
Frailty Status Improvement after 5-Month Multicomponent Program PROMUFRA in Community-Dwelling Older People: A Randomized Controlled Trial

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Study Subjects
2.3. Procedures
2.3.1. Physical Frailty Assessment
2.3.2. Kinanthropometric Assessments
2.3.3. Muscle Function Assessments
2.3.4. Training Program
- (1)
- Warm-up exercises, including aerobic exercises and joint mobility for 10 min. The aerobic exercises consisted of vigorous walks. Balance and coordination exercises were also performed in addition to the joint mobility exercises [4];
- (2)
- Progressive HIRT (main part I) lasting 42 to 45 min. Adequate intensity (70–80% of 1RM) was attained, after overcoming the previous adaptation and progression period (20–30% of 1RM) [7]. Six strength exercises were performed (two trunk, two arms and two legs) to achieve integrated work and global body improvement, although only the leg exercises (leg press and knee extension) were assessed. During the resistance training circuit, the muscle groups (arms, trunk and legs) were alternated, though always, and for every three exercises performed, one was on the legs. The circuit had three sets per exercise and 8–12 repetitions per set, until failure [24]. From a practical point of view, performing between 8–12 RM is equivalent to a training intensity of between 70–80% of 1RM, which guaranteed that they were training at high intensity [31]. The exercises were performed at a pace of 2:3 (2 s concentric action: 3 s eccentric action), with a two-minute rest between series [32]. To maintain the correct progression of the load every six sessions, the maximum repetition of each participant was calculated [24]. In this way, when the participant had reached a new milestone in the 1RM valuation, the workload was adjusted to that value;
- (3)
- SMMR (main part II) lasting 9–10 min. The volume of work in each session consisted of performing seven exercises per session (four lower limbs, one chest and two back). Each exercise had one set of 10 repetitions, with approximately 60 s per exercise, since each repetition (round trip cycle) lasted 6 s. The participants applied self-pressure by following the direction of the forces generated by each muscle group throughout the body. The load progression took into account the amount of pressure exerted on the soft tissue to be treated. To do this, we combined the position of the people performing the SMMR and two physical properties of the materials: size and hardness. The rollers included foam rollers (Ø 15 cm), a rubber hedgehog ball (perimeter 25 cm), a medium soft rubber hedgehog ball (perimeter 38 cm), a medium smooth rubber inflatable ball (perimeter 43.5 cm) and a large smooth foam rubber ball (perimeter 62 cm). In general, progress was made from a larger size and lesser hardness to a smaller size and greater hardness of the implements used. Two of the exercises went from sitting to standing (gluteal muscles and abductors). All of this was completed to ensure greater pressure, that is, a progression of the load, in the area to be treated. A physiotherapist and a graduate in Physical Activity, specialized in physical activity for the frail and pre-frail older adults, monitored the training sessions. Each week there were two different SMMR sessions, according to the muscle groups involved (session 1: quadriceps, hamstrings, abductors, gluteus, pectoral, full back and trapezius; session 2: quadriceps, adductors, hip flexors, calves, pectoral, full back and trapezius). The different devices were applied from the muscle origin to its insertion, at a pace of 3:3 (3 s down or right/3 s up or left) set by a metronome, and applying as much pressure as possible, without reaching pain. The exercises were carried out bilaterally whenever possible;
- (4)
- Finally, static exercises were performed during cool down. Maintaining between 10–30 s of muscle stretching to provoke a relaxed disposition of the active muscles during the session. In addition, mechanical stress was applied to the myofascial tissue according to the direction of the muscle group in order to influence the disposition of the new muscle fibers.
2.3.5. Pain Assessment
2.3.6. Treatment Fidelity
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
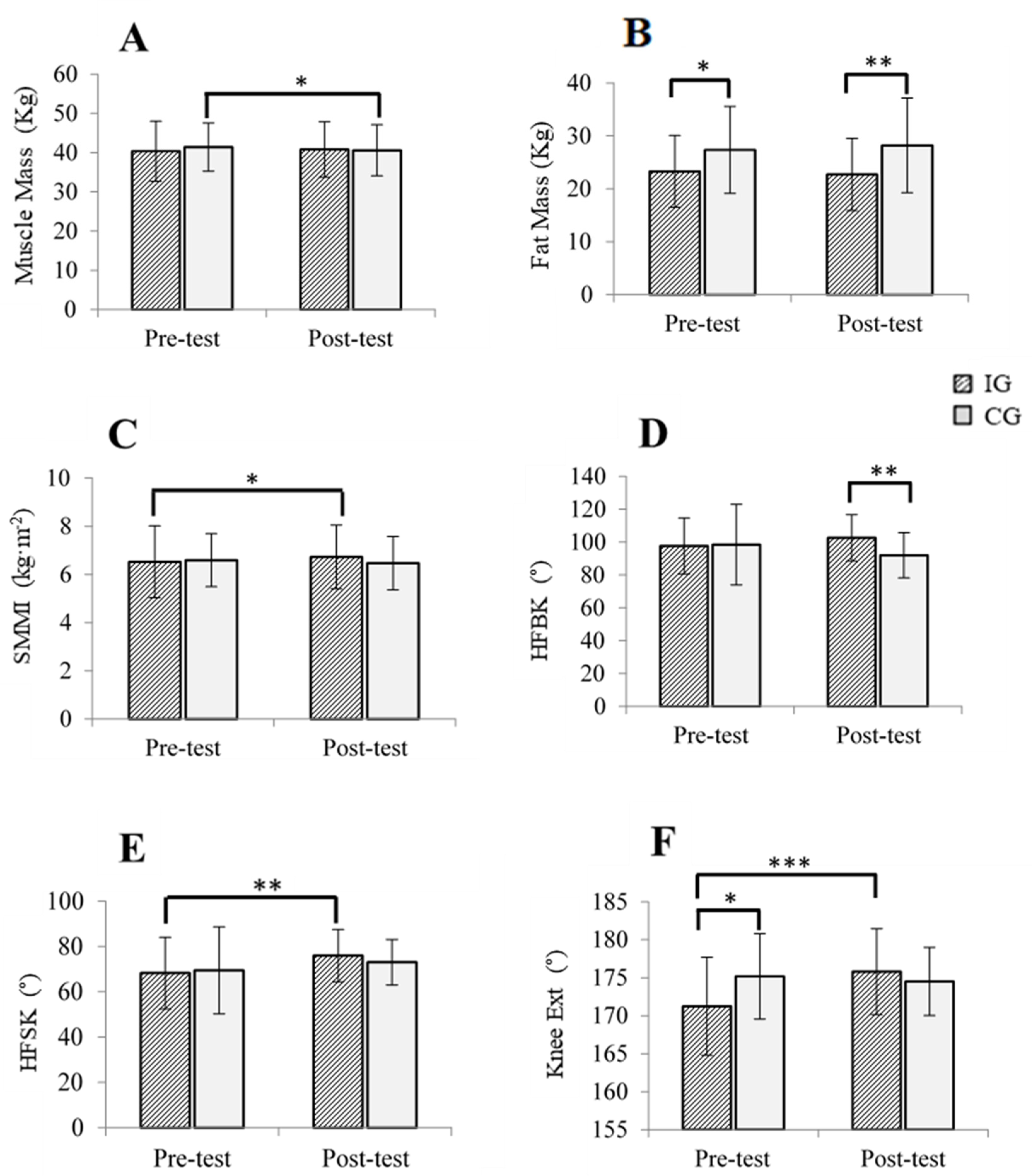
3.2. Kinanthropometry, Physical Frailty, and Muscle Function Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.; Doehner, W.; Evans, J.; et al. Frailty Consensus: A Call to Action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Voshaar, R.O. Prevalence of Frailty in Community-Dwelling Older Persons: A Systematic Review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Abizanda Soler, P.; Rodríguez-Mañas, L. Fragilidad en el Anciano. In Tratado de Medicina Geriátrica, 2nd ed.; Abizanda Soler, P., Rodríguez-Mañas, L., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; ISBN 84-9113-759-9. [Google Scholar]
- Izquierdo, M.; Cadore, E.L.; Casas-Herrero, Á. Ejercicio Físico en el Anciano Frágil: Entrenamiento de Fuerza, Resistencia Cardiovascular y Entrenamiento Multicomponente. In Tratado de Medicina Geriátrica, 2nd ed.; Abizanda Soler, P., Rodrí-guez-Mañas, L., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; ISBN 84-9113-759-9. [Google Scholar]
- Herrero, C.; Cadore, E.; Velilla, N.M.; Redin, M.I. El ejercicio físico en el anciano frágil: Una actualización. Rev. Española Geriatría Gerontol. 2015, 50, 74–81. [Google Scholar] [CrossRef]
- Fiatarone, M.A.; O′Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise Training and Nutritional Supplementation for Physical Frailty in Very Elderly People. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Csapo, R.; Gumpenberger, M.; Wessner, B. Skeletal Muscle Extracellular Matrix—What Do We Know About Its Composition, Regulation, and Physiological Roles? A Narrative Review. Front. Physiol. 2020, 11, 253. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Kostrominova, T.Y.; Faulkner, J.A.; Wineman, A.S. Age-related changes in the mechanical properties of the epimysium in skeletal muscles of rats. J. Biomech. 2008, 41, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Azizi, E.; DesLauriers, A.R.; Holt, N.C.; Eaton, C. Resistance to radial expansion limits muscle strain and work. Biomech. Model. Mechanobiol. 2017, 16, 1633–1643. [Google Scholar] [CrossRef] [Green Version]
- Sharafi, B.; Blemker, S.S. A mathematical model of force transmission from intrafascicularly terminating muscle fibers. J. Biomech. 2011, 44, 2031–2039. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M.F. The basic science of myofascial release: Morphologic change in connective tissue. J. Bodyw. Mov. Ther. 1997, 1, 231–238. [Google Scholar] [CrossRef]
- Schroeder, A.N.; Best, T.M. Is Self Myofascial Release an Effective Preexercise and Recovery Strategy? A Literature Review. Curr. Sports Med. Rep. 2015, 14, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Weerapong, P.; Hume, P.A.; Kolt, G. The Mechanisms of Massage and Effects on Performance, Muscle Recovery and Injury Prevention. Sports Med. Auckl. 2005, 35, 235–256. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, G.Z.; Penney, M.D.; Mullaley, M.E.; Cuconato, A.L.; Drake, C.D.; Behm, D.G.; Button, D.C. An Acute Bout of Self-Myofascial Release Increases Range of Motion Without a Subsequent Decrease in Muscle Activation or Force. J. Strength Cond. Res. 2013, 27, 812–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearcey, G.E.P.; Bradbury-Squires, D.J.; Kawamoto, J.-E.; Drinkwater, E.J.; Behm, D.G.; Button, D.C. Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures. J. Athl. Train. 2015, 50, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleip, R.; Müller, D.G. Training principles for fascial connective tissues: Scientific foundation and suggested practical applications. J. Bodyw. Mov. Ther. 2013, 17, 103–115. [Google Scholar] [CrossRef]
- Støve, M.P.; Hirata, R.P.; Palsson, T.S. Muscle stretching—the potential role of endogenous pain inhibitory modulation on stretch tolerance. Scand. J. Pain 2019, 19, 415–422. [Google Scholar] [CrossRef]
- Gumpenberger, M.; Wessner, B.; Graf, A.; Narici, M.V.; Fink, C.; Braun, S.; Hoser, C.; Blazevich, A.J.; Csapo, R. Remodeling the Skeletal Muscle Extracellular Matrix in Older Age—Effects of Acute Exercise Stimuli on Gene Expression. Int. J. Mol. Sci. 2020, 21, 7089. [Google Scholar] [CrossRef]
- Barrachina-Igual, J.; Martínez-Arnau, F.M.; Pérez-Ros, P.; Flor-Rufino, C.; Sanz-Requena, R.; Pablos, A. Effectiveness of the Promufra program in pre-frail, community-dwelling older people: A randomized controlled trial. Geriatr. Nurs. 2020, 42, 582–591. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Jang, I.-Y.; Jung, H.-W.; Lee, H.Y.; Park, H.; Lee, E.; Kim, D.H. Evaluation of Clinically Meaningful Changes in Measures of Frailty. J. Gerontol. A. Biol. Sci. Med. Sci. 2020, 75, 1143–1147. [Google Scholar] [CrossRef]
- Keleszade, E.; Willner, T.; Patterson, M.; Trangmar, S.; Kolida, S.; Costabile, A. A pilot study to assess the effect of a fibre and mineral formulation on satiety and satiation when taken as part of a calorie restriction diet in overweight and obese women. J. Funct. Foods 2020, 74, 104157. [Google Scholar] [CrossRef]
- Brzycki, M. Strength Testing &Ndash; Predicting a One-Rep Max from Reps-to-Fatigue. J. Phys. Educ. Recreat. Amp Danc. 1993, 64, 88–90. [Google Scholar]
- Oliveira, A.; Rebelo, P.; Paixão, C.; Jácome, C.; Cruz, J.; Martins, V.; Simão, P.; Brooks, D.; Marques, A. Minimal Clinically Important Difference for Quadriceps Muscle Strength in People with COPD Following Pulmonary Rehabilitation. COPD 2021, 18, 35–44. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-held dynamometry: A practicable alternative for obtaining objective measures of muscle strength. Isokinet. Exerc. Sci. 2012, 20, 301–315. [Google Scholar] [CrossRef]
- Francis, P.; Toomey, C.; McCormack, W.; Lyons, M.; Jakeman, P. Measurement of maximal isometric torque and muscle quality of the knee extensors and flexors in healthy 50- to 70-year-old women. Clin. Physiol. Funct. Imaging 2016, 37, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Maffiuletti, N.A.; Bizzini, M.; Desbrosses, K.; Babault, N.; Munzinger, U. Reliability of knee extension and flexion measurements using the Con-Trex isokinetic dynamometer. Clin. Physiol. Funct. Imaging 2007, 27, 346–353. [Google Scholar] [CrossRef]
- Horowitz, B.P.; Tollin, R.; Cassidy, G. Grip Strength. Phys. Occup. Ther. Geriatr. 1997, 15, 53–64. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Kashman, N.; Volland, G.; Weber, K.; Dowe, M.; Rogers, S. Grip and pinch strength: Normative data for adults. Arch. Phys. Med. Rehabil. 1985, 66, 69–74. [Google Scholar]
- Casas-Herrero, A.; Izquierdo, M. Ejercicio Físico Como Intervención Eficaz En El Anciano Frágil. An. Sist. Sanit. Navar. 2012, 35, 69–85. [Google Scholar] [CrossRef]
- Van Roie, E.; Delecluse, C.; Coudyzer, W.; Boonen, S.; Bautmans, I. Strength training at high versus low external resistance in older adults: Effects on muscle volume, muscle strength, and force–velocity characteristics. Exp. Gerontol. 2013, 48, 1351–1361. [Google Scholar] [CrossRef]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Ahlers, S.J.G.M.; van der Veen, A.M.; van Dijk, M.; Tibboel, D.; Knibbe, C.A.J. The Use of the Behavioral Pain Scale to Assess Pain in Conscious Sedated Patients. Anesth. Analg. 2010, 110, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellg, A.J.; Borrelli, B.; Resnick, B.; Hecht, J.; Minicucci, D.S.; Ory, M.G.; Ogedegbe, G.; Orwig, D.; Ernst, D.; Czajkowski, S. Enhancing Treatment Fidelity in Health Behavior Change Studies: Best Practices and Recommendations from the NIH Behavior Change Consortium. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2004, 23, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Vellas, B.; Hsu, F.-C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.; Miller, M.E.; et al. A Physical Activity Intervention to Treat the Frailty Syndrome in Older Persons--Results From the LIFE-P Study. J. Gerontol. A. Biol. Sci. Med. Sci. 2014, 70, 216–222. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; 12 Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1988; p. 13. [Google Scholar]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Ota, N.; Shimotoyodome, A.; Hase, T.; Hosoi, E.; Yoshida, H. Effects of Exercise and Milk Fat Globule Membrane (MFGM) Supplementation on Body Composition, Physical Function, and Hematological Parameters in Community-Dwelling Frail Japanese Women: A Randomized Double Blind, Placebo-Controlled, Follow-Up Trial. PLoS ONE 2015, 10, e0116256. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236. [Google Scholar] [CrossRef] [Green Version]
- Serra-Prat, M.; Sist, X.; Domenich, R.; Jurado, L.; Saiz, A.; Roces, A.; Palomera, E.; Tarradelles, M.; Papiol, M. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: A randomised controlled trial. Age Ageing 2017, 46, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Binder, E.F.; Yarasheski, K.E.; Steger-May, K.; Sinacore, D.R.; Brown, M.; Schechtman, K.B.; Holloszy, J.O. Effects of Progressive Resistance Training on Body Composition in Frail Older Adults: Results of a Randomized, Controlled Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1425–1431. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodríguez-Mañas, L.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. AGE 2014, 36, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Seynnes, O.; Singh, M.A.F.; Hue, O.; Pras, P.; Legros, P.; Bernard, P.L. Physiological and Functional Responses to Low-Moderate Versus High-Intensity Progressive Resistance Training in Frail Elders. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M503–M509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Rexach, J.A.; Bustamante-Ara, N.; Villarán, M.H.; Gil, P.G.; Ibáñez, M.J.S.; Bsc, N.B.S.; Bsc, V.O.S.; Bsc, N.G.S.; Bsc, A.B.M.P.; Gallardo, C.; et al. Short-Term, Light- to Moderate-Intensity Exercise Training Improves Leg Muscle Strength in the Oldest Old: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2011, 59, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R.; Meredith, C.N.; O′Reilly, K.P.; Knuttgen, H.G.; Evans, W.J. Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J. Appl. Physiol. 1988, 64, 1038–1044. [Google Scholar] [CrossRef] [PubMed]
- Irina, G.; Refaela, C.; Adi, B.; Avia, D.; Liron, H.; Chen, A.; Gad, S. Low Blood ALT Activity and High FRAIL Questionnaire Scores Correlate with Increased Mortality and with Each Other. A Prospective Study in the Internal Medicine Department. J. Clin. Med. 2018, 7, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| TotalMean (SD) | IGMean (SD) | CGMean (SD) | p-Value | |
|---|---|---|---|---|
| Age, years | 77.56 (7.51) | 78.15 (7.092) | 77.00 (7.92) | 0.484 |
| Female gender, % | 84 | 79.5 | 88.1 | 0.292 |
| CCI, score (0–37) | 5.11 (1.71) | 5.51 (1.95) | 4.73 (1.36) | 0.206 |
| Height, cm | 1.55 (0.08) | 1.55 (0.08) | 1.55 (0.07) | 0.772 |
| BW, kg | 67.96 (12.03) | 65.71 (11.07) | 70.47 (12.72) | 0.094 |
| MM, kg | 40.85 (6.93) | 40.36 (7.64) | 41.40 (6.11) | 0.527 |
| FM, kg | 25.20 (7.73) | 23.28 (6.80) | 27.35 (8.23) | 0.025 * |
| SMMI, kg | 6.56 (1.31) | 6.53 (1.48) | 6.59 (1.10) | 0.844 |
| Frailty status, % | 100 | 46.9 | 53.1 | 0.818 |
| 52.1 | 53.3 | 51.0 | |
| 47.9 | 46.7 | 49.0 | |
| KE, kg | 4.98 (4.18) | 5.22 (4.38) | 4.69 (3.96) | 0.601 |
| LP, kg | 68.24 (22.22) | 66.65 (23.71) | 70.06 (20.57) | 0.523 |
| IKE, kg | 19.98 (6.78) | 20.75 (7.12) | 19.06 (6.34) | 0.317 |
| HG, kg | 22.11 (6.85) | 21.72 (6.77) | 22.54 (7.02) | 0.616 |
| Hip joint | ||||
| 98.01 (20.48) | 97.64 (17.07) | 98.48 (24.47) | 0.871 |
| 68.74 (17.28) | 68.20 (15.85) | 69.42 (19.20) | 0.782 |
| 16.51 (12.60) | 15.13 (12.01) | 18.27 (13.33) | 0.319 |
| Knee joint | ||||
| 113.81 (17.92) | 114.18 (16.22) | 113.34 (20.18) | 0.851 |
| 173.00 (6.33) | 171.25 (6.42) | 175.17 (5.60) | 0.012 * |
| SMNA, score (0–14) | 12.64 (1.83) | 12.43 (2.08) | 12.83 (1.56) | 0.333 |
| PA level, METs | 1011.59 (887.09) | 1122.35 (1037.04) | 908.73 (718.47) | 0.335 |
| Post-Intervention | Pre-Post | Pre-Post | Inter-Group Difference | ||||
|---|---|---|---|---|---|---|---|
| Outcome | Group | Mean (SD) | Mean Difference | 95% CI | F | p-Value | η2p |
| BW, kg | CG | 70.45 (13.11) | 0.02 | −0.59/0.64 | 0.003 | 0.956 | <0.001 |
| IG | 65.66 (11.30) | 0.47 | −0.54/0.63 | ||||
| MM, kg | CG | 40.59 (6.49) | 0.81 | 0.83/1.54 | 6.304 | 0.014 * | 0.083 |
| IG | 40.81 (7.04) | −0.45 | −1.14/0.23 | ||||
| FM, kg | CG | 28.21 (8.95) | −0.85 | −1.75/0.05 | 5.266 | 0.025 * | 0.070 |
| IG | 22.70 (6.84) | 0.57 | −0.27/1.43 | ||||
| SMMI, kg/m2 | CG | 6.47 (1.10) | 0.12 | −0.45/0.29 | 7.624 | 0.007 ** | 0.098 |
| IG | 6.72 (1.32) | −0.19 | −0.35/−0.38 | ||||
| HFBK, ° | CG | 92.00 (13.76) | 6.48 | −0.83/13.79 | 5.486 | 0.022 * | 0.079 |
| IG | 102.62 (14.10) | −4.97 | −11.45/1.50 | ||||
| HFSK, ° | CG | 73.03 (10.04) | −3.60 | −9.60/2.38 | 1.057 | 0.308 | 0. 017 |
| IG | 75.94 (11.50) | −7.74 | −13.10/−2.38 | ||||
| HE, ° | CG | 17.10 (10.60) | 1.17 | −2.57/4.92 | 2.631 | 0.110 | 0.039 |
| IG | 18.02 (9.55) | −2.89 | −6.21/0.42 | ||||
| Knee Flex, ° | CG | 114.72 (18.01) | −1.38 | −6.80/4.04 | 0.895 | 0.348 | 0.014 |
| IG | 119.00 (10.18) | −4.81 | −9.61/−0.007 | ||||
| Knee Ext, ° | CG | 174.51 (4.49) | 0.65 | −2.06/3.37 | 8.115 | 0.006 ** | 0.114 |
| IG | 175.80 (5.65) | −4.55 | −6.99/−2.11 | ||||
| Frailty Status | IG | CG | |||
|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||
| Robust, % | 0 | 26.3 | 0 | 5.9 | |
| Pre-frail, % | 53.8 | 55.3 | 54.8 | 58.8 | |
| Frail, % | 46.2 | 18.4 | 45.2 | 35.3 | |
| Mean adherence | |||||
| Robust, % | HA | 76.18 | |||
| Pre-frail, % | HA | 71.77 | |||
| Frail, % | HA | 62.45 | |||
| Post-Intervention | Pre-Post | Pre-Post | Inter-Group Difference | ||||
|---|---|---|---|---|---|---|---|
| Outcome | Group | Mean (SD) | Mean Difference | 95% CI | F | p-Value | η2p |
| KE, kg | CG | 4.72 (4.38) | −0.02 | −1.51/1.465 | 64.089 | <0.001 *** | 0.482 |
| IG | 13.32 (7.59) | −8.10 | −9.454/−6.75 | ||||
| LP, kg | CG | 65.25 (24.61) | 4.81 | −2.78/12.41 | 38.54 | <0.001 *** | 0.358 |
| IG | 94.18 (24.44) | −27.52 | −34.61/−20.44 | ||||
| IKE, kg | CG | 20.33 (7.86) | −1.27 | −3.81/1.28 | 11.466 | 0.001 ** | 0.152 |
| IG | 27.87 (10.04) | −7.11 | −9.44/−4.78 | ||||
| HG, kg | CG | 21.47 (7.08) | 1.07 | −0.15/2.30 | 10.90 | 0.002 ** | 0.135 |
| IG | 23.44 (7.08) | −1.72 | −2.88/−0.563 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrachina-Igual, J.; Pablos, A.; Pérez-Ros, P.; Flor-Rufino, C.; Martínez-Arnau, F.M. Frailty Status Improvement after 5-Month Multicomponent Program PROMUFRA in Community-Dwelling Older People: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 4077. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144077
Barrachina-Igual J, Pablos A, Pérez-Ros P, Flor-Rufino C, Martínez-Arnau FM. Frailty Status Improvement after 5-Month Multicomponent Program PROMUFRA in Community-Dwelling Older People: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(14):4077. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144077
Chicago/Turabian StyleBarrachina-Igual, Joaquín, Ana Pablos, Pilar Pérez-Ros, Cristina Flor-Rufino, and Francisco M. Martínez-Arnau. 2022. "Frailty Status Improvement after 5-Month Multicomponent Program PROMUFRA in Community-Dwelling Older People: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 14: 4077. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144077