
Point-of-Care Virtual Surgical Planning and 3D Printing in Oral and Cranio-Maxillofacial Surgery: A Narrative Review
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Collection Process
3. Results
3.1. Selection of Sources of Evidence
3.2. Clinical Applications
3.3. Infrastructure
3.3.1. Housing of Virtual Planning and 3D Printing Infrastructure
3.3.2. Software
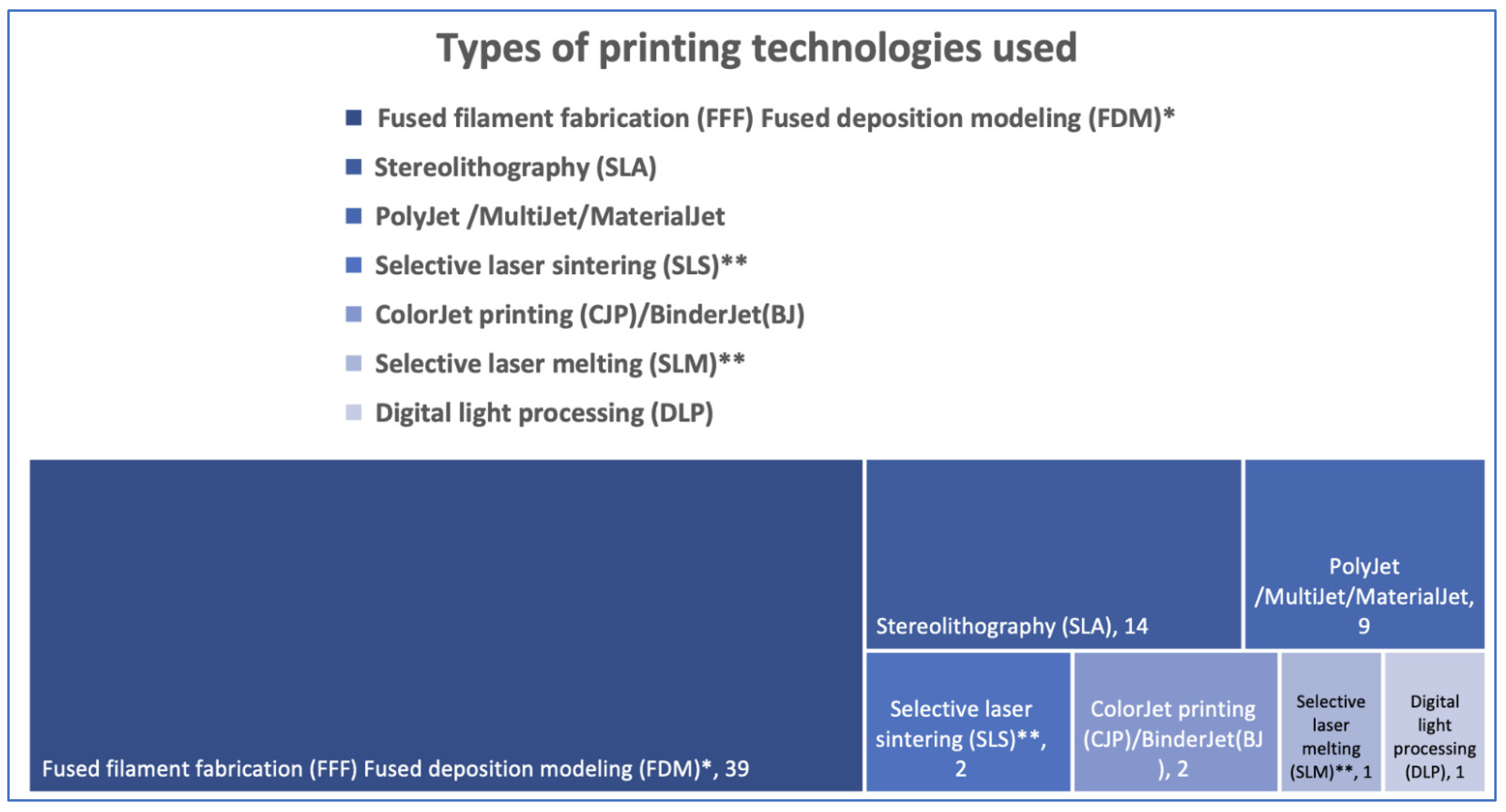
3.3.3. The 3D Printers and Materials Used at Point-of-Care
3.4. Human Resources Involvement
3.5. Time Management for in-House 3DP Products
3.5.1. Planning Time
3.5.2. Three-Dimensional Printing Time
3.5.3. Operating Time
3.6. Costs
3.7. Outcome of Point-of-Care Virtual Planning and 3D Printing
4. Discussion
4.1. Limitations and Strengths
4.2. Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hull, C.W. Apparatus for Production of Three-Dimensional Objects by Stereolithography. U.S. Patent 4575330A, 19 December 1986. [Google Scholar]
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. How useful is 3D printing in maxillofacial surgery? J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Sharkh, H.A.; Makhoul, N. In-House Surgeon-Led Virtual Surgical Planning for Maxillofacial Reconstruction. J. Oral Maxillofac. Surg. 2020, 78, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Zhang, C.-Y.; Choi, W.; Zhu, W.-Y.; Li, D.; Chen, X.-S.; Du, R.; Su, Y.-X. A novel ‘surgeon-dominated’ approach to the design of 3D-printed patient-specific surgical plates in mandibular reconstruction: A proof-of-concept study. Int. J. Oral Maxillofac. Surg. 2019, 49, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Rustemeyer, J.; Melenberg, A.; Sari-Rieger, A. Costs incurred by applying computer-aided design/computer-aided manufacturing techniques for the reconstruction of maxillofacial defects. J. Cranio-Maxillofac. Surg. 2014, 42, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Marschall, J.S.; Dutra, V.; Flint, R.L.; Kushner, G.M.; Alpert, B.; Scarfe, W.; Azevedo, B. In-House Digital Workflow for the Management of Acute Mandible Fractures. J. Oral Maxillofac. Surg. 2019, 77, 2084.e1–2084.e9. [Google Scholar] [CrossRef]
- Arce, K.; Morris, J.M.; Alexander, A.E.; Ettinger, K.S. Developing a Point-of-Care Manufacturing Program for Craniomaxillofacial Surgery. Atlas Oral Maxillofac. Surg. Clin. 2020, 28, 165–179. [Google Scholar] [CrossRef]
- State of the Healthcare Market 2020: Point-of-Care 3D Printing Trends. Available online: https://www.materialise.com/en/blog/healthcare-market-trends-point-of-care (accessed on 20 April 2022).
- Spaas, C.; Lenssen, O. Economic analysis of a low-cost virtual surgical planning protocol for mandibular reconstruction: A case series. Br. J. Oral Maxillofac. Surg. 2019, 57, 743–748. [Google Scholar] [CrossRef]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, C.A.; Lin, A.Y. A New Classification of Three-Dimensional Printing Technologies: Systematic review of three-dimensional printing for patient-specific craniomaxillofacial surgery. Plast. Reconstr. Surg. 2017, 139, 1211–1220. [Google Scholar] [CrossRef]
- Hoang, D.; Perrault, D.; Stevanovic, M.; Ghiassi, A. Surgical applications of three-dimensional printing: A review of the current literature & how to get started. Ann. Transl. Med. 2016, 4, 456. [Google Scholar] [CrossRef]
- Malik, H.H.; Darwood, A.R.; Shaunak, S.; Kulatilake, P.; El-Hilly, A.A.; Mulki, O.; Baskaradas, A. Three-dimensional printing in surgery: A review of current surgical applications. J. Surg. Res. 2015, 199, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Martelli, N.; Serrano, C.; van den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef]
- Lin, H.-H.; Lonic, D.; Lo, L.-J. 3D printing in orthognathic surgery—A literature review. J. Formos. Med. Assoc. 2018, 117, 547–558. [Google Scholar] [CrossRef]
- Murtezani, I.; Sharma, N.; Thieringer, F.M. Medical 3D printing with a focus on Point-of-Care in Cranio- and Maxillofacial Surgery. A systematic review of literature. Ann. 3D Print. Med. 2022, 6, 100059. [Google Scholar] [CrossRef]
- Mendez, B.M.; Chiodo, M.V.; Patel, P.A. Customized “In-Office” Three-Dimensional Printing for Virtual Surgical Planning in Craniofacial Surgery. J. Craniofacial Surg. 2015, 26, 1584–1586. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, P.; Prabhu, S.P.; Flynn, K.; Orbach, D.B.; Smith, E. Optimizing cerebrovascular surgical and endovascular procedures in children via personalized 3D printing. J. Neurosurg. Pediatr. 2015, 16, 584–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottini, M.; Seyed Jafari, S.M.; Shafighi, M.; Schaller, B. New approach for virtual surgical planning and mandibular reconstruction using a fibula free flap. Oral Oncol. 2016, 59, e6–e9. [Google Scholar] [CrossRef] [PubMed]
- Legocki, A.T.; Duffy-Peter, A.; Scott, A.R. Benefits and Limitations of Entry-Level 3-Dimensional Printing of Maxillofacial Skeletal Models. JAMA Otolaryngol.-Head Neck Surg. 2017, 143, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Velasco, I.; Vahdani, S.; Ramos, H. Low-cost Method for Obtaining Medical Rapid Prototyping Using Desktop 3D printing: A Novel Technique for Mandibular Reconstruction Planning. J. Clin. Exp. Dent. 2017, 9, e1103–e1108. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; VanKoevering, K.K.; Kline, S.; Green, G.E.; Arts, H.A. Middle cranial fossa approach to repair tegmen defects assisted by three-dimensionally printed temporal bone models. Laryngoscope 2017, 127, 2347–2351. [Google Scholar] [CrossRef]
- Elegbede, A.; Diaconu, S.C.; McNichols, C.H.; Seu, M.; Rasko, Y.M.; Grant, M.P.; Nam, A.J. Office-Based Three-Dimensional Printing Workflow for Craniomaxillofacial Fracture Repair. J. Craniofacial Surg. 2018, 29, e440–e444. [Google Scholar] [CrossRef] [PubMed]
- Valding, B.; Zrounba, H.; Martinerie, S.; May, L.; Broome, M. Should You Buy a Three-Dimensional Printer? A Study of an Orbital Fracture. J. Craniofacial Surg. 2018, 29, 1925–1927. [Google Scholar] [CrossRef] [PubMed]
- Naros, A.; Weise, H.; Tilsen, F.; Hoefert, S.; Naros, G.; Krimmel, M.; Reinert, S.; Polligkeit, J. Three-dimensional accuracy of mandibular reconstruction by patient-specific pre-bent reconstruction plates using an “in-house” 3D-printer. J. Cranio-Maxillofacial Surg. 2018, 46, 1645–1651. [Google Scholar] [CrossRef] [PubMed]
- Guest, W.; Forbes, D.; Schlosser, C.; Yip, S.; Coope, R.; Chew, J. Imaging-Based 3-Dimensional Printing for Improved Maxillofacial Presurgical Planning: A Single Center Case Series. Can. Assoc. Radiol. J. 2019, 70, 74–82. [Google Scholar] [CrossRef] [Green Version]
- King, C.; Shafi, A.; Burke, E. Optimising the management of concurrent symphyseal/parasymphyseal and bilateral extracapsular condylar fractures using three-dimensional printing. Oral Maxillofac. Surg. 2019, 24, 217–219. [Google Scholar] [CrossRef]
- Hatz, C.R.; Msallem, B.; Aghlmandi, S.; Brantner, P.; Thieringer, F.M. Can an entry-level 3D printer create high-quality anatomical models? Accuracy assessment of mandibular models printed by a desktop 3D printer and a professional device. Int. J. Oral Maxillofac. Surg. 2020, 49, 143–148. [Google Scholar] [CrossRef]
- Hassan, S.; Jelon, A.; Rahim, N.I.H.A.; Yahya, M.A.; Omar, N. Fast and economical protocol for in-house virtual planning and 3D-printed surgical templates in mandibular reconstruction. J. 3D Print. Med. 2020, 4, 83–90. [Google Scholar] [CrossRef]
- Sigron, G.R.; Rüedi, N.; Chammartin, F.; Meyer, S.; Msallem, B.; Kunz, C.; Thieringer, F.M. Three-Dimensional Analysis of Isolated Orbital Floor Fractures Pre- and Post-Reconstruction with Standard Titanium Meshes and “Hybrid” Patient-Specific Implants. J. Clin. Med. 2020, 9, 1579. [Google Scholar] [CrossRef]
- Narita, M.; Takaki, T.; Shibahara, T.; Iwamoto, M.; Yakushiji, T.; Kamio, T. Utilization of desktop 3D printer-fabricated “Cost-Effective” 3D models in orthognathic surgery. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 24. [Google Scholar] [CrossRef]
- Lassausaie, A.; Sesqué, A.; Barthélémy, I.; Depeyre, A. Virtual Surgery Planning and Three-Dimensional Printing Template for Osteotomy of the Zygoma to Correct Untreated Zygomaticomaxillary Complex Fracture. J. Craniofacial Surg. 2020, 31, 1142–1145. [Google Scholar] [CrossRef]
- Akiki, R.K.; Jehle, C.C.; Crozier, J.; Woo, A.S. Using 3D Printing and Mirror Image Modeling in Orbital Floor Reconstruction. J. Craniofacial Surg. 2021, 32, 2465–2467. [Google Scholar] [CrossRef] [PubMed]
- Dvoracek, L.A.; Lee, J.Y.; Unadkat, J.V.; Lee, Y.H.; Thakrar, D.; Losee, J.E.; Goldstein, J.A. Low-Cost, Three-Dimensionally–Printed, Anatomical Models for Optimization of Orbital Wall Reconstruction. Plast. Reconstr. Surg. 2020, 147, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Sigron, G.; Barba, M.; Chammartin, F.; Msallem, B.; Berg, B.-I.; Thieringer, F. Functional and Cosmetic Outcome after Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) with and without the Support of 3D-Printed Orbital Anatomical Models. J. Clin. Med. 2021, 10, 3509. [Google Scholar] [CrossRef]
- Bergeron, L.; Bonapace-Potvin, M.; Bergeron, F. In-house 3D Model Printing for Acute Cranio-maxillo-facial Trauma Sur-gery: Process, Time, and Costs. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3804. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, J.S.; Morris, J.M.; Foley, T.A.; Williamson, E.E.; Leng, S.; McGee, K.P.; Kuhlmann, J.L.; Nesberg, L.E.; Vrtiska, T.J. Three-dimensional Physical Modeling: Applications and Experience at Mayo Clinic. RadioGraphics 2015, 35, 1989–2006. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Feria, J.; Narros, J.L.; Ciriza, G.G.; Roldan-Lora, F.; Schrader, I.M.; Martin-Rodríguez, J.F.; Mir, P. 3D Printing of Diffuse Low-Grade Gliomas Involving Eloquent Cortical Areas and Subcortical Functional Pathways: Technical Note. World Neurosurg. 2021, 147, 164–171.e4. [Google Scholar] [CrossRef] [PubMed]
- Goetze, E.; Gielisch, M.; Moergel, M.; Al-Nawas, B. Accelerated workflow for primary jaw reconstruction with microvascular fibula graft. 3D Print. Med. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosc, R.; Hersant, B.; Carloni, R.; Niddam, J.; Bouhassira, J.; De Kermadec, H.; Bequignon, E.; Wojcik, T.; Julieron, M.; Meningaud, J.-P. Mandibular reconstruction after cancer: An in-house approach to manufacturing cutting guides. Int. J. Oral Maxillofac. Surg. 2017, 46, 24–31. [Google Scholar] [CrossRef]
- Hatamleh, M.M.; Yeung, E.; Osher, J.; Huppa, C. Novel Treatment Planning of Hemimandibular Hyperplasia by the Use of Three-Dimensional Computer-Aided-Design and Computer-Aided-Manufacturing Technologies. J. Craniofacial Surg. 2017, 28, 764–767. [Google Scholar] [CrossRef]
- Ganry, L.; Quilichini, J.; Bandini, C.M.; Leyder, P.; Hersant, B.; Meningaud, J.P. Three-dimensional surgical modelling with an open-source software protocol: Study of precision and reproducibility in mandibular reconstruction with the fibula free flap. Int. J. Oral Maxillofac. Surg. 2017, 46, 946–957. [Google Scholar] [CrossRef]
- Ganry, L.; Hersant, B.; Quilichini, J.; Leyder, P.; Meningaud, J. Use of the 3D surgical modelling technique with open-source software for mandibular fibula free flap reconstruction and its surgical guides. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Numajiri, T.; Morita, D.; Nakamura, H.; Yamochi, R.; Tsujiko, S.; Sowa, Y. Designing CAD/CAM Surgical Guides for Maxillary Reconstruction Using an In-house Approach. J. Vis. Exp. 2018, 138, e58015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orabona, G.D.; Abbate, V.; Maglitto, F.; Bonavolontà, P.; Salzano, G.; Romano, A.; Reccia, A.; Committeri, U.; Iaconetta, G.; Califano, L. Low-cost, self-made CAD/CAM-guiding system for mandibular reconstruction. Surg. Oncol. 2018, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Smithers, F.A.E.; Cheng, K.; Jayaram, R.; Mukherjee, P.; Clark, J.R. Maxillofacial reconstruction using in-house virtual surgical planning. ANZ J. Surg. 2018, 88, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Numajiri, T.; Morita, D.; Nakamura, H.; Tsujiko, S.; Yamochi, R.; Sowa, Y.; Toyoda, K.; Tsujikawa, T.; Arai, A.; Yasuda, M.; et al. Using an In-House Approach to Computer-Assisted Design and Computer-Aided Manufacturing Reconstruction of the Maxilla. J. Oral Maxillofac. Surg. 2017, 76, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Zavattero, E.; Fasolis, M.; Novaresio, A.; Gerbino, G.; Borbon, C.; Ramieri, G. The Shape of Things to Come: In-Hospital Three-Dimensional Printing for Mandibular Reconstruction Using Fibula Free Flap. Laryngoscope 2020, 130, E811–E816. [Google Scholar] [CrossRef] [PubMed]
- McAllister, P.; Watson, M.; Burke, E. A Cost-Effective, In-House, Positioning and Cutting Guide System for Orthognathic Surgery. J. Maxillofac. Oral Surg. 2017, 17, 112–114. [Google Scholar] [CrossRef]
- Beckers, O.; Coppey, E.; Mommaerts, M. Computer-aided design and manufacturing construction of a pilot guide for a bone-anchored epithesis to replace an absent pinna. Int. J. Oral Maxillofac. Surg. 2020, 50, 815–819. [Google Scholar] [CrossRef]
- Ostas, D.; Hedesiu, M.; Roman, C.R.; Cosma, C.; Ciurea, M.; Rotaru, H. Design Workflow for Mandibular Reconstruction. Opportunities and Limitations of In-house Virtual Surgical Planning. J. Med Biol. Eng. 2021, 41, 482–493. [Google Scholar] [CrossRef]
- Mascarenhas, W.; Makhoul, N. Efficient in-house 3D printing of an orthognathic splint for single-jaw cases. Int. J. Oral Maxillofac. Surg. 2021, 50, 1075–1077. [Google Scholar] [CrossRef]
- Maglitto, F.; Orabona, G.D.; Committeri, U.; Salzano, G.; De Fazio, G.R.; Vaira, L.A.; Abbate, V.; Bonavolontà, P.; Piombino, P.; Califano, L. Virtual Surgical Planning and the “In-House” Rapid Prototyping Technique in Maxillofacial Surgery: The Current Situation and Future Perspectives. Appl. Sci. 2021, 11, 1009. [Google Scholar] [CrossRef]
- Šimić, L.; Kopačin, V.; Mumlek, I.; Butković, J.; Zubčić, V. Improved technique of personalised surgical guides generation for mandibular free flap reconstruction using an open-source tool. Eur. Radiol. Exp. 2021, 5, 30. [Google Scholar] [CrossRef] [PubMed]
- Postl, L.; Mücke, T.; Hunger, S.; Bissinger, O.; Malek, M.; Holberg, S.; Burgkart, R.; Krennmair, S. In-house 3D-printed surgical guides for osseous lesions of the lower jaw: An experimental study. Eur. J. Med Res. 2021, 26, 25. [Google Scholar] [CrossRef]
- Ritschl, L.M.; Kilbertus, P.; Grill, F.D.; Schwarz, M.; Weitz, J.; Nieberler, M.; Wolff, K.-D.; Fichter, A.M. In-House, Open-Source 3D-Software-Based, CAD/CAM-Planned Mandibular Reconstructions in 20 Consecutive Free Fibula Flap Cases: An Explorative Cross-Sectional Study with Three-Dimensional Performance Analysis. Front. Oncol. 2021, 11, 3751. [Google Scholar] [CrossRef]
- Hay, J.A.; Smayra, T.; Moussa, R. Customized Polymethylmethacrylate Cranioplasty Implants Using 3-Dimensional Printed Polylactic Acid Molds: Technical Note with 2 Illustrative Cases. World Neurosurg. 2017, 105, 971–979.e1. [Google Scholar] [CrossRef] [PubMed]
- Evins, A.I.; Dutton, J.; Imam, S.S.; Dadi, A.O.; Xu, T.; Cheng, D.; Stieg, P.E.; Bernardo, A. On-Demand Intraoperative 3-Dimensional Printing of Custom Cranioplastic Prostheses. Oper. Neurosurg. 2018, 15, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Morales-Gómez, J.A.; Garcia-Estrada, E.; Leos-Bortoni, J.E.; Delgado-Brito, M.; Flores-Huerta, L.E.; De La Cruz-Arriaga, A.A.; Torres-Díaz, L.J.; de León, R.M.-P. Cranioplasty with a low-cost customized polymethylmethacrylate implant using a desktop 3D printer. J. Neurosurg. 2019, 130, 1721–1727. [Google Scholar] [CrossRef] [Green Version]
- Tel, A.; Tuniz, F.; Fabbro, S.; Sembronio, S.; Costa, F.; Robiony, M. Computer-Guided In-House Cranioplasty: Establishing a Novel Standard for Cranial Reconstruction and Proposal of an Updated Protocol. J. Oral Maxillofac. Surg. 2020, 78, 2297.e1–2297.e16. [Google Scholar] [CrossRef]
- Tel, A.; Tuniz, F.; Sembronio, S.; Costa, F.; Bresadola, V.; Robiony, M. Cubik system: Maximizing possibilities of in-house computer-guided surgery for complex craniofacial reconstruction. Int. J. Oral Maxillofac. Surg. 2021, 50, 1554–1562. [Google Scholar] [CrossRef]
- Pöppe, J.P.; Spendel, M.; Schwartz, C.; Winkler, P.A.; Wittig, J. The “springform” technique in cranioplasty: Custom made 3D-printed templates for intraoperative modelling of polymethylmethacrylate cranial implants. Acta Neurochir. 2021, 164, 679–688. [Google Scholar] [CrossRef]
- Callahan, A.B.; Campbell, A.A.; Petris, C.; Kazim, M. Low-Cost 3D Printing Orbital Implant Templates in Secondary Orbital Reconstructions. Ophthalmic Plast. Reconstr. Surg. 2017, 33, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Abbate, V.; Iaconetta, G.; Califano, L.; Pansini, A.; Bonavolonta, P.; Romano, A.; Salzano, G.; Somma, T.; D’Andrea, L.; Orabona, G.D. Self-Made Rapid Prototyping Technique for Orbital Floor Reconstruction: Showcases for Technical Descriptio. J. Craniofacial Surg. 2019, 30, 2106–2110. [Google Scholar] [CrossRef]
- Menzel, C.L.; Hammacher, A.; Lommen, J.; Schorn, L.K.F.; Handschel, J.; Holtmann, H. Orbit in a Box: A Simplified Technique for Patient-Specific Virtually Planned Orbital Floor Reconstruction. J. Craniofacial Surg. 2020, 31, 1117–1119. [Google Scholar] [CrossRef]
- Honigmann, P.; Sharma, N.; Okolo, B.; Popp, U.; Msallem, B.; Thieringer, F.M. Patient-Specific Surgical Implants Made of 3D Printed PEEK: Material, Technology, and Scope of Surgical Application. BioMed Res. Int. 2018, 2018, 4520636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freiser, M.E.; Ghodadra, A.; Hirsch, B.E.; McCall, A.A. Evaluation of 3D Printed Temporal Bone Models in Preparation for Middle Cranial Fossa Surgery. Otol. Neurotol. 2019, 40, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.C.; Hammer, D.A.; Wentland, T.R.; Kim, R.Y. Immediate Teeth in Fibulas: Planning and Digital Workflow With Point-of-Care 3D Printing. J. Oral Maxillofac. Surg. 2020, 78, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Schön, S.N.; Skalicky, N.; Sharma, N.; Zumofen, D.W.; Thieringer, F.M. 3D-Printer-Assisted Patient-Specific Polymethyl Methacrylate Cranioplasty: A Case Series of 16 Consecutive Patients. World Neurosurg. 2021, 148, e356–e362. [Google Scholar] [CrossRef]
- Cole, T.S.; Graham, D.T.; Wakim, A.A.; Bohl, M.A.; Morgan, C.D.; Catapano, J.S.; Smith, K.A.; Sanai, N.; Lawton, M.T. Local 3-Dimensional Printing of a Calvarium-Anchored Ventricular Catheter Occlusion Device. Neurosurg. Open 2021, 2, okab024. [Google Scholar] [CrossRef]
- Sharma, N.; Aghlmandi, S.; Dalcanale, F.; Seiler, D.; Zeilhofer, H.-F.; Honigmann, P.; Thieringer, F. Quantitative Assessment of Point-of-Care 3D-Printed Patient-Specific Polyetheretherketone (PEEK) Cranial Implants. Int. J. Mol. Sci. 2021, 22, 8521. [Google Scholar] [CrossRef]
- Msallem, B.; Beiglboeck, F.; Honigmann, P.; Jaquiéry, C.; Thieringer, F. Craniofacial Reconstruction by a Cost-Efficient Template-Based Process Using 3D Printing. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1582. [Google Scholar] [CrossRef]
- Liu, Y.; Gao, Q.; Du, S.; Chen, Z.; Fu, J.; Chen, B.; Liu, Z.; He, Y. Fabrication of cerebral aneurysm simulator with a desktop 3D printer. Sci. Rep. 2017, 7, srep44301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamo, D.; Msallem, B.; Sharma, N.; Aghlmandi, S.; Kunz, C.; Thieringer, F.M. Accuracy Assessment of Molded, Patient-Specific Polymethylmethacrylate Craniofacial Implants Compared to Their 3D Printed Originals. J. Clin. Med. 2020, 9, 832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werz, S.M.; Zeichner, S.J.; Berg, B.-I.; Zeilhofer, H.-F.; Thieringer, F. 3D Printed Surgical Simulation Models as educational tool by maxillofacial surgeons. Eur. J. Dent. Educ. 2018, 22, e500–e505. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Brigs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Int. J. Technol. Assess. Health Care 2013, 29, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H.M. Clinical efficacy and effectiveness of 3D printing: A systematic review. BMJ Open 2017, 7, e016891. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostaș, D.; Almășan, O.; Ileșan, R.R.; Andrei, V.; Thieringer, F.M.; Hedeșiu, M.; Rotar, H. Point-of-Care Virtual Surgical Planning and 3D Printing in Oral and Cranio-Maxillofacial Surgery: A Narrative Review. J. Clin. Med. 2022, 11, 6625. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226625
Ostaș D, Almășan O, Ileșan RR, Andrei V, Thieringer FM, Hedeșiu M, Rotar H. Point-of-Care Virtual Surgical Planning and 3D Printing in Oral and Cranio-Maxillofacial Surgery: A Narrative Review. Journal of Clinical Medicine. 2022; 11(22):6625. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226625
Chicago/Turabian StyleOstaș, Daniel, Oana Almășan, Robert R. Ileșan, Vlad Andrei, Florian M. Thieringer, Mihaela Hedeșiu, and Horațiu Rotar. 2022. "Point-of-Care Virtual Surgical Planning and 3D Printing in Oral and Cranio-Maxillofacial Surgery: A Narrative Review" Journal of Clinical Medicine 11, no. 22: 6625. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11226625