
Multimodality Approach to Lymphedema Surgery Achieves and Maintains Normal Limb Volumes: A Treatment Algorithm to Optimize Outcomes


Abstract
:1. Introduction
2. Materials and Methods
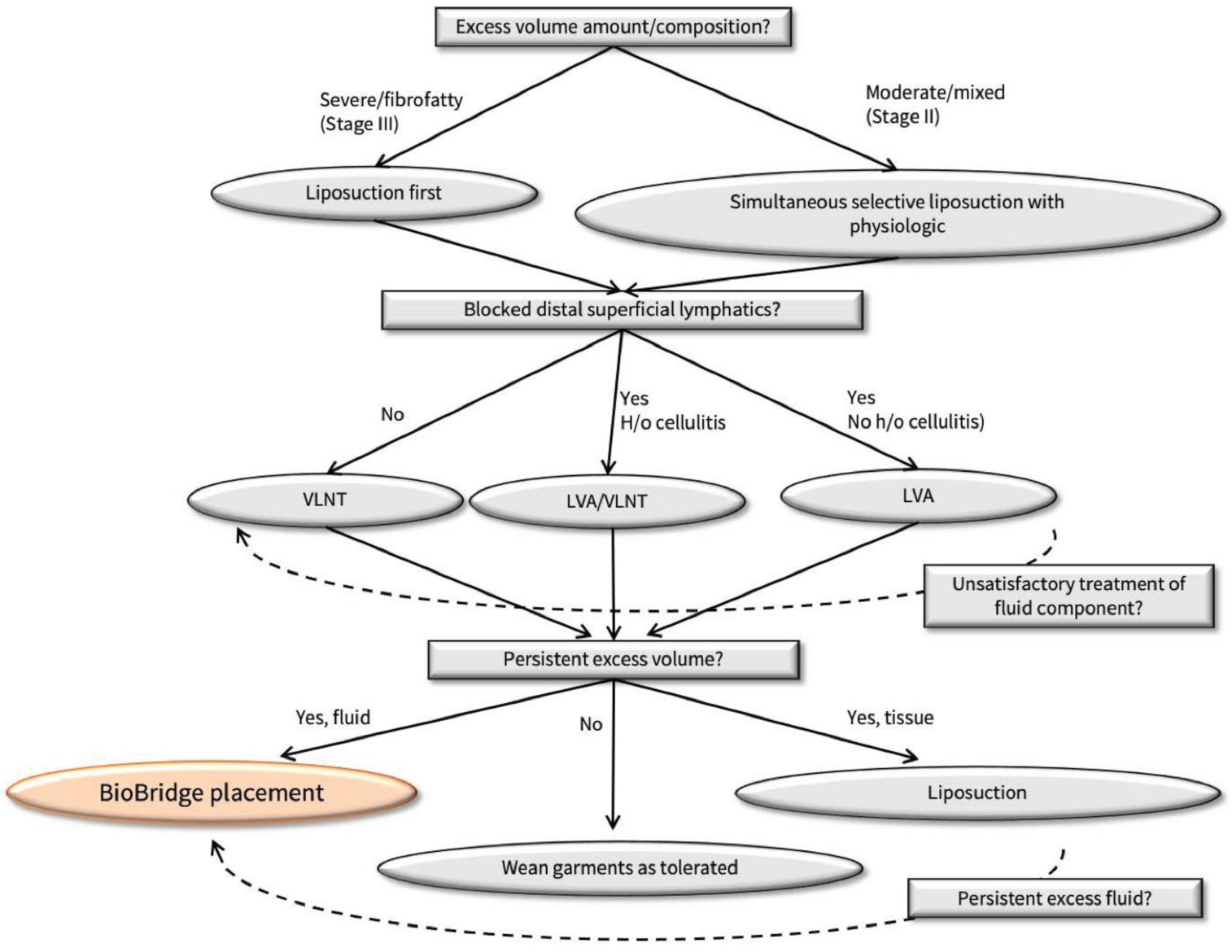
Treatment Protocol
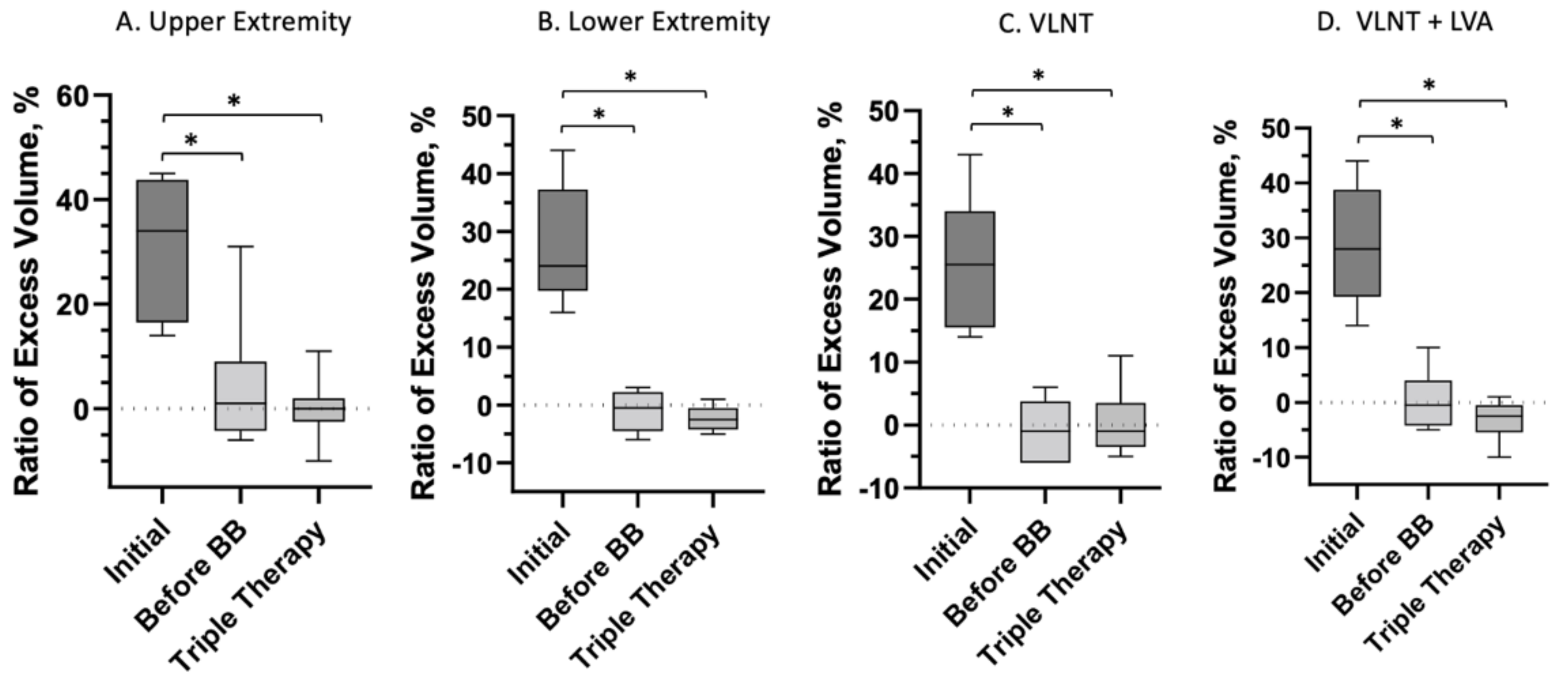
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Brazio, P.S.; Nguyen, D.H. Combined Liposuction and Physiologic Treatment Achieves Durable Limb Volume Normalization in Class II–III Lymphedema: A Treatment Algorithm to Optimize Outcomes. Ann. Plast. Surg. 2021, 86, S384–S389. [Google Scholar] [CrossRef]
- Schaverien, M.V.; Coroneos, C.J. Surgical treatment of lymphedema. Plast. Reconstr. Surg. 2019, 144, 738–758. [Google Scholar] [CrossRef]
- Nguyen, D.H.; Zhou, A.; Posternak, V.; Rochlin, D.H. Nanofibrillar Collagen Scaffold Enhances Edema Reduction and Formation of New Lymphatic Collectors after Lymphedema Surgery. Plast. Reconstr. Surg. Publish Ahead of Print. 2021. [Google Scholar] [CrossRef]
- Rochlin, D.; Inchauste, S.; Zelones, J.; Nguyen, D.H. The role of adjunct nanofibrillar collagen scaffold implantation in the surgical management of secondary lymphedema: Review of the literature and summary of initial pilot studies. J. Surg. Oncol. 2020, 121, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, D.; Zaitseva, T.S.; Zhou, A.; Rochlin, D.; Sue, G.; Deptula, P.; Tabada, P.; Wan, D.; Loening, A.; Paukshto, M.; et al. Lymphatic regeneration after implantation of aligned nanofibrillar collagen scaffolds: Preliminary preclinical and clinical results. J. Surg. Oncol. 2021, 125, 113–122. [Google Scholar] [CrossRef]
- Sitzia, J. Volume measurement in lymphoedema treatment: Examination of formulae. Eur. J. Cancer Care 1995, 4, 11–16. [Google Scholar] [CrossRef]
- Hadamitzky, C.; Zaitseva, T.S.; Bazalova Carter, M.; Paukshto, M.V.; Hou, L.; Strassberg, Z.; Ferguson, J.; Matsuura, Y.; Dash, R.; Yang, P.C.; et al. Aligned nanofibrillar collagen scaffolds—Guiding lymphangiogenesis for treatment of acquired lymphedema. Biomaterials 2016, 102, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Karges, J.R.; Mark, B.E.; Stikeleather, S.J.; Worrell, T.W. Concurrent validity of upper-extremity volume estimates: Comparison of calculated volume derived from girth measure- ments and water displacement volume. Phys. Ther. 2003, 83, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Brorson, H.; Höijer, P. Standardised measurements used to order compression gar- ments can be used to calculate arm volumes to evaluate lymphoedema treatment. J. Plast. Surg. Hand Surg. 2012, 46, 410–415. [Google Scholar] [CrossRef] [Green Version]
- Szuba, A.; Rockson, S.G. Lymphedema: Classification, diagnosis and therapy. Vasc. Med. 1998, 3, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Szuba, A.; Cooke, J.P.; Yousuf, S.; Rockson, S.G. Decongestive lymphatic therapy for patients with cancer related or primary lymphedema. Am. J. Med. 2000, 109, 296–300. [Google Scholar] [CrossRef]
- Casley Smith, J.R.; Casley Smith, J.R. Modern treatment of lymphoedema. I. Complex physical therapy: The first 200 Australian limbs. Australas. J. Dermatol. 1992, 33, 61–68. [Google Scholar] [CrossRef] [PubMed]
- McNeely, M.L.; Magee, D.J.; Lees, A.W.; Bagnall, K.M.; Haykowsky, M.; Hanson, J. The addition of manual lymph drainage to compression therapy for breast cancer related lymphedema: A randomized controlled trial. Breast Cancer Res. Treat. 2004, 86, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Rockson, S.G. Current concepts and future directions in the diagnosis and management of lymphatic vascular disease. Vasc. Med. 2010, 15, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Brorson, H.; Svensson, H. Complete reduction of lymphoedema of the arm by lipo- suction after breast cancer. Scand. J. Plast. Reconstr. Surg. Hand Surg. 1997, 31, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Frick, A.; Hoffmann, J.N.; Baumeister, R.G.; Putz, R. Liposuctiontechnique and lymphatic lesions in lower legs: Anatomic study to reduce risks. Plast. Reconstr. Surg. 1999, 103, 1868–1873. [Google Scholar] [CrossRef]
- Hoffmann, J.N.; Fertmann, J.P.; Baumeister, R.G.; Putz, R.; Frick, A. Tumescent and dry liposuc- tion of lower extremities: Differences in lymph vessel injury. Plast. Reconstr. Surg. 2004, 113, 718–724, 725–726. [Google Scholar] [CrossRef]
- Campisi, C.C.; Ryan, M.; Boccardo, F.; Campisi, C. Fibro-lipo-lymph-aspiration with a lymph vessel sparing procedure to treat advanced lymphedema after multiple lymphatic-venous anastomoses: The complete treatment protocol. Ann. Plast. Surg. 2017, 78, 184–190. [Google Scholar] [CrossRef]
- Liu, N.F.; Lu, Q.; Jiang, Z.H.; Wang, C.G.; Zhou, J.G. Anatomic and functional evaluation of the lym- phatics and lymph nodes in diagnosis of lymphatic circulation disorders with con- trast magnetic resonance lymphangiography. J. Vasc. Surg. 2009, 49, 980–987. [Google Scholar] [CrossRef] [Green Version]
- O'Brien, B.; Khazanchi, R.K.; Kumar, P.V.; Dvir, E.; Pederson, W. Liposuction in the treatment of lymphoedema; a preliminary report. Br. J. Plast. Surg. 1989, 42, 530–533. [Google Scholar] [CrossRef]
- Hoffner, M.; Ohlin, K.; Svensson, B.; Manjer, J.; Hansson, E.; Troëng, T.; Brorson, H. Liposuction gives complete reduction of arm lymphedema following breast cancer treatment—A 5-year prospective study in 105 patients without recurrence. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1912. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC6181505/ (accessed on 7 April 2020). [CrossRef] [PubMed]
- Brorson, H. Liposuction normalizes lymphedema induced adipose tissue hypertro- phy in elephantiasis of the leg—A prospective study with a ten-year follow-up. Plast. Reconstr. Surg. 2015, 136, 133–134. [Google Scholar] [CrossRef] [Green Version]
- Brorson, H.; Svensson, H.; Norrgren, K.; Thorsson, O. Liposuctionreducesarmlymphedema without significantly altering the already impaired lymph transport. Lymphology 1998, 31, 156–172. [Google Scholar] [PubMed]
- Becker, C.; Assouad, J.; Riquet, M.; Hidden, G. Postmastectomy lymphedema: Long-term re- sults following microsurgical lymph node transplantation. Ann. Surg. 2006, 243, 313–315. [Google Scholar] [CrossRef]
- Nicoli, F.; Constantinides, J.; Ciudad, P.; Sapountzis, S.; Kiranantawat, K.; Lazzeri, D.; Lim, S.Y.; Nicoli, M.; Chen, P.-Y.; Yeo, M.S.-W.; et al. Free lymph node flap transfer and laser-assisted liposuction: A combined technique for the treatment of moderate up- per limb lymphedema. Lasers Med. Sci. 2015, 30, 1377–1385. [Google Scholar] [CrossRef]
- Agko, M.; Ciudad, P.; Chen, H.-C. Staged surgical treatment of extremity lymph- edema with dual gastroepiploic vascularized lymph node transfers followed by suction-assisted lipectomy—A prospective study. J. Surg. Oncol. 2018, 117, 1148–1156. [Google Scholar] [CrossRef]
- Di Taranto, G.; Bolletta, A.; Chen, S.H. A prospective study on combined lymphedema surgery: Gastroepiploic vascularized lymph nodes transfer and lymphaticovenous anastomosis followed by suction lipectomy. Microsurgery 2021, 41, 34–43. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Details | |
|---|---|
| Number of patients | 14 |
| Average Age | 62 ± 12.1 years |
| Lymphedema Stage | |
| Late stage 2 | 11 |
| Stage 3 | 3 |
| Extremity affected | |
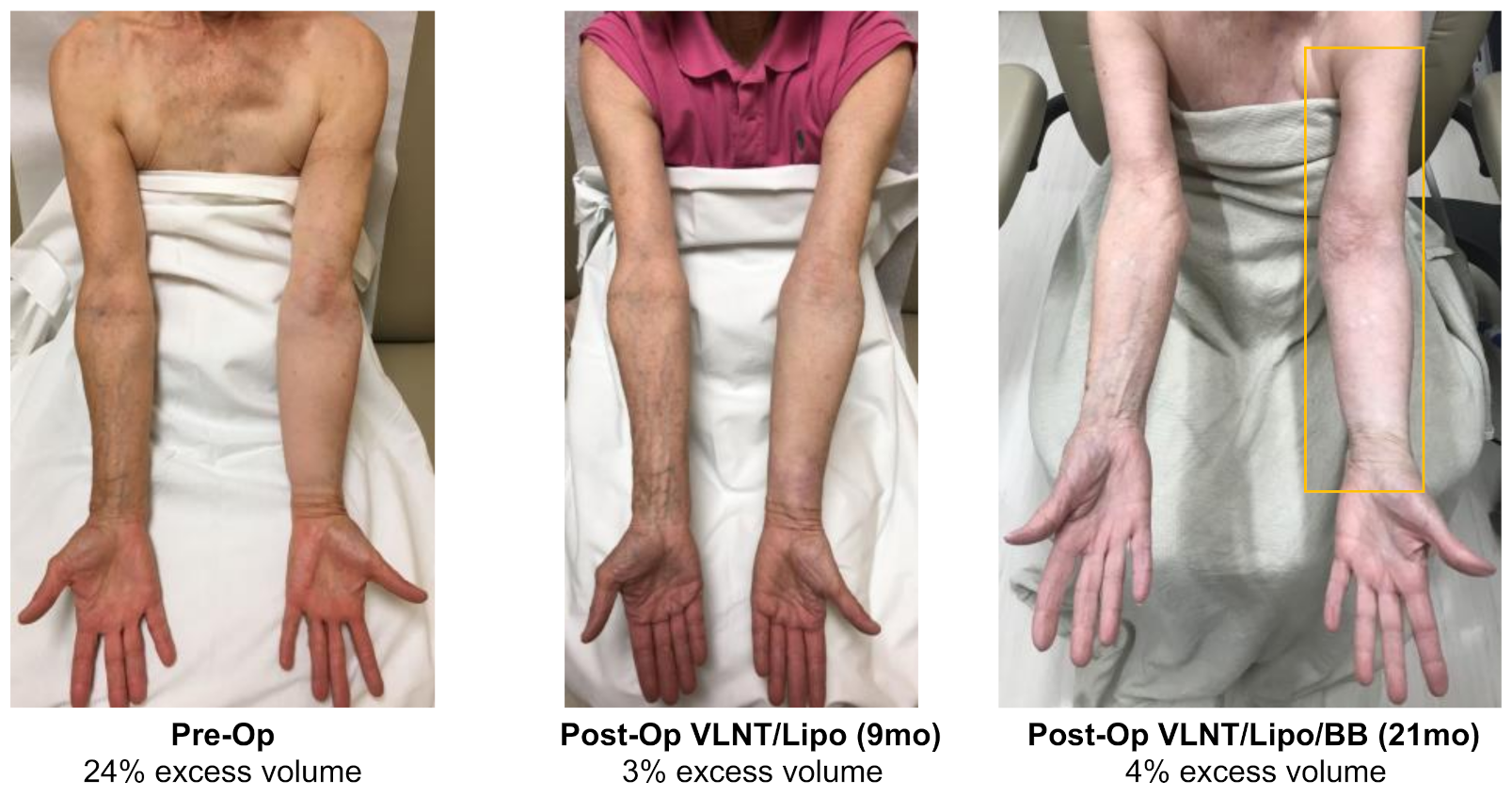
| Upper extremity | 8 |
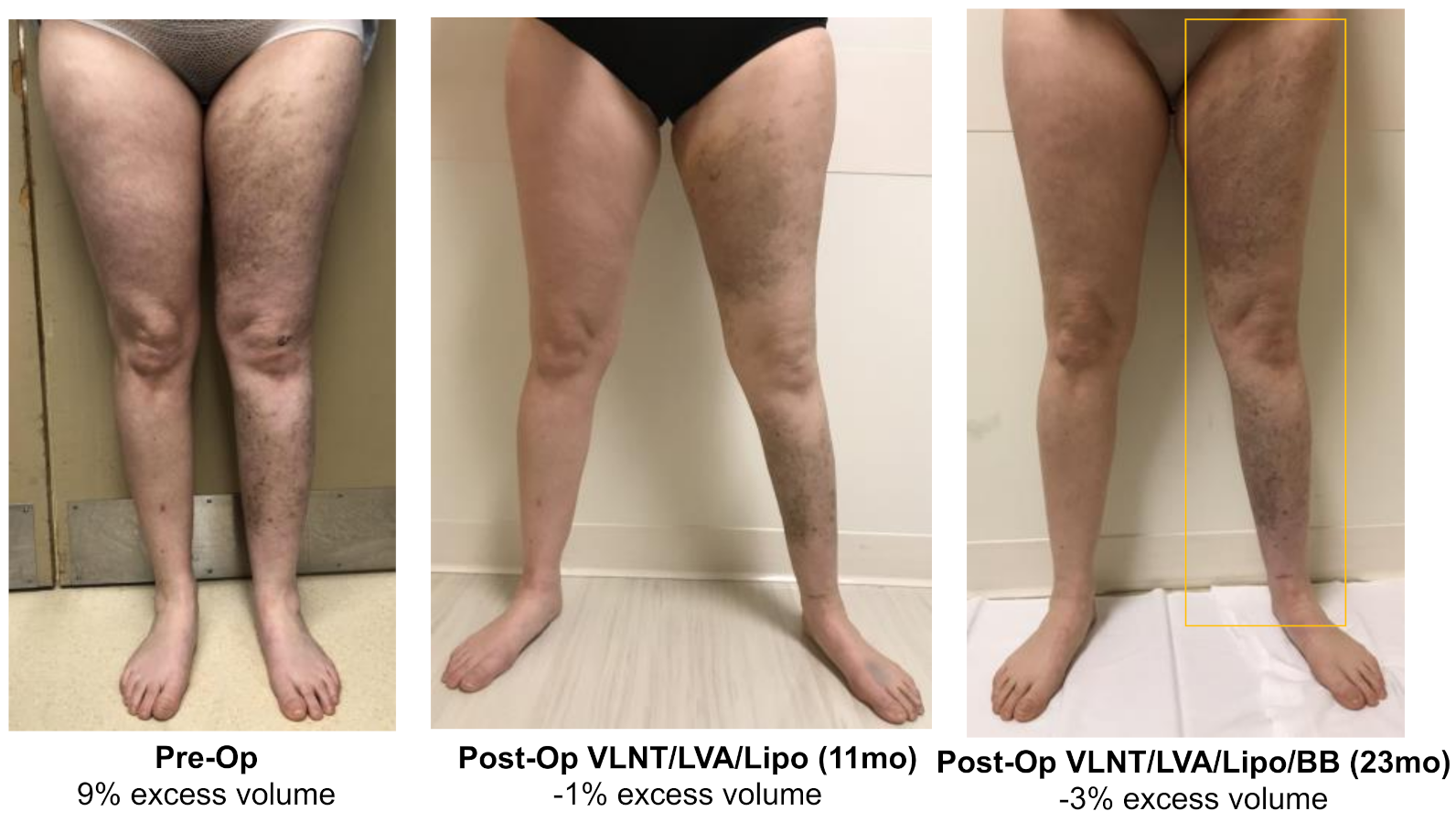
| Lower extremity | 6 |
| Treatment Summary | |
|---|---|
| Order of Treatment | |
| Large volume liposuction, then physiologic (VLNT/LVA), then BioBridge placement | N = 3 |
| Simultaneous liposuction with physiologic (VLNT/LVA), then BB | N = 11 |
| Liposuction average volume | |
| Upper extremity | 500 ± 168 cc |
| Lower extremity | 1983 ± 1748 cc |
| Physiologic surgeries performed | |
| VLNT + LVA VLNT | N = 6 N = 6 |
| LVA (1-3 LVAs performed) | N = 2 |
| Limb Volume Excess | ||||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Post Lipo & Physiologic | Post BB Placement | ||||||
| % | cc | % | cc | p | % | cc | p | |
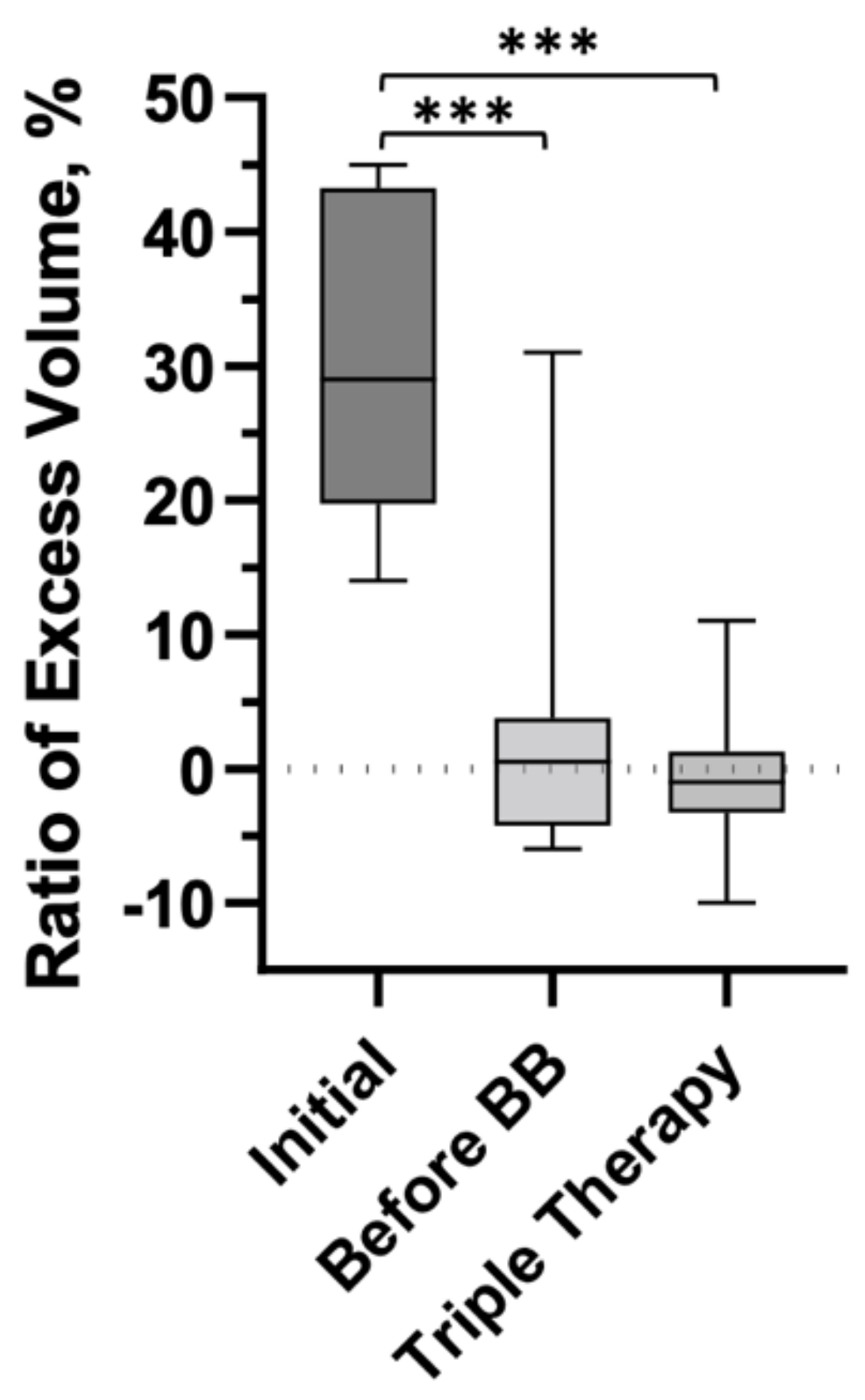
| Total | 29 (14, 43) | 1086 (585, 1554) | 0.5 (−4.3, 3.8) | 26 (−187, 130) | 0.0001 | −1 (−3.3, 1.3) | −36 (−216, 30) | 0.0001 |
| UE | 34 (17, 44) | 629 (406, 1010) | 1.0 (−4.3, 9.0) | 26 (−111, 126) | 0.0078 | 0.0 (−2.5, 2.0) | −5 (−38, 47) | 0.0078 |
| LE | 24 (20, 37) | 1696 (1128, 3029) | −0.5 (−4.5, 2.3) | −57 (−343, 156) | 0.0313 | −2.5 (−4.3, −0.5) | −209 (−346, −57) | 0.0313 |
| VLNT | 26 (16, 34) | 870 (339, 1218) | −1.0 (−6.0, 3.8) | −31 (−257, 139) | 0.0156 | −1.0 (−3.5, 3.5) | −24 (−117, 122) | 0.0313 |
| VLNT + LVA | 28 (19, 39) | 1487 (574, 3029) | −0.5 (−4.3, 4.0) | −57 (−212, 132) | 0.0313 | −2.5 (−5.5, −0.5) | −209 (−353, −74) | 0.0313 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deptula, P.; Zhou, A.; Posternak, V.; He, H.; Nguyen, D. Multimodality Approach to Lymphedema Surgery Achieves and Maintains Normal Limb Volumes: A Treatment Algorithm to Optimize Outcomes. J. Clin. Med. 2022, 11, 598. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030598
Deptula P, Zhou A, Posternak V, He H, Nguyen D. Multimodality Approach to Lymphedema Surgery Achieves and Maintains Normal Limb Volumes: A Treatment Algorithm to Optimize Outcomes. Journal of Clinical Medicine. 2022; 11(3):598. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030598
Chicago/Turabian StyleDeptula, Peter, Anna Zhou, Victoria Posternak, Hui He, and Dung Nguyen. 2022. "Multimodality Approach to Lymphedema Surgery Achieves and Maintains Normal Limb Volumes: A Treatment Algorithm to Optimize Outcomes" Journal of Clinical Medicine 11, no. 3: 598. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030598