
Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature

 ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
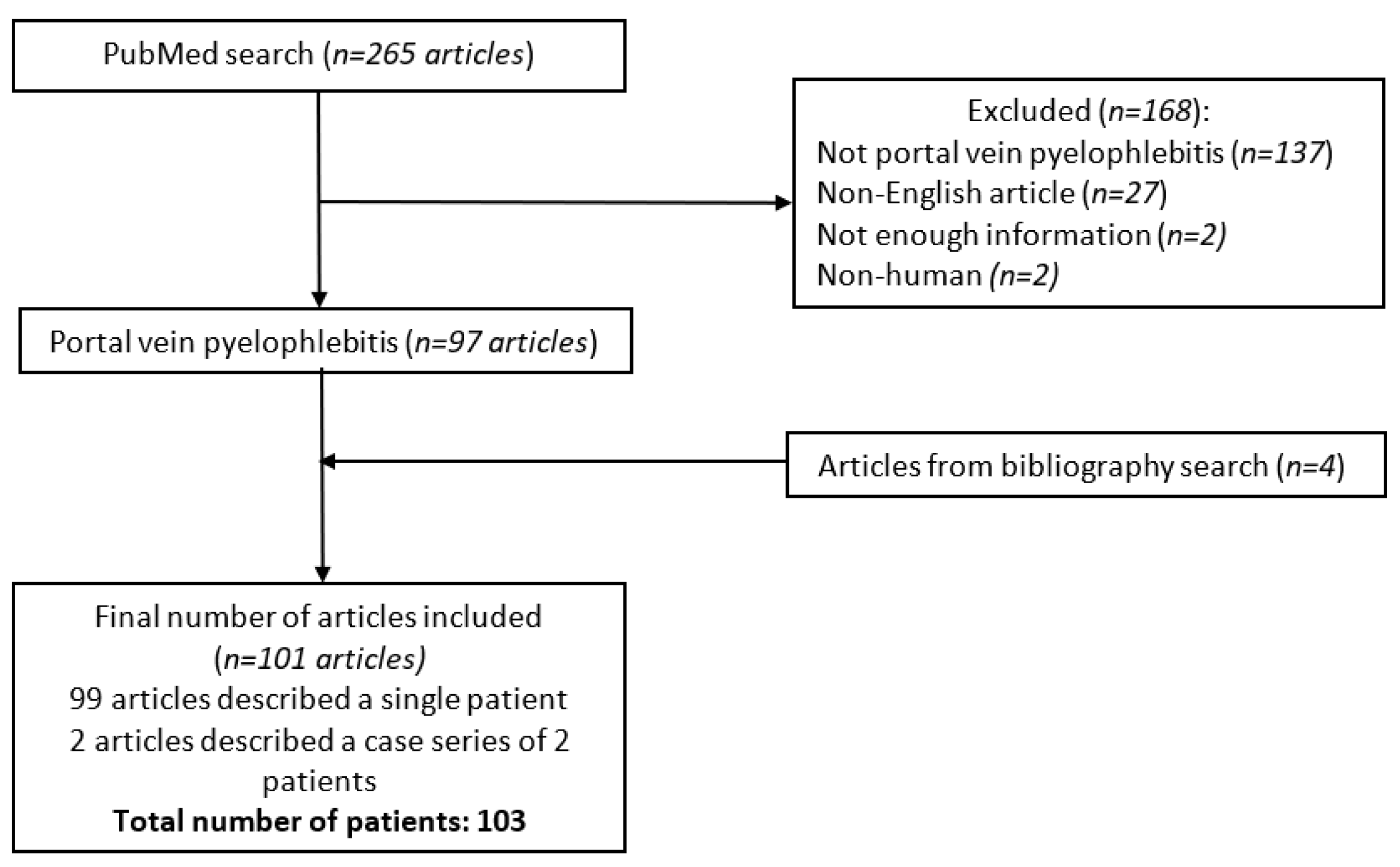
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Types of Infection
3.3. Clinical Presentation
3.4. Thrombosis Site and Characteristics
3.5. Imaging Modalities
3.6. Treatment
3.7. Complications and Outcome
3.8. Pediatric Population
4. Discussion
4.1. Epidemiology
4.2. Microbiology
4.3. Clinical Presentation
4.4. Radiological Findings
4.5. Treatment
4.6. Complications and Outcome
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Naymagon, L.; Tremblay, D.; Schiano, T.; Mascarenhas, J. The role of anticoagulation in pylephlebitis: A retrospective examination of characteristics and outcomes. J. Thromb. Thrombolysis 2020, 49, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulou, T.; Alexopoulou, A.; Theodossiades, G.; Koskinas, J.; Archimandritis, A.J. Pylephlebitis: An overview of non-cirrhotic cases and factors related to outcome. Scand. J. Infect. Dis. 2010, 42, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, A.J.; Baghdadi, Y.M.; Amr, M.A.; Alzghari, M.J.; Jenkins, D.H.; Zielinski, M.D. Pylephlebitis: A Review of 95 Cases. J. Gastrointest. Surg. 2016, 20, 656–661. [Google Scholar] [CrossRef]
- Phoompoung, P.; Chayakulkeeree, M.; Ngamskulrungroj, P.; Pongpaibul, A. Asymptomatic Histoplasma Pylephlebitis in an Orthotopic Liver Transplant Recipient: A Case Report and Literature Review. Mycopathologia 2019, 184, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Lauretta, A.; Almoudaris, A.M.; Jiao, L.R. Septic thrombophlebitis of portal vein: Unusual presentation of appendicitis. Am. Surg. 2011, 77, E206–E207. [Google Scholar] [CrossRef] [PubMed]
- Szanto, P.; Vasile, T.; Ciobanu, L.; Munteanu, D.; Badea, R. Ingested foreign body causing pylephlebitis identified by trans-abdominal ultrasound. Balkan Med. J. 2016, 33, 587–588. [Google Scholar] [CrossRef] [PubMed]
- Tharu, B.; Nigussie, B.; Woredekal, D.; Abaleka, F.I.; Gizaw, M. A Sporadic Case of Disseminated Fusobacterium Causing Pylephlebitis and Intracranial and Hepatic Abscesses in a Healthy Young Patient. Cureus 2020, 12, e9229. [Google Scholar] [PubMed]
- Rea, J.D.; Jundt, J.P.; Jamison, R.L. Pylephlebitis: Keep it in your differential diagnosis. Am. J. Surg. 2010, 200, e69–e71. [Google Scholar] [CrossRef]
- Ogah, K.; Sethi, K.; Karthik, V. Clostridium clostridioforme liver abscess complicated by portal vein thrombosis in childhood. J. Med. Microbiol. 2012, 61, 297–299. [Google Scholar] [CrossRef]
- Hakeem, A.R.; Nasim, N.; Raza, S.S.; Ahmad, N. Portal pyaemia following renal transplantation. BMJ Case Rep. 2014, 2014, bcr2014204026. [Google Scholar] [CrossRef] [Green Version]
- Bockmeyer, J.; Taha-Mehlitz, S.; Heeren, N.; Ristic, S.; Metzger, J.; Gass, J.-M. Jejunal Diverticulosis Probably Leading to Pylephlebitis of the Superior Mesenteric Vein. Case Rep. Surg. 2020, 2020, 2343218. [Google Scholar] [CrossRef]
- Shin, A.R.; Lee, C.K.; Kim, H.J.; Shim, J.-J.; Jang, J.Y.; Dong, S.H.; Kim, B.H.; Chang, Y.W. Septic Pylephlebitis as a Rare Complication of Crohn’s Disease. Korean J. Gastroenterol. 2013, 61, 219–224. [Google Scholar] [CrossRef]
- Karam, M.M.; Abdalla, M.F.; Bedair, S. Isolated superior mesenteric venous thrombophlebitis with acute appendicitis. Int. J. Surg. Case Rep. 2013, 4, 432–434. [Google Scholar] [CrossRef]
- Pradka, S.P.; Trankiem, C.T.; Ricotta, J.J. Pylephlebitis and acute mesenteric ischemia in a young man with inherited thrombophilia and suspected foodborne illness. J. Vasc. Surg. 2012, 55, 1769–1772. [Google Scholar] [CrossRef]
- Furuncuoğlu, Y.; Oven, B.B.; Mert, B.; Yilmaz, E.C.; Demir, M.K. Abdominal variant of lemierre’s syndrome in a patient with pancreatic adenocarcinoma. Medeni. Med. J. 2021, 36, 58–62. [Google Scholar]
- Falkowski, A.L.; Cathomas, G.; Zerz, A.; Rasch, H.; Tarr, P.E. Pylephlebitis of a variant mesenteric vein complicating sigmoid diverticulitis. J. Radiol. Case Rep. 2014, 8, 37–45. [Google Scholar] [CrossRef]
- Mailleux, P.; Maldague, P.; Coulier, B. Pylephlebitis complicating peridiverticulitis without hepatic abscess: Early detection with contrast-enhanced CT of the abdomen. JBR-BTR 2012, 95, 13–14. [Google Scholar]
- Zimhony, O.; Katz, M. A patient with fever and jaundice. QJM 2012, 105, 381–382. [Google Scholar] [CrossRef]
- Gajendran, M.; Muniraj, T.; Yassin, M. Diverticulitis complicated by pylephlebitis: A case report. J. Med. Case Rep. 2011, 5, 514. [Google Scholar] [CrossRef]
- Ozawa, K.; Shikino, K. Pylephlebitis due to acute cholecystitis and cholangitis. BMJ Case Rep. 2021, 14, e244912. [Google Scholar] [CrossRef]
- Sapmaz, F.; Kalkan, I.H.; Guliter, S.; Bilgili, Y.K. Acute cholecystitis complicated by pylephlebitis. Turk. J. Gastroenterol. 2014, 25, 266–267. [Google Scholar] [CrossRef] [PubMed]
- Milner, D.A.; Chatterjee, A. A case of portal vein thrombosis caused by ingestion of a foreign body. Gastrointest. Endosc. 2011, 74, 1168–1170. [Google Scholar] [CrossRef]
- Rustagi, T.; Uy, E.M.; Rai, M. Pyogenic liver abscesses secondary to pylephlebitis complicating acute on chronic pancreatitis. J. Dig. Dis. 2012, 13, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Jadrijević, S.; Sef, D.; Kocman, B.; Mrzljak, A.; Matasic, H.; Škegro, D. Right hepatectomy due to portal vein thrombosis in vasculobiliary injury following laparoscopic cholecystectomy: A case report. J. Med. Case Rep. 2014, 8, 412. [Google Scholar] [CrossRef] [PubMed]
- De Zylva, J.; Padley, J.; Badbess, R.; Dedigama, M. Multiorgan failure following gastroenteritis: A case report. J. Med. Case Rep. 2020, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- L’Ollivier, C.; Eldin, C.; Lambourg, E.; Brouqui, P.; Lagier, J.C. Case Report: First Molecular Diagnosis of Liver Abscesses Due to Fasciola hepatica Acute Infection Imported from Vietnam. Am. J. Trop. Med. Hyg. 2020, 102, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Davarpanah, A.H.; Eberhardt, L.W. Case 282: Fishbone Pylephlebitis. Radiology 2020, 297, 239–243. [Google Scholar] [CrossRef]
- Al Hajjar, N.; Crişan, D.; Grigorescu, M.; Boruah, P. Acute diverticulitis—An unusual cause of liver abcesses in a young man: A case report. Chirurgia 2012, 107, 267–272. [Google Scholar]
- Tang, R.; Tian, X.; Xie, X.; Yang, Y. Intestinal Infarction Caused by Thrombophlebitis of the Portomesenteric Veins as a Complication of Acute Gangrenous Appendicitis After Appendectomy: A Case Report. Medicine 2015, 94, e1033. [Google Scholar] [CrossRef]
- Lim, E.Y.T.; Taneja, R. Thrombophlebitis of abdominal veins as an unusual cause for acute abdomen: Avoiding the diagnostic pitfalls. Emerg. Radiol. 2021, 28, 187–192. [Google Scholar] [CrossRef]
- Granero Castro, P.; Raposo Rodríguez, L.; Moreno Gijón, M.; Prieto Fernández, A.; Granero Trancón, J.; González González, J.J.; Barneo Serra, L. Pylephlebitis as a complication of acute appendicitis. Rev. Esp. Enferm. Dig. 2010, 102, 217–218. [Google Scholar] [CrossRef]
- Coyne, C.J.; Jain, A. Pylephlebitis in a previously healthy emergency department patient with appendicitis. West J. Emerg. Med. 2013, 14, 428–430. [Google Scholar] [CrossRef]
- Altamirano, J.; Zapata, L.; Poblano, M.; Rodríguez, A.; Camargo, L.; Martínez, B.; Bataller, R. Acute pylephlebitis following gastrointestinal infection: An unrecognized cause of septic shock. South Med. J. 2010, 103, 956–959. [Google Scholar] [CrossRef]
- Wang, W.; Chen, S.; Li, W.; Qu, J. An unusual increase of D-dimer level-pylephlebitis caused by acute appendicitis: A case report. Ann. Palliat. Med. 2021, 10, 4917–4921. [Google Scholar] [CrossRef]
- Wong, K.; Weisman, D.S.; Patrice, K.-A. Pylephlebitis: A rare complication of an intra-abdominal infection. J. Community Hosp. Intern. Med. Perspect. 2013, 3, 20732. [Google Scholar] [CrossRef]
- Figueiras, R.G.; Paz, M.L.; González, S.B.; Martín, C.V. Case 158: Pylephlebitis. Radiology 2010, 255, 1003–1007. [Google Scholar] [CrossRef]
- Yamashita, T.; Yamanaka, K.; Izumi, A.; Matsui, J.; Kurimoto, M.; Aoki, H.; Tamura, J. Endovascular repair using a covered stent for a ruptured infected aneurysm of the superior mesenteric artery after pancreaticoduodenectomy: A case report. Surg. Case Rep. 2020, 6, 270. [Google Scholar] [CrossRef]
- Gilany, N.; Iqbal, J. Simulation of Glacial Avalanche Hazards in Shyok Basin of Upper Indus. Sci. Rep. 2019, 9, 20077. [Google Scholar] [CrossRef]
- De Jong, I.M.; Muller, M.C.A.; Peterson, G.; Polle, S.W. An uncommon cause of portal vein thrombosis. Neth. J. Med. 2013, 71, 431–435. [Google Scholar]
- El Mouhadi, S.; Ait-Oufella, H.; Maury, É.; Menu, Y.; Arrivé, L. Ileal diverticulitis complicated by portal-mesenteric pylephlebitis and pulmonary septic foci. Diagn. Interv. Imaging 2012, 93, 57–59. [Google Scholar] [CrossRef]
- Warren, L.R.; Chandrasegaram, M.D.; Madigan, D.J.; Dolan, P.M.; Neo, E.L.; Worthley, C.S. Falciform ligament abscess from left sided portal pyaemia following malignant obstructive cholangitis. World J. Surg. Oncol. 2012, 10, 278. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M.; Verso, C.L.; Serra, G.; Moceri, G.; Cimador, M.; Corsello, G. Portal Vein Thrombosis in a Preterm Newborn with Mutation of the MTHFR and PAI-1 Genes and Sepsis by Candida parapsilosis. Am. J. Perinatol. 2016, 33, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Fukahori, M.; Shirayama, S.; Kawasaki, A.; Takasugi, T.; Sano, H.; Iwasaki, H. A case of silent perforated diverticulitis in the ascending colon combined with pylephlebitis resulting in complete occlusion of the portal trunk. Clin. J. Gastroenterol. 2015, 8, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Řezáč, T.; Zbořil, P.; Vomáčková, K.; Špička, P. A biliary tract obstruction complicated by acute appendicitis and portal vein thrombosis-a case report and review of literature. Int. J. Surg. Case Rep. 2021, 84, 106140. [Google Scholar] [CrossRef] [PubMed]
- Castro, R.; Fernandes, T.; Oliveira, M.I.; Castro, M. Acute Appendicitis Complicated by Pylephlebitis: A Case Report. Case Rep. Radiol. 2013, 2013, 627521. [Google Scholar] [CrossRef] [PubMed]
- Kashiura, M.; Tanabe, T.; Akashi, A.; Hamabe, Y. Pylephlebitis: A Severe Complication of Intra-abdominal Infection. Intern. Med. 2014, 53, 2829. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, R.; Natarajan, A.; Krishna, S.; Thangavelu, S. Portal pyaemia secondary to open haemorrhoidectomy: Need for prophylactic broad spectrum antibiotics. BMJ Case Rep. 2013, 2013, bcr2013200222. [Google Scholar] [CrossRef] [PubMed]
- Wakui, N.; Takayama, R.; Matsukiyo, Y.; Shinohara, M.; Kobayashi, S.; Kanekawa, T.; Nakano, S.; Nagai, H.; Kudo, T.; Maruyama, K.; et al. Visualization of segmental arterialization with arrival time parametric imaging using Sonazoid-enhanced ultrasonography in portal vein thrombosis: A case report. Exp. Ther. Med. 2013, 5, 673–677. [Google Scholar] [CrossRef]
- Wali, L.; Shah, A.; Sleiman, S.; Hogsand, T.; Humphries, S. Acute pylephlebitis secondary to perforated sigmoid diverticulitis: A case report. Radiol. Case Rep. 2021, 16, 1504–1507. [Google Scholar] [CrossRef]
- Menclova, K.; Parobkova, H.; Murinova, I.; Pudil, J.; Langer, D.; Ryska, M. Pylephlebitis in patient with covered perforated rectosigmoid cancer. Rozhl. Chir. 2014, 93, 507–511. [Google Scholar]
- Garrett, A.; Carnish, E.; Das, N.; Slome, M.; Measley, R. Once universally fatal: Pylephlebitis. Am. J. Med. 2014, 127, 595–597. [Google Scholar] [CrossRef]
- Bakti, N.; Hussain, A.; El-Hasani, S. A rare complication of acute appendicitis: Superior mesenteric vein thrombosis. Int. J. Surg. Case Rep. 2011, 2, 250–252. [Google Scholar] [CrossRef]
- Kenny, C.; Sohan, O.; Murray, L.; Fox, T.P. Branch portal vein pyaemia secondary to amoebic liver abscess. BMJ Case Rep. 2015, 2015, bcr2014209098. [Google Scholar] [CrossRef]
- Lee, B.K.; Ryu, H.H. A case of pylephlebitis secondary to cecal diverticulitis. J. Emerg. Med. 2012, 42, e81–e85. [Google Scholar] [CrossRef]
- Gallinger, Z.R.; May, G.; Kortan, P.; Bayoumi, A.M. Pylephlebitis After Colonic Polypectomy Causing Fever and Abdominal Pain. ACG Case Rep. J. 2015, 2, 142–145. [Google Scholar] [CrossRef]
- Hale, G.R.; Sakkal, L.A.; Galanis, T. Pylephlebitis treated with apixaban. Hosp. Prac. 2019, 47, 192–195. [Google Scholar] [CrossRef]
- Meersseman, W. Candida tropicalis pylephlebitis with persistent fungaemia in a 72-year-old lady with severe pancreatitis. Mycoses 2011, 54, 28–30. [Google Scholar] [CrossRef]
- Shahani, L.; Khardori, N. Fusobacterium necrophorum—Beyond Lemierres syndrome. BMJ Case Rep. 2011, 2011, bcr0720114527. [Google Scholar] [CrossRef]
- Tamaki, I.; Kami, K.; Yamamoto, E.; Morimoto, T. Catheter-directed thrombolysis through the operatively recanalized umbilical vein for acute extensive portal vein thrombosis: Report of a case. Clin. J. Gastroenterol. 2014, 7, 376–380. [Google Scholar] [CrossRef]
- Lazar, N.; Sardarli, K.; Imam, Z.; Khasawneh, M.; Hader, I. A Rare Twist of the Forgotten Disease: A Case of Fusobacterium necrophorum Sepsis with Portomesenteric Thrombosis and a Review of the Literature. Case Rep. Gastrointest. Med. 2021, 2021, 6699867. [Google Scholar] [CrossRef]
- Serracant-Barrera, A.; Llaquet-Bayo, H.; Sánchez-Delgado, J.; Romaguera-Monzonis, A.; Dalmau-Obrador, B.; Bejarano-González, N.; Navas-Pérez, A.M.; Llopart-Valdor, E.; García-Borobia, F.J.; Navarro-Soto, S. Pylephlebitis and liver abscesses secondary to acute advanced appendicitis. Rev. Esp. Enferm. Dig. 2015, 107, 397–398. [Google Scholar] [PubMed]
- Hadano, Y.; Iwata, H. Septic thrombophlebitis of the superior mesenteric vein with bacteraemia caused by Bacteroides fragilis and Streptococcus intermedius as a complication of diverculitis. BMJ Case Rep. 2013, 2013, bcr2013008661. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sung, K.; Cho, J. Retroperitoneal abscess with pylephlebitis caused by lumbar acupuncture: A case report. BMC Surg. 2019, 19, 145. [Google Scholar] [CrossRef] [PubMed]
- Al Akhrass, F.; Abdallah, L.; Berger, S.; Sartawi, R. Gastrointestinal variant of Lemierre’s syndrome complicating ruptured appendicitis. IDCases 2015, 2, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, S.; França, N.J.; Mineiro, F.; Capela, G.; Duarte, C.; Mendes, A.R. Pylephlebitis—A rare complication of a fish bone migration mimicking metastatic pancreatic cancer: A case report. World J. Clin. Cases 2021, 9, 6768–6774. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Umeh, C.A.; Giberson, C.; Wassel, E.; Nguyen, A.; Porter, H.; Choday, P.; Kaur, H.; Kundu, A.; Penaherrera, J. Septic Portal Vein Thrombosis, Clinical Presentation, and Management. Cureus 2021, 13, e19840. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, H.; Jindal, P.; Pandiarajan, V.; Kumar, J.; Sudhakar, M.; Ezhumalai, G.; Nada, R.; Gupta, K. Portal vein thrombosis, livedo reticularis, polymicrobial sepsis and high antiphospholipid antibody titers in a newborn: A clinicopathological conference of antiphospholipid-associated neonatal syndrome. Lupus 2021, 30, 141–148. [Google Scholar] [CrossRef]
- Gonzales Zamora, J.A.; Romero Alvarez, M.; Henry, Z.; Baracco, G.J.; Dickinson, G.; Lichtenberger, P. Liver abscess caused by Lawsonella clevelandensis in a patient with rheumatoid arthritis: A case report and literature review. IDCases 2020, 20, e00734. [Google Scholar] [CrossRef]
- Kalbitz, S.; Ermisch, J.; Schmidt, J.M.; Wallstabe, I.; Lübbert, C. Unhappy Triad: Infection with Leptospira spp. Escherichia coli and Bacteroides uniformis Associated with an Unusual Manifestation of Portal Vein Thrombosis. Case Rep. Gastroenterol. 2021, 15, 598–602. [Google Scholar] [CrossRef]
- Yazgan, C.; Akkas, M.; Ozmen, M.M. Inferior mesenteric vein pylephlebitis due to sigmoid diverticulitis. BMJ Case Rep. 2015, 2015, bcr2015212599. [Google Scholar] [CrossRef]
- Cho, E.; Jun, C.H.; Yoon, J.H.; Wi, J.W.; Shin, S.S.; Cho, S.B.; Park, C.H.; Kim, H.S.; Choi, S.K.; Rew, J.S. A Rare Case of Portal Biliopathy and Pylephlebitis Following the Injection of Cyanoacrylate into the Duodenal Varix. J. Clin. Gastroenterol. 2016, 50, 897. [Google Scholar] [CrossRef]
- Shyam, V.; Rana, S.; Kumar, B.V.; Choudhury, A.; Mukund, A. Suppurative Pylephlebitis With Portal Vein Abscess Mimicking Portal Vein Thrombosis: A Report of Two Cases. J. Clin. Exp. Hepatol. 2022, 12, 208–211. [Google Scholar] [CrossRef]
- Adnan, M.M.; Gavin, M.; Eberhardt, S.C.; McCarthy, D.M. Pylephlebitis: Through These Portals Pass Bad Bugs. Am. J. Dig. Dis. 2016, 61, 2807–2811. [Google Scholar] [CrossRef]
- Kashiura, M.; Sugiyama, K.; Akashi, A.; Hamabe, Y. Diverticulitis-induced pylephlebitis possibly misdiagnosed as biliary duct obstruction. Acute Med. Surg. 2016, 3, 404–406. [Google Scholar] [CrossRef]
- Pinto, S.; Lerner, T.; Lingamaneni, G.; Richards, K. Superior mesenteric vein thrombosis as a complication of cecal diverticulitis: A case report. Int. J. Surg. Case Rep. 2016, 25, 71–74. [Google Scholar] [CrossRef] [Green Version]
- Ufuk, F.; Herek, D.; Karabulut, N. Pylephlebitis Complicating Acute Appendicitis: Prompt Diagnosis with Contrast-Enhanced Computed Tomography. J. Emerg. Med. 2016, 50, e147–e149. [Google Scholar] [CrossRef]
- Lawler, C.; King, B.; Milliron, M.L. Portomesenteric Venous Thrombosis in an Emergency Department Patient After Laparoscopic Sleeve Gastrectomy. Cureus 2021, 13, e19872. [Google Scholar] [CrossRef]
- Abdallah, M.; Gohar, A.; Gowda, S.N.; Abdullah, H.M.; Al-Hajjaj, A. Pylephlebitis Associated with Inferior Mesenteric Vein Thrombosis Treated Successfully with Anticoagulation and Antibiotics in a 37-Year-Old Male. Case Rep. Gastrointest. Med. 2020, 2020, 3918080–3918083. [Google Scholar] [CrossRef]
- Queiroz, R.M.; Sampaio, F.D.C.; Marques, P.E.; Ferez, M.A.; Febronio, E.M. Pylephlebitis and septic thrombosis of the inferior mesenteric vein secondary to diverticulitis. Radiol. Bras. 2018, 51, 336–337. [Google Scholar] [CrossRef]
- Bshabshe, A.; Al Joseph, M.R.P.; Battayah, E.S.; Hamid, M.E. Fungal peritonitis caused by Pichia kudriavzevii following sleeve gastrectomy. Ann. Saudi Med. 2019, 39, 205–208. [Google Scholar] [CrossRef]
- Wong, C.S.; Cho, G.; Godfrey, E.M.; Harper, S. Portal pyaemia secondary to colonic perforation. BMJ Case Rep. 2019, 12, e228400. [Google Scholar] [CrossRef]
- Zardi, E.M.; Giorgi, C.; Zardi, D.M. Pylephlebitis as a Complication of Cholangitis and Sepsis in an HIV-Positive Patient. Am. J. Dig. Dis. 2019, 64, 1719–1721. [Google Scholar] [CrossRef]
- Radovanovic, N.; Dumic, I.; Veselinovic, M.; Burger, S.; Milovanovic, T.; Nordstrom, C.W.; Niendorf, E.; Ramanan, P. Fusobacterium necrophorum subsp. necrophorum Liver Abscess with Pylephlebitis: An Abdominal Variant of Lemierre’s Syndrome. Case Rep. Infect. Dis. 2020, 2020, 9237267. [Google Scholar] [CrossRef]
- Kaenkumchorn, T.; Kesavan, A. A Rare Complication of Campylobacter Sepsis in an Infant. Clin. Pediatr. 2018, 57, 484–487. [Google Scholar] [CrossRef]
- Rahmati, E.; She, R.C.; Kazmierski, B.; Geiseler, P.J.; Wong, D. A case of liver abscess and fusobacterium septicemia. IDCases 2017, 9, 98–100. [Google Scholar] [CrossRef]
- Kubo, H.; Asai, G.; Haraguchi, K.; Shibahara, Y.; Kihara, T.; Yamakawa, G.; Kira, F.; Higashi, H.; Morishita, S.; Fujie, H.; et al. Liver Abscess and Portal Vein Thrombosis Due to Ileal Diverticulitis Mediated by Barium Fluoroscopy. Intern. Med. 2017, 56, 3255–3259. [Google Scholar] [CrossRef]
- Moore, J.A.; Rambally, S. Fusobacterium nucleatum Bacteremia Presenting with Portal Vein Thrombosis: An Abdominal Lemierre Syndrome? Am. J. Med. 2017, 130, e255–e256. [Google Scholar] [CrossRef]
- Imaoka, K.; Fukuda, S.; Tazawa, H.; Fukuhara, S.; Hirata, Y.; Fujisaki, S.; Takahashi, M.; Sakimoto, H. A Rare Case of Pylephlebitis as a Complication of Cholecystocolonic Fistula. Case Rep. Surg. 2018, 2018, 3931674. [Google Scholar] [CrossRef]
- Ackermann, T.; D’Souza, D.; Varma, P.; Burnes, J.; Croagh, D. A minimally invasive solution for a complication of minimally invasive treatment. ANZ J. Surg. 2018, 88, 1079–1081. [Google Scholar] [CrossRef]
- Hamera, L.; Abraham, S.; Jordan, J. Pylephlebitis as a Rare Complication of Ulcerative Colitis: A Case Report. Cureus 2019, 11, e4792. [Google Scholar] [CrossRef]
- Santosh, D.; Low, G. Pylephlebitis with Liver Abscess Secondary to Chronic Appendicitis: A Radiological Conundrum. J. Clin. Imaging Sci. 2016, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kwon, H.Y.; Durey, A. Thrombophlebitis of superior mesenteric vein with bacteremia of Gemella sanguinis and Streptococcus gordonii. J. Microbiol. Immunol. Infect. 2019, 52, 672–673. [Google Scholar] [CrossRef] [PubMed]
- Nazir, S.; Jehangir, A.; Siddiqui, A.; Tachamo, N.; Lohani, S.; York, E. A rare case of pylephlebitis after colonic polypectomy. J. Community Hosp. Intern. Med. Perspect. 2017, 7, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Khandwala, K.; Ahmed, A.; Abid, S. Migration of Fish Bone Into the Portal Vein Resulting in Pylephlebitis and Pyogenic Liver Abscesses. Am. J. Gastroenterol. 2019, 114, 1414. [Google Scholar] [CrossRef]
- Zia, A.; Sohal, S.; Costas, C. Pylephlebitis: A Case of Inferior Mesenteric Vein Thrombophlebitis in a Patient with Acute Sigmoid Diverticulitis—A Case Report and Clinical Management Review. Case Rep. Infect. Dis. 2019, 2019, 5341281–53412814. [Google Scholar] [CrossRef]
- James, T.W.; Sheikh, S.Z.; McGowan, C.E. Perigastric abscess as a delayed adverse event in endoscopic sleeve gastroplasty. Gastrointest. Endosc. 2019, 89, 890–891. [Google Scholar] [CrossRef]
- Mouat, S.; Bishop, J.; Glamuzina, E.; Chin, S.; Best, E.J.; Evans, H.M. Fatal hyperammonemia associated with disseminated Serratia marcescens infection in a pediatric liver transplant recipient. Pediatr. Transpl. 2018, 22, e13180. [Google Scholar] [CrossRef]
- Chao, G.F.; Hirji, S.; Shikora, S.A. Extensive Thrombus and Brain Microabscesses After Sleeve Gastrectomy. J. Radiol. Case Rep. 2018, 12, 10–17. [Google Scholar] [CrossRef]
- Ram, P.; Lapumnuaypol, K.; Punjabi, C. Diverticular Pylephlebitis and Polymicrobial Septicemia. Case Rep. Infect. Dis. 2017, 2017, 6819474. [Google Scholar] [CrossRef]
- Mellor, T.E.; Mitchell, N.; Logan, J. Lemierre’s syndrome variant of the gut. BMJ Case Rep. 2017, 2017, bcr2017221567. [Google Scholar] [CrossRef]
- Krzak, A.M.; Townson, A.; Malam, Y.; Mathews, J. Diverticulitis complicated by colovenous fistula formation and pylephlebitis. J. Surg. Case Rep. 2022, 2022, rjab591. [Google Scholar] [CrossRef]
- Abughanimeh, O.; Tahboub, M.; Zafar, Y.; Abu Ghanimeh, M. Pylephlebitis Caused by Actinomyces Bacteremia. Cureus 2018, 10, e2887. [Google Scholar] [CrossRef]
- Greene, B.; Jones, D.; Sarrazin, J.; Coburn, N.G. Porta hepatis abscess and portal vein thrombosis following ingestion of a fishbone. BMJ Case Rep. 2019, 12, e227271. [Google Scholar] [CrossRef]
- Stone, N.R.H.; Barrett, J.; Hickish, T.; Dasgupta, D.; Newsholme, W.; Biswas, J.; Martin, T. Bacteroides-Associated Pylephlebitis in a Patient with Strongyloidiasis. Am. J. Trop. Med. Hyg. 2015, 92, 340–341. [Google Scholar] [CrossRef]
- Angus, D.C.; van der Poll, T. Severe sepsis and septic shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef]
- Belhassen-García, M.; Gomez-Munuera, M.; Pardo-Lledias, J.; Velasco-Tirado, V.; Perez-Persona, E.; Galindo-Perez, I.; Alvela-Suárez, L.; Romero-Alegría, A.; Muñoz-Bellvis, L.; Cordero-Sánchez, M. Pylephlebitis: Incidence and prognosis in a tertiary hospital. Enferm. Infecc. Microbiol. Clin. 2014, 32, 350–354. [Google Scholar] [CrossRef]
- Tursi, A. Diverticular disease: A therapeutic overview. World J. Gastrointest. Pharmacol. Ther. 2010, 1, 27. [Google Scholar] [CrossRef]
- Murray, J.L.; Connell, J.L.; Stacy, A.; Turner, K.H.; Whiteley, M. Mechanisms of synergy in polymicrobial infections. J. Microbiol. 2014, 52, 188–199. [Google Scholar] [CrossRef]
- Shah, P.M.; Edwards, B.L.; Dietch, Z.C.; Guidry, C.A.; Davies, S.W.; Hennessy, S.A.; Duane, T.M.; O’Neill, P.J.; Coimbra, R.; Cook, C.H.; et al. Do Polymicrobial Intra-Abdominal Infections Have Worse Outcomes than Monomicrobial Intra-Abdominal Infections? Surg. Infect. 2016, 17, 27. [Google Scholar] [CrossRef]
- Johannesen, K.M.; Bodtger, U. Lemierre’s syndrome: Current perspectives on diagnosis and management. Infect. Drug Resist. 2016, 9, 221–227. [Google Scholar] [CrossRef]
- Balthazar, E.J.; Gollapudi, P. Septic Thrombophlebitis of the Mesenteric and Portal Veins: CT Imaging. J. Comput. Assist. Tomogr. 2000, 24, 755–760. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristics | Number (%) | |
|---|---|---|
| Gender | ||
| Male | 74 (71.8) | |
| Female | 29 (28.2) | |
| Pertinent Comorbidities | ||
| Total | 29 (28.2) | |
| Intra-abdominal surgery | 10 (9.7) | |
| Pancreatitis | 8 (7.8) | |
| Cirrhosis | 5 (4.9) | |
| Thrombophilia | 4 (3.9) | |
| IBD | 2 (1.9) | |
| HCC | 1 (0.9) | |
| Blood cultures | ||
| Positive | 64 (62.1) | |
| Negative | 21 (20.4) | |
| Not reported | 18 (17.5) | |
| Isolated pathogens | ||
| E. coli | 21 (20.4) | |
| Bacteroides spp. | 13 (12.6) | |
| Streptococcus spp. | 12 (11.7) | |
| Fusobacterium spp. | 10 (9.7) | |
| Staphylococcus spp. | 6 (5.8) | |
| Klebsiella spp. | 6 (5.8) | |
| Clostridium spp. | 5 (4.8) | |
| Enterococcus spp. | 5 (4.8) | |
| Candida spp. | 2 (1.9) | |
| Proteus mirabilis | 2 (1.9) | |
| Actinomyces spp.; Micromonas micros; Eggerthella lenta; Gemella sanguinis; Morganella morganii | 1 (0.9) | |
| Sites of infection | ||
| Diverticulitis | 29 (28.2) | |
| Appendicitis | 20 (19.4) | |
| Hepatic abscess | 8 (7.8) | |
| Pancreatitis | 6 (5.8) | |
| Cholangitis | 6 (5.8) | |
| Cholecystitis; colitis; foreign object ingestion; intra-abdominal surgery | 4(3.9) | |
| Odontogenic bacteria | 3 (2.9) | |
| Perisplenic abscess | 2 (1.9) | |
| Retroperitoneal abscess; jejunitis; bowel ischemia | 1 (0.9) | |
| Signs and symptoms | ||
| Fever | 89 (86.4) | |
| Abdominal pain | 81 (78.6) | |
| Sepsis/septic shock | 60 (58.3) | |
| Diarrhea | 27 (26.2) | |
| Vomiting | 24 (23.3) | |
| Jaundice | 21 (20.4) | |
| Anorexia | 19 (18.4) | |
| Nausea | 15 (14.6) | |
| Hepatomegaly | 10 (9.7) | |
| Ascites | 8 (7.8) | |
| Splenomegaly | 7 (6.8) | |
| GI bleeding | 5 (4.9) | |
| Laboratory findings | ||
| High CRP | 40/44 (90.9) | |
| Leukocytosis | 78/87 (89.7) | |
| High ESR | 12/14 (85.7) | |
| Hyperbilirubinemia | 44/59 (74.6) | |
| Increased AST, ALT | 53/74 (71.6) | |
| Hypoalbuminemia | 11/16 (68.8) | |
| Thrombocytopenia | 19/30 (63.3) | |
| Anemia | 25/42 (59.5) | |
| Treatments | Duration *** | |
| Antimicrobials | 97 (94.2) | 25.9 (1–120) |
| Anticoagulation | 79 (76.7) | 128.7 (1–365) |
| Heparin | 29 (28.2) | |
| Warfarin | 24 (23.3) | |
| LMWH | 24 (23.3) | |
| Xa inhibitors | 12 11.7) | |
| Antithrombin III | 6 (5.8) | |
| Other **** | 5 (4.9) | |
| Acenocoumarol | 3 (2.9) | |
| Outcome | ||
| Alive | 89 (86.4) | |
| Dead | 9 (8.7) | |
| Unknown | 5 (4.9) |
| Imaging | Number (%) |
|---|---|
| CT | 92 (89.3) |
| US | 40 (38.8) |
| MRI | 19 (18.4) |
| Site of thrombosis | |
| Main PV | 59 (57.3) |
| SMV | 40 (38.8) |
| Right branch PV | 30 (29.1) |
| Left branch PV | 25 (24.3) |
| Splenic vein | 13 (12.6) |
| IMV | 10 (9.7) |
| Umbilical veins | 1 (0.9) |
| Occlusive thrombosis | |
| Yes | 26 (25.2) |
| No | 16 (15.6) |
| Not reported | 61 (59.2) |
| Thrombosis resolution | |
| Yes | 25 (24.3) |
| No | 17 (16.5) |
| Partial | 5 (4.9) |
| Unknown | 56 (54.3) |
| Variables | Alive n (%) or Mean ± SD | Died n (%) or Mean ± SD | Univariate p-Value | Multivariate OR | Multivariate p-Value |
|---|---|---|---|---|---|
| Gender Female Male Age, years Pertinent comorbidities No Yes Diverticulitis as a cause No Yes Appendicitis as a cause No Yes Isolated bacteria No Yes Number of bacteria isolated Mono- or polymicrobial infection Monomicrobial Polymicrobial Sepsis No Yes Number of thrombosis sites Occlusive thrombosis No Yes Anticoagulation No Yes | 26 (29.2) 63 (70.8) 49.14 ± 19.57 68 (76.4) 21 (23.6) 63 (70.8) 26 (29.5) 71 (79.8) 18 (20.2) 17 (23.3) 56 (76.7) 1.48 ± 0.68 35 (62.5) 21 (37.5) 13 (20.6) 50 (79.4) 1.77 ± 0.95 14 (36.8) 24 (63.2) 8 (10.3) 70 (89.7) | 3 (33.3) 6 (66.7) 42.39 ± 28.62 3 (33.3) 6 (66.7) 7 (77.8) 2 (22.2) 9 (100.0) 0 (0.0) 3 (37.5) 5 (62.5) 2.40 ± 1.14 1 (20.1) 4 (80.0) 1 (11.1) 8 (88.9) 1.44 ± 0.72 1 (50.0) 1 (50.0) 1 (14.3) 6 (85.7) | 0.796 * 0.348 ** 0.006 * 0.658 * 0.135 * 0.376 * 0.009 ** 0.064 * 0.042 * 0.314 ** 0.708 * 0.740 * | 2.428 0.967 5.500 1.598 0.000 2.215 13.784 0.403 17.182 0.512 0.321 1.080 | 0.258 0.234 0.021 0.748 0.998 0.022 0.085 0.727 0.049 0.533 0.447 0.948 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jevtic, D.; Gavrancic, T.; Pantic, I.; Nordin, T.; Nordstrom, C.W.; Antic, M.; Pantic, N.; Kaljevic, M.; Joksimovic, B.; Jovanovic, M.; et al. Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature. J. Clin. Med. 2022, 11, 4992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11174992
Jevtic D, Gavrancic T, Pantic I, Nordin T, Nordstrom CW, Antic M, Pantic N, Kaljevic M, Joksimovic B, Jovanovic M, et al. Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature. Journal of Clinical Medicine. 2022; 11(17):4992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11174992
Chicago/Turabian StyleJevtic, Dorde, Tatjana Gavrancic, Ivana Pantic, Terri Nordin, Charles W. Nordstrom, Marina Antic, Nikola Pantic, Marija Kaljevic, Bojan Joksimovic, Milan Jovanovic, and et al. 2022. "Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature" Journal of Clinical Medicine 11, no. 17: 4992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11174992