
Effect of Preoperative Anxiety on Postoperative Pain after Craniotomy

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galvin, I.M.; Levy, R.; Day, A.G.; Gilron, I. Interventions for the prevention of acute postoperative pain in adults following brain surgery. Cochrane Database Syst. Rev. 2019, 2019, CD011931. [Google Scholar] [CrossRef] [PubMed]
- Kotak, D.; Cheserem, B.; Solth, A. A survey of post-craniotomy analgesia in British neurosurgical centres: Time for perceptions and prescribing to change? Br. J. Neurosurg. 2009, 23, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Valero, R.; Carrero, E.; Fàbregas, N.; Iturri, F.; Saiz-Sapena, N.; Valencia, L. National survey on postoperative care and treatment circuits in neurosurgery. Rev. Esp. AnestesiolReanim. 2017, 64, 441–452. [Google Scholar] [CrossRef]
- Vacas, S.; Van de Wiele, B. Designing a pain management protocol for craniotomy: A narrative review and consideration of promising practices. Surg. Neurol. Int. 2017, 8, 291. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.M.H.; Hartley, R.L.; Leung, A.A.; Ronksley, P.E.; Jetté, N.; Casha, S.; Riva-Cambrin, J. Preoperative predictors of poor acute postoperative pain control: A systematic review and meta-analysis. BMJ Open 2019, 9, e025091. [Google Scholar] [CrossRef]
- Carl, R.; Wajer, H.I.; Robe, P.; van Zandvoort, M.L. Anxiety in the pre-operative phase of awake brain tumor surgery. Clin. Neurol. Neurosurg. 2017, 157, 7–10. [Google Scholar]
- Perks, A.; Chakravarti, S.; Manninen, P. Preoperative anxiety in neurosurgical patients. J. Neurosurg. Anesthesiol. 2009, 21, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Oteri, V.; Martinelli, A.; Crivellaro, E.; Gigli, F. The impact of preoperative anxiety on patients undergoing brain surgery: A systematic review. Neurosurg. Rev. 2021, 44, 3047–3057. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Spielberger, C.D. Assessment of state and trait anxiety: Conceptual and methodological issues. South Psychol. 1985, 2, 6–16. [Google Scholar]
- Bermúdez, J. Anxiety and performance. Rev. Psicol. Gen. Apl. 1978, 151, 183–207. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R. Manual del Cuestionario de Ansiedad Estado-Rasgo (STAI); TEA Ediciones: Madrid, Spain, 1982. [Google Scholar]
- Vittorio Stumpo, V.; Staartjes, E.; Quddusi, A.; Corniola, M.V.; Tessitore, E.; Schröder, M.L.; Anderer, E.G.; Stienen, M.N.; Serra, S.; Regli, L. Enhanced Recovery After Surgery strategies for elective craniotomy: A systematic review. J. Neurosurg. 2021, 135, 1857–1881. [Google Scholar] [CrossRef]
- Liu, B.; Liu, S.; Wang, Y.; Zhao, B.; Zhao, T.; Zhao, L.; Lv, W.; Zhang, Y.; Zheng, T.; Xue, Y.; et al. Neurosurgical enhanced recovery after surgery (ERAS) programme for elective craniotomies: Are patients satisfied with their experiences? A quantitative and qualitative analysis. BMJ Open 2019, 9, e028706. [Google Scholar] [CrossRef]
- Peng, K.; Jin, X.H.; Liu, S.L.; Ji, F.H. Effect of intraoperative dexmedetomidine on post-craniotomy pain. Clin. Ther. 2015, 37, 1114–1121.e1. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Ji, Q.; Sun, Q.; Gao, T.; Liu, K.; Li, L. The opioid-sparing effect of intraoperative dexmedetomidine infusion after craniotomy. J. Neurosurg. Anesthesiol. 2016, 28, 14–20. [Google Scholar] [CrossRef]
- Iturri, F.; Valencia, L.; Honorato, C.; Martínez, A.; Valero, R.; Fàbregas, N. Narrative review of acute post-craniotomy pain. Concept and strategies for prevention and treatment of pain. Rev. Esp. Anestesiol. Reanim. 2020, 67, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Powell, R.; Scott, N.W.; Manyande, A.; Bruce, J.; Vögele, C.; Byrne-Davis, L.M.; Unsworth, M.; Osmer, C.; Johnston, M. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst. Rev. 2016, 5, CD008646. [Google Scholar] [CrossRef] [PubMed]
- Hejrati, N.; Spieler, D.; Samuel, R.; Regli, L.; Weyerbrock, A.; Surbeck, W. Conscious Experience and Psychological Consequences of Awake Craniotomy. World Neurosurg. 2019, 129, e381–e386. [Google Scholar] [CrossRef] [PubMed]
- Peduto, V.A.; Chevallier, P.; Casati, A. A multicenter survey on anaesthesia practice in Italy. Minerva Anestesiol. 2004, 70, 473–491. [Google Scholar]
- Pranckeviciene, A.; Deltuva, V.P.; Tamasauskas, A.; Bunevicius, A. Association between psychological distress, subjective cognitive complaints and objective neuropsychological functioning in brain tumor patients. Clin. Neurol. Neurosurg. 2017, 163, 18–23. [Google Scholar] [CrossRef]
- Taphoorn, M.J.B.; Klein, M. Cognitive deficits in adult patients with brain tumours. Lancet Neurol. 2004, 3, 159–168. [Google Scholar] [CrossRef]
- Moerman, N.; van Dam, F.S.; Muller, M.J.; Oosting, H. The Amsterdam preoperative anxiety and information scale (APAIS). Anesth. Analg. 1996, 82, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snait, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theunissen, M.; Peters, M.L.; Bruce, J.; Gramke, H.F.; Marcus, M.A. Preoperative anxiety and catastrophizing: A systematic review and meta-analysis of the association with chronic postsurgical pain. Clin. J. Pain 2012, 28, 819–841. [Google Scholar] [CrossRef]
- Sobol-Kwapinska, M.; Bąbel, P.; Plotek, W.; Stelcer, B. Psychological correlates of acute postsurgical pain: A systematic review and meta-analysis. Eur. J. Pain 2016, 20, 1573–1586. [Google Scholar] [CrossRef] [PubMed]
- Goebel, S.; Mehdorn, H.M. Assessment of preoperative anxiety in neurosurgical patients: Comparison of widely used measures and recommendations for clinic and research. Clin. Neurol. Neurosurg. 2018, 172, 62–68. [Google Scholar] [CrossRef]
- Mordhorst, C.; Latz, B.; Kerz, T.; Wisser, G.; Schmidt, A.; Schneider, A.; Jahn-Eimermacher, A.; Werner, C.; Engelhard, K. Prospective assessment of postoperative pain after craniotomy. J. Neurosurg. Anesthesiol. 2010, 22, 202–206. [Google Scholar] [CrossRef]



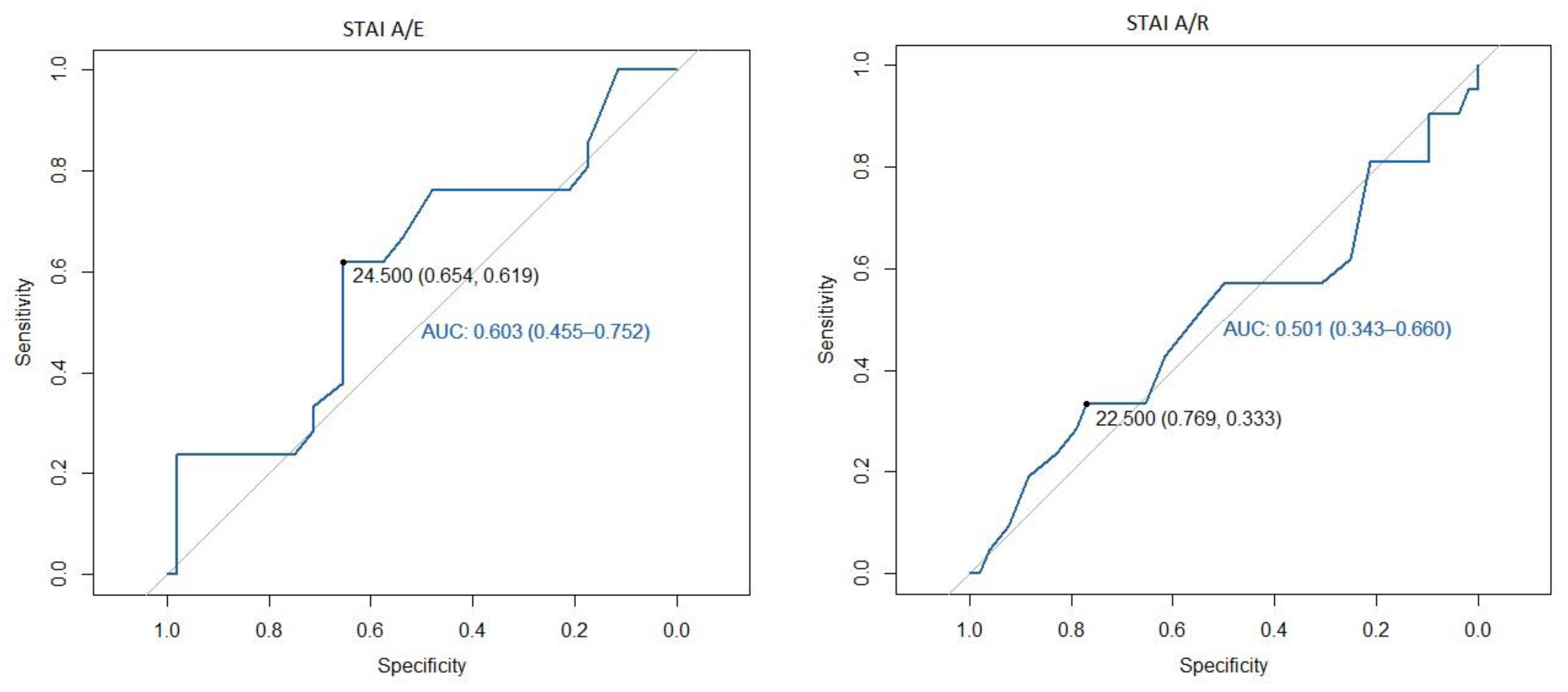{kind=link}
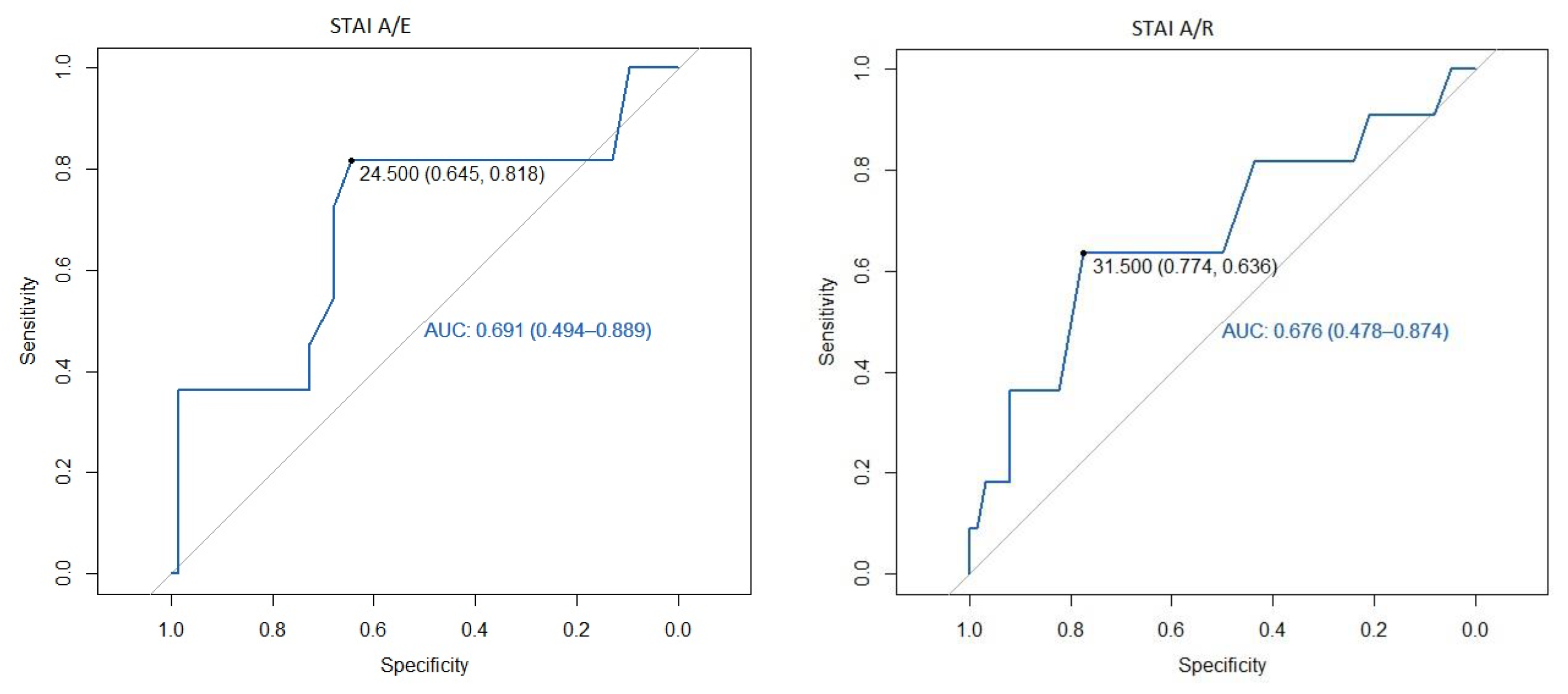{kind=link}
| Study Population (n = 73) | ||
|---|---|---|
| Age, years | 55 ± 15 | |
| Female, No. (%) | 45 (61.6) | |
| BMI, kg·m−1 | 24.9 ± 5.5 | |
| ASA 3, No. (%) | 38 (52.1) | |
| Medical history | ||
| Depression, No. (%) | 16 (21.9) | |
| Anxiety, No. (%) | 5 (6.9) | |
| Rheumatological diseases, No. (%) | 4 (5.5) | |
| Previous use of drugs | ||
| Metamizole, No. (%) | 27 (36.9) | |
| Corticosteroids, No. (%) | 22 (30.1) | |
| Antidepressants, No. (%) | 14 (19.2) | |
| Chronic use of analgesics, No. (%) | 12 (16.4) | |
| Educational level: Basic elementary education, No. (%) | 43 (58.9) | |
| MMSE, points | 28.9 ± 1.3 | |
| STAI A/E, score | 22.4 ± 10.8 | |
| STAI A/R, score | 26.9 ± 7.5 | |
| Main diagnosis: tumoral, No. (%) | 68 (93.2) | |
| Craniotomy frontal/temporal, No. (%) | 51 (69.9) | |
| Length of surgery, min | 241 ± 89 | |
| Intraoperative drugs | ||
| Remifentanil 0.1 mcg·kg−1·min−1, No. (%) | 27 (37.0) | |
| Remifentanil 0.1 mcg·kg−1·min−1 + Fentanyl, No. (%) | 42 (57.5) | |
| Remifentanil 0.1 mcg·kg−1·min−1 + Tramadol, No. (%) | 4 (5.5) | |
| Not remifentanil, No. (%) | 19 (26.0) | |
| Dexamethasone 4 mg, No. (%) | 29 (39.7) | |
| Dexamethasone >4 mg, No. (%) | 25 (34.3) | |
| Postoperative drain (%) | 45 (61.6) | |
| Variable | STAI A/E < 20 (N = 29) | STAI A/E ≥ 20 (N = 44) | p-Value | |
|---|---|---|---|---|
| Age, years | 58 ± 15 | 54 ± 15 | 0.250 | |
| Gender | ||||
| Female, No. (%) | 16 (55.2) | 29 (65.9) | 0.462 | |
| Male, No. (%) | 13 (44.8) | 15 (34.1) | ||
| BMI, kg·m−1 | 24.6 ± 4.7 | 25.0 ± 6.1 | 0.767 | |
| Educational level | ||||
| Basic elementary, No. (%) | 20 (69.0) | 23 (52.3) | 0.224 | |
| Other No. (%) | 9 (31.0) | 21 (47.7) | ||
| MMSE, points | 29.0 ± 1.1 | 28.9 ± 1.5 | 0.886 | |
| Medicalhistory | ||||
| Depression, No. (%) | 5 (17.2) | 11 (25) | 0.567 | |
| Anxiety, No. (%) | 2 (6.9) | 3 (6.8) | 1.000 | |
| Rheumatological diseases, No. (%) | 2 (6.9) | 2 (4.5) | 0.66 | |
| Previous useof drugs | ||||
| Metamizole, No. (%) | 8 (27.6) | 19 (43.2) | 0.220 | |
| Corticosteroids, No. (%) | 6 (20.7) | 16 (36.4) | 0.197 | |
| Antidepressants, No. (%) | 6 (20.7) | 8 (18.2) | 1.000 | |
| Chronic use of analgesics, No. (%) | 7 (24.1) | 5 (11.4) | 0.200 | |
| Variable | STAI A/R < 20 (N = 10) | STAI A/R ≥ 20 (N = 63) | p-Value | |
|---|---|---|---|---|
| Age, years | 53 ± 18 | 56 ± 14 | 0.659 | |
| Gender | ||||
| Female, No. (%) | 5 (50) | 23 (36.5) | 0.492 | |
| Male, No. (%) | 5 (50) | 40 (63.5) | ||
| BMI, kg·m−1 | 25.7 ± 4.3 | 24.7 ± 5.7 | 0.480 | |
| Educational level | ||||
| Basic elementary education, No. (%) | 7 (70) | 36 (57.1) | 0.510 | |
| Other, No. (%) | 3 (30) | 27 (42.9) | ||
| MMSE, points | 29.1 ± 0.9 | 28.9 ± 1.4 | 0.885 | |
| Medicalhistory | ||||
| Depression, No. (%) | 1 (10) | 15 (23.8) | 0.443 | |
| Anxiety, No. (%) | 1 (10) | 4 (6.3) | 0.532 | |
| Rheumatological diseases, No. (%) | 1 (10) | 3 (4.8) | 0.499 | |
| Previous use of drugs | ||||
| Metamizole, No. (%) | 4 (40) | 23 (36.5) | 1.000 | |
| Corticosteroids, No. (%) | 1 (10) | 21 (33.3) | 0.264 | |
| Antidepressants, No. (%) | 2 (20) | 12 (19) | 1.000 | |
| Chronic use of analgesics, No. (%) | 2 (20) | 10 (15.9) | 0.665 | |
| NRS at 1 h | NRS at 8 h | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Univariate | p-Value | Multivariate | p-Value | Univariate | p-Value | Multivariate | p-Value |
| STAI A/E | 0.08 (0.04–0.11) | <0.001 | 0.06 (0.02–0.1) | 0.003 | 0.04 (0.01–0.08) | 0.024 | 0.04 (0–0.08) | 0.029 |
| STAI A/R | 0.05 (−0.01–0.11) | 0.09 | −0.01 (−0.07–0.05) | 0.76 | 0.04 00280.01–0.09) | 0.13 | 0.03 00280.06–0.06) | 0.968 |
| Age | –0.06 (−0.09–−0.03) | <0.001 | −0.07 (−0.1–−0.04) | <0.001 | −0.04 (−0.07–−0.02) | 0.001 | −0.05 (−0.08–−0.03) | <0.001 |
| Female gender | 0.07 (−0.88–1.02) | 0.88 | −0.7 (−1.55–0.15) | 0.11 | −0.19 (−1.01–0.63) | 0.648 | −0.72 (−1.5–0.06) | 0.068 |
| Depression | 0.23 (–0.89–1.34) | 0.69 | 0.93 (−0.05–1.9) | 0.06 | 0.8 (–0.15–1.75) | 0.097 | 1.48 (0.6–2.36) | 0.001 |
| ASA physical status 3–4 | 0.32 (−0.6–1.24) | 0.49 | 0.63 (−0.13–1.4) | 0.1 | - | - | - | - |
| MMSE | –0.03 (−0.38–0.32) | 0.87 | –0.25 (−0.56–0.06) | 0.11 | - | - | - | - |
| Parietal/occipital craniotomy | - | - | - | - | 0.04 (−0.83–0.92) | 0.924 | 0.76 (−0.02–1.54) | 0.056 |
| Length of surgery | - | - | - | - | 0 (−0.01–0) | 0.138 | −0.003 (−0.01–0) | 0.163 |
| NRS at 24 h | NRS at 48 h | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Univariate | p-Value | Multivariate | p-Value | Univariate | p-Value | Multivariate | p-Value |
| STAI A/E | 0.04 (0.01–0.07) | 0.018 | 0.04 (0–0.07) | 0.029 | 0.03 (0–0.05) | 0.053 | 0.02 (0–0.05) | 0.078 |
| STAI A/R | 0.04 (−0.01–0.08) | 0.083 | 0.02 (−0.03–0.07) | 0.502 | 0.04 (0–0.07) | 0.061 | 0.01 (−0.03–0.06) | 0.53 |
| Age | −0.04 (0.06–−0.02) | <0.001 | −0.04 (−0.06–−0.02) | <0.001 | −0.02 (−0.04–0) | 0.069 | −0.01 (−0.03–0) | 0.145 |
| Female gender | −0.11 (−0.81–0.6) | 0.762 | −0.48 (−1.17–0.22) | 0.17 | - | - | - | - |
| Depression | 0.11 (−0.72–0.93) | 0.796 | 0.61 (−0.17–1.39) | 0.12 | - | - | - | - |
| ASA physical status 3–4 | 0.35 (−0.33–1.03) | 0.306 | 0.44 (−0.17–1.06) | 0.153 | - | - | - | - |
| Parietal/occipital craniotomy | 0.01 (−0.74–0.75) | 0.987 | 0.54 (−0.15–1.24) | 0.123 | - | - | - | - |
| Length of surgery | 0 (−0.01–0) | 0.02 | −0.002 (−0.01–0) | 0.183 | 0 (−0.01–0) | 0.009 | −0.003 (−0.01–0) | 0.025 |
| Intraoperative dexamethasone 4 mg | - | - | - | - | −0.83 (−1.52–−0.14) | 0.019 | −0.76 (−1.42–−0.1) | 0.025 |
| Intraoperative dexamethasone >4 mg | - | - | - | - | −0.44 (−1.15–0.28) | 0.226 | −0.39 (−1.06–0.29) | 0.255 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valencia, L.; Becerra, Á.; Ojeda, N.; Domínguez, A.; Prados, M.; González-Martín, J.M.; Rodríguez-Pérez, A. Effect of Preoperative Anxiety on Postoperative Pain after Craniotomy. J. Clin. Med. 2022, 11, 556. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030556
Valencia L, Becerra Á, Ojeda N, Domínguez A, Prados M, González-Martín JM, Rodríguez-Pérez A. Effect of Preoperative Anxiety on Postoperative Pain after Craniotomy. Journal of Clinical Medicine. 2022; 11(3):556. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030556
Chicago/Turabian StyleValencia, Lucía, Ángel Becerra, Nazario Ojeda, Ancor Domínguez, Marcos Prados, Jesús María González-Martín, and Aurelio Rodríguez-Pérez. 2022. "Effect of Preoperative Anxiety on Postoperative Pain after Craniotomy" Journal of Clinical Medicine 11, no. 3: 556. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030556