
Different Machine Learning Approaches for Implementing Telehealth-Based Cancer Pain Management Strategies

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
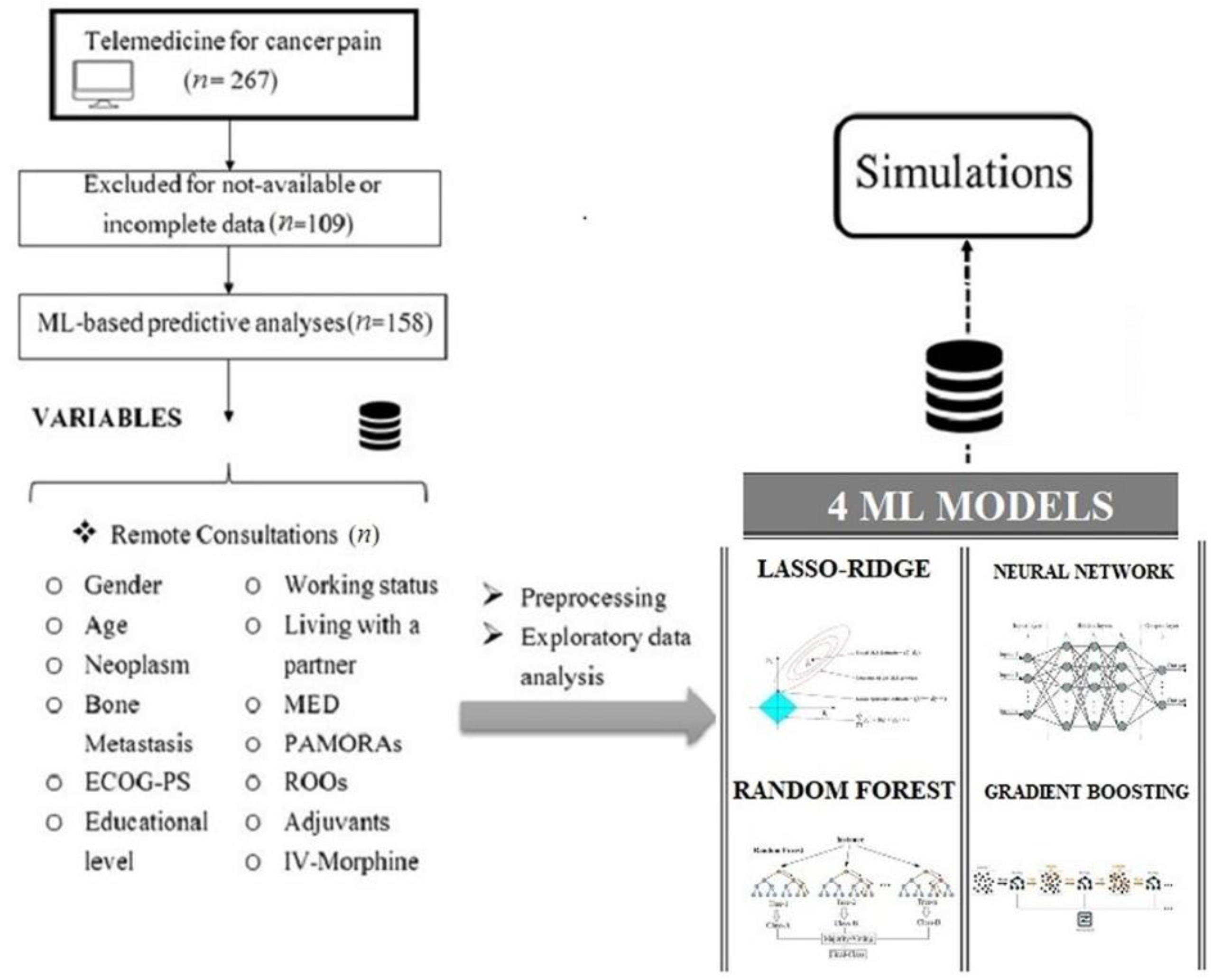
2.1. Study Population
2.2. Data Collection
2.3. Predictive Analysis
2.3.1. Preprocessing and Exploratory Data Analysis
2.3.2. Machine Learning Algorithms
- LASSO–RIDGE regression (elastic model): This is a generalized linear regression model that penalizes a loss function through regressor resizing (16 in all). Most of them are made small or led to zero if not important to explain the dependent variable. This approach reduces model complexity and prevents the over-fitting phenomena [16];
- Random forest (RF) algorithm: This algorithm can be used for both regression and classification. It is one of the most popular ML methods, belonging to the specific category of bagging methods. RF works on various overall models (decision trees) to improve the performance of each of them individually. The output is the whole contribution from all of them [17];
- Gradient boosting machine (GBM) is aimed at optimizing previsions by operating on the previous tree regression or classification error and reducing the error function (boosting method). In this way, the succeeding one can improve the prevision skills let by its preceding tree [18];
- Single hidden layer artificial neural network (ANN): This strategy can minimize a loss function by acting on some weights which tune connections between two neurons of two adjoining layers [19].
2.3.3. Model Processing and Evaluation
- GBM: The number of sequential trees from 20 to 100 by 10, tree depth from 2 to 5 shrinkage parameter (regularizing the error function) from 0.01 to 0.1 by 0.01, and a minimum observation-in-a-leaf from 10 to 20 for a total of 3960 were assessed;
- RF: Only the number of splitting variables was required, which was from 3 to 13;
- LASSO–RIDGE: Regression alpha and beta were, respectively, given as from 0 to 1 by 0.05 and 0 to 10 by 0.1, for a total of 2121 trials;
- ANN: This layer was made from 1 to 12 neurons and the decay (a regularization parameter to avoid the over-fitting of weights) ranged from 0.01 to 0.2 by 0.01, for a total of 240 trials.
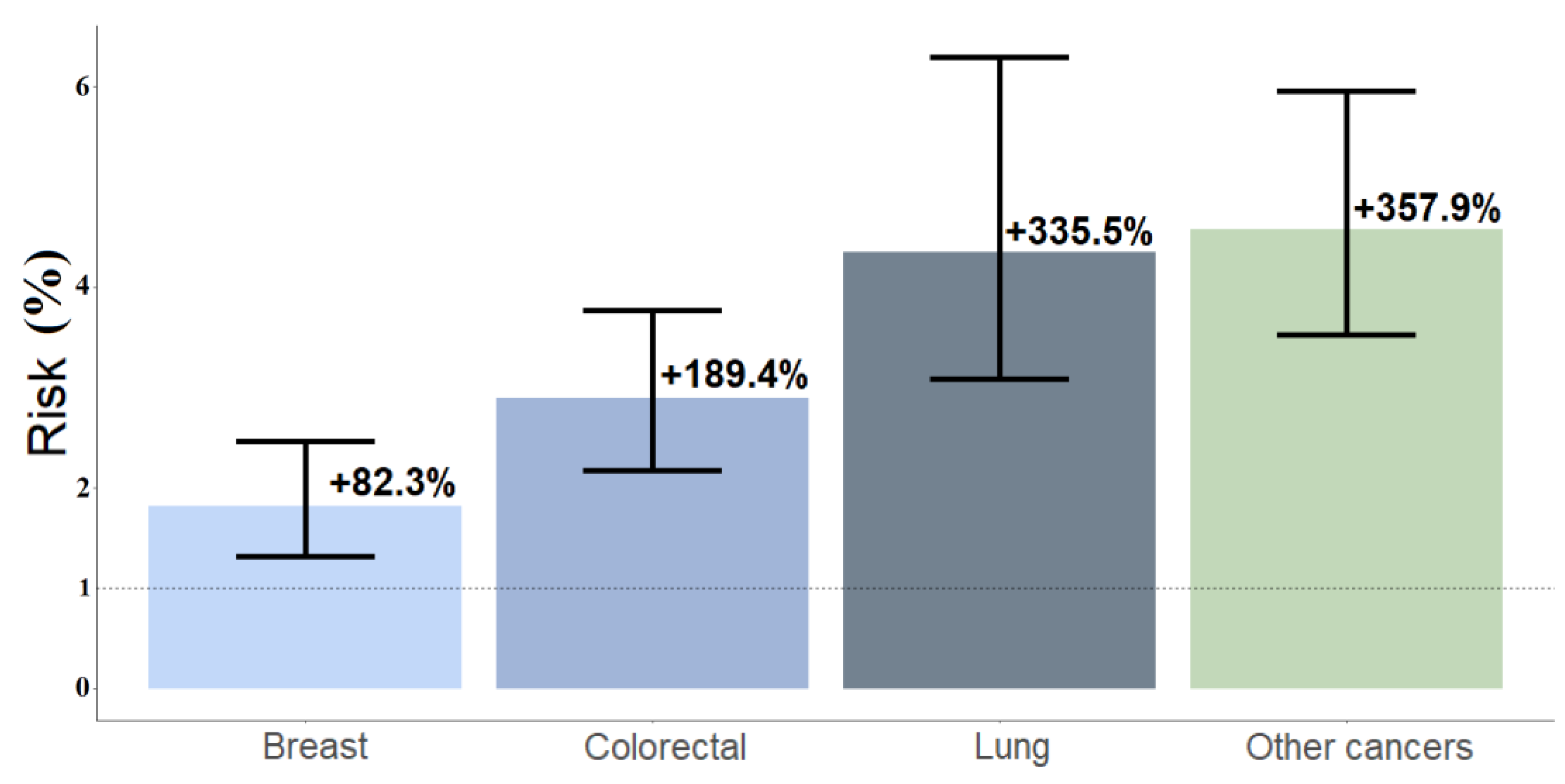
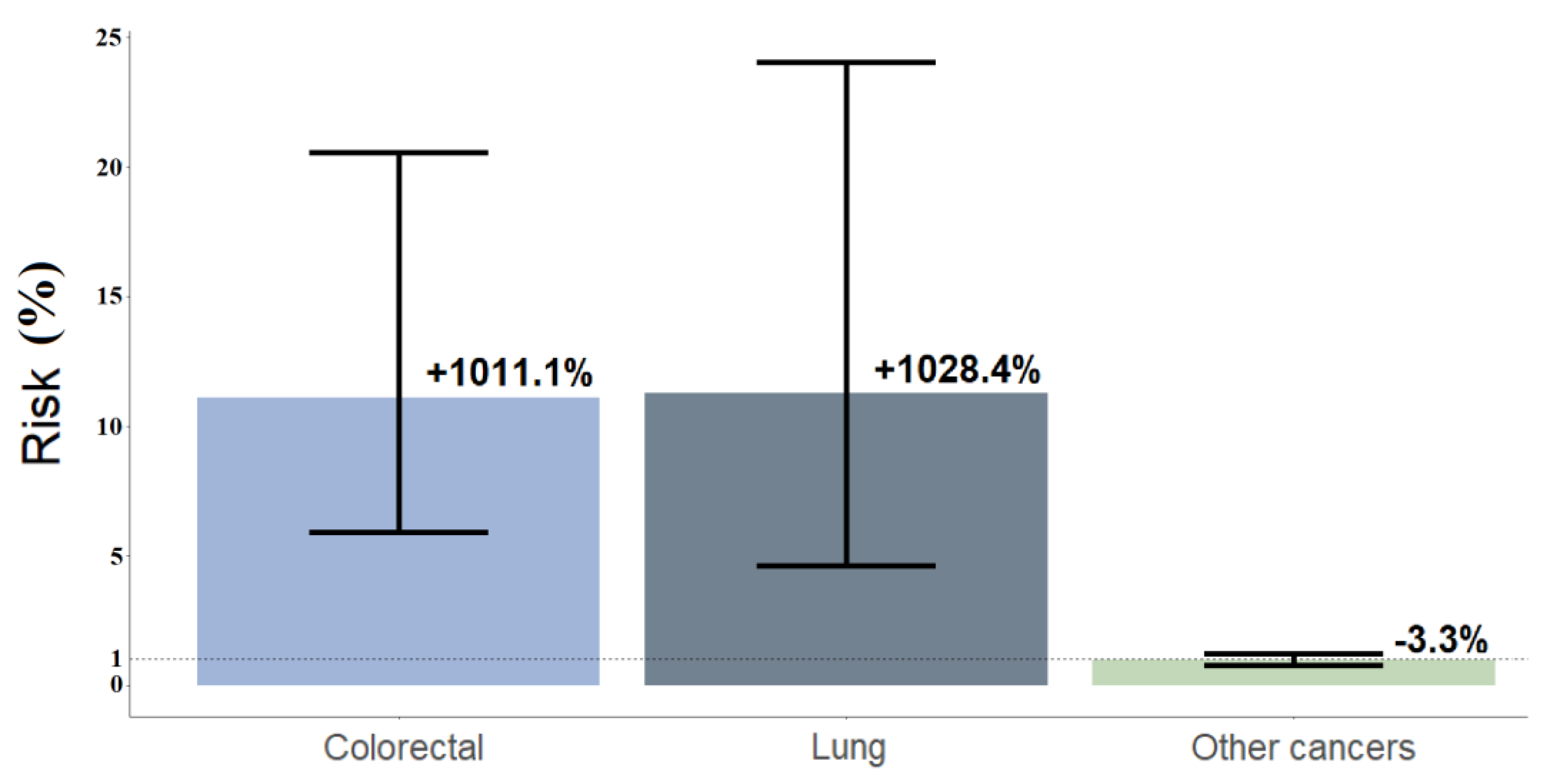
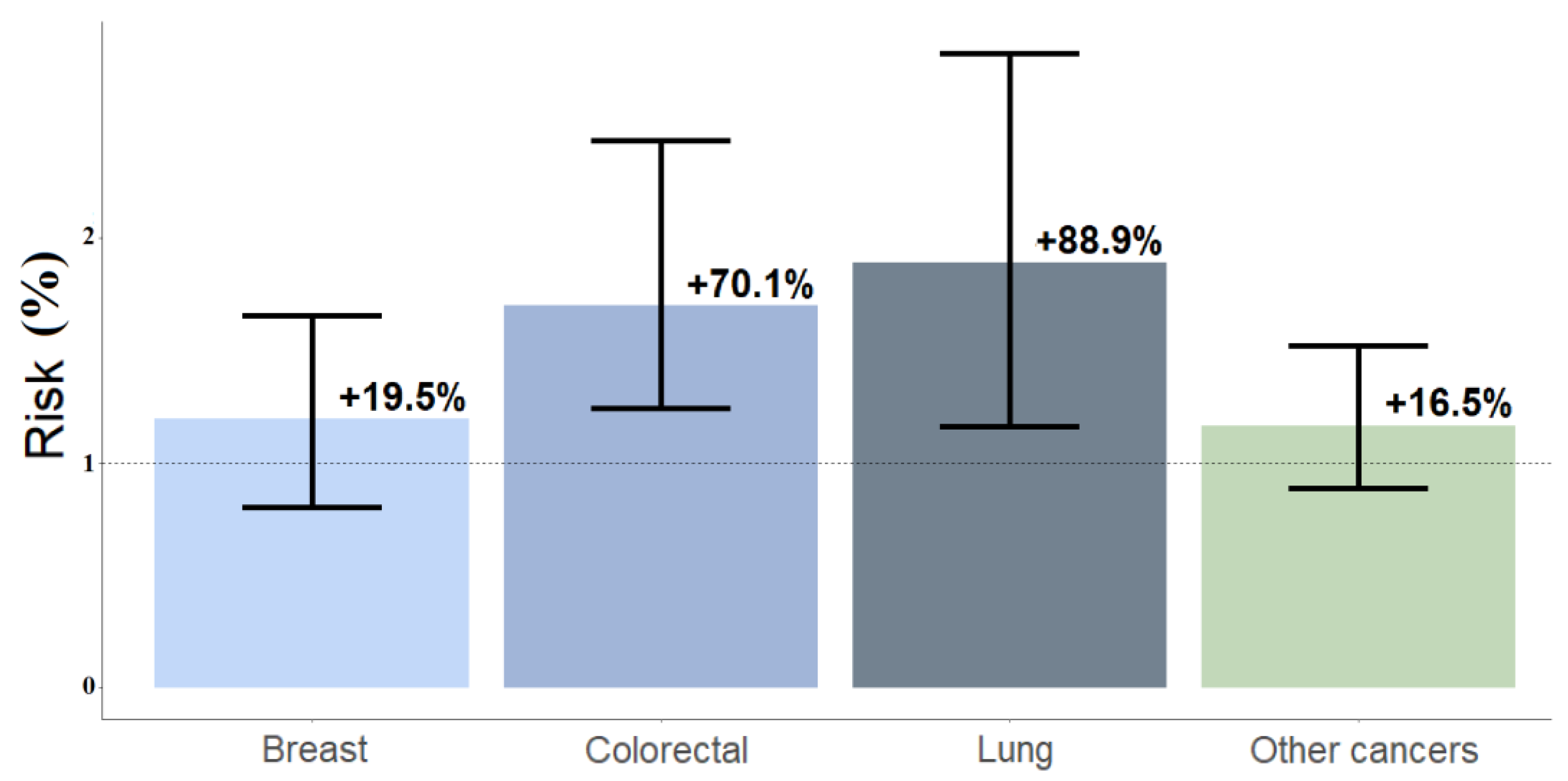
2.3.4. Risk Analysis
- Condition 1: Young patients (≤55 years old) with bone metastases and rapid-acting oral and nasal transmucosal fentanyl formulation (ROO) use (morphine-equivalent dose, MED > 60 mg) for breakthrough cancer pain (BTcP);
- Condition 2: Older cancer patients (>75 years old), with and without bone metastases;
- Condition 3:Male and female young patients (≤55 years old) with bone metastases;
- Condition 4: Younger (≤55 years old) vs. older (>75 years old) patients with bone metastases with gender differences.
2.4. Algorithmic Toolkit
3. Results
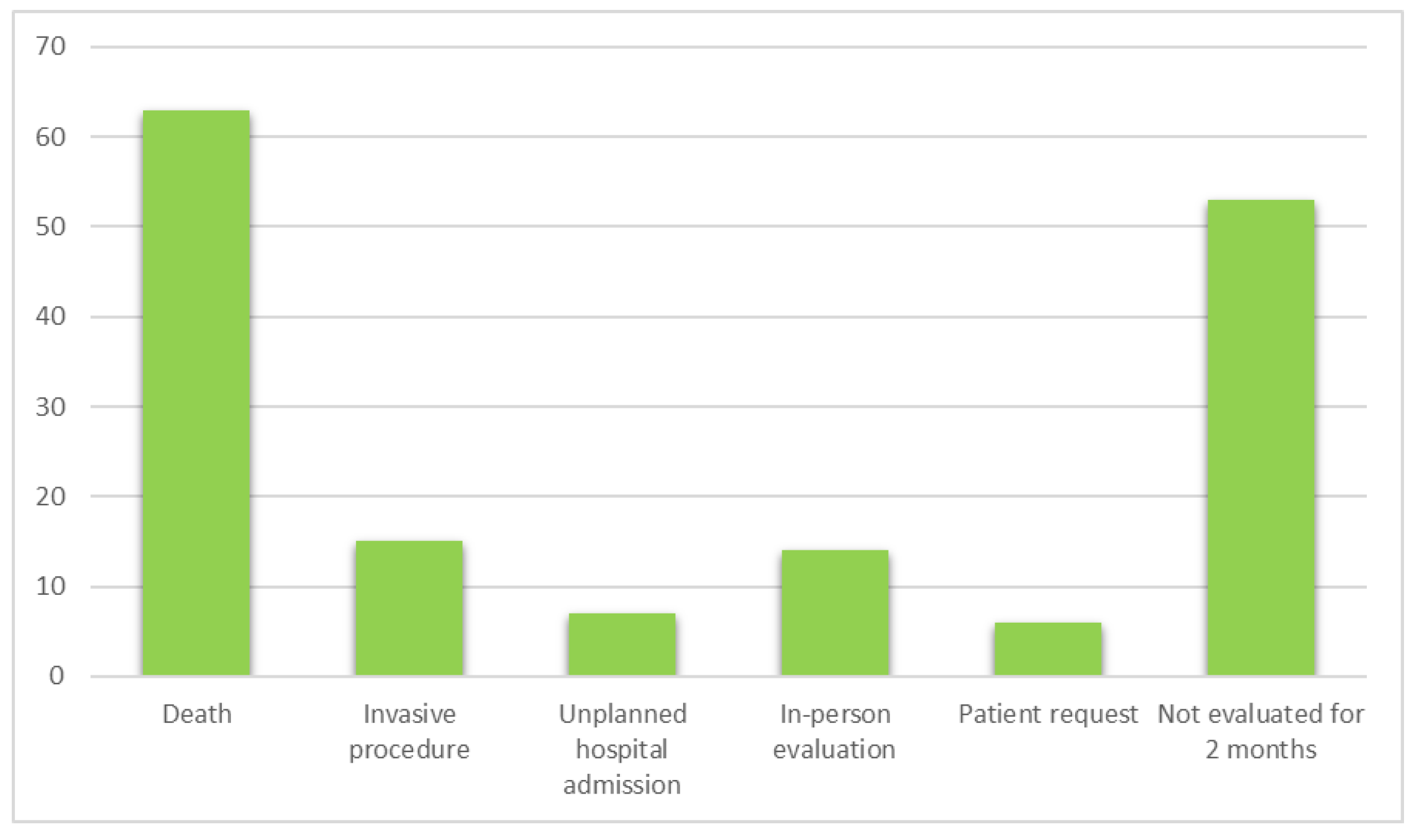
3.1. Descriptive Analysis
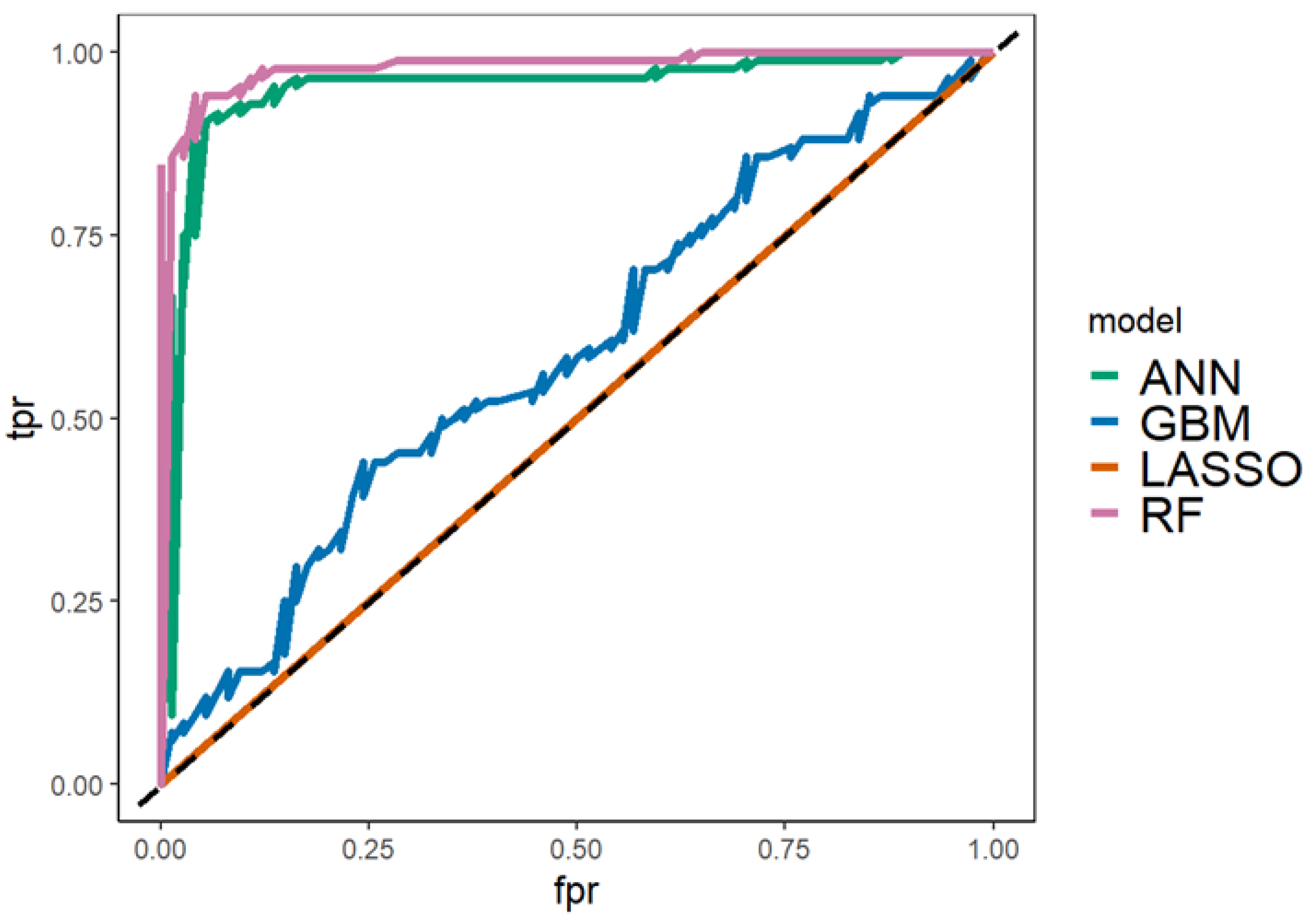
3.2. Predictive Analysis
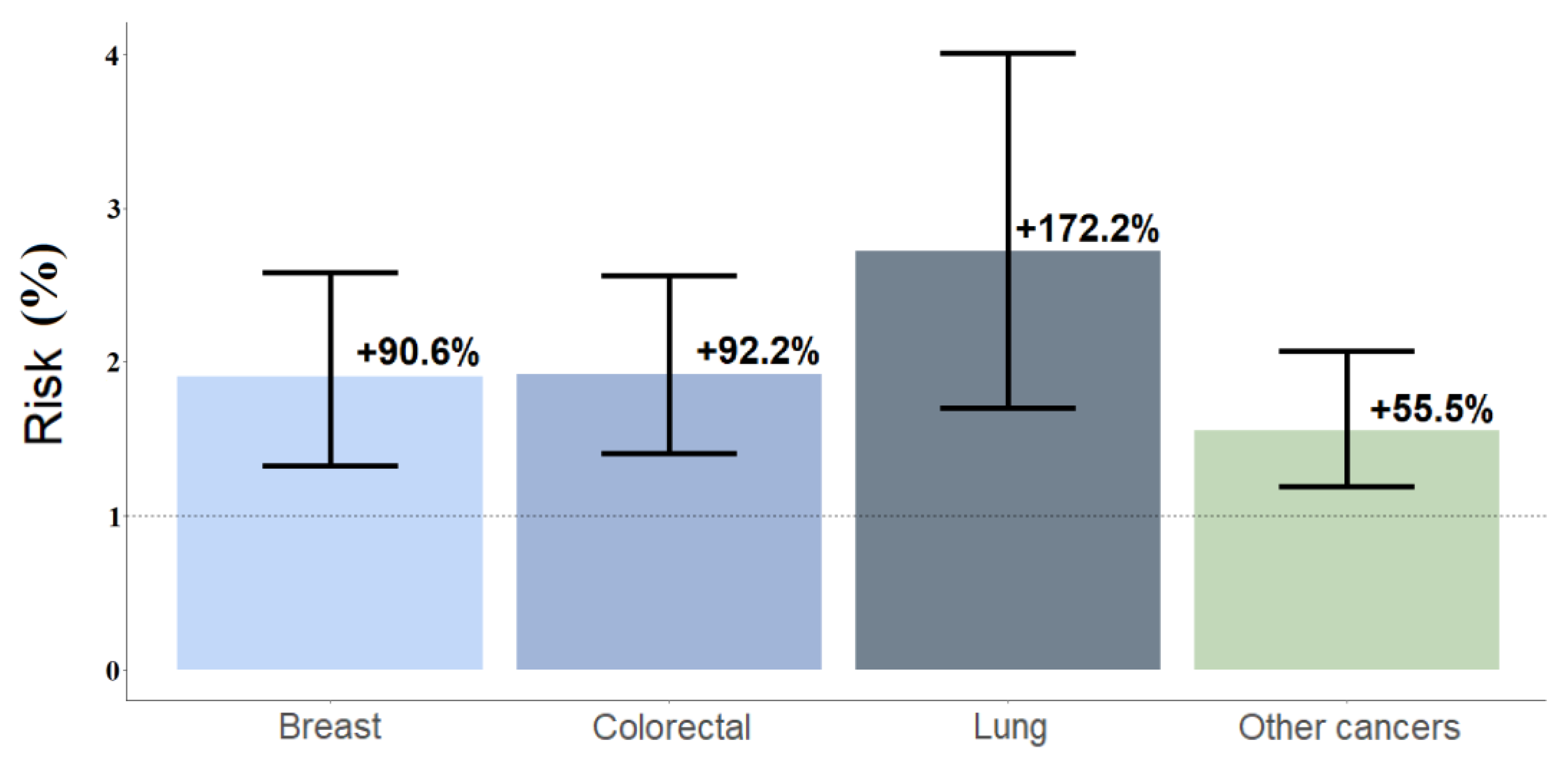
3.3. Risk Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. ESMO Guidelines Committee. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef]
- Farquhar-Smith, P. Clinical practice guidelines for cancer pain: Problems and solutions. Curr. Opin. Support. Palliat. Care 2021, 15, 84–90. [Google Scholar] [CrossRef]
- Hill, B.; Moulin, D.; Sanatani, M. Follow-up Visits and Changes in Pain Scores Reported by Oncology Outpatients after Initial Presentation with Severe Pain. Cureus 2017, 9, e965. [Google Scholar] [CrossRef]
- Cascella, M.; Marinangeli, F.; Vittori, A.; Scala, C.; Piccinini, M.; Braga, A.; Miceli, L.; Vellucci, R. Open Issues and Practical Suggestions for Telemedicine in Chronic Pain. Int. J. Environ. Res. Public Health 2021, 18, 12416. [Google Scholar] [CrossRef]
- Coyne, C.J.; Reyes-Gibby, C.C.; Durham, D.D.; Abar, B.; Adler, D.; Bastani, A.; Bernstein, S.L.; Baugh, C.W.; Bischof, J.J.; Grudzen, C.R.; et al. Cancer pain management in the emergency department: A multicenter prospective observational trial of the Comprehensive Oncologic Emergencies Research Network (CONCERN). Support. Care Cancer 2021, 29, 4543–4553. [Google Scholar] [CrossRef]
- Bramati, P.S.; Amaram-Davila, J.S.; Reddy, A.S.; Bruera, E. Reduction of Missed Palliative Care Appointments after the Implementation of Telemedicine. J. Pain Symptom Manag. 2022, 63, e777–e779. [Google Scholar] [CrossRef]
- Li, J.; Zhu, C.; Liu, C.; Su, Y.; Peng, X.; Hu, X. Effectiveness of eHealth interventions for cancer-related pain, fatigue, and sleep disorders in cancer survivors: A systematic review and meta-analysis of randomized controlled trials. J. Nurs. Scholarsh. 2022, 54, 184–190. [Google Scholar] [CrossRef]
- Rahman, S.; Speed, T.; Xie, A.; Shechter, R.; Hanna, M.N. Perioperative Pain Management during the COVID-19 Pandemic: A Telemedicine Approach. Pain Med. 2021, 22, 3–6. [Google Scholar] [CrossRef]
- Cascella, M.; Miceli, L.; Cutugno, F.; Di Lorenzo, G.; Morabito, A.; Oriente, A.; Massazza, G.; Magni, A.; Marinangeli, F.; Cuomo, A.; et al. A Delphi Consensus Approach for the Management of Chronic Pain during and after the COVID-19 Era. Int. J. Environ. Res. Public Health 2021, 18, 13372. [Google Scholar] [CrossRef]
- Cascella, M.; Del Gaudio, A.; Vittori, A.; Bimonte, S.; Del Prete, P.; Forte, C.A.; Cuomo, A.; De Blasio, E. COVID-Pain: Acute and Late-Onset Painful Clinical Manifestations in COVID-19—Molecular Mechanisms and Research Perspectives. J. Pain Res. 2021, 14, 2403–2412. [Google Scholar] [CrossRef]
- Noorbakhsh-Sabet, N.; Zand, R.; Zhang, Y.; Abedi, V. Artificial Intelligence Transforms the Future of Health Care. Am. J. Med. 2019, 132, 795–801. [Google Scholar] [CrossRef]
- DiMartino, L.; Miano, T.; Wessell, K.; Bohac, B.; Hanson, L.C. Identification of Uncontrolled Symptoms in Cancer Patients Using Natural Language Processing. J. Pain Symptom Manag. 2022, 63, 610–617. [Google Scholar] [CrossRef]
- Cascella, M.; Coluccia, S.; Grizzuti, M.; Romano, M.C.; Esposito, G.; Crispo, A.; Cuomo, A. Satisfaction with Telemedicine for Cancer Pain Management: A Model of Care and Cross-Sectional Patient Satisfaction Study. Curr. Oncol. 2022, 29, 5566–5578. [Google Scholar] [CrossRef]
- Cascella, M. PainDatafor_Telemedicine_ML [Data set]. Zenodo 2022. [Google Scholar] [CrossRef]
- Hu, H.; Yao, W.; Wu, Y. The Robust EM-type Algorithms for Log-concave Mixtures of Regression Models. Comput. Stat. Data Anal. 2017, 111, 14–26. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Natekin, A.; Knoll, A. Gradient boosting machines, a tutorial. Front. Neurorobot. 2013, 7, 21. [Google Scholar] [CrossRef]
- Tian, Y.; Shu, M.; Jia, Q. Artificial Neural Network. In Encyclopedia of Mathematical Geosciences. Encyclopedia of Earth Sciences Series; Daya Sagar, B., Cheng, Q., McKinley, J., Agterberg, F., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Li, Y.; Ji, L.; Oravecz, Z.; Brick, T.R.; Hunter, M.D.; Chow, S.M. dynr.mi: An R Program for Multiple Imputation in Dynamic Modeling. World Acad. Sci. Eng. Technol. 2019, 13, 302–311. [Google Scholar] [CrossRef]
- Kuhn, M. Building Predictive Models in R Using the caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Calton, B.; Abedini, N.; Fratkin, M. Telemedicine in the Time of Coronavirus. J Pain Symptom Manage. 2020, 60, e12–e14. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, M.; Oakden-Rayner, L.; Beam, A.L. The false hope of current approaches to explainable artificial intelligence in health care. Lancet Digit Health 2021, 3, e745–e750. [Google Scholar] [CrossRef]
- Health Resources & Services Administration Telehealth Programs. Available online: https://www.hrsa.gov/rural-health/telehealth (accessed on 26 August 2022).
- Cascella, M.; Crispo, A.; Esposito, G.; Forte, C.A.; Coluccia, S.; Porciello, G.; Amore, A.; Bimonte, S.; Mercadante, S.; Caraceni, A.; et al. Multidimensional Statistical Technique for Interpreting the Spontaneous Breakthrough Cancer Pain Phenomenon. A Secondary Analysis from the IOPS-MS Study. Cancers 2021, 13, 4018. [Google Scholar] [CrossRef]
- Ahmed, Y.; Popovic, M.; Wan, B.A.; Lam, M.; Lam, H.; Ganesh, V.; Milakovic, M.; DeAngelis, C.; Malek, L.; Chow, E. Does gender affect self-perceived pain in cancer patients? -A meta-analysis. Ann. Palliat. Med. 2017, 6, S177–S184. [Google Scholar] [CrossRef]
- Davies, A.N.; Elsner, F.; Filbet, M.J.; Porta-Sales, J.; Ripamonti, C.; Santini, D.; Webber, K. Breakthrough cancer pain (BTcP) management: A review of international and national guidelines. BMJ Support. Palliat. Care 2018, 8, 241–249. [Google Scholar] [CrossRef]
- Cuomo, A.; Cascella, M.; Forte, C.A.; Bimonte, S.; Esposito, G.; De Santis, S.; Cavanna, L.; Fusco, F.; Dauri, M.; Natoli, S.; et al. Careful Breakthrough Cancer Pain Treatment through Rapid-Onset Transmucosal Fentanyl Improves the Quality of Life in Cancer Patients: Results from the BEST Multicenter Study. J. Clin. Med. 2020, 9, 1003. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Collected | Variable(s) |
|---|---|
| Demographic and Social Information | Age Gender |
| Working status (Y/N) Living with a partner * (Y/N) Education level | |
| Clinical Data | Type of primary tumor Bone metastases ECOG-PS |
| Pain Therapy | MED Drugs for NP ROOs PAMORAs IV-Morphine |
| Remote Visits | Number |
| Variable | n = 158 * |
|---|---|
| Age (years) | |
| Mean (SD) | 63 (13) |
| Median (IQR) | 65 (55, 72) |
| Class of Age (years old) | |
| ≤55 | 43 (27%) |
| 56–75 | 86 (54%) |
| >75 | 29 (18%) |
| Gender | |
| Female | 81 (51%) |
| Male | 77 (49%) |
| Working Status (n = 153) | |
| Not Working | 110 (72%) |
| Working | 43 (28%) |
| Education Level (n = 146) | |
| Secondary School | 41 (28%) |
| High School | 68 (47%) |
| Bachelor’s or Higher Degrees | 37 (25%) |
| Living with a Partner (n = 153) | |
| Yes | 107 (70%) |
| No | 46 (30%) |
| Neoplasm | |
| Lung | 22 (14%) |
| Colorectal | 39 (25%) |
| Breast | 21 (13%) |
| Others | 76 (48%) |
| Bone metastases (n = 156) | |
| No | 72 (46%) |
| Yes | 84 (54%) |
| ECOG-PS | |
| ECOG-PS <3 | 84 (53%) |
| ECOG-PS = 3 | 74 (47%) |
| MED | |
| ≤60 mg | 64 (41%) |
| >60 mg | 94 (59%) |
| Assuming ROOs | |
| No | 114 (72%) |
| Yes | 44 (28%) |
| Assuming PAMORAs | |
| No | 125 (79%) |
| Yes | 33 (21%) |
| Assuming drugs for NP | |
| No | 78 (49%) |
| Yes | 80 (51%) |
| Assuming IV-morphine | |
| No | 146 (92%) |
| Yes | 12 (7.6%) |
| Remote consultations (n = 158) | |
| Mean (SD) | 2.27 (2.05) |
| Median (IQR) | 2 (1, 3) |
| Min–Max for Patient | 1–16 |
| Remote consultations (categories) | |
| 1 | 74 (47%) |
| >1 | 84 (53%) |
| Remote Consultations | |||
|---|---|---|---|
| Variable | one, n = 74 * | ≥2, n = 84 * | p-value ^ |
| Age (years) | 0.019 | ||
| n | 74 | 84 | |
| Mean (SD) | 65 (13) | 61 (13) | |
| Median (IQR) | 68 (57, 75) | 62 (53, 70) | |
| Class of Age (years old) | 0.030 | ||
| ≤55 | 13 (18%) | 30 (36%) | |
| 56–75 | 44 (59%) | 42 (50%) | |
| >75 | 17 (23%) | 12 (14%) | |
| Gender | 0.537 | ||
| Female | 36 (49%) | 45 (54%) | |
| Male | 38 (51%) | 39 (46%) | |
| Working Status | 0.987 | ||
| No | 51 (72%) | 59 (72%) | |
| Yes | 20 (28%) | 23 (28%) | |
| (Missing) | 3 | 2 | |
| Education Level | 0.374 | ||
| Secondary School | 22 (33%) | 19 (24%) | |
| High School | 31 (46%) | 37 (47%) | |
| Graduation | 14 (21%) | 23 (29%) | |
| (Missing) | 7 | 5 | |
| Cohabiting/Marriage | 0.711 | ||
| Yes | 50 (71%) | 57 (69%) | |
| No | 20 (29%) | 26 (31%) | |
| (Missing) | 4 | 1 | |
| Cancer Type | 0.516 | ||
| Lung | 8 (11%) | 14 (17%) | |
| Colorectal | 19 (26%) | 20 (24%) | |
| Breast | 8 (11%) | 13 (15%) | |
| Others | 39 (53%) | 37 (44%) | |
| Bone Metastases | 0.458 | ||
| No | 36 (49%) | 36 (43%) | |
| Yes | 37 (51%) | 47 (57%) | |
| (Missing) | 1 | 1 | |
| ECOG-PS | 0.396 | ||
| <3 | 42 (57%) | 42 (50%) | |
| =3 | 32 (43%) | 42 (50%) | |
| MED | |||
| <60 mg | 33 (45%) | 31 (37%) | |
| >60 mg | 41 (55%) | 53 (63%) | |
| Assuming ROOs | 0.829 | ||
| No | 54 (73%) | 60 (71%) | |
| Yes | 20 (27%) | 24 (29%) | |
| Assuming PAMORA | 0.831 | ||
| No | 58 (78%) | 67 (80%) | |
| Yes | 16 (22%) | 17 (20%) | |
| Assuming anti-NP Drugs | 0.269 | ||
| No | 40 (54%) | 38 (45%) | |
| Yes | 34 (46%) | 46 (55%) | |
| Assuming IV-Morphine | 0.115 | ||
| No | 71 (96%) | 75 (89%) | |
| Yes | 3 (4.1%) | 9 (11%) | |
| Classifier | AUC | ACC (tr) | ACC (tst) | L | U | p | Sens (tst) | Spec (tst) | F1 Score | MCC |
|---|---|---|---|---|---|---|---|---|---|---|
| GBM | 0.59 | 0.58 | 0.5 | 0.31 | 0.69 | 0.71 | 0.69 | 0.29 | 0.59 | −0.03 |
| RF | 0.98 | 1 | 0.7 | 0.51 | 0.85 | 0.05 | 0.69 | 0.71 | 0.71 | 0.40 |
| LASSO | 0.5 | 0.53 | 0.53 | 0.34 | 0.72 | 0.57 | 1 | 0 | 0.7 | - |
| ANN | 0.95 | 1 | 0.57 | 0.37 | 0.75 | 0.43 | 0.5 | 0.64 | 0.55 | 0.14 |
| RF | ANN | |||
|---|---|---|---|---|
| One | ≥2 | One | ≥2 | |
| One | 10 | 5 | 9 | 8 |
| ≥ 2 | 4 | 11 | 5 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascella, M.; Coluccia, S.; Monaco, F.; Schiavo, D.; Nocerino, D.; Grizzuti, M.; Romano, M.C.; Cuomo, A. Different Machine Learning Approaches for Implementing Telehealth-Based Cancer Pain Management Strategies. J. Clin. Med. 2022, 11, 5484. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11185484
Cascella M, Coluccia S, Monaco F, Schiavo D, Nocerino D, Grizzuti M, Romano MC, Cuomo A. Different Machine Learning Approaches for Implementing Telehealth-Based Cancer Pain Management Strategies. Journal of Clinical Medicine. 2022; 11(18):5484. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11185484
Chicago/Turabian StyleCascella, Marco, Sergio Coluccia, Federica Monaco, Daniela Schiavo, Davide Nocerino, Mariacinzia Grizzuti, Maria Cristina Romano, and Arturo Cuomo. 2022. "Different Machine Learning Approaches for Implementing Telehealth-Based Cancer Pain Management Strategies" Journal of Clinical Medicine 11, no. 18: 5484. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11185484