
HCV-HIV Chronic Coinfection Prevalence in Amazon Region
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
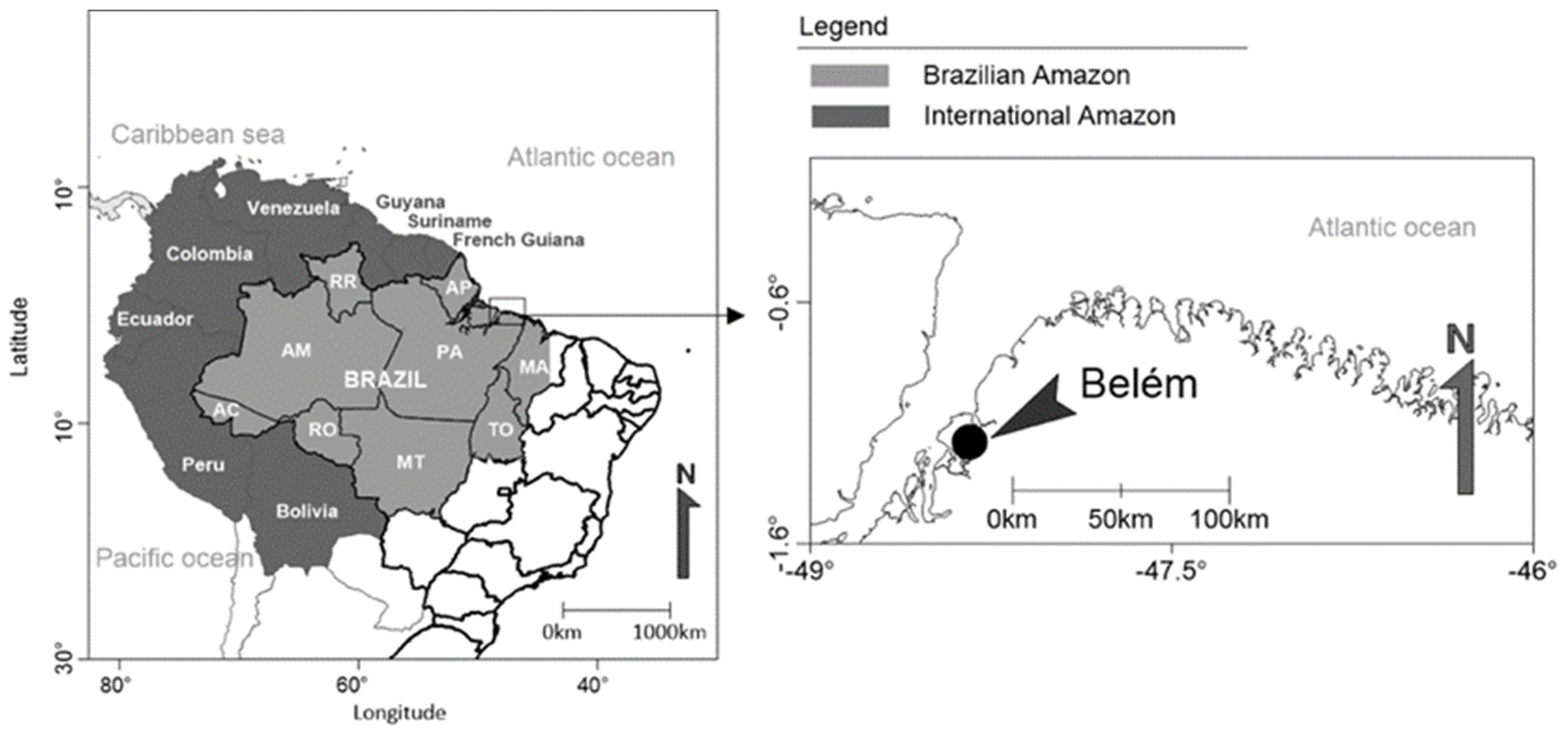
2.1. Type of Study and Sample Collection
2.2. Ethics
2.3. HCV Diagnosis
2.4. Genotyping and Phylogenetic Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Hepatitis C Fact Sheets. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 21 November 2022).
- Messina, J.P.; Humphreys, I.; Flaxman, A.; Brown, A.; Cooke, G.S.; Pybus, O.G.; Barnes, E. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 2015, 61, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, R.; Ahovegbe, L.; Niebel, M.; Shepherd, J.; Thomson, E.C. Non-epidemic HCV genotypes in low- and middle-income countries and the risk of resistance to current direct-acting antiviral regimens. J. Hepatol. 2021, 75, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Castro, G.L.C.; Amoras, E.D.G.S.; Araújo, M.S.M.; Conde, S.R.S.D.S.; Vallinoto, A.C.R. Hepatitis C virus genotypes and associated risk factors in the state of Pará, Northern Brazil. Braz. J. Infect. Dis. 2020, 24, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.M.D.; Peder, L.D.; Thomazella, M.V.; Teixeira, J.J.V.; Bertolini, D.A. Profile of HCV genotypes and HIV-subtypes among HIV-coinfected patients in southern Brazil. Arq. Gastroenterol. 2019, 56, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Lampe, E.; Lewis-Ximenez, L.; Espírito-Santo, M.P.; Delvaux, N.M.; A Pereira, S.; Peres-Da-Silva, A.; Martins, R.M.; A Soares, M.; Santos, A.F.; Vidal, L.L.; et al. Genetic diversity of HCV in Brazil. Antivir. Ther. 2013, 18, 435–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazilian Ministry of Health (BMH)—Health Surveillance Secretary. Hepatitis C [Internet]. 2022. Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/h/hepatites-virais/hepatite-c-1 (accessed on 21 November 2022).
- Brazilian Ministry of Health (BMH)—Health Surveillance Secretary. Annual Epidemiological Bulletin of Viral Hepatitis [Internet]. 2022. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim-epidemiologico-de-hepatite-2021.pdf (accessed on 21 November 2022).
- Nutini, M.F.R.; Hunter, J.; Giron, L.; Pires, A.F.N.P.C.; Kohiyama, I.M.; Camargo, M.; Sucupira, M.C.A.; Benzaken, A.S.; Ferreira, P.A.; Truong, H.-H.M.; et al. HCV genotype profile in Brazil of mono-infected and HIV co-infected individuals: A survey representative of an entire country. PLoS ONE 2020, 15, e0227082. [Google Scholar] [CrossRef]
- Sawada, L.; Pinheiro, A.; Locks, D.; Pimenta, A.; Rezende, P.; Crespo, D.; Crescente, J.; Lemos, J.; Oliveira-Filho, A. Distribution of hepatitis C virus genotypes among different exposure categories in the State of Pará, Brazilian Amazon. Rev. Soc. Bras. Med. Trop. 2011, 44, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Sikavi, C.; Chen, P.H.; Lee, A.D.; Saab, E.G.; Choi, G.; Saab, S. Hepatitis C and human immunodeficiency virus coinfection in the era of direct-acting antiviral agents: No longer a difficult-to-treat population. Hepatology 2018, 67, 847–857. [Google Scholar] [CrossRef] [Green Version]
- Távora, L.G.; Hyppolito, E.B.; Cruz, J.N.; Portela, N.M.; Pereira, S.M.; Veras, C.M. Hepatitis B, C and HIV co-infections seroprevalence in a northeast Brazilian center. Arq. Gastroenterol. 2013, 50, 277–280. [Google Scholar] [CrossRef] [Green Version]
- Freitas, S.Z.; Teles, S.A.; Lorenzo, P.C.; Puga, M.A.M.; Tanaka, T.S.O.; Thomaz, D.Y.; Martins, R.M.B.; Druzian, A.F.; Lindenberg, A.S.C.; Torres, M.S.; et al. HIV and HCV coinfection: Prevalence, associated factors and genotype characterization in the Midwest Region of Brazil. Rev. Inst. Med. Trop. Paulo 2014, 56, 517–524. [Google Scholar] [CrossRef]
- Brandão, N.A.; Pfrimer, I.A.; Martelli, C.M.; Turchi, M.D. Prevalence of hepatitis B and C infection and associated factors in people living with HIV in Midwestern Brazil. Braz. J. Infect. Dis. 2015, 19, 426–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menezes, T.O.; Rodrigues, M.C.; Nogueira, B.M.; Menezes, S.A.; Silva, S.H.; Vallinoto, A.C. Oral and systemic manifestations in HIV-1 patients. Rev. Soc. Bras. Med. Trop. 2015, 48, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Enomoto, N.; Takada, A.; Nakao, T.; Date, T. There are two major types of hepatitis C virus in Japan. Biochem. Biophys. Res. Commun. 1990, 170, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, A.; Aires, D.; Cavalcante, N.; Raiol, N.; Lisboa, B.; Frade, P.; da Costa, L.; Pinheiro, L.M.L.; Machado, L.F.A.; Martins, L.C.; et al. Hepatitis C Virus among Female Sex Workers: A Cross-Sectional Study Conducted along Rivers and Highways in the Amazon Region. Pathogens 2019, 8, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, A. AliView: A fast and lightweight alignment viewer and editor for large datasets. Bioinformatics 2014, 30, 3276–3278. [Google Scholar] [CrossRef] [Green Version]
- Kalaghatgi, P.; Sikorski, A.M.; Knops, E.; Rupp, D.; Sierra, S.; Heger, E.; Neumann-Fraune, M.; Beggel, B.; Walker, A.; Timm, J.; et al. Geno2pheno[HCV]—A Web-based Interpretation System to Support Hepatitis C Treatment Decisions in the Era of Direct-Acting Antiviral Agents. PLoS ONE 2016, 11, e0155869. [Google Scholar] [CrossRef]
- Guindon, S.; Dufayard, J.; Lefort, V.; Anisimova, M.; Hordijk, W.; Gascuel, O. New algorithms and methods to estimate maximum-likelihood phylogenies: Assessing the performance of PhyML 3.0. Syst. Biol. 2010, 59, 307–321. [Google Scholar] [CrossRef] [Green Version]
- Lefort, V.; Longueville, J.; Gascuel, O. SMS: Smart Model Selection in PhyML. Mol. Biol. Evol. 2017, 34, 2422–2424. [Google Scholar] [CrossRef] [Green Version]
- Singer, J.B.; Thomson, E.C.; Hughes, J.; Aranday-Cortes, E.; McLauchlan, J.; Filipe, A.D.S.; Tong, L.; Manso, C.F.; Gifford, R.J.; Robertson, D.L.; et al. Interpreting Viral Deep Sequencing Data with GLUE. Viruses 2019, 11, 323. [Google Scholar] [CrossRef] [Green Version]
- Busek, S.U.; Babá, E.H.; Tavares Filho, H.A.; Pimenta, L.; Salomão, A.; Corrêa-Oliveira, R.; Oliveira, G.C. Hepatitis C and hepatitis B virus infection in different hemodialysis units in Belo Horizonte, Minas Gerais, Brazil. Memórias Inst. Oswaldo Cruz 2002, 97, 775–778. [Google Scholar] [CrossRef]
- da Silva, N.M.; Germano, F.N.; Mendoza-Sassi, R.A.; Seuánez, H.N.; Soares, M.A.; de Martinez, A.M. Evidence of association between hepatitis C virus genotype 2b and nosocomial transmissions in hemodialysis centers from southern Brazil. Virol. J. 2013, 29, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jesus Rodrigues de Freitas, M.; Fecury, A.A.; de Almeida, M.K.; Freitas, A.S.; de Souza Guimarães, V.; da Silva, A.M.; da Costa, Y.F.; da Costa, R.A.A.; Ferreira, P.; Martins, L.C. Prevalence of hepatitis C virus infection and genotypes in patient with chronic kidney disease undergoing hemodialysis. J. Med. Virol. 2013, 85, 1741–1745. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, A.B.; Sawada, L.; Pinto, L.C.; Locks, D.; Bahia, S.L.; Castro, J.A.; Hermes, R.B.; Brasil-Costa, I.; Amaral, C.M.; Lemos, J.A.R. Epidemiological aspects of HCV infection in non-injecting drug users in the Brazilian state of Pará, eastern Amazon. Virol. J. 2014, 25, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacheco, S.D.; Silva-Oliveira, G.C.; Maradei-Pereira, L.M.; Crescente, J.Â.; Lemos, J.A.; Oliveira-Filho, A.B. Prevalence of HCV infection and associated factors among illicit drug users in Breves, State of Pará, northern Brazil. Rev. Soc. Bras. Med. Trop. 2014, 47, 367–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, F.Q.; Santos, F.J.A.; Andrade, A.P.; Pacheco, S.D.B.; Fischer, B.; Pinho, J.R.R.; Lemos, J.A.R.; Oliveira-Filho, A.B. Hepatitis C virus infection among illicit drug users in an archipelago of the Amazon. Arch. Virol. 2018, 163, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, A.B.; Santos, F.J.A.; Silva, F.Q.; Raiol, N.C.; Costa, C.C.S.; Piauiense, J.N.F.; Martins, L.C.; Cardoso, Y.M.N.; Di Miceli, J.F.F.; Resque, R.L.; et al. Hepatitis C virus infection status and associated factors among a multi-site sample of people who used illicit drugs in the Amazon region. BMC Infect. Dis. 2019, 19, 634. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, A.B.; Pimenta, A.S.; Rojas, M.F.; Chagas, M.C.; Crescente, J.A.; Crespo, D.M.; Lemos, J.A. Prevalence and genotyping of hepatitis C virus in blood donors in the state of Pará, Northern Brazil. Memórias Inst. Oswaldo Cruz 2010, 105, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, V.; Melo, T.; Ferreira, R.; Almeida, S.; Martins, L. Prevalence of hepatitis C virus genotypes in the State of Pará, Brazil. Rev. Soc. Bras. Med. Trop. 2018, 51, 508–512. [Google Scholar] [CrossRef]
- Markov, P.V.; van de Laar, T.J.; Thomas, X.V.; Aronson, S.J.; Weegink, C.J.; Berk, G.E.V.D.; Prins, M.; Pybus, O.G.; Schinkel, J. Colonial history and contemporary transmission shape the genetic diversity of hepatitis C virus genotype 2 in Amsterdam. J. Virol. 2012, 86, 7677–7687. [Google Scholar] [CrossRef] [Green Version]
- Park, H.K.; Lee, S.S.; Bin Im, C.; Im, C.; Cha, R.R.; Kim, W.S.; Cho, H.C.; Lee, J.M.; Kim, H.J.; Kim, T.H.; et al. Hepatitis C virus genotype affects survival in patients with hepatocellular carcinoma. BMC Cancer 2019, 19, 822. [Google Scholar] [CrossRef]
- da Silva, D.L.; Nunes, H.M.; Freitas, P.E.B. Natural prevalence of NS3 gene resistance-associated substitutions (RASs) in patients with chronic hepatitis C from the state of Pará/Brazil. Virus Res. 2021, 15, 198251. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.; Wang, C.; Cheng, J.; Chen, W.; Bair, M.; Lo, C. Sofosbuvir-based regimen for genotype 2 HCV infected patients in Taiwan: A real world experience. PLoS ONE 2020, 15, e0227424. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Information | |
|---|---|
| Age (years) | 63 years |
| Sex | Male |
| HIV diagnosed (years) | 7 years (2010) |
| Sexual orientation | Heterosexual |
| Marital status | Single |
| Smoking status | Occasionally |
| Drinking status | Occasionally |
| Illegal drugs | Never used |
| HIV-related medications | Tenofovir + Lamivudine + Efavirenz (300 mg + 300 mg + 600 mg/day) |
| Laboratory values | |
| CD4 T lymphocyte (cells/mm3) | 4.610 cells/mm3 |
| Leukocytes count (cells/mm3) | 846 cells/mm3 |
| Hemoglobin (g/dL) | 35.6 g/dL |
| Platelet count (per μL) | 219.000/μL |
| Viral load (copies/mL) | Undetectable |
| Anti-HCV antibodies | Detected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobo, M.N.; Irias, S.D.F.; Neto, P.L.F.; Avelino, M.E.S.; da Silva Torres, M.K.; de Carvalho Souza, M.; Fonseca, R.R.S.; Freitas, P.E.B.; Nunes, H.M.; de Araújo Júnior, J.R.R.; et al. HCV-HIV Chronic Coinfection Prevalence in Amazon Region. J. Clin. Med. 2022, 11, 7284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247284
Lobo MN, Irias SDF, Neto PLF, Avelino MES, da Silva Torres MK, de Carvalho Souza M, Fonseca RRS, Freitas PEB, Nunes HM, de Araújo Júnior JRR, et al. HCV-HIV Chronic Coinfection Prevalence in Amazon Region. Journal of Clinical Medicine. 2022; 11(24):7284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247284
Chicago/Turabian StyleLobo, Marcio Nahum, Susan Denice Flores Irias, Pedro Leão Fontes Neto, Maria Eduarda Sousa Avelino, Maria Karoliny da Silva Torres, Marlinda de Carvalho Souza, Ricardo Roberto Souza Fonseca, Pedro Eduardo Bonfim Freitas, Heloisa Marceliano Nunes, José Raul Rocha de Araújo Júnior, and et al. 2022. "HCV-HIV Chronic Coinfection Prevalence in Amazon Region" Journal of Clinical Medicine 11, no. 24: 7284. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247284