
Association between Metformin Use and Risk of Total Knee Arthroplasty and Degree of Knee Pain in Knee Osteoarthritis Patients with Diabetes and/or Obesity: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
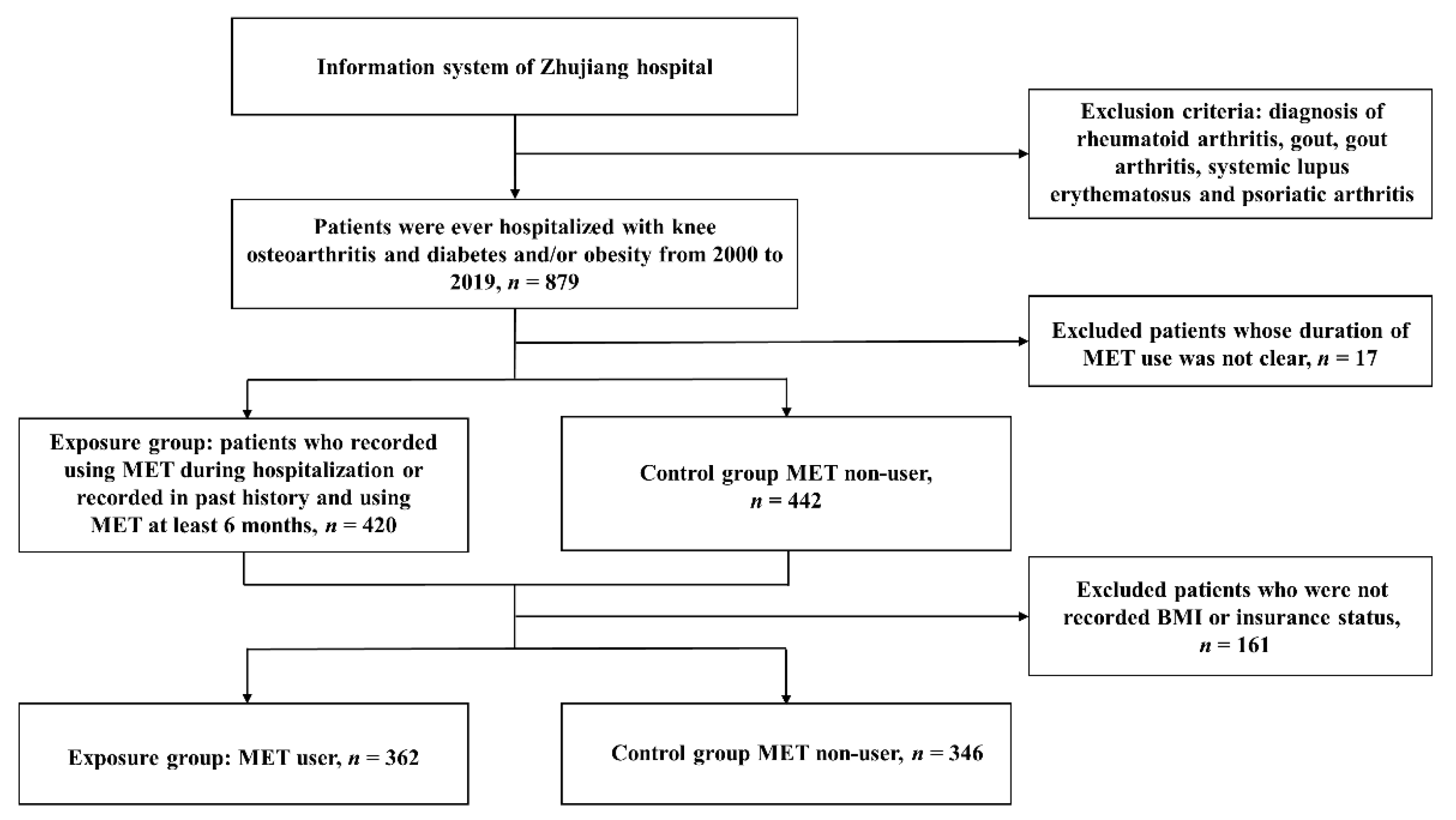
2.1. Participants
2.2. Exposure
2.3. Outcome Assessment
2.3.1. Total Knee Arthroplasty
2.3.2. Knee Pain
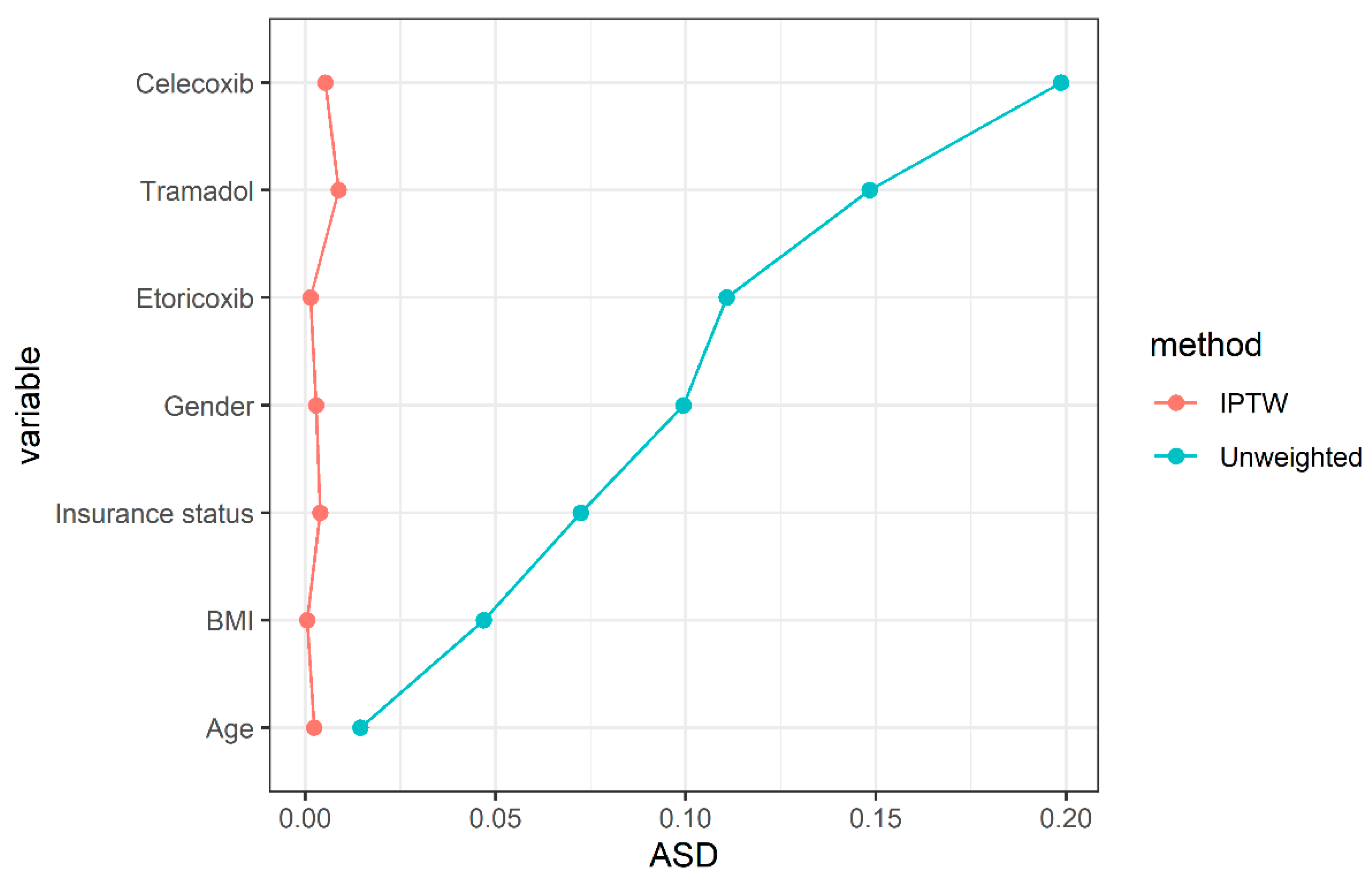
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Associations between MET Use and Risk of TKA and Degree of Knee Pain
3.3. The Accumulative Effect of MET Use on the Risk of TKA and Severity of Knee Pain
3.4. The Dose-Dependent Effect of MET Use on the Risk of TKA and Severity of Knee Pain
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tang, X.; Wang, S.; Zhan, S.; Niu, J.; Tao, K.; Zhang, Y.; Lin, J. The Prevalence of Symptomatic Knee Osteoarthritis in China: Results from the China Health and Retirement Longitudinal Study. Arthritis. Rheumatol. 2016, 68, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Li, J.; Ruan, G.; Wang, G.; Huang, C.; Ding, C. Investigational drugs for the treatment of osteoarthritis, an update on recent developments. Expert. Opin. Investig. Drugs 2018, 27, 881–900. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Ding, C.; Li, T.; Yu, S.P. Current status and future prospects for disease modification in osteoarthritis. Rheumatology 2018, 57, iv108–iv123. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, D., Jr.; Koenig, L.; Dall, T.M.; Gallo, P.; Narzikul, A.; Parvizi, J.; Tongue, J. The direct and indirect costs to society of treatment for end-stage knee osteoarthritis. J. Bone Joint. Surg. Am. 2013, 95, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Knoop, J.; van der Leeden, M.; Thorstensson, C.A.; Roorda, L.D.; Lems, W.F.; Knol, D.L.; Steultjens, M.P.M.; Dekker, J. Identification of phenotypes with different clinical outcomes in knee osteoarthritis: Data from the Osteoarthritis Initiative. Arthritis Care Res. 2011, 63, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Hinman, R.S.; Crossley, K.M. Patellofemoral joint osteoarthritis: An important subgroup of knee osteoarthritis. Rheumatology 2007, 46, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Courties, A.; Sellam, J.; Berenbaum, F. Metabolic syndrome-associated osteoarthritis. Curr. Opin. Rheumatol. 2017, 29, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-H.; Zhao, C.; Liu, B.; Dong, N.; Ding, L.; Li, Y.-R.; Liu, J.-G.; Feng, W.; Qi, X.; Jin, X.-H. An update on the association between metabolic syndrome and osteoarthritis and on the potential role of leptin in osteoarthritis. Cytokine 2020, 129, 155043. [Google Scholar] [CrossRef]
- Yerevanian, A.; Soukas, A.A. Metformin: Mechanisms in Human Obesity and Weight Loss. Curr. Obes. Rep. 2019, 8, 156–164. [Google Scholar] [CrossRef]
- Park, M.J.; Moon, S.J.; Baek, J.A.; Lee, E.J.; Jung, K.A.; Kim, E.K.; Kim, D.S.; Lee, J.H.; Kwok, S.K.; Min, J.K.; et al. Metformin Augments Anti-Inflammatory and Chondroprotective Properties of Mesenchymal Stem Cells in Experimental Osteoarthritis. J. Immunol. 2019, 203, 127–136. [Google Scholar] [CrossRef]
- Li, J.; Zhang, B.; Liu, W.X.; Lu, K.; Pan, H.; Wang, T.; Yi, D.; Huang, J.; Zhao, L.; Ning, G.; et al. Metformin limits osteoarthritis development and progression through activation of AMPK signalling. Ann. Rheum. Dis. 2020, 79, 635–645. [Google Scholar] [CrossRef]
- Guo, H.; Ding, D.; Wang, L.; Yan, J.; Ma, L.; Jin, Q. Metformin attenuates osteoclast-mediated abnormal subchondral bone remodeling and alleviates osteoarthritis via AMPK/NF-κB/ERK signaling pathway. PLoS ONE 2021, 16, e0261127. [Google Scholar] [CrossRef]
- Yan, J.; Ding, D.; Feng, G.; Yang, Y.; Zhou, Y.; Ma, L.; Guo, H.; Lu, Z.; Jin, Q. Metformin reduces chondrocyte pyroptosis in an osteoarthritis mouse model by inhibiting NLRP3 inflammasome activation. Exp. Ther. Med. 2022, 23, 222. [Google Scholar] [CrossRef]
- Yan, J.; Feng, G.; Ma, L.; Chen, Z.; Jin, Q. Metformin alleviates osteoarthritis in mice by inhibiting chondrocyte ferroptosis and improving subchondral osteosclerosis and angiogenesis. J. Orthop. Surg. Res. 2022, 17, 333. [Google Scholar] [CrossRef]
- Lu, C.-H.; Chung, C.-H.; Lee, C.-H.; Hsieh, C.-H.; Hung, Y.-J.; Lin, F.-H.; Tsao, C.-H.; Hsieh, P.-S.; Chien, W.-C. Combination COX-2 inhibitor and metformin attenuate rate of joint replacement in osteoarthritis with diabetes: A nationwide, retrospective, matched-cohort study in Taiwan. PLoS ONE 2018, 13, e0191242. [Google Scholar] [CrossRef]
- Wang, Y.; Hussain, S.M.; Wluka, A.E.; Lim, Y.Z.; Abram, F.; Pelletier, J.-P.; Martel-Pelletier, J.; Cicuttini, F.M. Association between metformin use and disease progression in obese people with knee osteoarthritis: Data from the Osteoarthritis Initiative-a prospective cohort study. Arthritis. Res. Ther. 2019, 21, 127. [Google Scholar] [CrossRef]
- Barnett, L.A.; Jordan, K.P.; Edwards, J.J.; van der Windt, D.A. Does metformin protect against osteoarthritis? An electronic health record cohort study. Prim. Health Care Res. Dev. 2017, 18, 623–628. [Google Scholar] [CrossRef]
- Lim, Y.Z.; Wang, Y.; Estee, M.; Abidi, J.; Kumar, M.U.; Hussain, S.M.; Wluka, A.E.; Little, C.B.; Cicuttini, F.M. Metformin as a potential disease-modifying drug in osteoarthritis: A systematic review of pre-clinical and human studies. Osteoarthr. Cartil. 2022.
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Li, H.; Ding, X.; Terkeltaub, R.; Lin, H.; Zhang, Y.; Zhou, B.; He, K.; Li, K.; Liu, Z.; Wei, J.; et al. Exploration of metformin as novel therapy for osteoarthritis: Preventing cartilage degeneration and reducing pain behavior. Arthritis. Res. Ther. 2020, 22, 34. [Google Scholar] [CrossRef]
- Mohammed, M.; Al-Shamma, K.; Jassim, N. Evaluation of the Clinical use of Metformin or Pioglitazone in Combination with MeloxicAm in Patients with Knee Osteoarthritis; using Knee Injury and Osteoarthritis outcome Score. Iraqi J. Pharm. Sci. 2014, 23, 13–23. [Google Scholar]
- Arai, M.; Uchiba, M.; Komura, H.; Mizuochi, Y.; Harada, N.; Okajima, K. Metformin, an antidiabetic agent, suppresses the production of tumor necrosis factor and tissue factor by inhibiting early growth response factor-1 expression in human monocytes in vitro. J. Pharmacol. Exp. Ther. 2010, 334, 206–213. [Google Scholar] [CrossRef]
- Cameron, A.R.; Morrison, V.; Levin, D.; Mohan, M.; Forteath, C.; Beall, C.; McNeilly, A.; Balfour, D.J.; Savinko, T.; Wong, A.K.; et al. Anti-Inflammatory Effects of Metformin Irrespective of Diabetes Status. Circ. Res. 2016, 119, 652–665. [Google Scholar] [CrossRef]
- Inyang, K.E.; Szabo-Pardi, T.; Wentworth, E.; McDougal, T.A.; Dussor, G.; Burton, M.D.; Price, T.J. The antidiabetic drug metformin prevents and reverses neuropathic pain and spinal cord microglial activation in male but not female mice. Pharmacol. Res. 2019, 139, 1–16. [Google Scholar] [CrossRef]
- Augusto, P.S.; Braga, A.V.; Rodrigues, F.F.; Morais, M.I.; Dutra, M.M.; Batista, C.R.; Melo, I.S.; Costa, S.O.; Goulart, F.A.; Coelho, M.M.; et al. Metformin antinociceptive effect in models of nociceptive and neuropathic pain is partially mediated by activation of opioidergic mechanisms. Eur. J. Pharmacol. 2019, 858, 172497. [Google Scholar] [CrossRef]
- Na, H.S.; Kwon, J.Y.; Lee, S.-Y.; Lee, S.H.; Lee, A.R.; Woo, J.S.; Jung, K.; Cho, K.-H.; Choi, J.-W.; Lee, D.H.; et al. Metformin Attenuates Monosodium-Iodoacetate-Induced Osteoarthritis via Regulation of Pain Mediators and the Autophagy-Lysosomal Pathway. Cells 2021, 10, 681. [Google Scholar] [CrossRef]
- Klop, C.; de Vries, F.; Lalmohamed, A.; Mastbergen, S.C.; Leufkens, H.G.; Noort-van der Laan, W.H.; Bijlsma, J.W.; Welsing, P.M. COX-2-selective NSAIDs and risk of hip or knee replacements: A population-based case-control study. Calcif. Tissue Int. 2012, 91, 387–394. [Google Scholar] [CrossRef]
- Dorais, M.; Martel-Pelletier, J.; Raynauld, J.P.; Delorme, P.; Pelletier, J.P. Impact of oral osteoarthritis therapy usage among other risk factors on knee replacement: A nested case-control study using the Osteoarthritis Initiative cohort. Arthritis. Res. Ther. 2018, 20, 172. [Google Scholar] [CrossRef]
- Hafezi-Nejad, N.; Guermazi, A.; Roemer, F.W.; Eng, J.; Zikria, B.; Demehri, S. Long term use of analgesics and risk of osteoarthritis progressions and knee replacement: Propensity score matched cohort analysis of data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2016, 24, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Adili, A.; Winemaker, M.; Bhandari, M. Management of osteoarthritis of the knee in younger patients. CMAJ 2018, 190, E72–E79. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Bhala, N.; Emberson, J.; Merhi, A.; Abramson, S.; Arber, N.; Baron, J.A.; Bombardier, C.; Cannon, C.; Farkouh, M.E.; FitzGerald, G.A.; et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: Meta-analyses of individual participant data from randomised trials. Lancet 2013, 382, 769–779. [Google Scholar]
- Gregori, D.; Giacovelli, G.; Minto, C.; Barbetta, B.; Gualtieri, F.; Azzolina, D.; Vaghi, P.; Rovati, L.C. Association of Pharmacological Treatments with Long-term Pain Control in Patients with Knee Osteoarthritis: A Systematic Review and Meta-analysis. JAMA 2018, 320, 2564–2579. [Google Scholar] [CrossRef]
- Bahrambeigi, S.; Yousefi, B.; Rahimi, M.; Shafiei-Irannejad, V. Metformin; an old antidiabetic drug with new potentials in bone disorders. Biomed. Pharmacother. 2019, 109, 1593–1601. [Google Scholar] [CrossRef]
- He, Y.; Ren, E.; Lu, Z.; Chen, H.; Qin, Z.; Wang, J.; He, M.; Liu, G.; Zheng, L.; Zhao, J. Rational engineering of ferritin nanocages for targeted therapy of osteoarthritis. Nanomedicine 2020, 28, 102210. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before IPTW | After IPTW | |||||
|---|---|---|---|---|---|---|
| Non-MET (n = 442) | MET (n = 420) | ASD ‡ | Non-MET (n = 346) | MET (n = 362) | ASD | |
| Age | 73.8 ± 11.0 | 73.6 ± 10.3 | 0.014 | 72.7 ± 10.7 | 72.7 ± 10.1 | 0.002 |
| Female | 79% | 73% | 0.099 | 77% | 77% | 0.003 |
| BMI, kg/m2 | 25.87 ± 4.3 | 25.9 ± 4.2 | 0.027 | 25.8 ± 4.4 | 25.8 ± 4.3 | <0.001 |
| Rural cooperative medical care system † | 79% | 82% | 0.072 | 82% | 82% | 0.004 |
| Celecoxib | 51% | 61% | 0.199 | 58% | 58% | 0.005 |
| Etoricoxib | 20% | 25% | 0.111 | 24% | 24% | 0.001 |
| Tramadol | 16% | 11% | 0.148 | 14% | 13% | 0.009 |
| No. (Rate %) of TKA | PR (95% CI) | Mean ± SD of Knee Pain | β (95% CI) | |||
|---|---|---|---|---|---|---|
| MET Non-Users | MET Users | MET Non-Users | MET Users | |||
| Univariable † | 83 (19%) | 21 (5%) | 0.23 (0.13, 0.37) | 2.1 ± 1.7 | 1.6 ± 1.9 | −0.54 (−0.93, −0.14) |
| Multivariable ‡ | 72 (21%) | 20 (6%) | 0.26 (0.15, 0.45) | 2.1 ± 1.7 | 1.6 ± 1.9 | −0.48 (−0.91, −0.05) |
| IPTW § | 72 (21%) | 20 (6%) | 0.29 (0.17, 0.49) | 2.1 ± 1.7 | 1.6 ± 1.9 | −0.49 (−0.94, −0.05) |
| MET Duration a | Number | TKA, No. (%) | Univariable † | Multivariable ‡ | IPTW § | |||
|---|---|---|---|---|---|---|---|---|
| PR (95% CI) | p | PR (95% CI) | p | PR (95%CI) | p | |||
| 0 | 442 | 83 (18.8) | Reference | Reference | Reference | |||
| 1 | 210 | 14 (6.7) | 0.31 (0.16, 0.54) | <0.001 | 0.37 (0.18, 0.69) | 0.003 | 0.44 (0.23, 0.84) | 0.014 |
| 2 | 210 | 7 (3.4) | 0.15 (0.06, 0.31) | <0.001 | 0.17 (0.07, 0.36) | <0.001 | 0.17 (0.07, 0.37) | <0.001 |
| p for trend | <0.001 | <0.001 | ||||||
| MET Duration a | Number | Knee Pain (Mean ± SE) | Univariable † | Multivariable ‡ | IPTW § | |||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |||
| 0 | 155 | 2.1 ± 0.1 | Reference | Reference | Reference | |||
| 1 | 94 | 1.6 ± 0.2 | −0.53 (−0.98, −0.09) | 0.020 | −0.51 (−1.00, −0.02) | 0.042 | −0.39 (−0.91, 0.13) | 0.141 |
| 2 | 47 | 1.6 ± 0.3 | −0.55 (−1.12, 0.03) | 0.065 | −0.43 (−1.03, 0.17) | 0.164 | −0.50 (−1.14, 0.13) | 0.124 |
| p for trend | 0.017 | 0.062 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Ruan, G.; Zeng, M.; Chen, T.; Cao, P.; Zhang, Y.; Li, J.; Wang, X.; Li, S.; Tang, S.; et al. Association between Metformin Use and Risk of Total Knee Arthroplasty and Degree of Knee Pain in Knee Osteoarthritis Patients with Diabetes and/or Obesity: A Retrospective Study. J. Clin. Med. 2022, 11, 4796. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164796
Chen S, Ruan G, Zeng M, Chen T, Cao P, Zhang Y, Li J, Wang X, Li S, Tang S, et al. Association between Metformin Use and Risk of Total Knee Arthroplasty and Degree of Knee Pain in Knee Osteoarthritis Patients with Diabetes and/or Obesity: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(16):4796. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164796
Chicago/Turabian StyleChen, Shibo, Guangfeng Ruan, Muhui Zeng, Tianyu Chen, Peihua Cao, Yan Zhang, Jia Li, Xiaoshuai Wang, Shengfa Li, Su’an Tang, and et al. 2022. "Association between Metformin Use and Risk of Total Knee Arthroplasty and Degree of Knee Pain in Knee Osteoarthritis Patients with Diabetes and/or Obesity: A Retrospective Study" Journal of Clinical Medicine 11, no. 16: 4796. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11164796