
LOQTEQ® VA Periprosthetic Plate—A New Concept for Bicortical Screw Fixation in Periprosthetic Fractures: A Technical Note

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
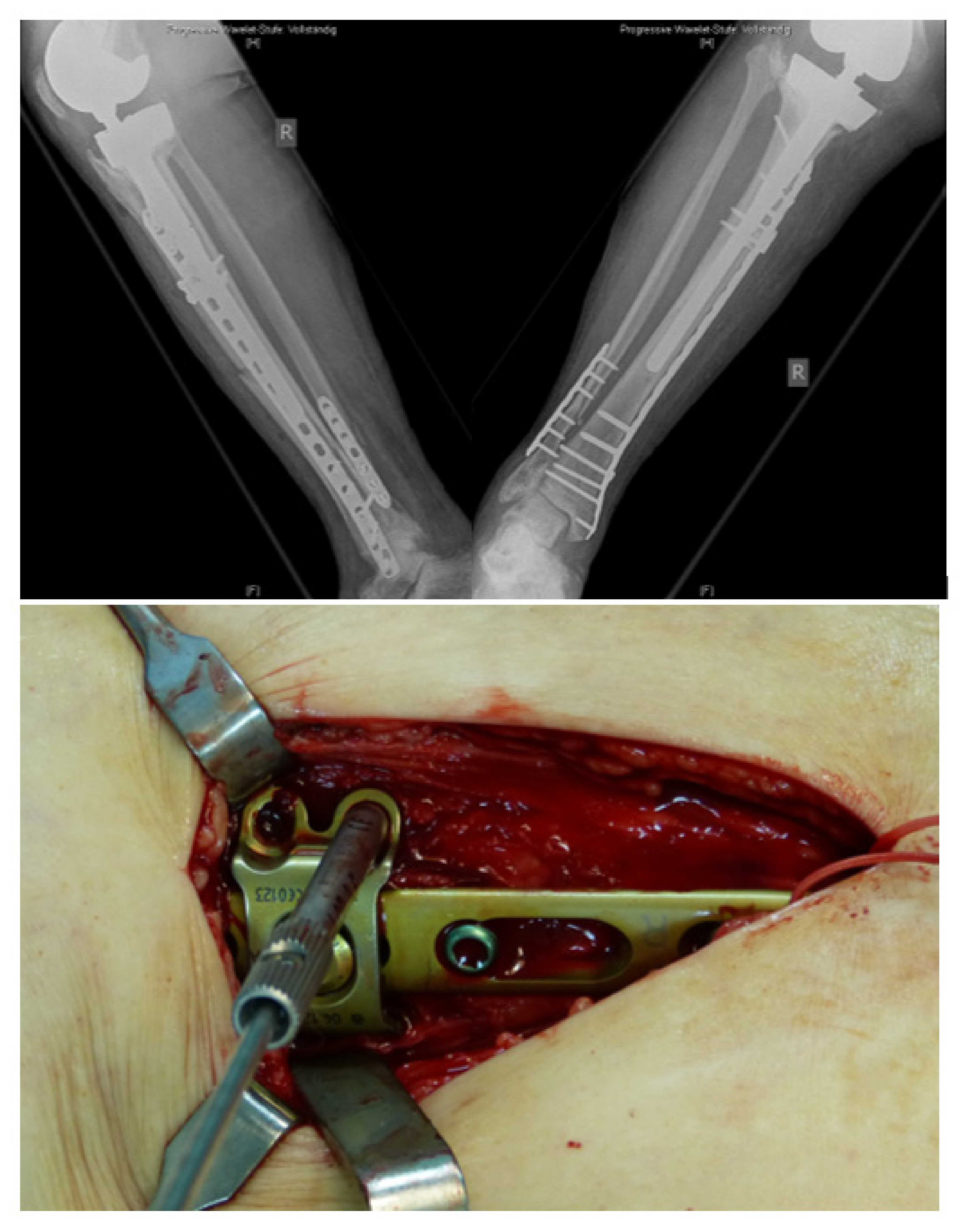
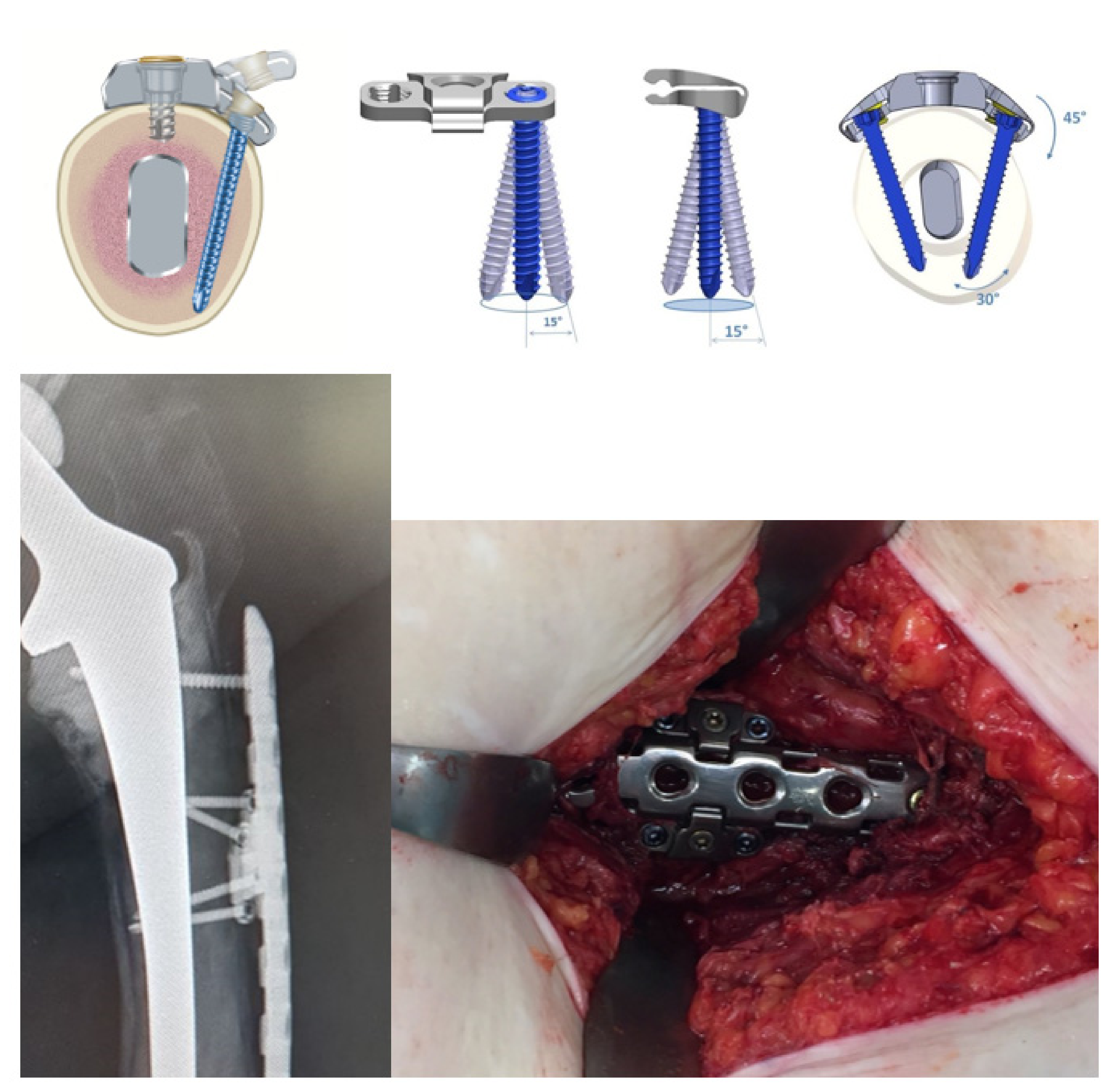
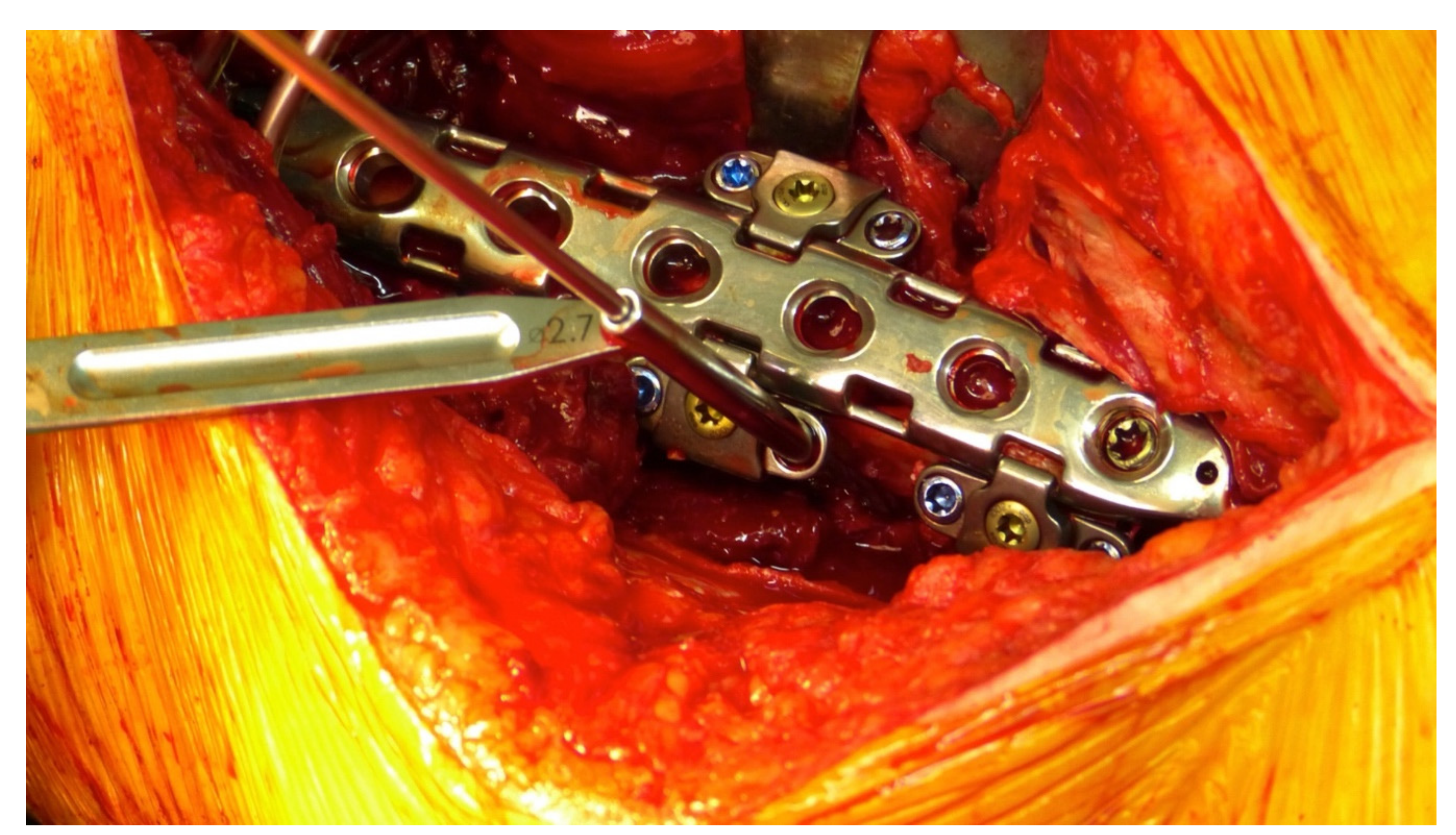
2.1. Surgical Technique and Implant
2.2. Intra- and Perioperative Data
2.3. Clinical Scores and Radiological Examinations
2.4. Statistics
3. Results
3.1. Epidemiological Data
3.2. Intraoperative Technical Data
3.3. Postoperative Clinical and Radiological Follow-Up
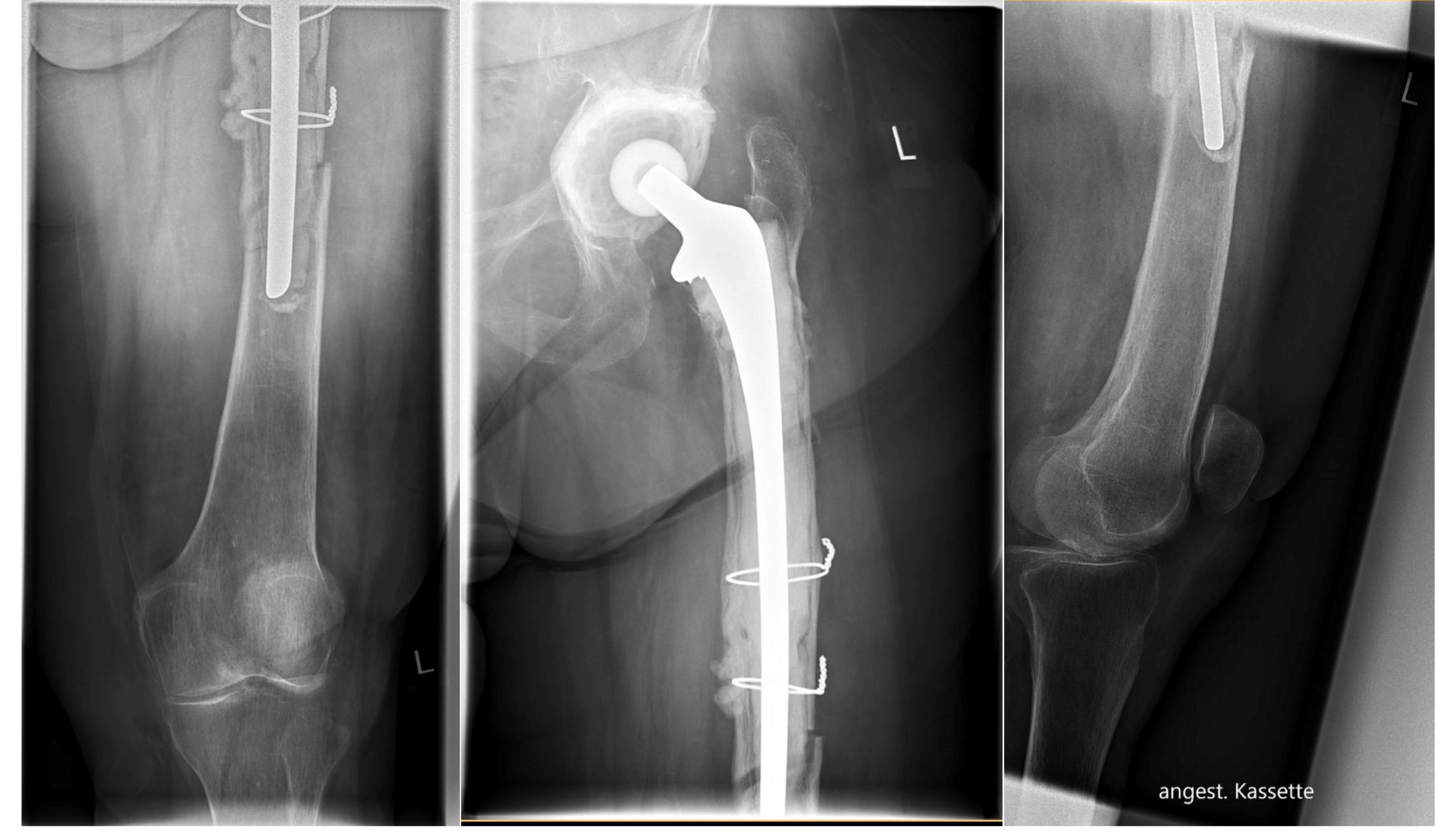
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Märdian, S.; Perka, C.; Schaser, K.-D.; Gruner, J.; Scheel, F.; Schwabe, P. Cardiac disease and advanced age increase the mortality risk following surgery for periprosthetic femoral fractures. Bone Jt. J. 2017, 99-B, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Füchtmeier, B.; Galler, M.; Müller, F. Mid-Term Results of 121 Periprosthetic Femoral Fractures: Increased Failure and Mortality Within but not After One Postoperative Year. J. Arthroplast. 2015, 30, 669–674. [Google Scholar] [CrossRef]
- Lindahl, H.; Garellick, G.; Regnér, H.; Herberts, P.; Malchau, H. Three Hundred and Twenty-one Periprosthetic Femoral Fractures. J. Bone Jt. Surg. 2006, 88, 1215–1222. [Google Scholar] [CrossRef]
- Märdian, S.; Schaser, K.-D.; Gruner, J.; Scheel, F.; Perka, C.; Schwabe, P. Adequate surgical treatment of periprosthetic femoral fractures following hip arthroplasty does not correlate with functional outcome and quality of life. Int. Orthop. 2015, 39, 1701–1708. [Google Scholar] [CrossRef] [PubMed]
- Della Rocca, G.J.; Leung, K.S.; Pape, H.-C. Periprosthetic Fractures: Epidemiology and Future Projections. J. Orthop. Trauma 2011, 25, S66–S70. [Google Scholar] [CrossRef] [PubMed]
- Young, S.W.; Pandit, S.; Munro, J.T.; Pitto, R.P. Periprosthetic femoral fractures after total hip arthroplasty. ANZ J. Surg. 2007, 77, 424–428. [Google Scholar] [CrossRef]
- Parvizi, J.; Vegari, D.N. Periprosthetic Proximal Femur Fractures: Current Concepts. J. Orthop. Trauma 2011, 25, S77–S81. [Google Scholar] [CrossRef]
- Parvizi, J.; Rapuri, V.R.; Purtill, J.J.; Sharkey, P.F.; Rothman, R.H.; Hozack, W.J. Treatment Protocol for Proximal Femoral Periprosthetic Fractures. J. Bone Jt. Surg. 2004, 86, 8–16. [Google Scholar] [CrossRef]
- Duncan, C.P.; Haddad, F.S. The Unified Classification System (UCS): Improving our understanding of periprosthetic fractures. Bone Jt. J. 2014, 96-B, 713–716. [Google Scholar] [CrossRef]
- Raschke, M.; Stange, R.; Kösters, C. Versorgung periprothetischer und periimplantärer Frakturen. Der Unfallchirurg 2012, 115, 1009–1021. [Google Scholar] [CrossRef]
- Kim, M.B.; Cho, J.-W.; Lee, Y.H.; Shon, W.-Y.; Park, J.W.; Kim, J.; Oh, J.-K. Locking attachment plate fixation around a well-fixed stem in periprosthetic femoral shaft fractures. Arch. Orthop. Trauma. Surg. 2017, 137, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Gwinner, C.; Märdian, S.; Dröge, T.; Schulze, M.; Raschke, M.J.; Stange, R. Bicortical screw fixation provides superior biomechanical stability but devastating failure modes in periprosthetic femur fracture care using locking plates. Int. Orthop. 2015, 39, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Lenz, M.; Perren, S.M.; Gueorguiev, B.; Höntzsch, D.; Windolf, M. Mechanical behavior of fixation components for periprosthetic fracture surgery. Clin. Biomech. 2013, 28, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A.; Mahoney, W.; Johnson, J.; Trompeter, A.; Lowe, J. Biomechanics of periprosthetic femur fractures and early weightbearing. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Wähnert, D.; Müller, M.; Tiedemann, H.; Märdian, S.; Raschke, M.J.; Kösters, C. Periprosthetic fracture fixation in Vancouver B1 femoral shaft fractures: A biomechanical study comparing two plate systems. J. Orthop. Transl. 2020, 24, 150–154. [Google Scholar] [CrossRef]
- Dumpies, C.; Conrad, T.; Marintschev, I.; Hofmann, G. Locking Attachment Plate—Erste Erfahrungen. Z. Orthop. Unfall. 2012, 150, 302–308. [Google Scholar] [CrossRef]
- Wähnert, D.; Grüneweller, N.; Gehweiler, D.; Brunn, B.; Raschke, M.J.; Stange, R. Double plating in Vancouver type B1 periprosthetic proximal femur fractures: A biomechanical study. J. Orthop. Res. 2016, 35, 234–239. [Google Scholar] [CrossRef] [Green Version]
- Lenz, M.; Stoffel, K.; Gueorguiev, B.; Klos, K.; Kielstein, H.; Hofmann, G.O. Enhancing fixation strength in periprosthetic femur fractures by orthogonal plating-A biomechanical study. J. Orthop. Res. 2015, 34, 591–596. [Google Scholar] [CrossRef] [Green Version]
- Stoffel, K.; Sommer, C.; Kalampoki, V.; Blumenthal, A.; Joeris, A. The influence of the operation technique and implant used in the treatment of periprosthetic hip and interprosthetic femur fractures: A systematic literature review of 1571 cases. Arch. Orthop. Trauma. Surg. 2016, 136, 553–561. [Google Scholar] [CrossRef]
- Moreta, J.; Aguirre, U.; de Ugarte, O.S.; Jáuregui, I.; Mozos, J.L.M.-D.L. Functional and radiological outcome of periprosthetic femoral fractures after hip arthroplasty. Injury 2015, 46, 292–298. [Google Scholar] [CrossRef]
- Aprato, A.; Tosto, F.; Comba, A.; Mellano, D.; Piccato, A.; Daghino, W.; Massè, A. The clinical and economic burden of proximal femur periprosthetic fractures. Musculoskelet. Surg. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Caruso, G.; Milani, L.; Marko, T.; Lorusso, V.; Andreotti, M.; Massari, L. Surgical treatment of periprosthetic femoral fractures: A retrospective study with functional and radiological outcomes from 2010 to 2016. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 931–938. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Year) | 80 (SD 11) | n |
|---|---|---|
| Sex | Female | 22 |
| Male | 4 | |
| ASA | ASA1 | 1 |
| ASA2 | 5 | |
| ASA3 | 12 | |
| ASA4 | 8 | |
| ASA5 | 0 | |
| Fracture side | Left | 14 |
| Right | 12 | |
| UCS Classification | IV.3-B1 | 5x |
| IV.3-C | 3x | |
| V.3-B1 | 8x | |
| V.3-B3 | 1x | |
| V.3-C | 3x | |
| V.3D | 6x | |
| Follow-up (month) | 13.9 (SD 12) |
| Patient | OP-Time (min) | Double Plate | HHP * | KSS ** | WOMAC *** | VAS **** | Complications | Fracture Healing |
|---|---|---|---|---|---|---|---|---|
| 1 | 127 | No | 59 | 144 | 20 | 2 | Yes | |
| 2 | 273 | Yes | 77 | 129 | 35 | 0 | Yes | |
| 3 | 191 | No | 99 | 169 | 11 | 0 | Yes | |
| 4 | 307 | No | 42 | 25 | 73 | 4 | sec. dislocation | Yes |
| 5 | 198 | No | 65 | 80 | 36 | 3 | Yes | |
| 6 | 173 | Yes | 37 | 65 | 62 | 3 | Yes | |
| 7 | 128 | Yes | 40 | 113 | 55 | 2 | Yes | |
| 8 | 113 | No | 78 | 175 | 22 | 5 | hematoma | Yes |
| 9 | 125 | No | 94 | 194 | 17 | 2 | Yes | |
| 10 | 113 | Yes | 90 | 169 | 13 | 0 | hematoma | Yes |
| 11 | 54 | Yes | 17 | 47 | 71 | 5 | Yes | |
| 12 | 87 | Yes | 29 | 42 | 62 | 6 | Yes | |
| 13 | 106 | No | 93 | 185 | 12 | 2 | Yes | |
| 14 | 272 | Yes | 63 | 122 | 46 | 2 | Yes | |
| 15 | 208 | Yes | - | - | - | 5 | implant failure | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kösters, C.; den Toom, D.; Märdian, S.; Roßlenbroich, S.; Metzlaff, S.; Daniilidis, K.; Everding, J. LOQTEQ® VA Periprosthetic Plate—A New Concept for Bicortical Screw Fixation in Periprosthetic Fractures: A Technical Note. J. Clin. Med. 2022, 11, 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051184
Kösters C, den Toom D, Märdian S, Roßlenbroich S, Metzlaff S, Daniilidis K, Everding J. LOQTEQ® VA Periprosthetic Plate—A New Concept for Bicortical Screw Fixation in Periprosthetic Fractures: A Technical Note. Journal of Clinical Medicine. 2022; 11(5):1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051184
Chicago/Turabian StyleKösters, Clemens, Daniel den Toom, Sven Märdian, Steffen Roßlenbroich, Sebastian Metzlaff, Kiriakos Daniilidis, and Jens Everding. 2022. "LOQTEQ® VA Periprosthetic Plate—A New Concept for Bicortical Screw Fixation in Periprosthetic Fractures: A Technical Note" Journal of Clinical Medicine 11, no. 5: 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051184