
Use of Neuronavigation and Augmented Reality in Transsphenoidal Pituitary Adenoma Surgery
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preoperative Planning
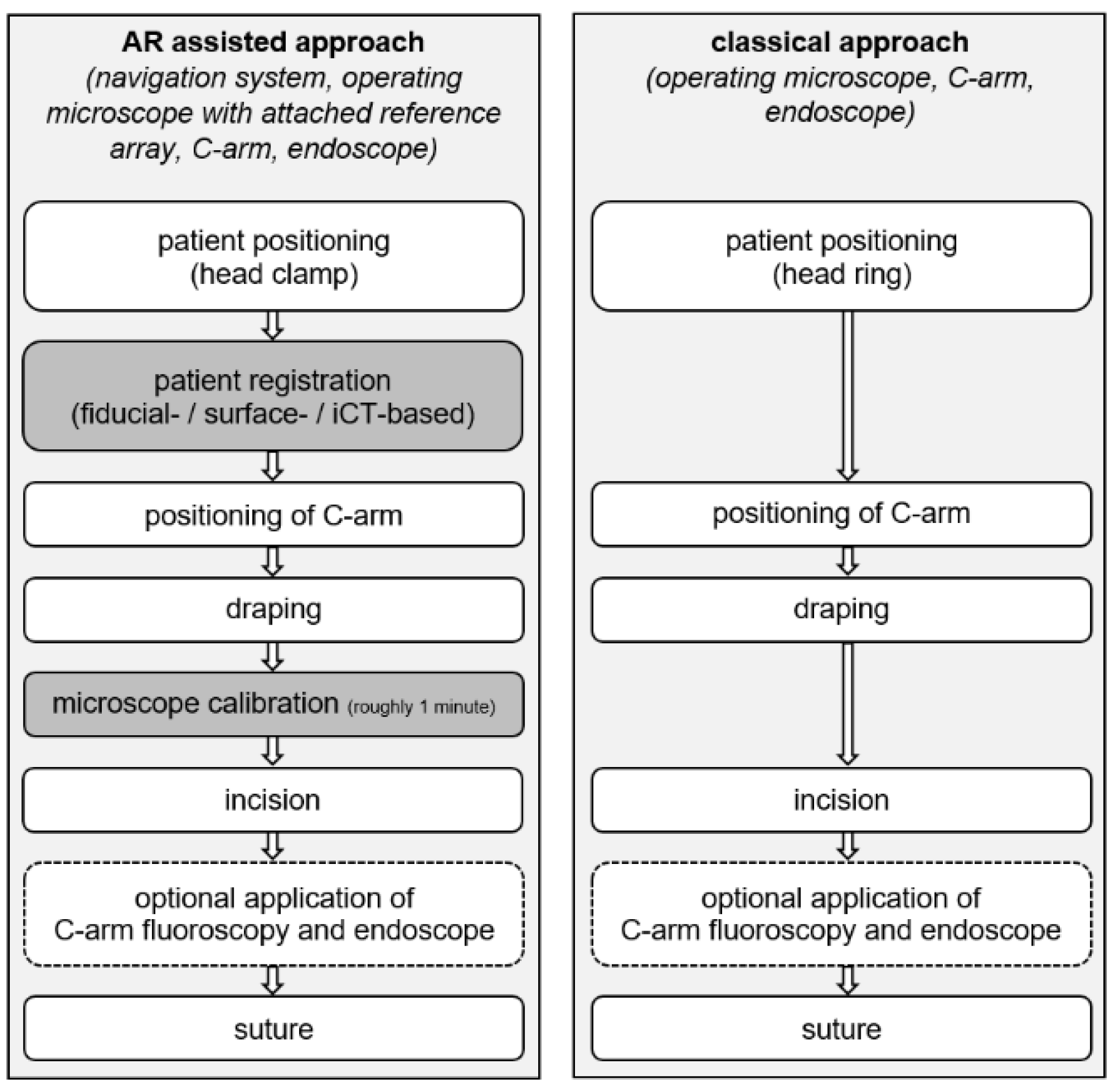
2.2. Patient Positioning and Registration
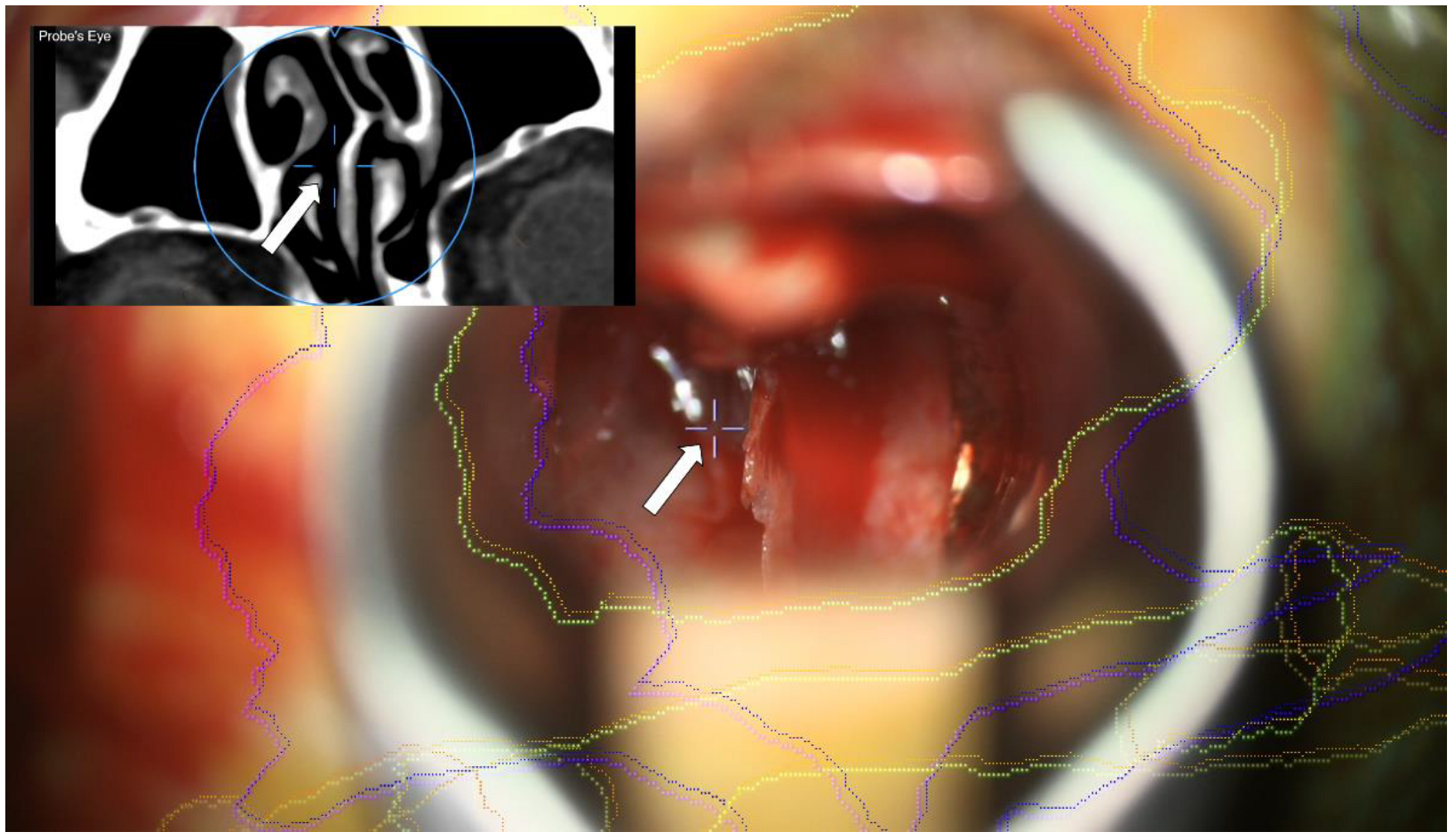
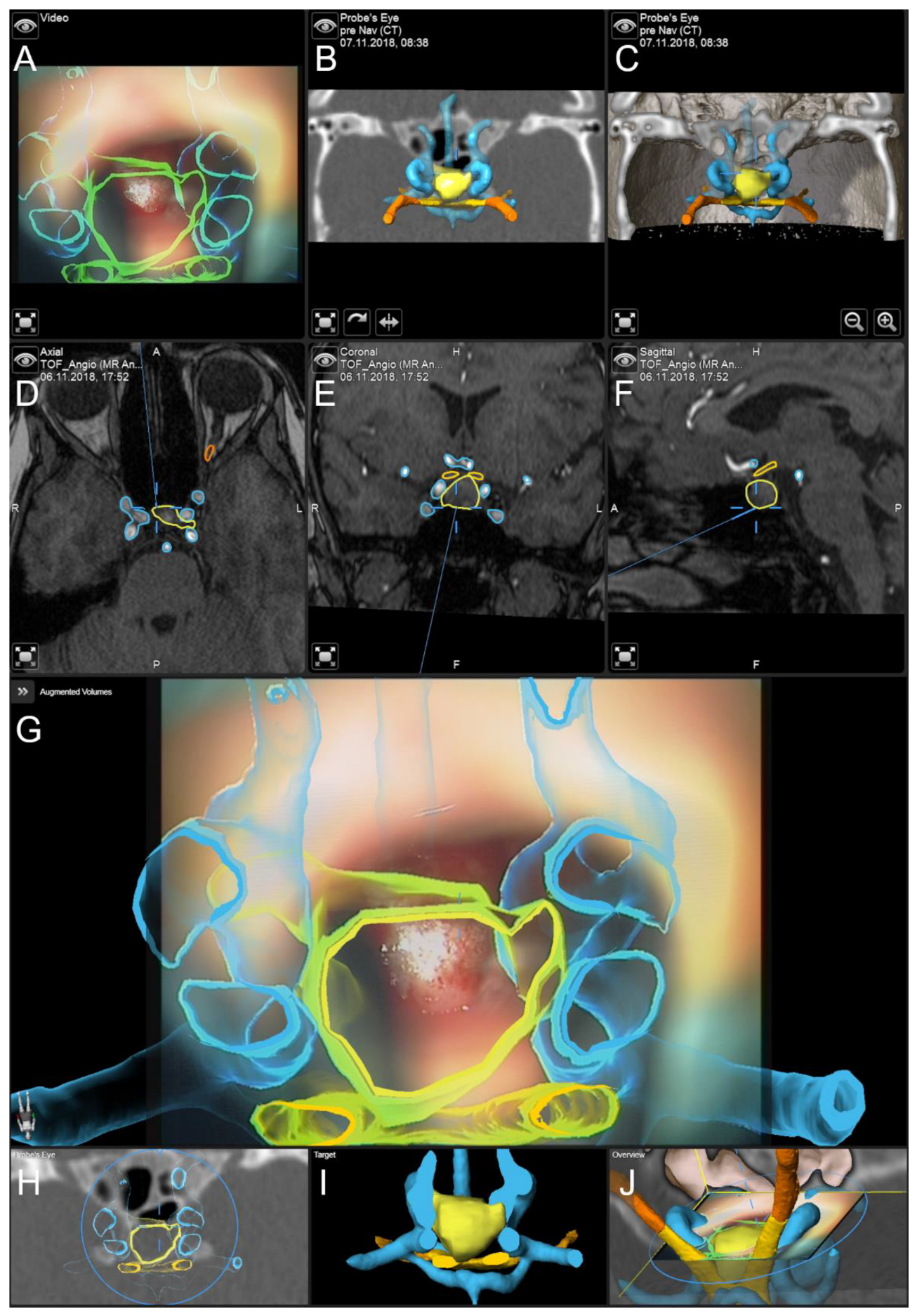
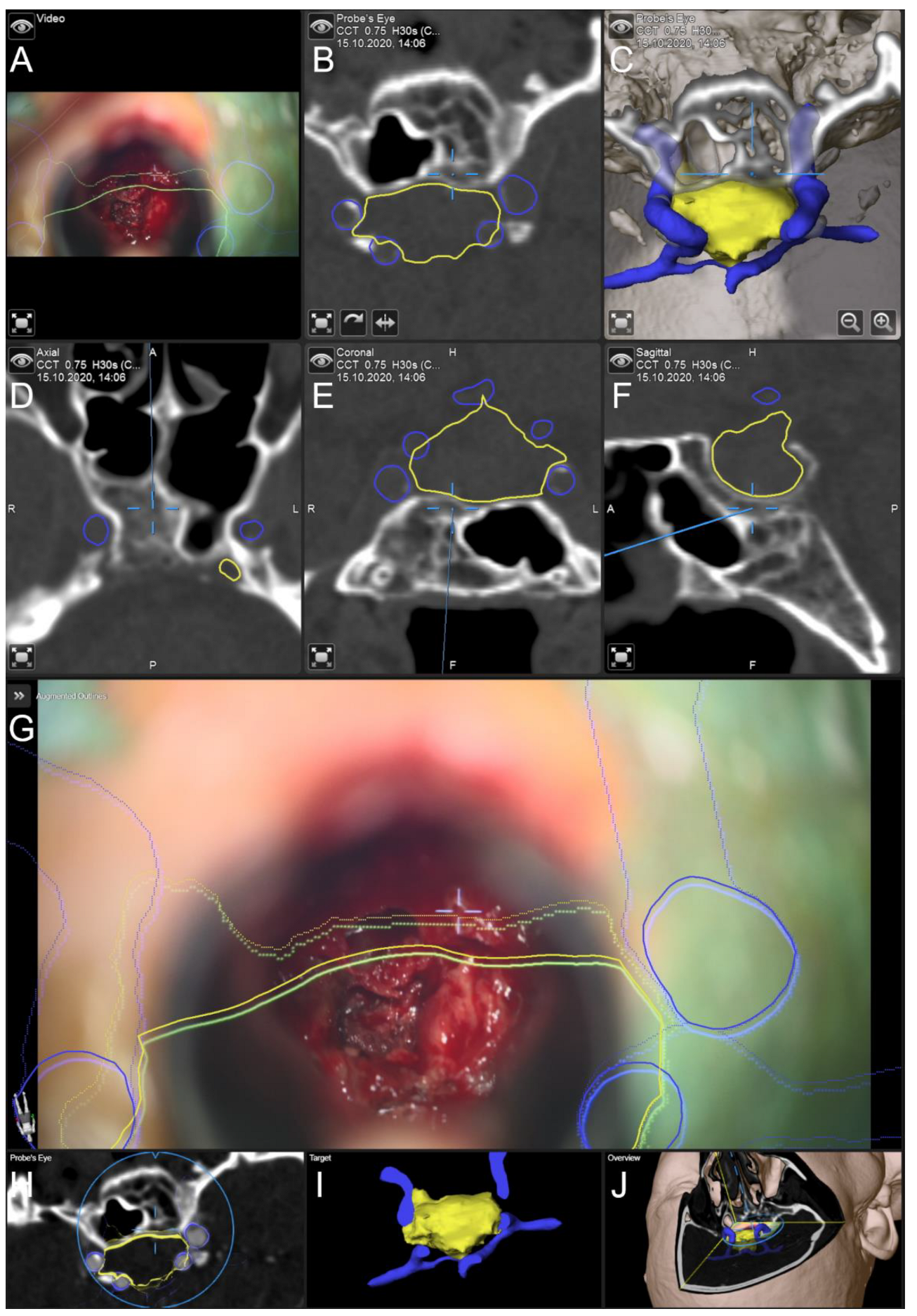
2.3. Augmented Reality
2.4. General Setup
2.5. Data Analysis
- Time for intraoperative patient preparation, defined as the duration between beginning of patient positioning and incision.
- Surgery time, defined as the time between incision and suture
- Occurrence of intraoperative CSF leakage followed by reconstruction of dural defects using autologous fascia lata
- Effective dosage of iCT for intraoperative automatic patient registration
3. Results
Illustrative Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, P.J.; Alker, G.J., Jr.; Goerss, S. Computer-assisted stereotactic microsurgery for the treatment of intracranial neoplasms. Neurosurgery 1982, 10, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Strohbehn, J.W.; Hatch, J.F.; Murray, W.; Kettenberger, H. A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J. Neurosurg. 1986, 65, 545–549. [Google Scholar] [CrossRef] [PubMed]
- King, A.P.; Edwards, P.J.; Maurer, C.R., Jr.; de Cunha, D.A.; Hawkes, D.J.; Hill, D.L.; Gaston, R.P.; Fenlon, M.R.; Strong, A.J.; Chandler, C.L.; et al. A system for microscope-assisted guided interventions. Stereotact. Funct. Neurosurg. 1999, 72, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Kiya, N.; Dureza, C.; Fukushima, T.; Maroon, J.C. Computer navigational microscope for minimally invasive neurosurgery. Min-Minim. Invasive Neurosurg. 1997, 40, 110–115. [Google Scholar] [CrossRef]
- Cabrilo, I.; Bijlenga, P.; Schaller, K. Augmented reality in the surgery of cerebral aneurysms: A technical report. Neurosurgery 2014, 10 (Suppl. 2), 252–260; discussion 260–261. [Google Scholar] [CrossRef]
- Cabrilo, I.; Bijlenga, P.; Schaller, K. Augmented reality in the surgery of cerebral arteriovenous malformations: Technique assessment and considerations. Acta Neurochir. 2014, 156, 1769–1774. [Google Scholar] [CrossRef]
- Cabrilo, I.; Schaller, K.; Bijlenga, P. Augmented reality-assisted bypass surgery: Embracing minimal invasiveness. World Neurosurg. 2015, 83, 596–602. [Google Scholar] [CrossRef]
- Cannizzaro, D.; Zaed, I.; Safa, A.; Jelmoni, A.J.M.; Composto, A.; Bisoglio, A.; Schmeizer, K.; Becker, A.C.; Pizzi, A.; Cardia, A.; et al. Augmented Reality in Neurosurgery, State of Art and Future Projections. A Systematic Review. Front. Surg. 2022, 9, 864792. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Chehab, S.; Bien, S.; Nimsky, C. Preoperative 3-Dimensional Angiography Data and Intraoperative Real-Time Vascular Data Integrated in Microscope-Based Navigation by Automatic Patient Registration Applying Intraoperative Computed Tomography. World Neurosurg. 2018, 113, e414–e425. [Google Scholar] [CrossRef]
- Kersten-Oertel, M.; Chen, S.S.; Drouin, S.; Sinclair, D.S.; Collins, D.L. Augmented reality visualization for guidance in neurovascular surgery. Stud. Health Technol. Inform. 2012, 173, 225–229. [Google Scholar] [PubMed]
- Mascitelli, J.R.; Schlachter, L.; Chartrain, A.G.; Oemke, H.; Gilligan, J.; Costa, A.B.; Shrivastava, R.K.; Bederson, J.B. Navigation-Linked Heads-Up Display in Intracranial Surgery: Early Experience. Oper. Neurosurg. 2018, 15, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.C.; Wang, F.; Chen, X.L.; Yu, X.G.; Ma, X.D.; Zhou, D.B.; Zhu, R.Y.; Xu, B.N. Impact of Virtual and Augmented Reality Based on Intraoperative Magnetic Resonance Imaging and Functional Neuronavigation in Glioma Surgery Involving Eloquent Areas. World Neurosurg. 2016, 96, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Voellger, B.; Sass, B.; Nimsky, C. Augmented Reality in Transsphenoidal Surgery. World Neurosurg. 2019, 125, e873–e883. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, M.; Bopp, M.H.A.; Sabeta, B.; Carl, B.; Nimsky, C. Microscope-Based Augmented Reality with Intraoperative Computed Tomography-Based Navigation for Resection of Skull Base Meningiomas in Consecutive Series of 39 Patients. Cancers 2022, 14, 2302. [Google Scholar] [CrossRef] [PubMed]
- Cabrilo, I.; Sarrafzadeh, A.; Bijlenga, P.; Landis, B.N.; Schaller, K. Augmented reality-assisted skull base surgery. Neurochirurgie 2014, 60, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Brinker, T.; Arango, G.; Kaminsky, J.; Samii, A.; Thorns, U.; Vorkapic, P.; Samii, M. An experimental approach to image guided skull base surgery employing a microscope-based neuronavigation system. Acta Neurochir. 1998, 140, 883–889. [Google Scholar] [CrossRef]
- Kajiwara, K.; Nishizaki, T.; Ohmoto, Y.; Nomura, S.; Suzuki, M. Image-guided transsphenoidal surgery for pituitary lesions using Mehrkoordinaten Manipulator (MKM) navigation system. Min-Minim. Invasive Neurosurg. 2003, 46, 78–81. [Google Scholar] [CrossRef]
- Thomale, U.W.; Stover, J.F.; Unterberg, A.W. The use of neuronavigation in transnasal transsphenoidal pituitary surgery. Zentralbl. Neurochir. 2005, 66, 126–132; discussion 132. [Google Scholar] [CrossRef]
- Sasagawa, Y.; Tachibana, O.; Doai, M.; Hayashi, Y.; Tonami, H.; Iizuka, H.; Nakada, M. Carotid artery protrusion and dehiscence in patients with acromegaly. Pituitary 2016, 19, 482–487. [Google Scholar] [CrossRef]
- Ebner, F.H.; Kuerschner, V.; Dietz, K.; Bueltmann, E.; Naegele, T.; Honegger, J. Reduced intercarotid artery distance in acromegaly: Pathophysiologic considerations and implications for transsphenoidal surgery. Surg. Neurol. 2009, 72, 456–460; discussion 460. [Google Scholar] [CrossRef]
- Hamid, O.; El Fiky, L.; Hassan, O.; Kotb, A.; El Fiky, S. Anatomic Variations of the Sphenoid Sinus and Their Impact on Trans-sphenoid Pituitary Surgery. Skull Base 2008, 18, 9–15. [Google Scholar] [CrossRef]
- Thavarajasingam, S.G.; Vardanyan, R.; Arjomandi Rad, A.; Thavarajasingam, A.; Khachikyan, A.; Mendoza, N.; Nair, R.; Vajkoczy, P. The use of augmented reality in transsphenoidal surgery: A systematic review. Br. J. Neurosurg. 2022, 36, 457–471. [Google Scholar] [CrossRef]
- Ahmadipour, Y.; Lemonas, E.; Maslehaty, H.; Goericke, S.; Stuck, B.A.; El Hindy, N.; Sure, U.; Mueller, O. Critical analysis of anatomical landmarks within the sphenoid sinus for transsphenoidal surgery. Eur. Arch. Otorhinolaryngol. 2016, 273, 3929–3936. [Google Scholar] [CrossRef]
- Ciric, I.; Ragin, A.; Baumgartner, C.; Pierce, D. Complications of transsphenoidal surgery: Results of a national survey, review of the literature, and personal experience. Neurosurgery 1997, 40, 225–236; discussion 236–237. [Google Scholar] [CrossRef]
- Laws, E.R., Jr. Vascular complications of transsphenoidal surgery. Pituitary 1999, 2, 163–170. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Sass, B.; Nimsky, C. Intraoperative computed tomography as reliable navigation registration device in 200 cranial procedures. Acta Neurochir. 2018, 160, 1681–1689. [Google Scholar] [CrossRef]
- Huda, W.; Magill, D.; He, W. CT effective dose per dose length product using ICRP 103 weighting factors. Med. Phys. 2011, 38, 1261–1265. [Google Scholar] [CrossRef]
- Roethe, A.L.; Rosler, J.; Misch, M.; Vajkoczy, P.; Picht, T. Augmented reality visualization in brain lesions: A prospective randomized controlled evaluation of its potential and current limitations in navigated microneurosurgery. Acta Neurochir. 2022, 164, 3–14. [Google Scholar] [CrossRef]
- Onizuka, M.; Tokunaga, Y.; Shibayama, A.; Miyazaki, H. Computer-assisted neurosurgical navigational system for transsphenoidal surgery—Technical note. Neurol. Med. Chir. 2001, 41, 565–568; discussion 569. [Google Scholar] [CrossRef]
- Mert, A.; Micko, A.; Donat, M.; Maringer, M.; Buehler, K.; Sutherland, G.R.; Knosp, E.; Wolfsberger, S. An advanced navigation protocol for endoscopic transsphenoidal surgery. World Neurosurg. 2014, 82, S95–S105. [Google Scholar] [CrossRef]
- Charalampaki, P.; Reisch, R.; Ayad, A.; Welschehold, S.; Conrad, J.; Wuster, C. Image-guided endonasal transsphenoidal microsurgical treatment of recurrent microadenomas of the pituitary gland. Min-Minim. Invasive Neurosurg. 2006, 49, 93–97. [Google Scholar] [CrossRef]
- Dolati, P.; Eichberg, D.; Golby, A.; Zamani, A.; Laws, E. Multimodal Navigation in Endoscopic Transsphenoidal Resection of Pituitary Tumors Using Image-Based Vascular and Cranial Nerve Segmentation: A Prospective Validation Study. World Neurosurg. 2016, 95, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Meola, A.; Cutolo, F.; Carbone, M.; Cagnazzo, F.; Ferrari, M.; Ferrari, V. Augmented reality in neurosurgery: A systematic review. Neurosurg. Rev. 2017, 40, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Leger, E.; Drouin, S.; Collins, D.L.; Popa, T.; Kersten-Oertel, M. Quantifying attention shifts in augmented reality image-guided neurosurgery. Healthc. Technol. Lett. 2017, 4, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Meola, A.; Chang, S.D. Letter: Navigation-Linked Heads-Up Display in Intracranial Surgery: Early Experience. Oper. Neurosurg. 2018, 14, E71–E72. [Google Scholar] [CrossRef]
- Edwards, P.J.; Johnson, L.G.; Hawkes, D.J.; Fenlon, M.R.; Strong, A.J.; Gleeson, M.J. Clinical Experience and Perception in Stereo Augmented Reality Surgical Navigation. In Medical Imaging and Augmented Reality, Proceedings of the 2nd International Workshop, MIAR 2004, Beijing, China, 19–20 August 2004; Springer: Berlin/Heidelberg, Germany, 2004; pp. 369–376. [Google Scholar]
- Su, Y.; Sun, Y.; Hosny, M.; Gao, W.; Fu, Y. Facial landmark-guided surface matching for image-to-patient registration with an RGB-D camera. Int. J. Med. Robot. Comput. Assist. Surg. 2022, 18, e2373. [Google Scholar] [CrossRef]
- West, J.B.; Fitzpatrick, J.M.; Toms, S.A.; Maurer, C.R., Jr.; Maciunas, R.J. Fiducial point placement and the accuracy of point-based, rigid body registration. Neurosurgery 2001, 48, 810–816; discussion 816–817. [Google Scholar] [CrossRef]
- Mitsui, T.; Fujii, M.; Tsuzaka, M.; Hayashi, Y.; Asahina, Y.; Wakabayashi, T. Skin shift and its effect on navigation accuracy in image-guided neurosurgery. Radiol. Phys. Technol. 2011, 4, 37–42. [Google Scholar] [CrossRef]
- Sass, B.; Pojskic, M.; Bopp, M.; Nimsky, C.; Carl, B. Comparing Fiducial-Based and Intraoperative Computed Tomography-Based Registration for Frameless Stereotactic Brain Biopsy. Stereotact. Funct. Neurosurg. 2021, 99, 79–89. [Google Scholar] [CrossRef]
- Nakajima, S.; Atsumi, H.; Kikinis, R.; Moriarty, T.M.; Metcalf, D.C.; Jolesz, F.A.; Black, P.M. Use of cortical surface vessel registration for image-guided neurosurgery. Neurosurgery 1997, 40, 1201–1208; discussion 1208–1210. [Google Scholar] [CrossRef]
- Stieglitz, L.H.; Fichtner, J.; Andres, R.; Schucht, P.; Krahenbuhl, A.K.; Raabe, A.; Beck, J. The silent loss of neuronavigation accuracy: A systematic retrospective analysis of factors influencing the mismatch of frameless stereotactic systems in cranial neurosurgery. Neurosurgery 2013, 72, 796–807. [Google Scholar] [CrossRef]
- Mirota, D.J.; Uneri, A.; Schafer, S.; Nithiananthan, S.; Reh, D.D.; Ishii, M.; Gallia, G.L.; Taylor, R.H.; Hager, G.D.; Siewerdsen, J.H. Evaluation of a system for high-accuracy 3D image-based registration of endoscopic video to C-arm cone-beam CT for image-guided skull base surgery. IEEE Trans. Med. Imaging 2013, 32, 1215–1226. [Google Scholar] [CrossRef]
- Zeiger, J.; Costa, A.; Bederson, J.; Shrivastava, R.K.; Iloreta, A.M.C. Use of Mixed Reality Visualization in Endoscopic Endonasal Skull Base Surgery. Oper. Neurosurg. 2020, 19, 43–52. [Google Scholar] [CrossRef]
- Esposito, F.; Dusick, J.R.; Fatemi, N.; Kelly, D.F. Graded repair of cranial base defects and cerebrospinal fluid leaks in transsphenoidal surgery. Oper. Neurosurg. 2007, 60, 295–303; discussion 303–304. [Google Scholar] [CrossRef]
- Mehta, G.U.; Oldfield, E.H. Prevention of intraoperative cerebrospinal fluid leaks by lumbar cerebrospinal fluid drainage during surgery for pituitary macroadenomas. J. Neurosurg. 2012, 116, 1299–1303. [Google Scholar] [CrossRef]
- Kawamata, T.; Iseki, H.; Shibasaki, T.; Hori, T. Endoscopic augmented reality navigation system for endonasal transsphenoidal surgery to treat pituitary tumors: Technical note. Neurosurgery 2002, 50, 1393–1397. [Google Scholar] [CrossRef]
- Bong, J.H.; Song, H.J.; Oh, Y.; Park, N.; Kim, H.; Park, S. Endoscopic navigation system with extended field of view using augmented reality technology. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1886. [Google Scholar] [CrossRef]
- Nimsky, C.; Rachinger, J.; Iro, H.; Fahlbusch, R. Adaptation of a hexapod-based robotic system for extended endoscope-assisted transsphenoidal skull base surgery. Min-Minim. Invasive Neurosurg. 2004, 47, 41–46. [Google Scholar] [CrossRef]
- Shinomiya, A.; Shindo, A.; Kawanishi, M.; Miyake, K.; Nakamura, T.; Matsubara, S.; Tamiya, T. Usefulness of the 3D virtual visualization surgical planning simulation and 3D model for endoscopic endonasal transsphenoidal surgery of pituitary adenoma: Technical report and review of literature. Interdiscip. Neurosurg. 2018, 13, 13–19. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Cohort (Classical Approach) | Study Cohort (AR Supported) | p-Value | |
|---|---|---|---|
| number of patients | 81 | 84 | - |
| mean age (years) | 55.19 ± 19.24 | 55.95 ± 17.65 | 0.792 4 |
| male/female ratio | 42/39 | 41/43 | 0.696 3 |
| endoscopic assistance | 66 (81.48%) | 63 (75.00%) | 0.314 3 |
| previous surgery | 0 | 17 | - |
| intraoperative CSF leakage | 35 (43.21%) | 36 (42.86%) | 0.964 3 |
| major complications | 0 | 0 | - |
| postoperative CSF fistula | 5 (6.17%) | 3 (3.57%) | 0.437 3 |
| patient preparation time (min) | 32.33 ± 13.35 | 44.13 ± 13.67 | <0.001 4 |
| surgery time (min) | 71.28 ± 29.52 | 69.87 ± 24.71 | 0.739 4 |
| TRE (fiducial) (mm) 1 | n.a. | 1.85 ± 1.02 [0.51; 3.43] | 0.001 5 |
| TRE (iCT) (mm) 1 | n.a. | 0.76 ± 0.33 [0.21; 2.07] | |
| ED (iCT) (mSv) 2 | n.a. | 0.128 ± 0.361 [0.041; 2.556] | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bopp, M.H.A.; Saß, B.; Pojskić, M.; Corr, F.; Grimm, D.; Kemmling, A.; Nimsky, C. Use of Neuronavigation and Augmented Reality in Transsphenoidal Pituitary Adenoma Surgery. J. Clin. Med. 2022, 11, 5590. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195590
Bopp MHA, Saß B, Pojskić M, Corr F, Grimm D, Kemmling A, Nimsky C. Use of Neuronavigation and Augmented Reality in Transsphenoidal Pituitary Adenoma Surgery. Journal of Clinical Medicine. 2022; 11(19):5590. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195590
Chicago/Turabian StyleBopp, Miriam H. A., Benjamin Saß, Mirza Pojskić, Felix Corr, Dustin Grimm, André Kemmling, and Christopher Nimsky. 2022. "Use of Neuronavigation and Augmented Reality in Transsphenoidal Pituitary Adenoma Surgery" Journal of Clinical Medicine 11, no. 19: 5590. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11195590