
Comparison of the Clinical Outcomes of Titanium and Zirconia Implant Abutments: A Systematic Review of Systematic Reviews
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
- Population: healthy patients with at least one dental implant connected to a titanium or zirconia abutment.
- Intervention: titanium or zirconia abutment with or without any surface modification.
- Comparison: titanium or zirconia abutment with or without any surface modification.
- Outcome: mechanical, biological and esthetic outcomes.
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
- Systematic reviews evaluating the analyzed outcomes.
- Systematic review of in vitro studies.
- Systematic reviews of animal studies.
- Studies focused on the implant–abutment interface.
- Studies comparing titanium and zirconia implants.
2.4. Screening Method
2.5. Data Extraction
2.6. Quality Assessment
3. Results
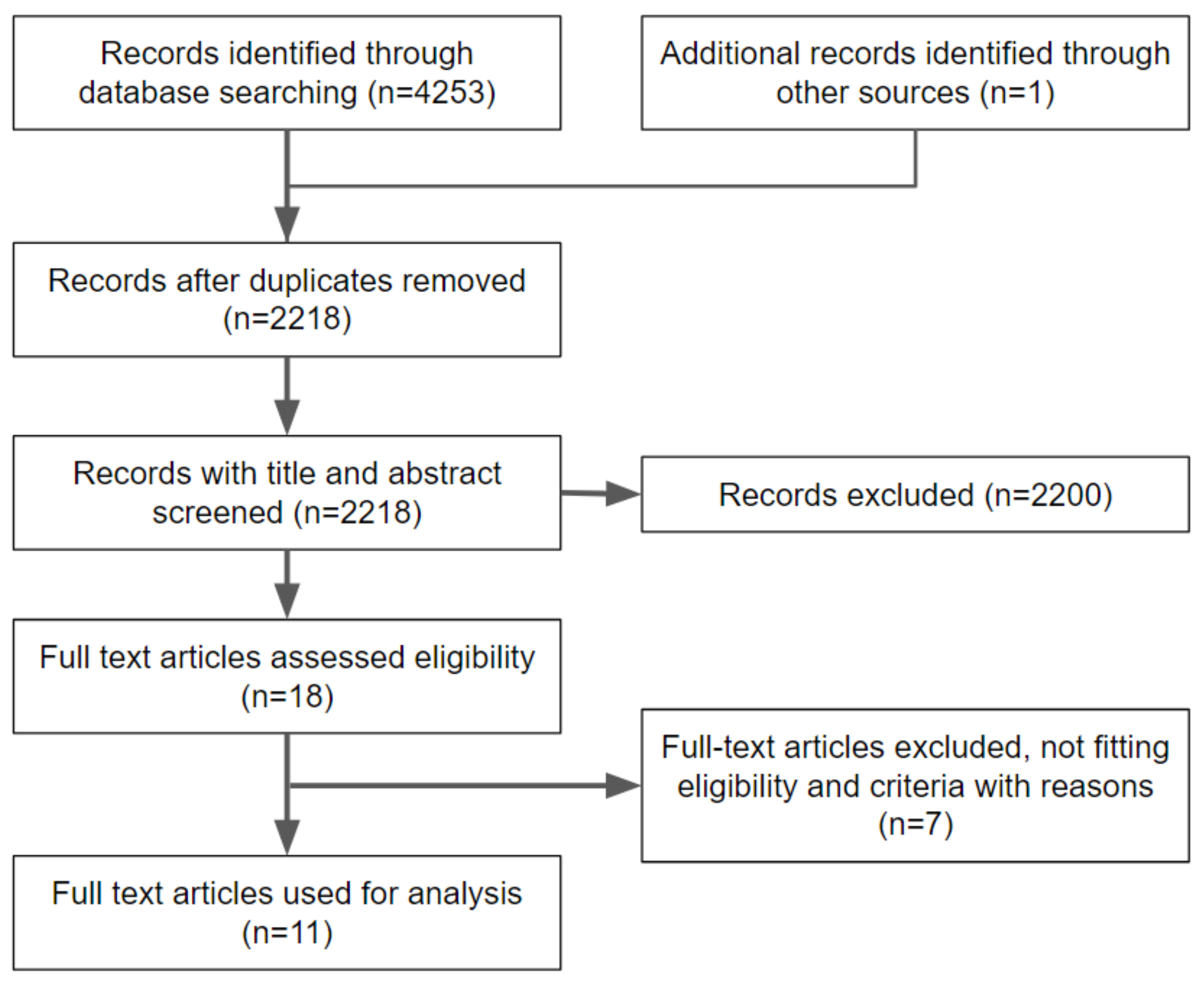
3.1. Inclusion and Exclusion of Articles
3.2. Description of Selected Articles
3.3. Quality Assessment
3.4. Comparison of Titanium and Zirconia Abutments
3.5. Mechanical Outcomes
3.6. Biological Complications
3.7. Esthetic Outcomes
4. Discussion
4.1. Mechanical Outcomes
4.2. Biological Outcomes
4.3. Esthetic Outcomes
5. Conclusions
- Titanium has proven to be mechanically superior compared to zirconia, although the difference in the incidence of mechanical failures was not significant in the majority of the studies. In the posterior area and where occlusal forces are stronger, a titanium implant abutment is the better option.
- There is no significant difference in the biological complications, marginal bone loss and periodontal probing depth between zirconia and titanium abutments, although titanium abutments showed a tendency to greater plaque accumulation compared to zirconia ones.
- BOP is slightly greater next to titanium abutments compared to zirconia ones, but it is not influenced by the macroscopic design, surface topography or surface manipulation.
- The macroscopic design of implant abutment seems to influence the soft tissue thickness only, with concave abutments allowing more soft tissue gain for both zirconia and titanium implant abutments. The position of the prosthetic margin also plays a big role especially in the case of cement-retained prostheses.
- Surface roughness or topography may play a role in soft tissue attachment; however, further research is needed to confirm this hypothesis.
- Marginal bone loss was not significantly influenced by the abutment material, but by the surface decontamination of titanium implant abutments. Plasma argon titanium abutments show less bone loss compared to steamed titanium abutments.
- Regarding the esthetic outcome, any implant abutment material can be used when the soft tissue thickness is sufficient (more than 3 mm). In cases with limited soft tissue thickness, especially in the esthetic area, zirconia abutments show better esthetic results. Further research is needed to evaluate modifications that can be made to both materials, such as anodization or veneering of the abutment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanz-Martín, I.; Sanz-Sánchez, I.; Carrillo de Albornoz, A.; Figuero, E.; Sanz, M. Effects of modified abutment characteristics on peri-implant soft tissue health: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 118–129. [Google Scholar] [CrossRef]
- Canullo, L.; Menini, M.; Santori, G.; Rakic, M.; Sculean, A.; Pesce, P. Titanium abutment surface modifications and peri-implant tissue behavior: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 1113–1124. [Google Scholar] [CrossRef]
- Daneshvar, S.; Matthews, D.; Michuad, P.-L.; Ghiabi, E. Success and Survival Rates of Dental Implants Restored at an Undergraduate Dental Clinic: A 13-Year Retrospective Study with a Mean Follow-up of 5.8 Years. Int. J. Oral Maxillofac. Implant. 2016, 31, 870–875. [Google Scholar] [CrossRef]
- Moraschini, V.; Poubel LD, C.; Ferreira, V.F.; dos Sp Barboza, E. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar]
- Menini, M.; Dellepiane, E.; Chvartszaid, D.; Baldi, D.; Schiavetti, I.; Pera, P. Influence of Different Surface Characteristics on Peri-implant Tissue Behavior: A Six-Year Prospective Report. Int. J. Prosthodont. 2015, 28, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Menini, M.; Pera, F.; Ravera, G.; Pera, P. Plaque accumulation on exposed titanium surfaces and peri-implant tissue behavior. A Preliminary 1-year clinical study. Int. J. Prosthodont. 2009, 22, 447–455. [Google Scholar]
- Menini, M.; Setti, P.; Pera, P.; Pera, F.; Pesce, P. Peri-implant tissue health and bone resorption in immediately loaded, implant-supported full-arch prostheses. Int. J. Prosthodont. 2018, 31, 327–333. [Google Scholar] [CrossRef]
- Delucchi, F.; Pozzetti, E.; Bagnasco, F.; Pesce, P.; Baldi, D.; Pera, F.; Di Tullio, N.; Pera, P.; Menini, M. Peri-implant tissue behaviour next to different titanium surfaces: 16-year post-trial follow-up. Appl. Sci. 2021, 11, 9625. [Google Scholar]
- Schwartz-Arad, D.; Laviv, A.; Levin, L. Failure Causes, Timing, and Cluster Behavior: An 8-Year Study of Dental Implants. Implant Dent. 2008, 17, 200–207. [Google Scholar] [CrossRef]
- Menini, M.; Conserva, E.; Tealdo, T.; Bevilacqua, M.; Pera, F.; Signori, A.; Pera, P. Shock absorption capacity of restorative materials for implant prostheses: An in vitro study. Int. J. Prosthodont. 2013, 26, 549–556. [Google Scholar] [CrossRef]
- Prisco, R.; Troiano, G.; Laino, L.; Zhurakivska, K. Rotational tolerances of a titanium abutment in the as-received condition and after screw tightening in a conical implant connection. J. Adv. Prosthodont. 2021, 13, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Menini, M.; Dellepiane, E.; Talita, D.; Fulcheri, E.; Pera, P.; Pesce, P. Comparison of bone-level and tissue-level implants: A pilot study with a histologic analysis and a 4-year follow-up. Int. J. Periodontics Restor. Dent. 2022, 42, 535–543. [Google Scholar]
- Carossa, M.; Alovisi, M.; Crupi, A.; Ambrogio, G.; Pera, F. Full-Arch Rehabilitation Using Trans-Mucosal Tissue-Level Implants with and without Implant-Abutment Units: A Case Report. Dent. J. 2022, 10, 116. [Google Scholar] [CrossRef]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Impl. Res. 2008, 19, 635–641. [Google Scholar] [CrossRef]
- Vohra, F.; Al-Kheraif, A.A.; Ab Ghani, S.M.; Abu Hassan, M.I.; Alnassar, T.; Javed, F. Crestal bone loss and periimplant inflammatory parameters around zirconia implants: A systematic review. J. Prosthet. Dent. 2015, 114, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Sampatanukul, T.; Serichetaphongse, P.; Pimkhaokham, A. Histological evaluations and inflammatory responses of different dental implant abutment materials: A human histology pilot study. Clin. Implant Dent. Relat. Res. 2017, 20, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Vaitelis, J. The effect of zirconia or titanium as abutment material on soft peri-implant tissues: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2015, 26, 139–147. [Google Scholar] [CrossRef]
- Sailer, I.; Zembic, A.; Jung, R.E.; Siegenthaler, D.; Holderegger, C.; Hämmerle, C.H. Randomized controlled clinical trial of customized zirconia and titanium implant abutments for canine and posterior single-tooth implant reconstructions: Preliminary results at 1 year of function. Clin. Oral Implant. Res. 2009, 20, 219–225. [Google Scholar] [CrossRef]
- Bharate, V.; Kumar, Y.; Koli, D.; Pruthi, G.; Jain, V. Effect of different abutment materials (zirconia or titanium) on the crestal bone height in 1 year. J. Oral Biol. Craniofacial Res. 2020, 10, 372–374. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Sanz-Martín, I.; Carrillo de Albornoz, A.; Figuero, E.; Sanz, M. Biological effect of the abutment material on the stability of peri-implant marginal bone levels: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 124–144. [Google Scholar] [CrossRef]
- Alovisi, M.; Carossa, M.; Mandras, N.; Roana, J.; Costalonga, M.; Cavallo, L.; Pira, E.; Putzu, M.G.; Bosio, D.; Roato, I.; et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials 2022, 15, 4850. [Google Scholar] [CrossRef] [PubMed]
- Poggio, C.E.; Ercoli, C.; Rispoli, L.; Maiorana, C.; Esposito, M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst. Rev. 2017, 12, CD009606. [Google Scholar] [CrossRef]
- Schlichting, L.H.; Magne, P. Double-milled CAD-CAM composite resin restorations: A proof-of-concept approach to producing histoanatomic bilaminar restorations. J. Prosthet. Dent. 2020, 124, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 399, b2700. [Google Scholar] [CrossRef] [PubMed]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E. Henry AMSTAR 2: A critical appraisal tool for systematic reviews thatinclude randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017, 358, j4008. [Google Scholar] [CrossRef]
- Canullo, L.; Pesce, P.; Patini, R.; Antonacci, D.; Tommasato, G. What Are the Effects of Different Abutment Morphologies on Peri-implant Hard and Soft Tissue Behavior? A Systematic Review and Meta-Analysis. Int. J. Prosthodont. 2020, 33, 297–306. [Google Scholar] [CrossRef]
- Al Rezk, F.; Trimpou, G.; Lauer, H.C.; Weigl, P.; Krockow, N. Response of soft tissue to different abutment materials with different surface topographies: A review of the literature. Gen. Dent. 2018, 66, 18–25. [Google Scholar]
- Linkevicius, T.; Apse, P. Influence of abutment material on stability of peri-implant tissues: A systematic review. Int. J. Oral Maxillofac. Implant. 2008, 23, 449–456. [Google Scholar]
- Pesce, P.; Menini, M.; Tommasato, G.; Patini, R.; Canullo, L. Influence of modified titanium abutment surface on peri-implant soft tissue behaviour: A systematic review of histological findings. Int. J. Oral Implant. (Berl) 2019, 12, 419–429. [Google Scholar]
- Yu, S.B.; Song, B.G.; Cheon, K.J.; Kim, J.W.; Kim, Y.H.; Yang, B.E. Clinical reliability of zirconium abutment in implant restorations in the English and Korean literature. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 26. [Google Scholar] [CrossRef] [PubMed]
- De Medeiros, R.A.; Vechiato-Filho, A.J.; Pellizzer, E.P.; Mazaro, J.V.; dos Santos, D.M.; Goiato, M.C. Analysis of the peri-implant soft tissues in contact with zirconia abutments: An evidence-based literature review. J. Contemp. Dent. Pract. 2013, 14, 567–572. [Google Scholar] [CrossRef]
- Bidra, A.S.; Rungruanganunt, P. Clinical outcomes of implant abutments in the anterior region: A systematic review. J. Esthet. Restor. Dent. 2013, 25, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Vechiato-Filho, A.J.; Pesqueira, A.A.; De Souza, G.M.; dos Santos, D.M.; Pellizzer, E.P.; Goiato, M.C. Are Zirconia Implant Abutments Safe and Predictable in Posterior Regions? A Systematic Review and Meta-Analysis. Int. J. Prosthodont. 2016, 29, 233–244. [Google Scholar] [CrossRef]
- Cai, H.; Chen, J.; Li, C.; Wang, J.; Wan, Q.; Liang, X. Quantitative discoloration assessment of peri-implant soft tissue around zirconia and other abutments with different colours: A systematic review and meta-analysis. J. Dent. 2018, 70, 110–117. [Google Scholar] [CrossRef]
- Cao, Y.; Yu, C.; Wu, Y.; Li, L.; Li, C. Long-Term Survival and Peri-Implant Health of Titanium Implants with Zirconia Abutments: A Systematic Review and Meta-Analysis. J. Prosthodont. 2019, 28, 883–892. [Google Scholar] [CrossRef]
- Hu, M.; Chen, J.; Pei, X.; Han, J.; Wang, J. Network meta-analysis of survival rate and complications in implant-supported single crowns with different abutment materials. J. Dent. 2019, 88, 103115. [Google Scholar] [CrossRef]
- Gou, M.; Chen, H.; Fu, M.; Wang, H. Fracture of Zirconia Abutments in Implant Treatments: A Systematic Review. Implant Dent. 2019, 28, 378–387. [Google Scholar] [CrossRef]
- Naveau, A.; Rignon-Bret, C.; Wulfman, C. Zirconia abutments in the anterior region: A systematic review of mechanical and esthetic outcomes. J. Prosthet. Dent. 2019, 121, 775–781.e1. [Google Scholar] [CrossRef]
- Pitta, J.; Zarauz, C.; Pjetursson, B.; Sailer, I.; Liu, X.; Pradies, G. A Systematic Review and Meta-Analysis of the Influence of Abutment Material on Peri-implant Soft Tissue Color Measured Using Spectrophotometry. Int. J. Prosthodont. 2020, 33, 39–47. [Google Scholar] [CrossRef]
- Pae, A.; Lee, H.; Kim, H.S.; Kwon, Y.D.; Woo, Y.H. Attachment and growth behaviour of human gingival fibroblasts on titanium and zirconia ceramic surfaces. Biomed. Mater. 2009, 4, 025005. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamed, M.I.; Galley, J.D.; Bailey, M.T.; Johnston, W.M.; Holloway, J.; McGlumphy, E.; Leblebicioglu, B. A Comparison of Zirconia and Titanium Abutments for Microleakage. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. 2), e643–e651. [Google Scholar] [CrossRef]
- Zembic, A.; Bösch, A.; Jung, R.E.; Hämmerle, C.H.; Sailer, I. Five-year results of a randomized controlled clinical trial comparing zirconia and titanium abutments supporting single-implant crowns in canine and posterior regions. Clin. Oral Implant. Res. 2013, 24, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Nothdurft, F.P. All-Ceramic Zirconium Dioxide Implant Abutments for Single-Tooth Replacement in the Posterior Region: A 5-Year Outcome Report. Int. J. Prosthodont. 2019, 32, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Menini, M.; Pesce, P.; Bagnasco, F.; Carossa, M.; Mussano, F.; Pera, F. Evaluation of internal and external hexagon connections in immediately loaded full-arch rehabilitations: A within-person randomised split-mouth controlled trial. Int. J. Oral Implant. 2019, 12, 169–179. [Google Scholar]
- Şen, N.; Şermet, I.B.; Gürler, N. Sealing capability and marginal fit of titanium versus zirconia abutments with different connection designs. J. Adv. Prosthodont. 2019, 11, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Rompen, E.; Raepsaet, N.; Domken, O.; Touati, B.; Van Dooren, E. Soft tissue stability at the facial aspect of gingivally converging abutments in the esthetic zone: A pilot clinical study. J. Prosthet. Dent. 2007, 97 (Suppl. 6), S119–S125. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Cordasco, G.; Rotondo, F.; Crupi, A.; Ramaglia, L. Anticoagulant therapy in patients undergoing dental interventions: A critical review of the literature and current perspectives. Minerva Stomatol. 2015, 64, 21–46. [Google Scholar]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]


{kind=link}
| Excluded Articles | Year | Reason of Exclusion | |
|---|---|---|---|
| 1 | Canullo L, Pesce P, Patini R, Antonacci D, Tommasato G. [28] | 2020 | Outcome cannot be retrieved |
| 2 | Al Rezk F, Trimpou G, Lauer HC, Weigl P, Krockow N. [29] | 2018 | Includes animal and in vitro studies |
| 3 | Linkevicius T, Apse P. [30] | 2008 | Includes animal studies |
| 4 | Pesce P, Menini M, Tommasato G, Patini R, Cannullo L [31] | 2019 | Discusses healing abutment modification |
| 5 | Canullo L, Menini M, Santori G, Rakic M, Sculean A, Pesce P. [2] | 2019 | Discusses healing abutment modification |
| 6 | Yu SB, Song BG, Cheon KJ, Kim JW, Kim YH, Yang BE. [32] | 2018 | Narrative review |
| 7 | de Medeiros RA, Vechiato-Filho AJ, et al. [33] | 2013 | Evidence based narrative literature review |
| Authors | Year of Publication | Design of the Studies Included | Focused Question | Databases Searched | n. of Studies Included | n. of Patients | n. of Implants | Abutment Materials Investigated | Outcomes Investigated | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bidra AS, et al. [34] | 2013 | RCT, prospective, retrospective, and cross sectional studies | Evaluate clinical outcomes including survival outcomes, mechanical outcomes, and biological and esthetic outcomes of implant abutments used exclusively in the maxillary and mandibular anterior regions. | Pubmed/Medline | 27 studies | NA | NA (implants abutments only in the anterior) | Titanium, cast metal alloy, alumina, zirconia and zirconia with titanium base abutments | Survival, mechanical, biological and esthetic outcomes |
| 2 | Linkevicius T, et al. [17] | 2015 | Clinical studies | To define the effect of zirconia and titanium as abutment materials on soft peri-implant tissues. The topic was divided into 2 parts: (a) biology and (b) esthetics. | Pubmed/Medline | 11 studies | 389 patients | 512 implants (280 titanium abutments and 232 zirconia abutments) | Titanium and zirconia abutments | Biological and esthetic outcomes |
| 3 | Vechiato-Filho AJ, et al. [35] | 2016 | RCT and prospective studies | Are zirconia implant abutments safe and predictable in posterior areas? | Pubmed/Medline and Cochrane Library | 11 studies | 353 patients | NA | Titanium and zirconia abutments | Mechanical or biological complications |
| 4 | Sanz-Sánchez I, et al. [20] | 2018 | RCT, CCT and case series studies | Which is the effect of the abutment material on the stability and health of the peri-implant tissues? | Pubmed/Medline and Cochrane Central Register of Controlled Trials | 29 studies | NA | NA | Titanium, zirconia, alumina, Li Dis, gold, | Biological, mechanical and esthetic outcome |
| 5 | Sanz-Martín I, et al. [1] | 2018 | RCT | Which is the effect of modifying the abutment characteristics for maintaining peri-implant soft tissue health? | Pubmed and Cochrane Central Register of Controlled Trials | 13 studies | NA | 889 implants | Titanium, alumina, zirconia, and ceramic | Biological outcome (peri-implant soft tissue health) |
| 6 | Cai H, et al. [36] | 2018 | RCT, prospective and retrospective studies | How do zirconia and other abutments with different tints affect the color of peri-implant soft tissue? | PubMed, EMBASE, Cochrane Database of Systematic Reviews (CDSR), and Cochrane Central Register of Controlled Trials (CENTRAL) | 8 studies | NA | 365 implants (128 titanium abutments, 141 zirconia abutments, 96 gold abutments (not reported in all included studies)) | Titanium, zirconia, and golden abutments | Esthetic outcome (quantitative discoloration assessment) |
| 7 | Cao Y, et al. [37] | 2019 | RCT, CCT, and long-term observational studies | In patients treated with titanium implants with zirconia abutments, what percentage of implants can survive, and what is the effect of zirconia abutments on the marginal bone loss (MBL) and pocket probing depth (PPD), compared with all-titanium implants? | Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE via OVID, EMBASE, and Chinese Biomedical Literature Database | 18 studies (10 studies included in part 1, 12 studies included in part 2) | Part 1: NA Part 2: 332 patients | Part I: 353 implants Part 2: 427 implants | Titanium and zirconia abutments | Biological outcomes |
| 8 | Hu M, et al. [38] | 2019 | RCT, CCT, prospective and retrospective studies | How do abutment materials influence the survival rate of the abutment, the marginal bone loss and the peri-implant soft tissue discoloration in implant-supported single crowns? | Medline, EMBASE, Web of Science, CENTRAL (Cochrane Library), CNKI (China National Knowledge Infrastructure), and the Chinese Biomedical Literature Database | 23 studies | NA | 1006 implants (403 titanium abutments, 35 alumina abutments, 447 zirconia abutments, 121 golden abutments) | Titanium, zirconia, alumina and golden abutments | Biological and esthetic outcome |
| 9 | Gou M, et al. [39] | 2019 | RCT, case reports, prospective and retrospective studies. | To determine the characteristics, causes, managements, and preventive measures with respect to zirconia abutment fracture. | Medline, Embase, and Cochrane library | 15 studies | NA | 1528 implants | Zirconia abutments | Mechanical outcomes |
| 10 | Naveau A, et al. [40] | 2019 | RCT, prospective and retrospective studies. | In patients requiring a single, anterior implant, what are zirconia abutments’ survival, mechanical, and esthetic outcomes? | Pubmed/Medline | 20 studies | NA | NA | Zirconia abutments | Mechanical and esthetic outcomes |
| 11 | Pitta J, et al. [41] | 2020 | RCT | (1) Do ceramic abutments exhibit differences in peri-implant soft tissue color when compared to metallic abutments in single-unit implant supported reconstructions? (2) Does the soft tissue thickness have an effect on the peri-implant soft tissue color differences when metallic or ceramic abutments are used for single-unit implant-supported reconstructions? | Pubmed/Medline | 6 studies | 265 patients | NA | Titanium, zirconia and gold alloy abutments | Esthetic outcomes |
| Criteria | Bidra AS et al. [34] | Linkevicius T et al. [17] | Vechiato-Filho AJ et al. [35] | Sanz-Sánchez I et al. [20] | Sanz-Martín I et al. [1] | Cai H et al. [36] | Cao Y et al. [37] | Hu M et al. [38] | Gou M et al. [39] | Naveau A et al. [40] | Pitta J et al. [41] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Research question and inclusion criteria PICO | |||||||||||
| 2. Protocol registered before commencement of the review | |||||||||||
| 3. Explanation of selection of drawings from the included studies | |||||||||||
| 4. Adequacy of the literature search | |||||||||||
| 5. Duplicate study selection | |||||||||||
| 6. Duplicate data extraction | |||||||||||
| 7. List and justification of excluded studies | |||||||||||
| 8. Studies included described in detail | |||||||||||
| 9. Risk of bias from individual studies being included in the review | |||||||||||
| 10. Sources of financing of included studies reported in review | |||||||||||
| 11. Appropriateness of meta-analytical methods | |||||||||||
| 12. If meta-analysis: bias risk of included studies taken into account | |||||||||||
| 13. Risk of bias taken into account in the interpretation and discussion | |||||||||||
| 14. Satisfactory explanation for any heterogeneity | |||||||||||
| 15. Assessment of presence and likely impact of publication bias | |||||||||||
| 16. Conflicts of interest |
 ; criterion partially identified in the text
; criterion partially identified in the text  ; unidentified criteria in the text
; unidentified criteria in the text  ; not applicable
; not applicable  .
.| Authors | Abutment Fracture | Screw Loosening | Abutment Screw Fracture | Veneer Failure |
|---|---|---|---|---|
| Bidra AS, et al. [34] | 11 studies reported fractures of ceramic abutments, 8 on alumina abutments and 3 on zirconia abutments. No fractures were found in titanium or cast metal abutments. | Abutment screw loosening was reported as primary mechanical complication, although screw loosening is a well-recognized complication for external hex implants which was used in the majority of these studies. | Only one study reported an abutment screw fracture, making it appear to be a rare complication for anterior abutments. | - |
| Linkevicius T, et al. [17] | - | - | - | - |
| Vechiato-Filho AJ, et al. [33] | Screw loosening was reported for both materials. | In the posterior area, the risk ratio (RR) showed that zirconia abutments were about 0.52 times more susceptible to veneer failure than titanium abutments. Veneer failure mostly occurs in the cusp tips and polishing was considered adequate to overcome the problem. | ||
| Sanz-Sánchez I, et al. [20] | Abutment fracture was reported. There was a higher, but non-significant, incidence of complications for ceramic when compared to titanium abutments. | Veneer chipping was reported. | ||
| Sanz-Martín I, et al. [1] | ||||
| Cai H, et al. [36] | ||||
| Cao Y, et al. [37] | ||||
| Hu M, et al. [38] | ||||
| Gou M, et al. [39] | Posterior teeth seemed more susceptible to zirconia abutment fracture. Fewer fractures were reported for two-piece internal connection zirconia abutments compared to external connection zirconia abutments and one-piece internal connection zirconia abutments. One-piece internal connection zirconia abutments had the highest fracture rates. Higher fracture rates were reported for abutments with platform switching compared to standard platforms. | |||
| Naveau A, et al. [40] | Considered as a major mechanical complication, varying from 1.2% to 8%, fractures were found in screw access holes with thin walls for abutments with an external connection, while for internal connections it was found in the implant necks. Implant diameter did not seem to have any influence on the fracture rate and no specific time frame could be defined. | Considered as a minor mechanical complication. The highest rate of screw loosening found was 6% in one study. | ||
| Pitta J, et al. [41] |
| Authors | Biological Complications | Recession | Pocket Probing Depth | Bleeding on Probing and Plaque Accumulation | Marginal Bone Loss | Esthetic Outcome |
|---|---|---|---|---|---|---|
| Bidra AS, et al. [34] | As for biological outcomes, fistulas were found to be the most common complication, both in screw-retained and cement-retained restorations. | Peri-implant mucosal recession was reported predominantly in studies using prefabricated titanium abutments. Concave-shaped abutments showed better soft tissue stability, minimized soft tissue recession, and even a gain in soft tissue height as reported in two studies. | - | - | - | In studies using spectrophotometric analysis, zirconia abutments showed less peri-implant mucosal discoloration compared with metal abutments. |
| Linkevicius T, et al. [17] | 12 out of 145 zirconia abutments experienced biological complications including a buccal marginal fistula, swelling, pain, suppuration, suppuration at probing, and a pocket probing depth of more than 5 mm. 5 titanium abutments out of 110 had biological complications, varied from a fistula, mucositis, suppuration at probing, a probing depth of more than 5 mm and a failure of the implant. The percentage of biological complications in titanium abutments was lower compared to zirconia abutments | In one study, there was slightly higher recession found in titanium abutments compared to zirconia, although there was no significant difference during a 5 year follow-up. In another study it was reported that stock titanium and zirconia abutments showed similar amounts of soft tissue recession while there was less recession in CAD/CAM zirconia abutments and an increase in soft tissue for CAD/CAM titanium abutments; although, the differences between the 4 groups were also not significant. Another study reported different results as the soft tissue recession was measured in two sites, the mesial and distal. In both titanium and zirconia abutments, there was soft tissue gain in the mesial site while soft tissue recession occurred in the distal site. | Pocket probing depth was reported to be slightly higher in titanium abutment but there was no significant difference between both materials. | Bleeding on probing was found to be slightly higher in zirconia abutments compared to titanium abutments, but the difference was not significant. | Marginal bone loss results were very similar between the two materials. | Soft tissue color around zirconia abutments showed a better color match to natural teeth compared to titanium abutments but no statistical differences was observed after several years of follow-up. Indexes such as the Copenhagen Index Score (CIS), Implant Crown Aesthetic Index (ICAI) and Papilla Index also showed no significant difference between both abutment materials, but zirconia had slightly higher scores in all indexes when compared to titanium. The Pink Esthetic Score (PES) was measured in one study during 12 months and 24 months of follow-up. The score was higher for zirconia, showing a significant difference between the two materials for both follow-up periods. |
| Vechiato-Filho AJ, et al. [35] | There was no significant difference in biological complications: mean bone loss for zirconia was 0.38 ± 0.87 mm and 0.2 ± 0.13 mm for titanium abutments; success rates were 99.3% for zirconia abutments and 99.57% for titanium abutments in the posterior area. | |||||
| Sanz-Sánchez I, et al. [20] | Overall incidence of biological complications was low. | Abutment material had no influence on probing depth. | Titanium showed a greater increase in BOP and greater plaque accumulation when compared to zirconia. | No significant difference was found between titanium and zirconia. When marginal bone loss was assessed over time, a significant loss occurred in all materials except for titanium nitride. | No differences in the esthetic outcome could be attributed to the abutment material. | |
| Sanz-Martín I, et al. [1] | Suppuration without bone loss was reported in one study for both titanium and zirconia abutments during the one-year follow-up. | Crown length of the implant restoration (CLI) was reported to increase in titanium abutments in one study. Abutments cleaned with plasma argon also showed higher recession compared to conventional/steam cleaning methods. | There was a significant increase in mucosal inflammation (BOP) for titanium abutments when compared to zirconia abutments; however, surface topography or manipulation did not have significant influence on soft tissue inflammation; trend for higher plaque accumulation for titanium abutments compared to zirconia abutments. | No significant difference was found when comparing abutment material and macroscopic design. The difference was significant when comparing surface manipulation, with greater bone loss reported for steamed titanium abutments compared to plasma argon titanium abutments. | Using a Visual Analog Scale (VAS), patients were equally satisfied regarding the esthetic outcome when comparing zirconia and titanium abutments. | |
| Cai H, et al. [36] | Soft-tissue discoloration was significantly lower around zirconia abutments than around titanium or golden abutments. | |||||
| Cao Y, et al. [37] | Survival rate of titanium implants with zirconia abutments appeared to be lower than those with titanium abutments in the long term. | Results favored implants with zirconia abutments. | Results favored implants with zirconia abutments. | |||
| Hu M, et al. [38] | Survival rate of titanium abutments and zirconia abutments were similar. | Zirconia abutment is better than gold or titanium abutment in terms of maintaining marginal bone. | There seemed to be no difference between zirconia and titanium abutments in discoloration of peri-implant soft tissue. | |||
| Gou M, et al. [39] | ||||||
| Naveau A, et al. [40] | Some studies reported that marginal bone loss was less with zirconia abutments compared to metal abutments. | Zirconia abutments provided better matching and integration of the color and surface of soft tissues than titanium abutments. They were particularly indicated in patients with thin peri-implant mucosa, because thick tissues are necessary to mask the grey color of the titanium abutment. | ||||
| Pitta J, et al. [41] | No significant difference was found between titanium and zirconia abutments, with limited information on the correlation between soft tissue thickness and ΔE values. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halim, F.C.; Pesce, P.; De Angelis, N.; Benedicenti, S.; Menini, M. Comparison of the Clinical Outcomes of Titanium and Zirconia Implant Abutments: A Systematic Review of Systematic Reviews. J. Clin. Med. 2022, 11, 5052. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11175052
Halim FC, Pesce P, De Angelis N, Benedicenti S, Menini M. Comparison of the Clinical Outcomes of Titanium and Zirconia Implant Abutments: A Systematic Review of Systematic Reviews. Journal of Clinical Medicine. 2022; 11(17):5052. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11175052
Chicago/Turabian StyleHalim, Felita Clarissa, Paolo Pesce, Nicola De Angelis, Stefano Benedicenti, and Maria Menini. 2022. "Comparison of the Clinical Outcomes of Titanium and Zirconia Implant Abutments: A Systematic Review of Systematic Reviews" Journal of Clinical Medicine 11, no. 17: 5052. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11175052