
Healing of Vertebral Compression Fractures in the Elderly after Percutaneous Vertebroplasty—An Analysis of New Bone Formation and Sagittal Alignment in a 3-Year Follow-Up

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement of Vertebral Parameters and New Bone Formation
2.3. Statistical Analysis
3. Results
Comparison with Conservatively Managed Group
4. Discussion
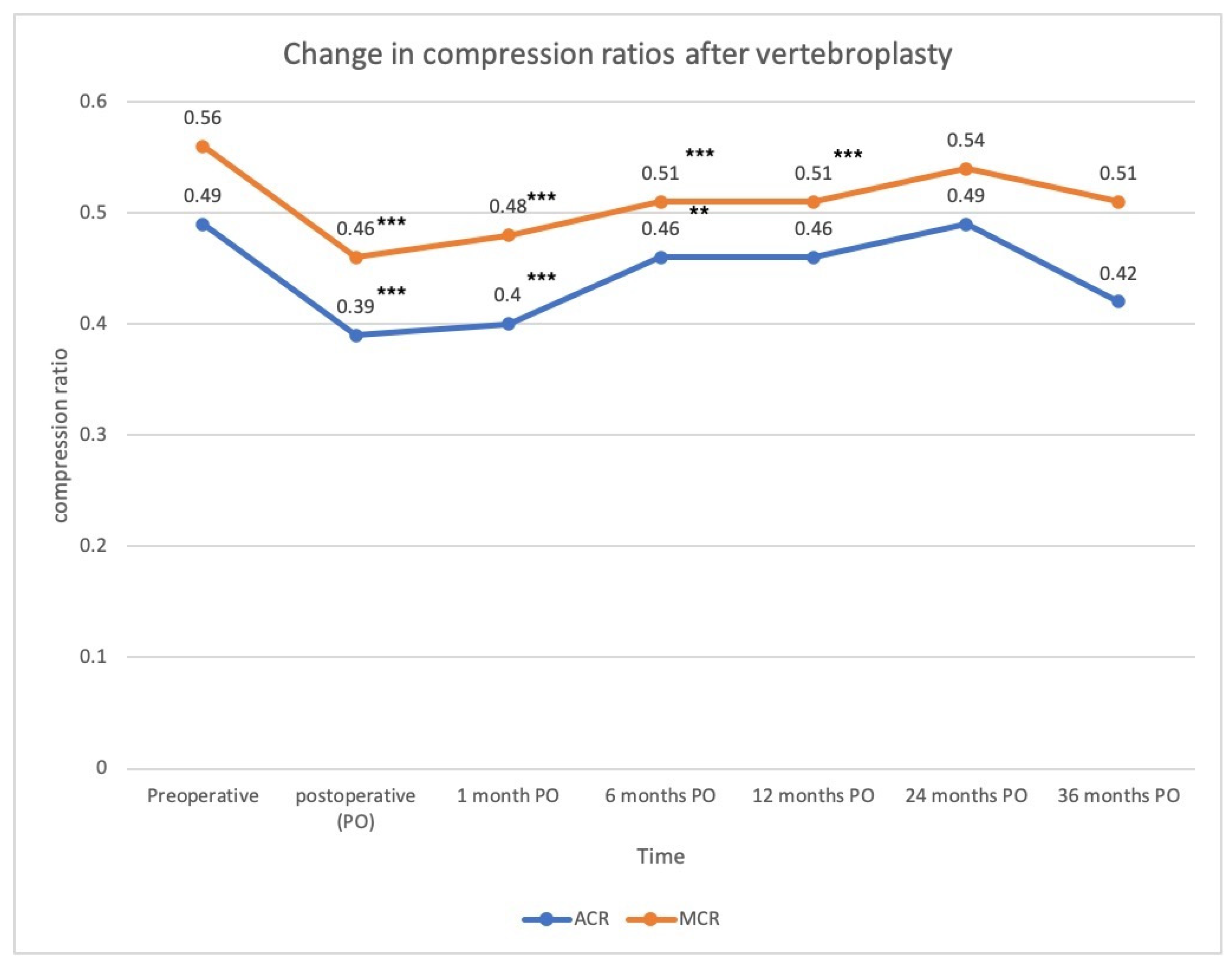
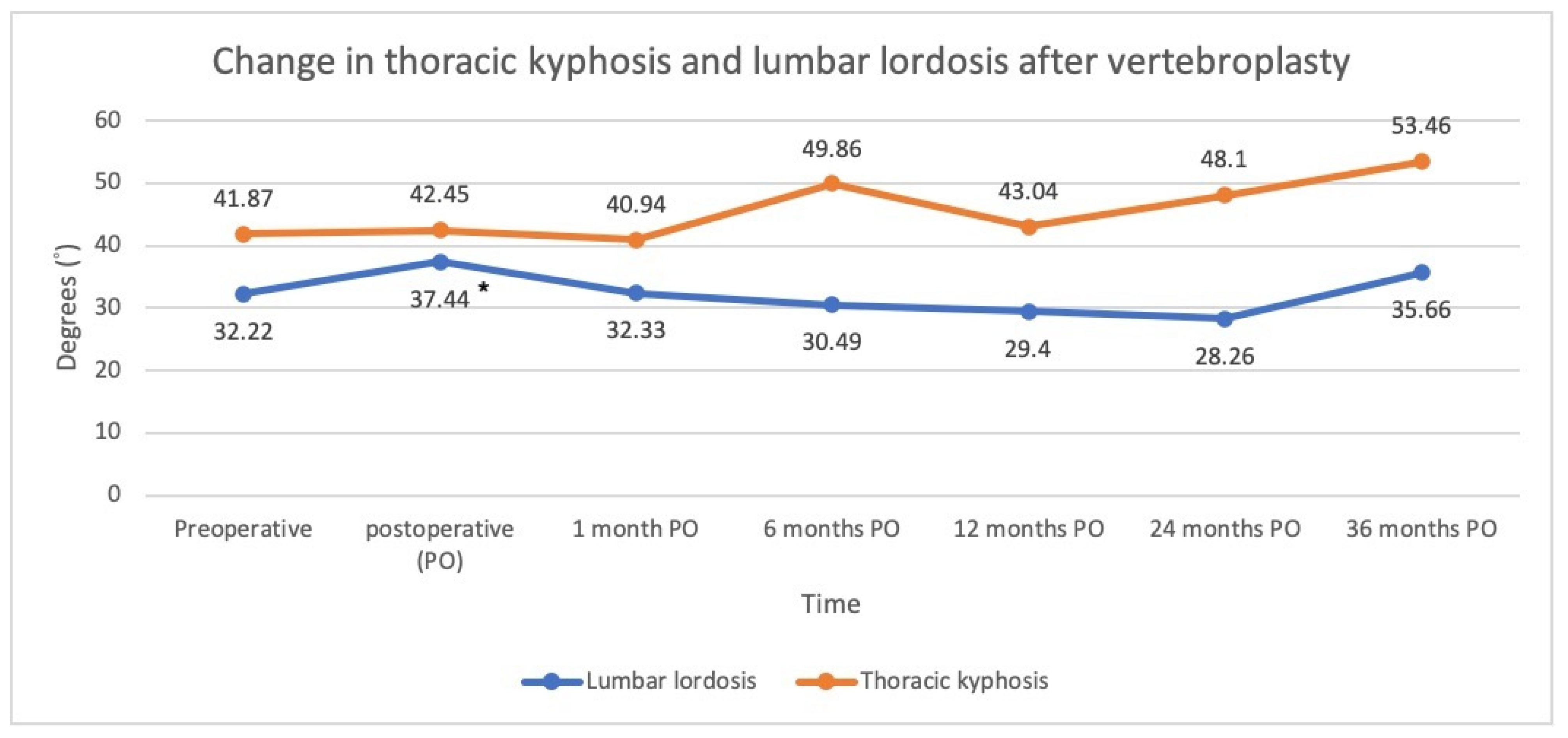
4.1. Trend in the Radiographic Parameters
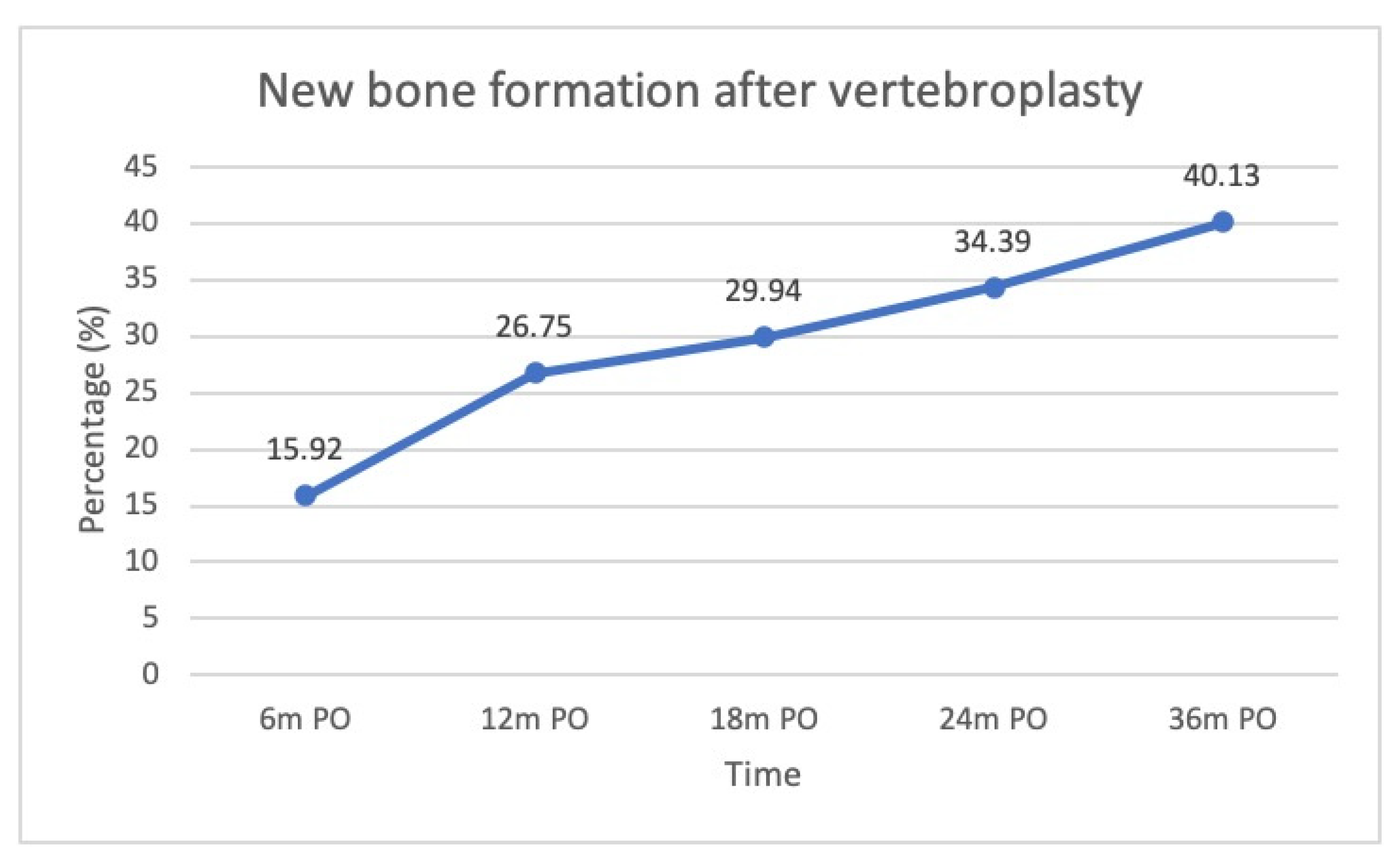
4.2. New Bone Formation
4.3. Comparison between Groups with and without New Bone Formation
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Kim, D.H.; Vaccaro, A.R. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006, 6, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Van der Klift, M.; De Laet, C.E.; McCloskey, E.V.; Hofman, A.; Pols, H.A. The incidence of vertebral fractures in men and women: The Rotterdam Study. J. Bone Miner. Res. 2002, 17, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Lou, S.; Shi, X.; Zhang, X.; Lyu, H.; Li, Z.; Wang, Y. Percutaneous vertebroplasty versus non-operative treatment for osteoporotic vertebral compression fractures: A meta-analysis of randomized controlled trials. Osteoporos. Int. 2019, 30, 2369–2380. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.H.; Hsu, H.C.; Lai, K.L. Vertebroplasty and balloon kyphoplasty versus conservative treatment for osteoporotic vertebral compression fractures: A meta-analysis. Medicine 2016, 95, e4491. [Google Scholar] [CrossRef]
- Zhang, H.; Xu, C.; Zhang, T.; Gao, Z.; Zhang, T. Does Percutaneous Vertebroplasty or Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures Increase the Incidence of New Vertebral Fractures? A Meta-Analysis. Pain Physician 2017, 20, E13–E28. [Google Scholar] [CrossRef]
- Buchbinder, R.; Golmohammadi, K.; Johnston, R.V.; Owen, R.J.; Homik, J.; Jones, A.; Dhillon, S.S.; Kallmes, D.F.; Lambert, R.G.W. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database Syst. Rev. 2015, CD006349. [Google Scholar] [CrossRef]
- Boszczyk, B. Percutaneous vertebroplasty does not reduce pain and disability from osteoporotic vertebral compression fracture. Evid.-Based Med. 2015, 20, 181. [Google Scholar] [CrossRef] [Green Version]
- Andrei, D.; Popa, I.; Brad, S.; Iancu, A.; Oprea, M.; Vasilian, C.; Poenaru, D.V. The variability of vertebral body volume and pain associated with osteoporotic vertebral fractures: Conservative treatment versus percutaneous transpedicular vertebroplasty. Int. Orthop. 2017, 41, 963–968. [Google Scholar] [CrossRef]
- Mattie, R.; Laimi, K.; Yu, S.; Saltychev, M. Comparing Percutaneous Vertebroplasty and Conservative Therapy for Treating Osteoporotic Compression Fractures in the Thoracic and Lumbar Spine: A Systematic Review and Meta-Analysis. J. Bone Jt. Surg. Am. 2016, 98, 1041–1051. [Google Scholar] [CrossRef]
- Yang, E.Z.; Xu, J.G.; Huang, G.Z.; Xiao, W.Z.; Liu, X.K.; Zeng, B.F.; Lian, X.F. Percutaneous Vertebroplasty Versus Conservative Treatment in Aged Patients With Acute Osteoporotic Vertebral Compression Fractures: A Prospective Randomized Controlled Clinical Study. Spine 2016, 41, 653–660. [Google Scholar] [CrossRef]
- Yi, H.J.; Jeong, J.H.; Im, S.B.; Lee, J.K. Percutaneous Vertebroplasty versus Conservative Treatment for One Level Thoracolumbar Osteoporotic Compression Fracture: Results of an Over 2-Year Follow-up. Pain Physician 2016, 19, E743–E750. [Google Scholar] [PubMed]
- Kawaguchi, S.; Horigome, K.; Yajima, H.; Oda, T.; Kii, Y.; Yoshimoto, M.; Takebayashi, T.; Yamashita, T. Conversion to hypertrophic vertebral pseudarthrosis following percutaneous vertebroplasty. Eur. Spine J. 2010, 19, 901–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunstein, V.; Sprecher, C.M.; Gisep, A.; Benneker, L.; Yen, K.; Schneider, E.; Heini, P.; Milz, S. Long-term reaction to bone cement in osteoporotic bone: New bone formation in vertebral bodies after vertebroplasty. J. Anat. 2008, 212, 697–701. [Google Scholar] [CrossRef]
- Denaro, L.; Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Piergentili, I.; Denaro, V. The burden of percutaneous vertebroplasty: An epidemiological nationwide study in Italy from 2009 to 2015. Eur. Spine J. 2021, 30, 3099–3106. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Alshahrani, M.; Chapurlat, R.; Chevalley, T.; Dennison, E.; Camargos, B.M.; Papaioannou, A.; Silverman, S.; Kaux, J.-F.; Lane, N.E.; et al. The global approach to rehabilitation following an osteoporotic fragility fracture: A review of the rehabilitation working group of the International Osteoporosis Foundation (IOF) committee of scientific advisors. Osteoporos. Int. 2022, 1–14. [Google Scholar] [CrossRef]
- Chen, C.; Li, D.; Wang, Z.; Li, T.; Liu, X.; Zhong, J. Safety and Efficacy Studies of Vertebroplasty, Kyphoplasty, and Mesh-Container-Plasty for the Treatment of Vertebral Compression Fractures: Preliminary Report. PLoS ONE 2016, 11, e0151492. [Google Scholar] [CrossRef] [Green Version]
- Garnier, L.; Tonetti, J.; Bodin, A.; Vouaillat, H.; Merloz, P.; Assaker, R.; Court, C. Kyphoplasty versus vertebroplasty in osteoporotic thoracolumbar spine fractures. Short-term retrospective review of a multicentre cohort of 127 consecutive patients. Orthop. Traumatol. Surg. Res. 2012, 98, S112–S119. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Yoo, S.H.; Kim, J.H. Long-term Follow-up of Percutaneous Vertebroplasty in Osteoporotic Compression Fracture: Minimum of 5 Years Follow-up. Asian Spine J. 2012, 6, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Movrin, I.; Vengust, R.; Komadina, R. Adjacent vertebral fractures after percutaneous vertebral augmentation of osteoporotic vertebral compression fracture: A comparison of balloon kyphoplasty and vertebroplasty. Arch. Orthop. Trauma. Surg. 2010, 130, 1157–1166. [Google Scholar] [CrossRef]
- Schofer, M.D.; Efe, T.; Timmesfeld, N.; Kortmann, H.-R.; Quante, M. Comparison of kyphoplasty and vertebroplasty in the treatment of fresh vertebral compression fractures. Arch. Orthop. Trauma. Surg. 2009, 129, 1391–1399. [Google Scholar] [CrossRef]
- Ee, G.W.; Lei, J.; Guo, C.M.; Yeo, W.; Tan, S.B.; Tow, P.B.; Chen, L.T.; Yue, W.M. Comparison of Clinical Outcomes and Radiographic Measurements in 4 Different Treatment Modalities for Osteoporotic Compression Fractures: Retrospective Analysis. J. Spinal Disord. Tech. 2015, 28, E328–E335. [Google Scholar] [CrossRef] [PubMed]
- Griffoni, C.; Lukassen, J.N.M.; Babbi, L.; Girolami, M.; Lamartina, C.; Cecchinato, R.; Gasbarrini, A.; Brodano, G.B. Percutaneous vertebroplasty and balloon kyphoplasty in the treatment of osteoporotic vertebral fractures: A prospective randomized comparison. Eur. Spine J. 2020, 29, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.T.; Liao, W.J.; Tan, W.C.; Lee, J.K.; Liu, C.H.; Chen, Y.H.; Lin, T.B. Balloon kyphoplasty versus vertebroplasty for treatment of osteoporotic vertebral compression fracture: A prospective, comparative, and randomized clinical study. Osteoporos. Int. 2009, 21, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Martikos, K.; Greggi, T.; Faldini, C.; Vommaro, F.; Scarale, A. Osteoporotic thoracolumbar compression fractures: Long-term retrospective comparison between vertebroplasty and conservative treatment. Eur. Spine J. 2018, 27, 244–247. [Google Scholar] [CrossRef]
- Teng, M.M.H.; Wei, C.-J.; Wei, L.-C.; Luo, C.-B.; Lirng, J.-F.; Chang, F.-C.; Liu, C.-L.; Chang, C.-Y. Kyphosis Correction and Height Restoration Effects of Percutaneous Vertebroplasty. Am. J. Neuroradiol. 2003, 24, 1893–1900. [Google Scholar]
- Chang, J.Z.; Bei, M.J.; Shu, D.P.; Sun, C.J.; Chen, J.B.; Xiao, Y.P. Comparison of the clinical outcomes of percutaneous vertebroplasty vs. kyphoplasty for the treatment of osteoporotic Kummell’s disease:a prospective cohort study. BMC Musculoskelet. Disord. 2020, 21, 238. [Google Scholar] [CrossRef] [Green Version]
- Yan, D.; Duan, L.; Li, J.; Soo, C.; Zhu, H.; Zhang, Z. Comparative study of percutaneous vertebroplasty and kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Arch. Orthop. Trauma. Surg. 2010, 131, 645–650. [Google Scholar] [CrossRef]
- Cao, Z.; Wang, G.; Hui, W.; Liu, B.; Liu, Z.; Sun, J. Percutaneous kyphoplasty for osteoporotic vertebral compression fractures improves spino-pelvic alignment and global sagittal balance maximally in the thoracolumbar region. PLoS ONE 2020, 15, e0228341. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, K.; Kawanishi, M.; Yamada, M.; Tanaka, H.; Ito, Y.; Kawabata, S.; Kuroiwa, T. Postoperative change in sagittal balance after Kyphoplasty for the treatment of osteoporotic vertebral compression fracture. Eur. Spine J. 2014, 24, 744–749. [Google Scholar] [CrossRef]
- Ailon, T.; Shaffrey, C.I.; Lenke, L.G.; Harrop, J.S.; Smith, J.S. Progressive Spinal Kyphosis in the Aging Population. Neurosurgery 2015, 77, S164–S172. [Google Scholar] [CrossRef]
- Park, S.-M.; Park, J.-W.; Kim, H.; Kim, H.-J.; Yeom, J.S.; Lee, C.-K.; Chang, B.-S. Morphological changes of vertebral compression fracture with intra-vertebral cleft treated with percutaneous vertebroplasty. J. Orthop. Sci. 2017, 23, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Xiao, X.; Zhang, J.; Li, Z.; Wang, X.; Tang, F.; Jiang, X.; Zhong, Y. Cement Distribution Patterns in Osteoporotic Vertebral Compression Fractures with Intravertebral Cleft: Effect on Therapeutic Efficacy. World Neurosurg. 2018, 123, e408–e415. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q1–Q3 | |||
|---|---|---|---|
| Gender | Male | 38 (24.2) | |
| Female | 119 (75.8) | ||
| Age | 75.2 (7.95) | 71, 76, 81 | |
| T-score | −2.76 (1.08) | −3.6, −2.9, −1.9 | |
| Vacuum sign | + | 115 (73.2) | |
| − | 42 (26.8) | ||
| Amount of cement (mL) | 3.72 (1.94) | 2.5, 3.3, 4.9 |
| Variables | Month | Callus (+) | Callus (−) | p-Value | Adj. p |
|---|---|---|---|---|---|
| Age | 6 | 79 | 75 | 0.31 | 0.62 |
| 12 | 79 | 75 | 0.07 | 0.28 | |
| 24 | 78.5 | 75 | 0.17 | 0.51 | |
| 36 | 77 | 76 | 0.76 | 0.76 | |
| T-score | 6 | −2.75 | −2.80 | 0.69 | 0.84 |
| 12 | −2.90 | −2.60 | 0.14 | 0.56 | |
| 24 | −2.90 | −2.60 | 0.23 | 0.69 | |
| 36 | −2.90 | −2.60 | 0.42 | 0.84 | |
| Vacuum (−) Vacuum (+) | 6 | 4 (13%) | 27 (87%) | 0.16 | 0.48 |
| 6 | 21 (28%) | 54 (72%) | |||
| 12 | 9 (29%) | 22 (71%) | 0.22 | 0.48 | |
| 12 | 33 (44%) | 42 (56%) | |||
| 24 | 11 (35%) | 20 (65%) | 0.07 | 0.28 | |
| 24 | 43 (57%) | 32 (43%) | |||
| 36 | 16 (52%) | 15 (48%) | 0.40 | 0.48 | |
| 36 | 47 (63%) | 28 (37%) | |||
| Amount of Cement | 6 | 4.15 | 3.20 | 0.01 | 0.04 * |
| 12 | 4.00 | 3.20 | 0.04 | 0.12 | |
| 24 | 3.75 | 3.30 | 0.22 | 0.44 | |
| 36 | 3.50 | 3.40 | 0.45 | 0.45 | |
| Wedge angle | 6 | 15.56 | 16.17 | 0.66 | >0.99 |
| 12 | 15.41 | 16.49 | 0.69 | >0.99 | |
| 24 | 15.87 | 16.12 | 0.67 | >0.99 | |
| 36 | 14.55 | 16.66 | 0.99 | >0.99 | |
| Anterior compression ratio | 6 | 0.47 | 0.49 | 0.57 | >0.99 |
| 12 | 0.47 | 0.49 | 0.94 | >0.99 | |
| 24 | 0.47 | 0.50 | 0.97 | >0.99 | |
| 36 | 0.46 | 0.51 | 0.52 | >0.99 | |
| Middle compression ratio | 6 | 0.58 | 0.54 | 0.28 | >0.99 |
| 12 | 0.56 | 0.54 | 0.43 | >0.99 | |
| 24 | 0.55 | 0.53 | 0.55 | >0.99 | |
| 36 | 0.54 | 0.54 | 0.81 | >0.99 | |
| Thoracic kyphotic angle | 6 | 48.54 | 39.50 | 0.84 | >0.99 |
| 12 | 38.82 | 40.18 | 0.77 | >0.99 | |
| 24 | 37.57 | 44.88 | 0.46 | >0.99 | |
| 36 | 37.69 | 44.88 | 0.76 | >0.99 | |
| Lumbar lordotic angle | 6 | 31.09 | 36.59 | 0.96 | >0.99 |
| 12 | 31.83 | 37.79 | 0.56 | >0.99 | |
| 24 | 30.35 | 38.93 | 0.22 | 0.66 | |
| 36 | 30.34 | 39.77 | 0.16 | 0.64 | |
| Wedge angle correction | 6 | −7.38 | −3.76 | 0.01 | 0.04 * |
| 12 | −7.04 | −3.52 | 0.03 | 0.09 | |
| 24 | −6.63 | −3.4 | 0.03 | 0.09 | |
| 36 | −6.15 | −3.89 | 0.26 | 0.26 | |
| ACR correction | 6 | −0.19 | −0.09 | 0.07 | 0.14 |
| 12 | −0.17 | −0.07 | 0.02 | 0.06 | |
| 24 | −0.18 | −0.06 | 0.01 | 0.04 * | |
| 36 | −0.14 | −0.07 | 0.09 | 0.14 | |
| MCR correction | 6 | −0.15 | −0.08 | 0.18 | 0.54 |
| 12 | −0.13 | −0.07 | 0.12 | 0.48 | |
| 24 | −0.12 | −0.07 | 0.24 | 0.54 | |
| 36 | −0.11 | −0.06 | 0.28 | 0.54 |
| Univariate Analysis | ||
|---|---|---|
| Variables | OR (95%) | p-Value |
| Age | 1.03 (0.98, 1.07) | 0.241 |
| T-score | 0.88 (0.65, 1.2) | 0.430 |
| Amount of cement | 1.19 (1, 1.42) | 0.052 |
| Vacuum | 1.82 (0.92, 3.61) | 0.084 |
| Pre-op wedge angle | 1.01 (0.97, 1.05) | 0.699 |
| Pre-op ACR | 1.13 (0.27, 4.74) | 0.864 |
| Pre-op MCR | 2.67 (0.37, 19.36) | 0.331 |
| Pre-op thoracic kyphosis | 1 (0.97, 1.04) | 0.893 |
| Pre-op lumbar lordosis | 0.98 (0.96, 1.01) | 0.249 |
| Wedge angle correction | 1.05 (0.99, 1.11) | 0.105 |
| ACR correction | 10.7 (0.87, 131.46) | 0.064 |
| MCR correction | 4.8 (0.27, 84.14) | 0.283 |
| Thoracic kyphosis correction | 1.2 (0.98, 1.48) | 0.073 |
| Lumbar lordosis correction | 0.91 (0.85, 0.97) | 0.004 |
| Multivariate Analysis | ||
| Variables | OR (95%) | p-value |
| Age | 1.02 (−0.03, 0.08) | 0.44 |
| ACR correction | 15.98 (0, 5.54) | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-R.; Cheng, T.-A.; Chou, P.-H.; Liu, Y.-F.; Chang, C.-J.; Chuang, C.-F.; Su, P.-F.; Lin, R.-M.; Lin, C.-L. Healing of Vertebral Compression Fractures in the Elderly after Percutaneous Vertebroplasty—An Analysis of New Bone Formation and Sagittal Alignment in a 3-Year Follow-Up. J. Clin. Med. 2022, 11, 708. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030708
Kuo Y-R, Cheng T-A, Chou P-H, Liu Y-F, Chang C-J, Chuang C-F, Su P-F, Lin R-M, Lin C-L. Healing of Vertebral Compression Fractures in the Elderly after Percutaneous Vertebroplasty—An Analysis of New Bone Formation and Sagittal Alignment in a 3-Year Follow-Up. Journal of Clinical Medicine. 2022; 11(3):708. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030708
Chicago/Turabian StyleKuo, Yuh-Ruey, Ting-An Cheng, Po-Hsin Chou, Yuan-Fu Liu, Chao-Jui Chang, Cheng-Feng Chuang, Pei-Fang Su, Ruey-Mo Lin, and Cheng-Li Lin. 2022. "Healing of Vertebral Compression Fractures in the Elderly after Percutaneous Vertebroplasty—An Analysis of New Bone Formation and Sagittal Alignment in a 3-Year Follow-Up" Journal of Clinical Medicine 11, no. 3: 708. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030708