
Effect of a Craniosacral Therapy Protocol in People with Migraine: A Randomized Controlled Trial

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Participants
2.2. Study Design
2.3. Randomization, Blinding, and Masking
2.4. Interventions
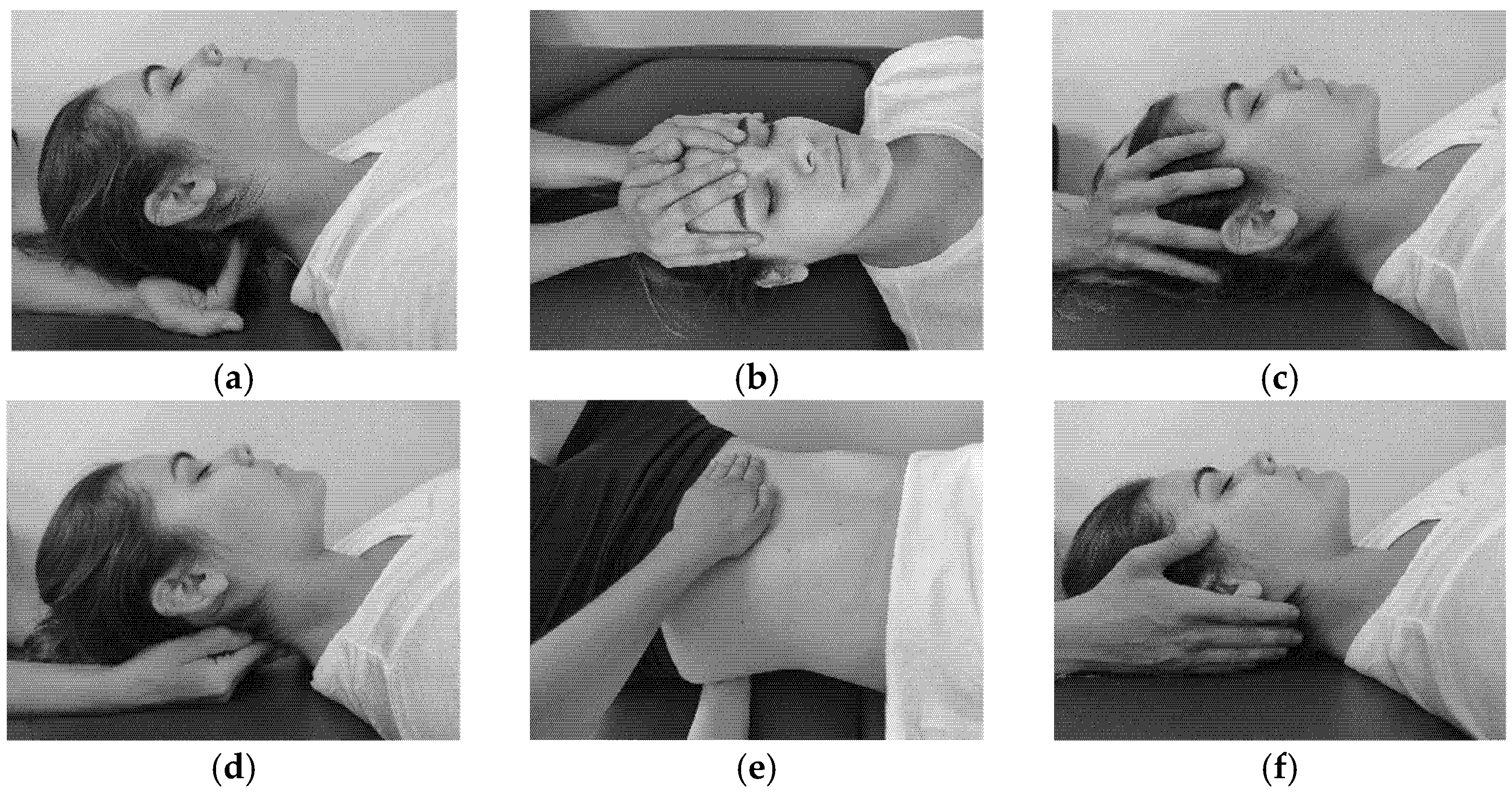
2.4.1. Craniosacral Therapy Group
2.4.2. Sham Control Group
2.5. Assessments
2.6. Sample Size Calculation
2.7. Data Collection and Statistical Analyses
3. Results
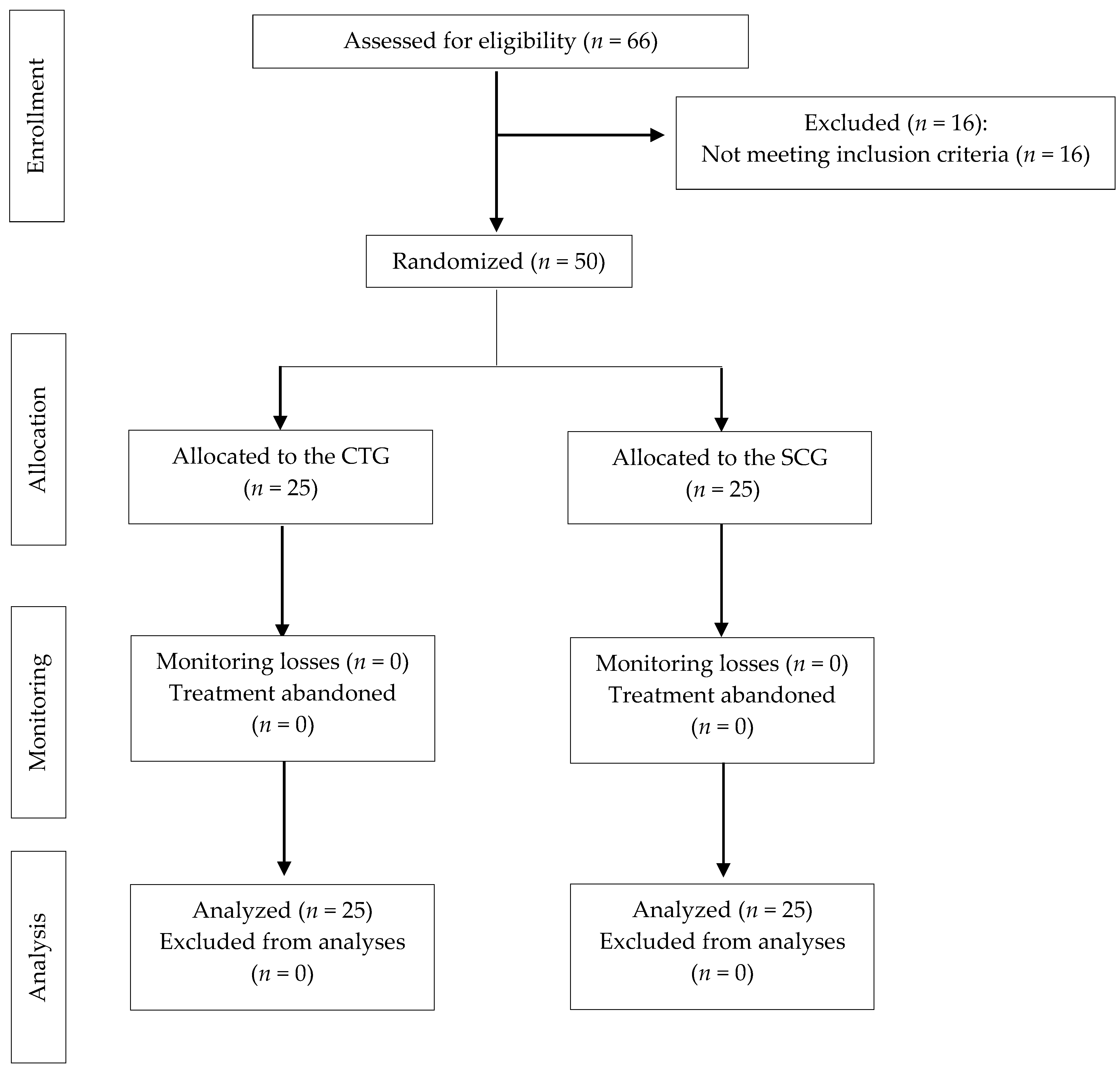
3.1. Participants
3.2. Effect of the Treatment on Pain and Disability
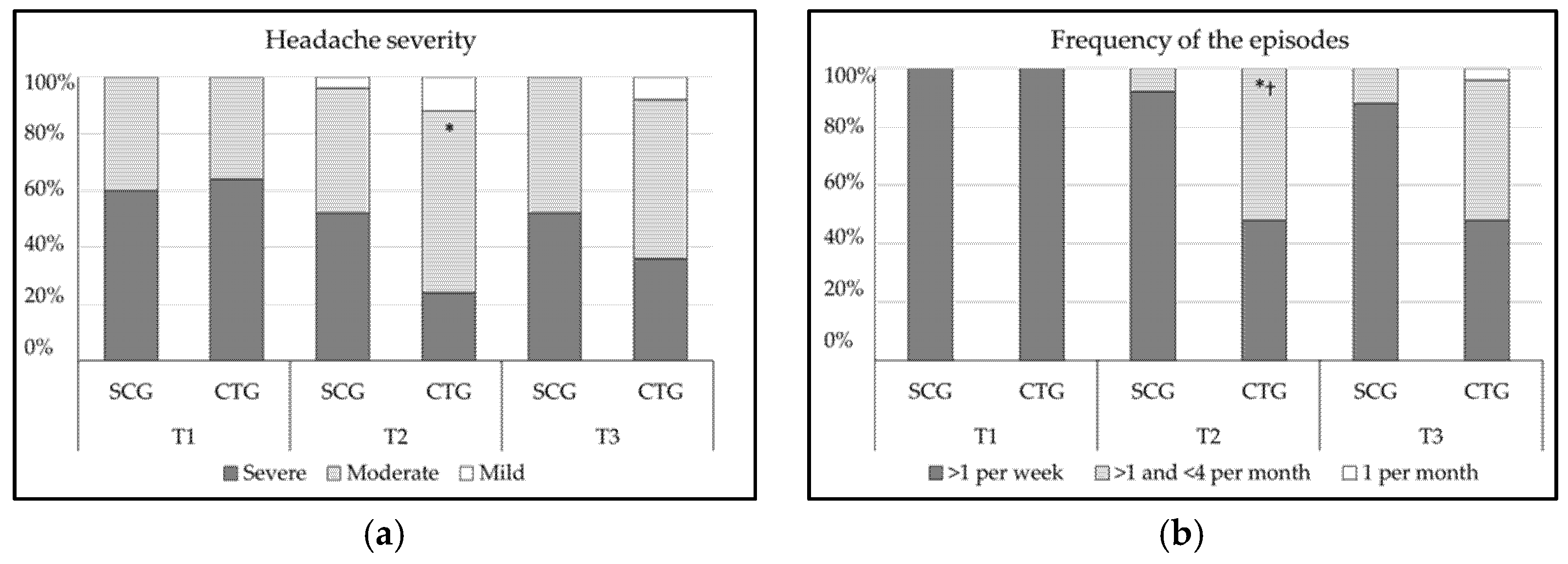
3.3. Effect of the Treatment on Migraine Severity and Frequency of the Episodes
3.4. Effect of the Treatment on Medication Intake
3.5. Self-Reported Perceived Change after Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

References
- Woldeamanuel, Y.W.; Cowan, R.P. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J. Neurol. Sci. 2017, 372, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.; Stovner, L.; Vos, T. Global Burden Disease 2015: Migraine is the third cause of disability in under 50s. J. Headache Pain 2016, 17, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puledda, F.; Messina, R.; Goadsby, P.J. An update on migraine: Current understanding and future directions. J. Neurol. 2017, 264, 2031–2039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luedtke, K.; Starke, W.; May, A. Musculoskeletal dysfunction in migraine patients. Cephalalgia 2017, 38, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Ferracini, G.N.; Florencio, L.L.; Dach, F.; Chaves, T.C.; Palacios-Ceña, M.; Fernández-de-Las-Peñas, C. Myofascial Trigger Points and Migraine-related Disability in Women with Episodic and Chronic Migraine. Clin. J. Pain 2017, 33, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Seng, E.K.; Seng, C.D. Understanding migraine and psychiatric comorbidity. Curr. Opin. Neurol. 2016, 29, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Kelman, L. The triggers or precipitants of the acute migraine attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef]
- Capi, M.; Gentile, G.; Lionetto, L.; Salerno, G.; Cipolla, F.; Curto, M.; Borro, M.; Martelletti, P. Pharmacogenetic considerations for migraine therapies. Expert Opin. Drug Metab. Toxicol. 2018, 14, 1161–1167. [Google Scholar] [CrossRef]
- Luedtke, K.; Allers, A.; Schulte, L.H.; May, A. Efficacy of interventions used by physiotherapists for patients with headache and migraine-systematic review and meta-analysis. Cephalalgia 2016, 36, 474–492. [Google Scholar] [CrossRef]
- Maistrello, L.F.; Geri, T.; Gianola, S.; Zaninetti, M.; Testa, M. Effectiveness of Trigger Point Manual Treatment on the Frequency, Intensity, and Duration of Attacks in Primary Headaches: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Neurol. 2018, 9, 254. [Google Scholar] [CrossRef] [Green Version]
- Beier, D.; Callesen, H.E.; Carlsen, L.N.; Birkefoss, K.; Tómasdóttir, H.; Wűrtzen, H. Manual joint mobilisation techniques, supervised physical activity, psychological treatment, acupuncture and patient education in migraine treatment. A systematic review and meta-analysis. Cephalalgia 2021, 42, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Bryans, R.; Decina, P.; Descarreaux, M.; Duranleau, M.; Marcoux, H.; Potter, B. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J. Manip. Physiol. Ther. 2014, 37, 42–63. [Google Scholar] [CrossRef] [PubMed]
- Chaibi, A.; Tuchin, P.J.; Russell, M.B. Manual therapies for migraine: A systematic review. J. Headache Pain 2011, 12, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maistrello, L.F.; Rafanelli, M.; Turolla, A. Manual Therapy and Quality of Life in People with Headache: Systematic Review and Meta-analysis of Randomized Controlled Trials. Curr. Pain Headache Rep. 2019, 23, 78. [Google Scholar] [CrossRef]
- Haller, H.; Lauche, R.; Sundberg, T.; Dobos, G.; Cramer, H. Craniosacral therapy for chronic pain: A systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2019, 21, 1. [Google Scholar] [CrossRef]
- Harrison, R.E.; Page, J.S. Multipractitioner Upledger CranioSacral Therapy: Descriptive outcome study 2007-2008. J. Altern. Complement. Med. 2011, 17, 13–17. [Google Scholar] [CrossRef]
- Green, C.; Martin, C.; Bassett, K.; Kazanjian, A. A systematic review of craniosacral therapy: Biological plausibility, assessment reliability and clinical effectiveness. Complement. Ther. Med. 1999, 7, 201–207. [Google Scholar] [CrossRef]
- Cutler, M.J.; Holland, B.S.; Stupski, B.A.; Gamber, R.G.; Smith, M.L. Cranial manipulation can alter sleep latency and sympathetic nerve activity in humans: A pilot study. J. Altern. Complement. Med. 2005, 11, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Miana, L.; Bastos, V.H.D.V.; Machado, S.; Arias-Carrión, O.; Nardi, A.E.; Almeida, L.; Ribeiro, P.; Machado, D.; King, H.; Silva, J.G. Changes in alpha band activity associated with application of the compression of fourth ventricular (CV-4) osteopathic procedure: A qEEG pilot study. J. Bodyw. Mov. Ther. 2013, 17, 291–296. [Google Scholar] [CrossRef]
- Jäkel, A.; von Hauenschild, P. A systematic review to evaluate the clinical benefits of craniosacral therapy. Complement. Ther. Med. 2012, 20, 456–465. [Google Scholar] [CrossRef]
- Voigt, K.; Liebnitzky, J.; Burmeister, U.; Sihvonen-Riemenschneider, H.; Beck, M.; Voigt, R.; Bergmann, A. Efficacy of osteopathic manipulative treatment of female patients with migraine: Results of a randomized controlled trial. J. Altern. Complement. Med. 2011, 17, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Cerritelli, F.; Ginevri, L.; Messi, G.; Caprari, E.; Di Vincenzo, M.; Renzetti, C.; Cozzolino, V.; Barlafante, G.; Foschi, N.; Provinciali, L. Clinical effectiveness of osteopathic treatment in chronic migraine: 3-Armed randomized controlled trial. Complement. Ther. Med. 2015, 23, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Rnadottir, T.S.; Sigurdardottir, A.K. Is craniosacral therapy effective for migraine? Tested with HIT-6 Questionnaire. Complement. Ther. Clin. Pract. 2013, 19, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Curtis, P.; Gaylord, S.A.; Park, J.; Faurot, K.R.; Coble, R.; Suchindran, C.; Coeytaux, R.R.; Wilkinson, L.; Mann, J.D. Credibility of low-strength static magnet therapy as an attention control intervention for a randomized controlled study of CranioSacral therapy for migraine headaches. J. Altern. Complement. Med. 2011, 17, 711–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamonseki, D.H.; Lopes, E.P.; Van Der Meer, H.A.; Calixtre, L.B. Effectiveness of manual therapy in patients with tension-type headache. A systematic review and meta-analysis. Disabil. Rehabil. 2020, 12, 1–10. [Google Scholar] [CrossRef]
- Harriott, A.M.; Schwedt, T.J. Migraine is associated with altered processing of sensory stimuli. Curr. Pain Headache Rep. 2014, 18, 458. [Google Scholar] [CrossRef]
- Owen, J.P.; Marco, E.J.; Desai, S.; Fourie, E.; Harris, J.; Hill, S.; Arnett, A.; Mukherjee, P. Abnormal white matter microstructure in children with sensory processing disorders. NeuroImage Clin. 2013, 2, 844–853. [Google Scholar] [CrossRef] [Green Version]
- Harrison, L.A.; Kats, A.; Williams, M.E.; Aziz-Zadeh, L. The importance of sensory processing in mental health: A proposed addition to the Research Domain Criteria (RDoC) and suggestions for RDoC 2.0. Front. Psychol. 2019, 10, 103. [Google Scholar] [CrossRef]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Monzani, L.; Espí-López, G.V.; Zurriaga, R.; Andersen, L.L. Manual therapy for tension-type headache related to quality of work life and work presenteeism: Secondary analysis of a randomized controlled trial. Complement. Ther. Med. 2016, 25, 86–91. [Google Scholar] [CrossRef]
- Espí-López, G.-V.; Ruescas-Nicolau, M.-A.; Nova-Redondo, C.; Benítez-Martínez, J.C.; Dugailly, P.-M.; Falla, D. Effect of Soft Tissue Techniques on Headache Impact, Disability, and Quality of Life in Migraine Sufferers: A Pilot Study. J. Altern. Complement. Med. 2018, 24, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Toro-Velasco, C.; Arroyo-Morales, M.; Fernández-De-Las-Peñas, C.; Cleland, J.A.; Hernández, F.J.B. Short-term effects of manual therapy on heart rate variability, mood state, and pressure pain sensitivity in patients with chronic tension-type headache: A pilot study. J. Manip. Physiol. Ther. 2009, 32, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Upledger, J.E. Craniosacral Therapy. In Complementary and Alternative Medicine; Novey, D.W., Ed.; Mosby: Maryland Heights, MO, USA, 2000; pp. 381–392. [Google Scholar]
- Schueler, M.; Neuhuber, W.L.; De Col, R.; Messlinger, K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache: J. Head Face Pain 2014, 54, 996–1009. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Martos, I.; Valenza, M.C.; Valenza-Demet, G.; Benítez-Feliponi, A.; Robles-Vizcaíno, C.; Ruiz-Extremera, A. Effects of manual therapy on treatment duration and motor development in infants with severe nonsynostotic plagiocephaly: A randomised controlled pilot study. Child’s Nerv. Syst. 2016, 32, 2211–2217. [Google Scholar] [CrossRef] [PubMed]
- Hanten, W.P.; Olson, S.L.; Hodson, J.L.; Imler, V.L.; Knab, V.M.; Magee, J.L. The Effectiveness of CV-4 and Resting Position Techniques on Subjects with Tension-Type Headaches. J. Man. Manip. Ther. 1999, 7, 64–70. [Google Scholar] [CrossRef]
- Zurowska, A.; Malak, R.; Kołcz-Trzęsicka, A.; Samborski, W.; Paprocka-Borowicz, M. Compression of the fourth ventricle using a craniosacral osteopathic technique: A systematic review of the clinical evidence. Evid.-Based Complement. Altern. Med. 2017, 2017, 2974962. [Google Scholar] [CrossRef] [Green Version]
- Cardoso-De-Mello-E-Mello-Ribeiro, A.P.; Blanco, C.R.; Riquelme, I.; Heredia-Rizo, A.M.; Ricard, F.; Oliva-Pascual-Vaca, Á. Effects of the Fourth Ventricle Compression in the Regulation of the Autonomic Nervous System: A Randomized Control Trial. Evid.-Based Complement. Altern. Med. 2015, 2015, 148285. [Google Scholar] [CrossRef] [Green Version]
- Núñez-Pereira, S.; Hitzl, W.; Bullmann, V.; Meier, O.; Koller, H. Sagittal balance of the cervical spine: An analysis of occipitocervical and spinopelvic interdependence, with C-7 slope as a marker of cervical and spinopelvic alignment. J. Neurosurg. Spine 2015, 23, 16–23. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the Visual Analog Scale for Measurement of Acute Pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Jacobson, G.P.; Ramadan, N.M.; Aggarwal, S.K.; Newman, C.W. The Henry Ford Hospital Headache Disability Inventory (HDI). Neurology 1994, 44, 837. [Google Scholar] [CrossRef]
- Luedtke, K.; Basener, A.; Bedei, S.; Castien, R.; Chaibi, A.; Falla, D.; Fernández-De-Las-Peñas, C.; Gustafsson, M.; Hall, T.; Jull, G.; et al. Outcome measures for assessing the effectiveness of non-pharmacological interventions in frequent episodic or chronic migraine: A Delphi study. BMJ Open 2020, 10, e029855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Gómez, E.; Inglés, M.; Serra-Añó, P.; Espí-López, G.V. Effectiveness of a manual therapy protocol based on articulatory techniques in migraine patients. A randomized controlled trial. Musculoskelet. Sci. Pract. 2021, 54, 102386. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.; Scheman, J. Patient global impression of change scores within the context of a chronic pain rehabilitation program. J. Pain 2009, 10, S73. [Google Scholar] [CrossRef]
- Kamper, S.J.; Maher, C.G.; Mackay, G. Global Rating of Change Scales: A Review of Strengths and Weaknesses and Considerations for Design. J. Man. Manip. Ther. 2009, 17, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Thalheimer, W.; Cook, S. How to calculate effect sizes from published research: A simplified methodology. Work-Learn. Res. 2002, 1, 1–9. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Fuensalida-Novo, S.; Parás-Bravo, P.; Jiménez-Antona, C.; Castaldo, M.; Wang, K.; Benito-González, E.; Arendt-Nielsen, L.; Fernández-De-Las-Peñas, C. Gender differences in clinical and psychological variables associated with the burden of headache in tension-type headache. Women Health 2020, 60, 652–663. [Google Scholar] [CrossRef]
- Pellegrino, A.B.W.; Davis-Martin, R.E.; Houle, T.; Turner, D.P.; Smitherman, T. Perceived triggers of primary headache disorders: A meta-analysis. Cephalalgia 2017, 38, 1188–1198. [Google Scholar] [CrossRef]
- Bushnell, M.C.; Ceko, M.; Low, L. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Diener, H.-C.; Tassorelli, C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of acute treatment of migraine attacks in adults: Fourth edition. Cephalalgia 2019, 39, 687–710. [Google Scholar] [CrossRef] [Green Version]
- Emshoff, R.; Bertram, S.; Emshoff, I. Clinically important difference thresholds of the visual analog scale: A conceptual model for identifying meaningful intraindividual changes for pain intensity. Pain 2011, 152, 2277–2282. [Google Scholar] [CrossRef] [PubMed]
- Garrigós-Pedrón, M.; La Touche, R.; Navarro-Desentre, P.; Gracia-Naya, M.; Segura-Ortí, E. Effects of a Physical Therapy Protocol in Patients with Chronic Migraine and Temporomandibular Disorders: A Randomized, Single-Blinded, Clinical Trial. J. Oral Facial Pain Headache 2018, 32, 137–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassorelli, C.; Tramontano, M.; Berlangieri, M.; Schweiger, V.; D’ippolito, M.; Palmerini, V.; Bonazza, S.; Rosa, R.; Cerbo, R.; Buzzi, M.G. Assessing and treating primary headaches and cranio-facial pain in patients undergoing rehabilitation for neurological diseases. J. Headache Pain 2017, 18, 99. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, J.E.; Becker, W.J. Migraine Frequency and Intensity: Relationship with Disability and Psychological Factors—PubMed. Headache J. Head Face Pain 2003, 43, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Louter, M.; Pijpers, J.; Wardenaar, K.; van Zwet, E.; van Hemert, A.; Zitman, F.; Ferrari, M.; Penninx, B.; Terwindt, G. Symptom dimensions of affective disorders in migraine patients. J. Psychosom. Res. 2015, 79, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Kong, F.; Buse, D.C. Predictors of episodic migraine transformation to chronic migraine: A systematic review and meta-analysis of observational cohort studies. Cephalalgia 2019, 40, 503–516. [Google Scholar] [CrossRef]
- Buse, D.C.; Greisman, J.D.; Baigi, K.; Lipton, R.B. Migraine Progression: A Systematic Review. Headache 2019, 59, 306–338. [Google Scholar] [CrossRef]
- May, A.; Schulte, L.H. Chronic migraine: Risk factors, mechanisms and treatment. Nat. Rev. Neurol. 2016, 12, 455–464. [Google Scholar] [CrossRef]
- D’ippolito, M.; Tramontano, M.; Buzzi, M.G. Effects of Osteopathic Manipulative Therapy on Pain and Mood Disorders in Patients with High-Frequency Migraine. J. Osteopat. Med. 2017, 117, 365–369. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.; Geroin, C.; Valè, N.; Marchioretto, F.; Turrina, A.; Dimitrova, E. Does myofascial and trigger point treatment reduce pain and analgesic intake in patients undergoing onabotulinumtoxin A injection due to chronic intractable migraine? Eur. J. Phys. Rehabil. Med. 2018, 54, 1–12. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Ceña, M.P.; Castaldo, M.; Wang, K.; Guerrero-Peral, Á.; Catena, A.; Arendt-Nielsen, L. Variables associated with use of symptomatic medication during a headache attack in individuals with tension-type headache: A European study. BMC Neurol. 2020, 20, 43. [Google Scholar] [CrossRef] [PubMed]
- Hurst, H.; Bolton, J. Assessing the clinical significance of change scores recorded on subjective outcome measures. J. Manip. Physiol. Ther. 2004, 27, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Perrot, S.; Lanteri-Minet, M. Patients’ Global Impression of Change in the management of peripheral neuropathic pain: Clinical relevance and correlations in daily practice. Eur. J. Pain 2019, 23, 1117–1128. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the Clinical Importance of Treatment Outcomes in Chronic Pain Clinical Trials: IMMPACT Recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef]
- Bevilaqua-Grossi, D.; Gonçalves, M.C.; Carvalho, G.; Florencio, L.L.; Dach, F.; Speciali, J.G.; Bigal, M.E.; Chaves, T. Additional Effects of a Physical Therapy Protocol on Headache Frequency, Pressure Pain Threshold, and Improvement Perception in Patients with Migraine and Associated Neck Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2016, 97, 866–874. [Google Scholar] [CrossRef]
- S.L.U 2022 Viguera Editores. 1st Post-European Headache Federation Meeting: A Review of the Latest Developments Presented at the 2020 European Headache Federation Congress: Neurología.com. Available online: http://www.neurologia.com/articulo/2021155/eng (accessed on 25 January 2022).
- Geri, T.; Viceconti, A.; Minacci, M.; Testa, M.; Rossettini, G. Manual therapy: Exploiting the role of human touch. Musculoskelet. Sci. Pract. 2019, 44, 102044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | SCG (n = 25) | CTG (n = 25) |
|---|---|---|
| Gender a | ||
| Male | 5 (20) | 5 (20) |
| Female | 20 (80) | 20 (80) |
| Migraine frequency a | ||
| From 4 to 15 days per month | 14 (56) | 15 (60) |
| >15 days per month | 11 (44) | 10 (40) |
| Medication a | ||
| Preventive medication | 1 (4) | 2 (8) |
| Symptomatic medication | 24 (96) | 22 (88) |
| No medication | 0 (0) | 1 (4) |
| Family history a | 17 (68) | 18 (72) |
| Trigger factors a | ||
| Hormonal changes | 9 (36) | 8 (32) |
| Food or drink | 7 (28) | 6 (24) |
| Stress | 16 (64) | 18 (72) |
| Fatigue, exertion | 8 (32) | 10 (40) |
| Other (change in weather, medication) | 7 (28) | 11 (44) |
| Hormonal changes | 9 (36) | 8 (32) |
| Food or drink | 7 (28) | 6 (24) |
| Accompanying symptoms a | ||
| Nausea/vomiting | 16 (64) | 12 (48) |
| Aura | 6 (24) | 4 (16) |
| Photophobia | 15 (60) | 16 (64) |
| Phonophobia | 10 (40) | 10 (40) |
| Age b | 37.64 (9.42) | 40.92 (7.95) |
| Age of onset b | 19.96 (10.71) | 18.72 (11.2) |
| Period of evolution (years) b | 17.68 (9.94) | 22.20 (12.36) |
| Pain b | 7.68 (1.02) | 7.60 (1.15) |
| MANOVA Interaction Results | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| F(6, 190) = 2.90, p = 0.01, ŋ2 = 0.09 | |||||||||
| Measurement Time Comparison Mean (Standard Deviation) | Group Comparison Mean Difference (95%CI); Effect Size (d) | p-Values of the Univariate Analysis | |||||||
| Variable | Group | T1 | T2 | T3 | T2 | T3 | PTime | PGroup | PTime × Group |
| Pain (VAS) | SCG | 7.68 (1.02) | 7.42 (1.57) | 7.26 (1.25) | 0.96 † (0.2 to 1.72); p = 0.01; d = 0.74 | 0.86 † (0.11 to 1.61); p = 0.03; d = 0.66 | <0.01 | 0.02 | 0.05 |
| CTG | 7.60 (1.15) | 6.46 * (1.04) | 6.40 * (1.38) | ||||||
| Functional disability (HDI) | SCG | 33.76 (7.06) | 32.64 (6.63) | 32.12 (5.99) | 7.76 † (3.46 to 12.06); p = 0.001; d = 0.18 | 6.76 † (2.44 to 11.08); p = 0.003; d = 1.03 | <0.01 | 0.01 | <0.01 |
| CTG | 32.40 (7.75) | 24.88 * (8.41) | 25.36 * (8.92) | ||||||
| Emotional disability (HDI) | SCG | 26.40 (10.65) | 25.44 (9.05) | 25.04 (10.71) | 5.12 (−1.85 to 12.09); p = 0.15 | 4.08 (−2.5 to 10.66); p = 0.22 | 0.08 | 0.26 | 0.29 |
| CTG | 26.32 (12.13) | 20.32 (14.8) | 20.96 * (12.36) | ||||||
| Overall disability (HDI) | SCG | 60.16 (15.87) | 58.08 (14.19) | 57.16 (14.71) | 12.88 † (2.58 to 23.18); p = 0.02; d = 0.73 | 10.84 † (0.85 to 20.83); p = 0.03; d = 0.62 | <0.01 | 0.05 | 0.05 |
| CTG | 58.72 (18.32) | 45.20 * (21.31) | 46.32 * (20.01) | ||||||
| Medication intake (%) | SCG | - | 14.54 (25.17) | 12.08 (27.34) | −21.5 † (−37.98 to -5.01); p = 0.01; d = −0.76 | −18.92 † (−34.3 to -3.53); p = 0.02; d = −0.71 | |||
| CTG | - | 36.04 * (31.66) | 31.00 * (26.18) | 0.48 | <0.01 | 0.81 | |||
| Measurement Times | ||||
|---|---|---|---|---|
| SCG (n = 25) | CTG (n = 25) | |||
| T2 | T3 | T2 | T3 | |
| Self-Reported Perceived Change after Treatment (PGIC Scale) | p > 0.05 | χ2(4) = 10.90, p < 0.01, CC = 0.42 | ||
| Minimally worse | 2 (8) | 3 (12) | 0 (0) | 0 (0) |
| No change | 15 (60) | 20 (80) | 7 (28) | 8 (32) |
| Minimally improved | 6 (24) | 2 (8) | 5 (20) | 14 (56) |
| Much improved | 2 (8) | 0 (0) | 11 (44) | 3 (12) |
| Very much improved | 0 (0) | 0 (0) | 2 (8) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Gómez, E.; Inglés, M.; Aguilar-Rodríguez, M.; Mollà-Casanova, S.; Sempere-Rubio, N.; Serra-Añó, P.; Espí-López, G.V. Effect of a Craniosacral Therapy Protocol in People with Migraine: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 759. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030759
Muñoz-Gómez E, Inglés M, Aguilar-Rodríguez M, Mollà-Casanova S, Sempere-Rubio N, Serra-Añó P, Espí-López GV. Effect of a Craniosacral Therapy Protocol in People with Migraine: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(3):759. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030759
Chicago/Turabian StyleMuñoz-Gómez, Elena, Marta Inglés, Marta Aguilar-Rodríguez, Sara Mollà-Casanova, Núria Sempere-Rubio, Pilar Serra-Añó, and Gemma V. Espí-López. 2022. "Effect of a Craniosacral Therapy Protocol in People with Migraine: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 3: 759. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030759