K.M.; Van de Luijtgaarden, M.W.; Johnson, D.W.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef]
- Nitta, K.; Goto, S.; Masakane, I.; Hanafusa, N.; Taniguchi, M.; Hasegawa, T.; Nakai, S.; Wada, A.; Hamano, T.; Hoshino, J.; et al. Annual dialysis data report for 2018, JSDT Renal Data Registry: Survey methods, facility data, incidence, prevalence, and mortality. Ren. Replace. Ther. 2020, 6, 41. [Google Scholar] [CrossRef]
- Stack, A.G. Determinants of modality selection among incident US dialysis patients: Results from a national study. J. Am. Soc. Nephrol. 2002, 13, 1279–1287. [Google Scholar] [CrossRef]
- Liebman, S.E.; Bushinsky, D.A.; Dolan, J.G.; Veazie, P. Differences between dialysis modality selection and initiation. Am. J. Kidney Dis. 2012, 59, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Schellartz, I.; Mettang, S.; Shukri, A.; Scholten, N.; Pfaff, H.; Mettang, T. Early referral to nephrological care and the uptake of peritoneal dialysis. An analysis of German claims data. Int. J. Env. Res. Public Health 2021, 18, 8359. [Google Scholar] [CrossRef]
- Devoe, D.J.; Wong, B.; James, M.T.; Ravani, P.; Oliver, M.J.; Barnieh, L.; Quinn, R.R. Patient education and peritoneal dialysis modality selection: A systematic review and meta-analysis. Am. J. Kidney Dis. 2016, 68, 422–433. [Google Scholar] [CrossRef]
- Abecassis, M.; Bartlett, S.T.; Collins, A.J. Kidney transplantation as primary therapy for end-stage renal disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference. Clin. J. Am. Soc. Nephrol. 2008, 3, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Payne, R.B.; Little, A.J.; Williams, R.B.; Milner, J.R. Interpretation of serum calcium in patients with abnormal serum proteins. Br. Med. J. 1973, 4, 643–646. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Cho, K.H.; Park, J.W.; Yoon, K.W.; Do, J.Y. Geriatric Nutritional Risk Index as a prognostic factor in peritoneal dialysis patients. Perit. Dial Int. 2013, 33, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Troidle, L.; Kliger, A.; Finkelstein, F. Barriers to utilization of chronic peritoneal dialysis in network #1, New England. Perit. Dial Int. 2006, 26, 452–457. [Google Scholar]
- Jassal, S.V.; Krishna, G.; Mallick, N.P.; Mendelssohn, D.C. Attitudes of British Isles nephrologists towards dialysis modality selection: A questionnaire study. Nephrol. Dial Transpl. 2002, 17, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Korevaar, J.C.; Dekker, F.W.; Krediet, R.T.; Boeschoten, E.W. The effect of contraindications and patient preference on dialysis modality selection in ESRD patients in the Netherlands. Am. J. Kidney Dis. 2004, 43, 891–899. [Google Scholar] [CrossRef] [PubMed]
- De Maar, J.S.; de Groot, M.A.; Luik, P.T.; Mui, K.W.; Hagen, E.C. Guide. GUIDE, a structured pre-dialysis programme that increases the use of home dialysis. Clin. Kidney J. 2016, 9, 826–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribitsch, W.; Haditsch, B.; Otto, R.; Schilcher, G.; Quehenberger, F.; Roob, J.M.; Rosenkranz, A.R. Effects of a pre-dialysis patient education program on the relative frequencies of dialysis modalities. Perit. Dial Int. 2013, 33, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Marsh, D.; Vonesh, E.; Peters, V.; Nissenson, A. Patient education and access of ESRD patients to renal replacement therapies beyond in-center hemodialysis. Kidney Int. 2005, 68, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Chanouzas, D.; Ng, K.P.; Fallouh, B.; Baharani, J. What influences patient choice of treatment modality at the pre-dialysis stage? Nephrol. Dial Transpl. 2012, 27, 1542–1547. [Google Scholar] [CrossRef] [Green Version]
- Etgen, T.; Chonchol, M.; Förstl, H.; Sander, D. Chronic kidney disease and cognitive impairment: A systematic review and meta-analysis. Am. J. Nephrol. 2012, 35, 474–482. [Google Scholar] [CrossRef]
- Drew, D.A.; Weiner, D.E.; Sarnak, M.J. Cognitive impairment in CKD: Pathophysiology, management, and prevention. Am. J. Kidney Dis. 2019, 74, 782–790. [Google Scholar] [CrossRef]
- Kurella, M.; Chertow, G.M.; Luan, J.; Yaffe, K. Cognitive impairment in chronic kidney disease. J. Am. Geriatr. Soc. 2004, 52, 1863–1869. [Google Scholar] [CrossRef]
- Zee, J.; Zhao, J.; Subramanian, L.; Perry, E.; Bryant, N.; McCall, M.; Restovic, Y.; Torres, D.; Robinson, B.M.; Pisoni, R.L.; et al. Perceptions about the dialysis modality decision process among peritoneal dialysis and in-center hemodialysis patients. BMC Nephrol. 2018, 19, 298. [Google Scholar] [CrossRef] [Green Version]
- Allen, L.A.; Stevenson, L.W.; Grady, K.L.; Goldstein, N.E.; Matlock, D.D.; Arnold, R.M.; Spertus, J.A. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation 2012, 125, 1928–1952. [Google Scholar] [CrossRef]
- Heaf, J.; Heiro, M.; Petersons, A. Choice of dialysis modality among patients initiating dialysis: Results of the Peridialysis study. Clin. Kidney J. 2021, 14, 2064–2074. [Google Scholar] [CrossRef]
- Marrón, B.; Ortiz, A.; de Sequera, P.; Martín-Reyes, G.; De Arriba, G.; Lamas, J.M.; Ocaña, J.C.M.; Arrieta, J.; Martínez, F. Impact of end-stage renal disease care in planned dialysis start and type of renal replacement therapy-a Spanish multicentre experience. Nephrol. Dial Transplant. 2006, 21 (Suppl. 2), ii51–ii55. [Google Scholar] [CrossRef] [Green Version]
- Ito, Y.; Ryuzaki, M.; Sugiyama, H.; Tomo, T.; Yamashita, A.C.; Ishikawa, Y.; Nakamoto, H. Peritoneal Dialysis Guidelines 2019 Part 1 (Position paper of the Japanese Society for Dialysis Therapy). Ren. Replace Ther. 2021, 7, 40. [Google Scholar] [CrossRef]
- Mendelssohn, D.C.; Mullaney, S.R.; Jung, B.; Blake, P.G.; Mehta, R.L. What do American nephrologists think about dialysis modality selection? Am. J. Kidney Dis. 2001, 37, 22–29. [Google Scholar] [CrossRef]
- Nakayama, M.; Itami, Y.; Kanazawa, Y.; Nakamoto, H.; Masakane, I.; Kawanishi, H. The report from the working committee of the preparation for revised JSDT PD guideline. Jpn. Dial Soc. 2011, 44, 1199–1204. (In Japanese) [Google Scholar] [CrossRef]
- Song, Q.; Yan, H.; Yu, Z.; Li, Z.; Yuan, J.; Ni, Z.; Fang, W. Assisted peritoneal dialysis: A feasible KRT modality for frail older patients with end-stage kidney disease (ESKD). Sci. Rep. 2021, 11, 14928. [Google Scholar] [CrossRef]
- Nakayama, T.; Uchiyama, K.; Washida, N.; Morimoto, K.; Muraoka, K.; Adachi, K.; Kasai, T.; Miyashita, K.; Wakino, S.; Itoh, H. Exercise parameters predict technique survival in patients on peritoneal dialysis. Blood Purif. 2021, 50, 380–389. [Google Scholar] [CrossRef]
- Lanot, A.; Bechade, C.; Boyer, A.; Ficheux, M.; Lobbedez, T. Assisted peritoneal dialysis and transfer to haemodialysis: A cause-specific analysis with data from the RDPLF. Nephrol. Dial Transpl. 2021, 36, 330–339. [Google Scholar] [CrossRef]
- Iyasere, O.U.; Brown, E.A.; Johansson, L.; Huson, L.; Smee, J.; Maxwell, A.P.; Farrington, K.; Davenport, A. Quality of life and physical function in older patients on dialysis: A comparison of assisted peritoneal dialysis with hemodialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Bargman, J.M.; Thorpe, K.E.; Churchill, D.N. Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: A reanalysis of the CANUSA study. J. Am. Soc. Nephrol. 2001, 12, 2158–2162. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Park, J.T.; Park, K.S.; Kwon, Y.E.; Oh, H.J.; Yoo, T.-H.; Kim, Y.-L.; Kim, Y.S.; Yang, C.W.; Kim, N.-H.; et al. Prognostic value of residual urine volume, GFR by 24-hour urine Collection, and eGFR in patients receiving dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 426–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | All Patients (n = 355) | Group with HD (n = 302) | Group with PD (n = 53) | p-Value |
|---|---|---|---|---|
| Age (year) | 70 (59–79) | 71 (61–80) | 59 (50–71) | <0.01 |
| Sex (% female) | 102 (28.7%) | 90 (29.8%) | 12 (22.6%) | 0.37 |
| Welfare public assistance recipient (%) | 13 (3.7%) | 12 (4.0%) | 1 (1.9%) | 0.46 |
| Living alone (%) | 69 (19.4%) | 61 (20.2%) | 8 (15.1%) | 0.39 |
| Smoking history | 207 (58.3%) | 178 (58.9%) | 29 (54.7%) | 0.67 |
| Body mass index | 23.2 (20.4–26.1) | 23.1 (20.2–25.7) | 23.9 (22.2–27.2) | <0.05 |
| Systolic blood pressure (mmHg) | 139.2 ± 19.6 | 139.7 ± 19.8 | 136.3 ± 18.3 | 0.26 |
| Diastolic blood pressure (mmHg) | 74.9 ± 14.9 | 74.3 ± 15.2 | 77.8 ± 12.5 | 0.12 |
| Charlson comorbidity index | 4 (3–6) | 5 (4–6) | 4 (3–4) | <0.01 |
| Underlying conditions | ||||
| Diabetic kidney disease | 130 (36.6%) | 108 (35.8%) | 22 (41.5%) | 0.52 |
| Renal sclerosis | 88 (24.8%) | 80 (26.5%) | 8 (15.1%) | 0.11 |
| Glomerulonephritis | 59 (16.6%) | 44 (14.6%) | 15 (28.3%) | <0.05 |
| Polycystic kidney disease | 14 (3.9%) | 11 (3.6%) | 3 (5.7%) | 0.75 |
| Tubulointerstitial nephritis | 15 (4.2%) | 14 (4.6%) | 1 (1.9%) | 0.58 |
| Others | 49 (13.8%) | 45 (14.9%) | 4 (7.5%) | 0.22 |
| Comorbidities | ||||
| Diabetes | 160 (45.1%) | 131 (43.4%) | 29 (54.7%) | 0.17 |
| Hypertension | 334 (94.1%) | 282 (93.4%) | 52 (98.1%) | 0.30 |
| Coronary artery disease | 63 (17.7%) | 54 (17.9%) | 9 (17.0%) | 1.00 |
| Congestive heart failure | 98 (27.6%) | 90 (29.8%) | 8 (15.1%) | <0.05 |
| Cerebrovascular disease | 65 (18.3%) | 59 (19.5%) | 6 (11.3%) | 0.22 |
| Malignancy | 82 (23.1%) | 76 (25.2%) | 6 (11.3%) | <0.05 |
| eGFR at first visit to the nephrology department (mL/min/1.73 m2) | 25.2 (16.8–37.6) | 24.9 (16.9–37.1) | 25.6 (14.1–42.1) | 0.89 |
| Variables | All Patients (n = 355) | Group with HD (n = 302) | Group with PD (n = 53) | p-Value |
|---|---|---|---|---|
| Urea nitrogen (mg/dL) | 85.3 (70.0–102.5) | 87.2 (71.6–104.4) | 75.7 (62.5–88.8) | <0.01 |
| Creatinine (mg/dL) | 8.8 (7.4–10.5) | 8.8 (7.4–10.5) | 8.6 (7.5–9.9) | 0.81 |
| eGFR (mL/min/1.73 m2) | 5.0 (4.0–6.1) | 4.9 (3.9–6.1) | 5.4 (4.4–6.1) | 0.14 |
| Albumin (g/dL) | 3.2 ± 0.6 | 3.2 ± 0.6 | 3.3 ± 0.5 | <0.05 |
| Geriatric nutritional risk index | 92 (83–100) | 91 (82–99) | 96 (90–103) | <0.01 |
| Hemoglobin (g/dL) | 9.8 ± 1.4 | 9.7 ± 1.4 | 10.0 ± 1.2 | 0.22 |
| Potassium (mEq/L) | 4.6 ± 0.9 | 4.6 ± 0.9 | 4.9 ± 0.8 | <0.05 |
| Corrected calcium (mg/dL) | 8.6 ± 1.1 | 8.6 ± 1.2 | 8.5 ± 0.5 | 0.17 |
| Phosphorus (mg/dL) | 6.5 ± 1.9 | 6.5 ± 2.0 | 6.2 ± 1.4 | 0.28 |
| Triglyceride (mg/dL) | 118 (84–156) | 116 (83–155) | 134 (88–175) | 0.14 |
| HDL–cholesterol (mg/dL) | 42 (33–54) | 42 (33–53) | 39 (33–53) | 0.98 |
| LDL–cholesterol (mg/dL) | 87 (67–110) | 85 (67–105) | 90 (74–109) | 0.50 |
| eGFR decline rate for 6 months before dialysis initiation (%) | 44.5 (31.2–57.3) | 45.0 (31.3–57.6) | 42.4 (31.0–53.9) | 0.31 |
| Variables | All Patients (n = 355) | Group with HD (n = 302) | Group with PD (n = 53) | p-Value |
|---|---|---|---|---|
| eGFR at RRT education (mL/min/1.73 m2) | 8.0 (6.3–9.7) | 7.9 (6.2–9.5) | 8.9 (7.4–11.0) | <0.01 |
| eGFR at general education on CKD (mL/min/1.73 m2) | 9.1 (6.9–11.7) | 8.9 (6.5–11.5) | 9.3 (8.0–11.8) | 0.13 |
| Time from RRT education to dialysis initiation (month) | 4 (2–9) | 4 (2–9) | 6 (4–10) | <0.05 |
| Time from general education on CKD to dialysis initiation (month) | 6 (2–16) | 6 (1–17) | 7 (4–11) | 0.20 |
| Variables | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (per 10 years) | 0.72 (0.57–0.91) | <0.01 | 0.70 (0.55–0.90) | <0.01 | 0.70 (0.55–0.90) | <0.01 |
| Sex (female) | 0.74 (0.34–1.60) | 0.44 | 0.72 (0.33–1.56) | 0.40 | 0.74 (0.33–1.63) | 0.45 |
| Welfare public assistance | 0.73 (0.08–6.33) | 0.78 | 0.70 (0.08–6.12) | 0.75 | 0.70 (0.08–6.09) | 0.74 |
| Living alone | 0.58 (0.23–1.46) | 0.25 | 0.60 (0.24–1.50) | 0.27 | 0.60 (0.24–1.51) | 0.28 |
| Charlson comorbidity index (per 1) | 0.78 (0.63–0.96) | <0.05 | 0.78 (0.63–0.96) | <0.05 | 0.77 (0.62–0.96) | <0.05 |
| Geriatric nutritional risk index (per 10) | 1.25 (0.96–1.62) | 0.10 | 1.22 (0.93–1.60) | 0.15 | 1.24 (0.94–1.64) | 0.14 |
| eGFR at first visit to the nephrology department (per 1 mL/min/1.73 m2) | 1.00 (0.99–1.02) | 0.83 | 1.00 (0.99–1.02) | 0.84 | 1.00 (0.98–1.02) | 0.88 |
| eGFR at RRT education (per 1 mL/min/1.73 m2) | 1.14 (1.02–1.27) | <0.05 | 1.12 (1.00–1.26) | <0.05 | 1.12 (0.99–1.26) | 0.07 |
| eGFR decline rate for 6 months before dialysis initiation (%) | – | – | 0.95 (0.80–1.14) | 0.60 | 0.97 (0.79–1.20) | 0.81 |
| eGFR at dialysis initiation (per 1 mL/min/1.73 m2) | – | – | – | – | 1.04 (0.84–1.29) | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, T.; Nishioka, K.; Uchiyama, K.; Morimoto, K.; Kusahana, E.; Washida, N.; Yamaguchi, S.; Azegami, T.; Yoshida, T.; Itoh, H. Late Dialysis Modality Education Could Negatively Predict Peritoneal Dialysis Selection. J. Clin. Med. 2022, 11, 4042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144042
Nakayama T, Nishioka K, Uchiyama K, Morimoto K, Kusahana E, Washida N, Yamaguchi S, Azegami T, Yoshida T, Itoh H. Late Dialysis Modality Education Could Negatively Predict Peritoneal Dialysis Selection. Journal of Clinical Medicine. 2022; 11(14):4042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144042
Chicago/Turabian StyleNakayama, Takashin, Ken Nishioka, Kiyotaka Uchiyama, Kohkichi Morimoto, Ei Kusahana, Naoki Washida, Shintaro Yamaguchi, Tatsuhiko Azegami, Tadashi Yoshida, and Hiroshi Itoh. 2022. "Late Dialysis Modality Education Could Negatively Predict Peritoneal Dialysis Selection" Journal of Clinical Medicine 11, no. 14: 4042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144042