
Possible Existence of Cochlear Synaptopathy in Patients Completely Recovered from Idiopathic Sudden Sensorineural Hearing Loss


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Ethical Issues
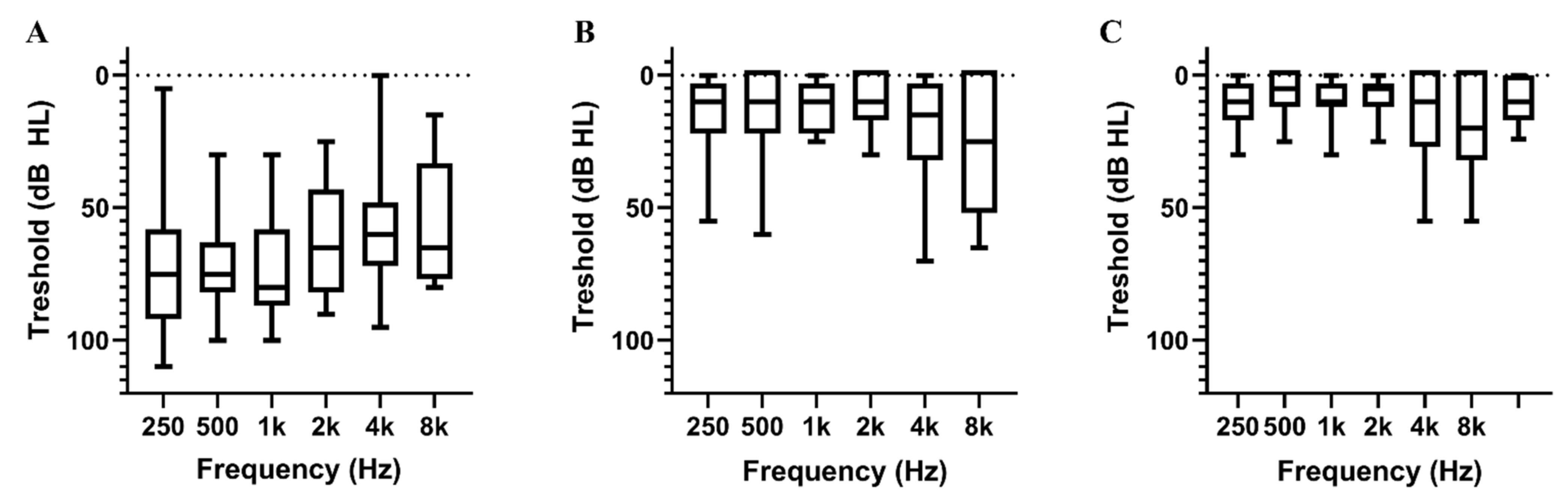
2.3. Audiometric Evaluation
2.4. Hearing Questionnaires
- (0)
- No hearing difficulty;
- (1)
- Mild hearing difficulty;
- (2)
- Moderate hearing difficulty;
- (3)
- Moderate to severe hearing difficulty;
- (4)
- Severe hearing difficulty;
- (5)
- Cannot hear at all.
- (1)
- Do you have trouble hearing when there is noise in the background?
- (2)
- Do you have a problem hearing on the telephone?
- (3)
- Is it difficult for you to follow a conversation when people talk at once?
- (4)
- Do you feel people you are talking to seem to mumble?
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
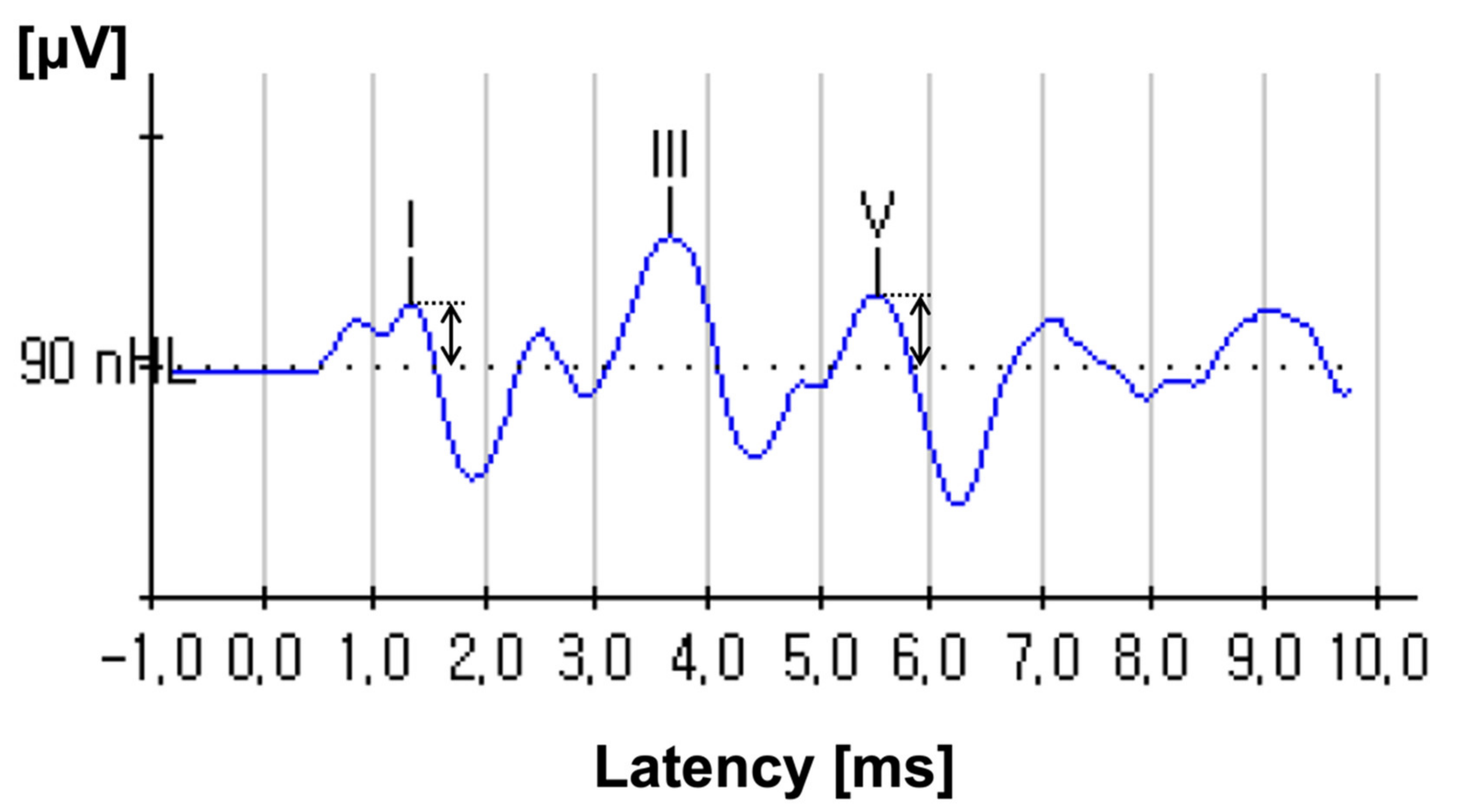
3.2. ABR Amplitudes
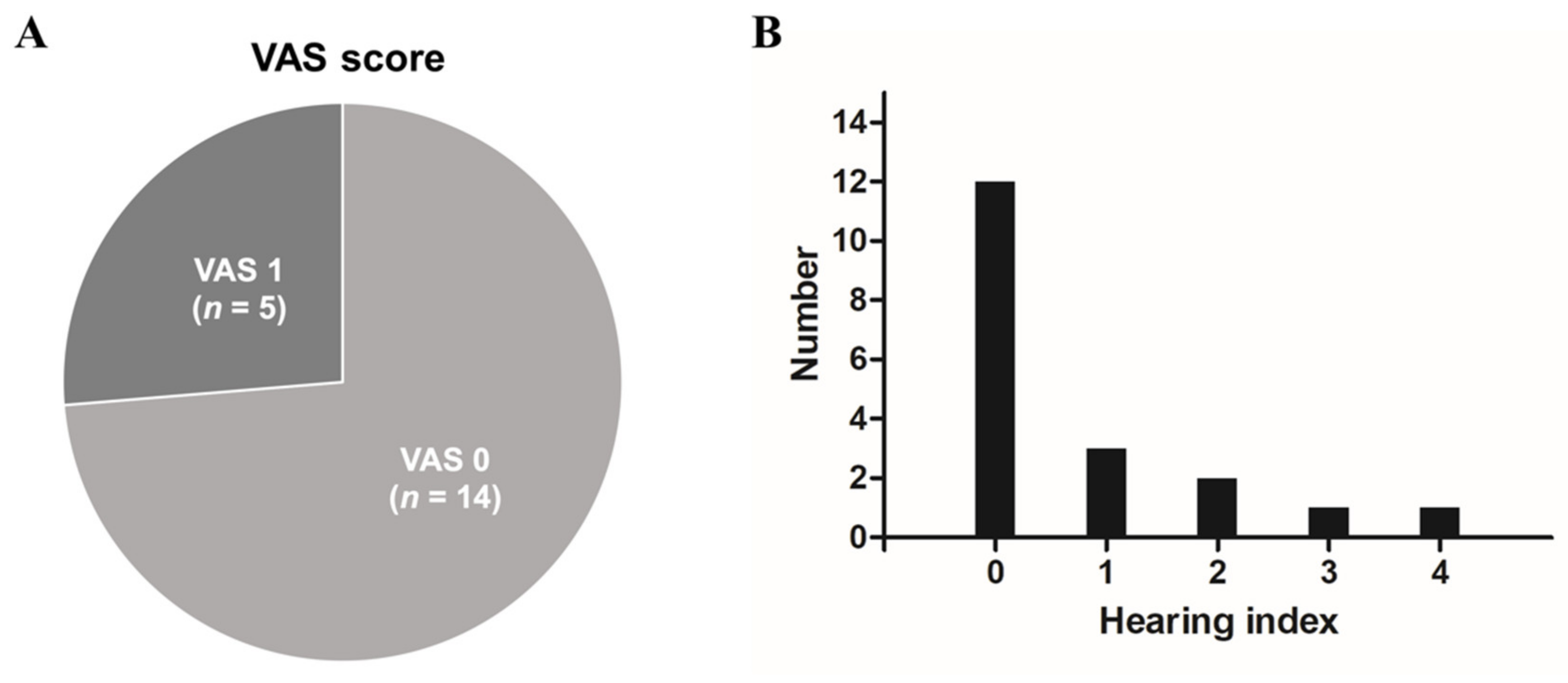
3.3. Hearing Questionnaire
3.4. Association between Wave I Amplitude and Other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marmel, F.; Cortese, D.; Kluk, K. The ongoing search for cochlear synaptopathy in humans: Masked thresholds for brief tones in Threshold Equalizing Noise. Hear. Res. 2020, 392, 107960. [Google Scholar] [CrossRef] [PubMed]
- Plack, C.J.; Barker, D.; Prendergast, G. Perceptual consequences of “hidden” hearing loss. Trends Hear. 2014, 18, 2331216514550621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaette, R.; McAlpine, D. Tinnitus with a normal audiogram: Physiological evidence for hidden hearing loss and computational model. J. Neurosci. 2011, 31, 13452–13457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohrman, D.C.; Wan, G.; Cassinotti, L.; Corfas, G. Hidden Hearing Loss: A Disorder with Multiple Etiologies and Mechanisms. Cold Spring Harb. Perspect. Med. 2020, 10, a035493. [Google Scholar] [CrossRef] [Green Version]
- Kujawa, S.G.; Liberman, M.C. Adding insult to injury: Cochlear nerve degeneration after “temporary” noise-induced hearing loss. J. Neurosci. 2009, 29, 14077–14085. [Google Scholar] [CrossRef] [Green Version]
- Kujawa, S.G.; Liberman, M.C. Synaptopathy in the noise-exposed and aging cochlea: Primary neural degeneration in acquired sensorineural hearing loss. Hear. Res. 2015, 330, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Chang, Y.; Li, X.; Aiken, S.; Liu, L.; Wang, J. Cochlear Synaptopathy and Noise-Induced Hidden Hearing Loss. Neural Plast. 2016, 2016, 6143164. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.K.; Lim, H.W.; Park, H.J.; Pak, J.H.; Chung, J.W. Changes of Cochlear Nerve Terminals after Temporary Noise-Induced Hearing Loss. Korean J. Otorhinolaryngol. Head Neck Surg. 2013, 56, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Rauch, S.D. Clinical practice. Idiopathic sudden sensorineural hearing loss. N. Engl. J. Med. 2008, 359, 833–840. [Google Scholar] [CrossRef]
- Edizer, D.T.; Çelebi, Ö.; Hamit, B.; Baki, A.; Yiğit, Ö. Recovery of Idiopathic Sudden Sensorineural Hearing Loss. J. Int. Adv. Otol. 2015, 11, 122–126. [Google Scholar] [CrossRef]
- Rhee, T.M.; Hwang, D.; Lee, J.S.; Park, J.; Lee, J.M. Addition of Hyperbaric Oxygen Therapy vs Medical Therapy Alone for Idiopathic Sudden Sensorineural Hearing Loss: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirian, C.; Ovesen, T. Intratympanic vs. Systemic Corticosteroids in First-line Treatment of Idiopathic Sudden Sensorineural Hearing Loss: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 421–428. [Google Scholar] [CrossRef]
- Seo, H.W.; Chung, J.H.; Byun, H.; Lee, S.H. Vestibular mapping assessment in idiopathic sudden sensorineural hearing loss. Ear Hear. 2021, 43, 242–2549. [Google Scholar] [CrossRef]
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G.; et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol. Head Neck Surg. 2019, 161, S1–S45. [Google Scholar] [CrossRef] [Green Version]
- Kamerer, A.M.; Neely, S.T.; Rasetshwane, D.M. A model of auditory brainstem response wave I morphology. J. Acoust. Soc. Am. 2020, 147, 25. [Google Scholar] [CrossRef] [PubMed]
- Dallos, P. Cochlear amplification, outer hair cells and prestin. Curr. Opin. Neurobiol. 2008, 18, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Moser, T.; Predoehl, F.; Starr, A. Review of hair cell synapse defects in sensorineural hearing impairment. Otol Neurotol 2013, 34, 995–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickman, T.T.; Smalt, C.; Bobrow, J.; Quatieri, T.; Liberman, M.C. Blast-induced cochlear synaptopathy in chinchillas. Sci. Rep. 2018, 8, 10740. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, K.A.; Guo, D.; Micucci, S.; De Gruttola, V.; Liberman, M.C.; Kujawa, S.G. Noise-induced Cochlear Synaptopathy with and Without Sensory Cell Loss. Neuroscience 2020, 427, 43–57. [Google Scholar] [CrossRef]
- Eggermont, J.J. Auditory brainstem response. Handb. Clin. Neurol. 2019, 160, 451–464. [Google Scholar] [CrossRef]
- Kikidis, D.; Vardonikolaki, A.; Zachou, Z.; Razou, A.; Pantos, P.; Bibas, A. ABR findings in musicians with normal audiogram and otoacoustic emissions: Evidence of cochlear synaptopathy? Hear. Balance Commun. 2020, 18, 36–45. [Google Scholar] [CrossRef]
- Byun, H.; Chung, J.H.; Lee, S.H. Clinical implications of posterior semicircular canal function in idiopathic sudden sensorineural hearing loss. Sci. Rep. 2020, 10, 8313. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients n = 19 |
|---|---|
| Sex (number, %) | |
| Male/Female | 10 (52.6%)/9 (47.4%) |
| Age (years, mean, (range)) | 45.7 ± 16.3, (16–64) |
| Underlying disease (number, %) | |
| Hypertension | 2 (10.5%) |
| Diabetes mellitus | 5 (26.3%) |
| Cardiovascular disease | 5 (26.3%) |
| Affected side | |
| Right/Left | 6 (31.6%)/13 (68.4%) |
| Associated symptom (number, %) | |
| Vertigo | 3 (15.8%) |
| Tinnitus | 17 (89.5%) |
| Ear fullness | 15 (78.9%) |
| Onset of treatment (days) | 3.5 ± 2.4 |
| Initial hearing | |
| Pure tone threshold (dB) | 65.7 ± 17.8 |
| Word recognition score (%) | 34.0 ± 31.3 |
| Hearing level after treatment | |
| Pure tone threshold (dB) | 12.6 ± 7.8 |
| Word recognition score (%) | 97.3 ± 3.9 |
| Hearing level of unaffected side | |
| Pure tone threshold (dB) | 9.3 ± 7.2 |
| Word recognition score (%) | 99.6 ± 1.2 |
| Treatment method (number, %) | |
| High dose steroid | 4 (21.1%) |
| Oral steroid + Intratympanic steroid | 13 (68.4%) |
| Intratympanic steroid only | 2 (10.5%) |
| Wave I (μV) | Wave V (μV) | Wave I/V Ratio | |
|---|---|---|---|
| Recovered side | 0.16 ± 0.10 | 0.21 ± 0.08 | 0.94 ± 0.73 |
| Healthy side | 0.22 ± 0.13 | 0.24 ± 0.10 | 0.97 ± 0.66 |
| p value * | 0.002 | 0.985 | 0.107 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, H.W.; Lee, S.Y.; Byun, H.; Lee, S.H.; Chung, J.H. Possible Existence of Cochlear Synaptopathy in Patients Completely Recovered from Idiopathic Sudden Sensorineural Hearing Loss. J. Clin. Med. 2022, 11, 875. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030875
Seo HW, Lee SY, Byun H, Lee SH, Chung JH. Possible Existence of Cochlear Synaptopathy in Patients Completely Recovered from Idiopathic Sudden Sensorineural Hearing Loss. Journal of Clinical Medicine. 2022; 11(3):875. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030875
Chicago/Turabian StyleSeo, Hee Won, Seung Yeol Lee, Hayoung Byun, Seung Hwan Lee, and Jae Ho Chung. 2022. "Possible Existence of Cochlear Synaptopathy in Patients Completely Recovered from Idiopathic Sudden Sensorineural Hearing Loss" Journal of Clinical Medicine 11, no. 3: 875. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030875