
Autologous Microfragmented Adipose Tissue for the Treatment of Knee Osteoarthritis: Real-World Data at Two Years Follow-Up

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Harvesting the Adipose Tissue
2.3. Processing the Lipoaspirate and Injecting the Microfragmented Adipose Tissue
2.4. Statistical Analysis
3. Results
3.1. Patients’ Demographic
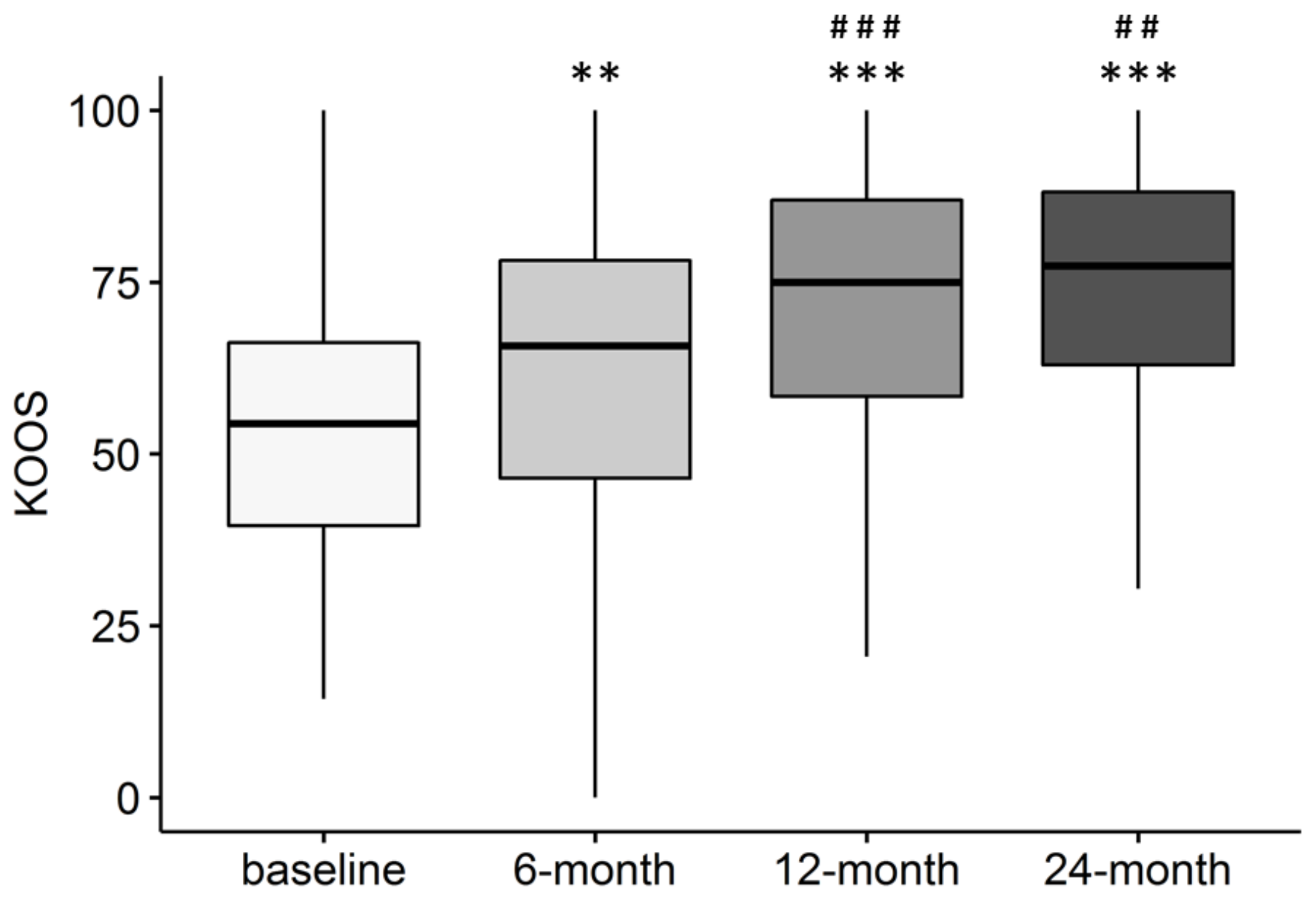
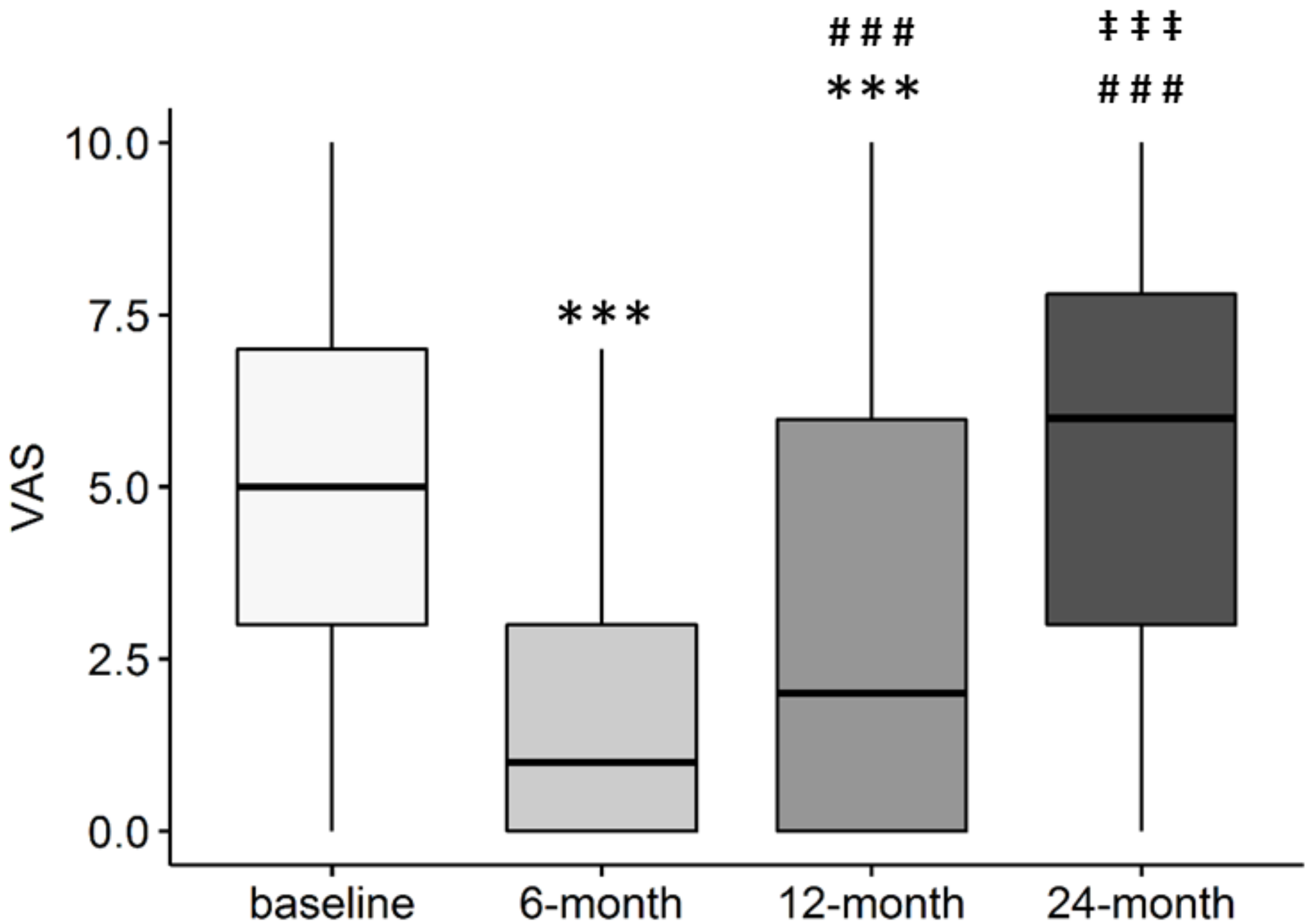
3.2. Patient-Reported Outcome Measures
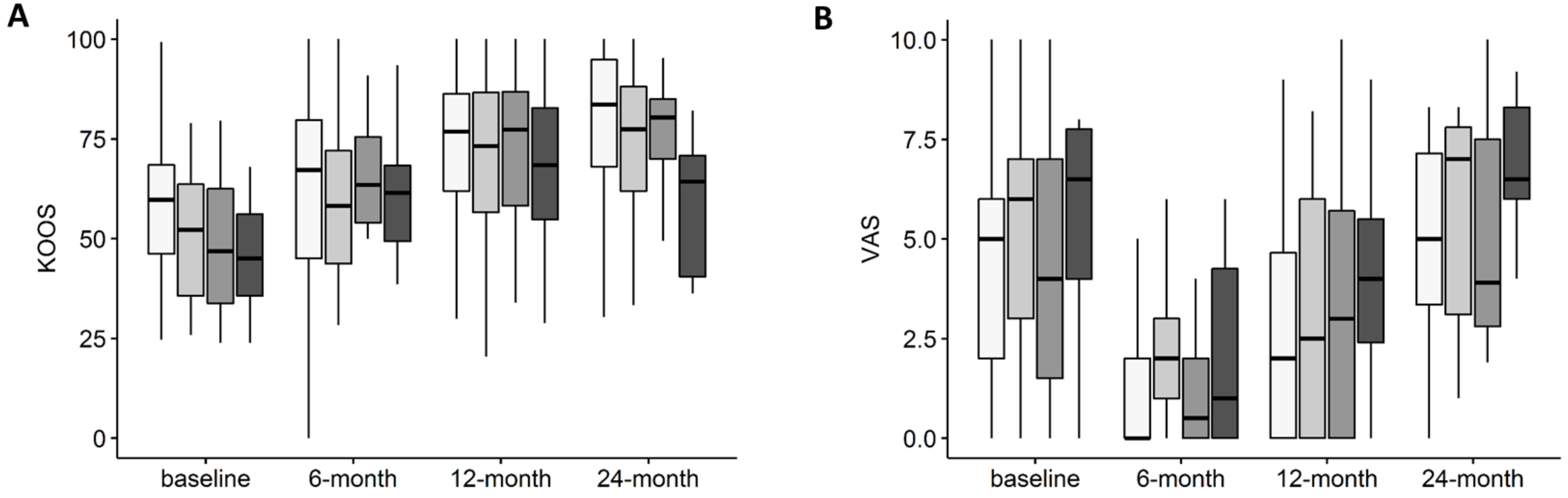
3.3. Variation of KOOS and VAS Depending on OA KL Grade
3.4. Objective Outcomes
3.5. Association of Patients’ Characteristics with Subjective and Objective Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Russo, A.; Screpis, D.; Di Donato, S.L.; Bonetti, S.; Piovan, G.; Zorzi, C. Autologous micro-fragmented adipose tissue for the treatment of diffuse degenerative knee osteoarthritis: An update at 3 year follow-up. J. Exp. Orthop. 2018, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Russo, A.; Condello, V.; Madonna, V.; Guerriero, M.; Zorzi, C. Autologous and micro-fragmented adipose tissue for the treatment of diffuse degenerative knee osteoarthritis. J. Exp. Orthop. 2017, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Natali, S.; Screpis, D.; Farinelli, L.; Iacono, V.; Vacca, V.; Gigante, A.; Zorzi, C. The use of intra-articular injection of autologous micro-fragmented adipose tissue as pain treatment for ankle osteoarthritis: A prospective not randomized clinical study. Int. Orthop. 2021, 45, 2239–2244. [Google Scholar] [CrossRef]
- Panni, A.S.; Vasso, M.; Braile, A.; Toro, G.; De Cicco, A.; Viggiano, D.; Lepore, F. Preliminary results of autologous adipose-derived stem cells in early knee osteoarthritis: Identification of a subpopulation with greater response. Int. Orthop. 2019, 43, 7–13. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, F.; Gravina, P.; Busato, A.; Farinelli, L.; Soranzo, C.; Vidal, L.; Zingaretti, N.; Zavan, B.; Sbarbati, A.; Riccio, M.; et al. Stem cells in autologous microfragmented adipose tissue: Current perspectives in osteoarthritis disease. Int. J. Mol. Sci. 2021, 22, 10197. [Google Scholar] [CrossRef]
- De Girolamo, L.; Kon, E.; Filardo, G.; Marmotti, A.G.; Soler, F.; Peretti, G.; Vannini, F.; Madry, H.; Chubinskaya, S. Regenerative approaches for the treatment of early OA. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1826–1835. [Google Scholar] [CrossRef] [PubMed]
- Zellner, J.; Johnstone, B.; Barry, F.; Madry, H. Mesenchymal stem cell based regenerative treatment of the knee: From basic science to clinics. Stem Cells Int. 2019, 2019, 7608718. [Google Scholar] [CrossRef]
- Malanga, G.A.; Bemanian, S. Microfragmented adipose injections in the treatment of knee osteoarthritis. J. Clin. Orthop. Trauma 2019, 10, 46–48. [Google Scholar] [CrossRef]
- Carelli, S.; Messaggio, F.; Canazza, A.; Hebda, D.M.; Caremoli, F.; Latorre, E.; Grimoldi, M.G.; Colli, M.; Bulfamante, G.; Tremolada, C.; et al. Characteristics and properties of mesenchymal stem cells derived from microfragmented adipose tissue. Cell Transplant. 2015, 24, 1233–1252. [Google Scholar] [CrossRef] [Green Version]
- Senesi, L.; De Francesco, F.; Farinelli, L.; Manzotti, S.; Gagliardi, G.; Papalia, G.F.; Riccio, M.; Gigante, A. Mechanical and enzymatic procedures to isolate the stromal vascular fraction from adipose tissue: Preliminary results. Front. Cell Dev. Biol. 2019, 7, 88. [Google Scholar] [CrossRef]
- The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 11 September 2020).
- Blonde, L.; Khunti, K.; Harris, S.B.; Meizinger, C.; Skolnik, N.S. Interpretation and Impact of Real-World Clinical Data for the Practicing Clinician. Adv. Ther. 2018, 35, 1763–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, F.; Maioli, M.; Leonardi, E.; Olivi, E.; Pasquinelli, G.; Valente, S.; Mendez, A.J.; Ricordi, C.; Raffaini, M.; Tremolada, C.; et al. A new nonenzymatic method and device to obtain a fat tissue derivative highly enriched in pericyte-like elements by mild mechanical forces from human lipoaspirates. Cell Transplant. 2013, 22, 2063–2077. [Google Scholar] [CrossRef]
- Tremolada, C.; Colombo, V.; Ventura, C. Adipose tissue and mesenchymal stem cells: State of the art and lipogems® technology development. Curr. Stem Cell Rep. 2016, 2, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Eymard, F.; Parsons, C.; Edwards, M.; Petit-Dop, F.; Reginster, J.-Y.; Bruyere, O.; Richette, P.; Cooper, C.; Chevalier, X. Diabetes is a risk factor for knee osteoarthritis progression. Osteoarthr. Cartil. 2015, 23, 851–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagoe, C.E.; Wang, W.; Wang, S.; Barbour, K.E. Association of anti-thyroid antibodies with radiographic knee osteoarthritis and chondrocalcinosis: A NHANES III study. Ther. Adv. Musculoskelet. Dis. 2021, 13, 13. [Google Scholar] [CrossRef]
- Mautner, K.; Bowers, R.; Easley, K.; Fausel, Z.; Robinson, R. Functional outcomes following microfragmented adipose tissue versus bone marrow aspirate concentrate injections for symptomatic knee osteoarthritis. Stem Cells Transl. Med. 2019, 8, 1149–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, C.; Lane, N.E.; Hunter, D.J.; Wei, J.; Choi, H.K.; McAlindon, T.E.; Li, H.; Lu, N.; Lei, G.; Zhang, Y. Intra-articular corticosteroids and the risk of knee osteoarthritis progression: Results from the osteoarthritis initiative. Osteoarthr. Cartil. 2019, 27, 855–862. [Google Scholar] [CrossRef]
- Rajamäki, T.J.; Puolakka, P.A.; Hietaharju, A.; Moilanen, T.; Jämsen, E. Predictors of the use of analgesic drugs 1 year after joint replacement: A single-center analysis of 13,000 hip and knee replacements. Arthritis Res. Ther. 2020, 22, 89. [Google Scholar] [CrossRef] [Green Version]
- Heidari, N.; Noorani, A.; Slevin, M.; Cullen, A.; Stark, L.; Olgiati, S.; Zerbi, A.; Wilson, A. Patient-centered outcomes of microfragmented adipose tissue treatments of knee osteoarthritis: An observational, intention-to-treat study at twelve months. Stem Cells Int. 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Borić, I.; Hudetz, D.; Rod, E.; Jeleč, Ž.; Vrdoljak, T.; Skelin, A.; Polašek, O.; Plečko, M.; Trbojević-Akmačić, I.; Lauc, G.; et al. A 24-month follow-up study of the effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2019, 10, 1051. [Google Scholar] [CrossRef] [Green Version]
- Parkes, M.J.; Callaghan, M.; O’Neill, T.; Forsythe, L.M.; Lunt, M.; Felson, D. Sensitivity to change of patient-preference measures for pain in patients with knee osteoarthritis: Data from two trials. Arthritis Care Res. 2016, 68, 1224–1231. [Google Scholar] [CrossRef]
- Hasson, D.; Arnetz, B.B. Validation and findings comparing VAS vs. likert scales for psychosocial measurements. Int. Electron. J. Health Educ. 2005, 8, 178–192. [Google Scholar]
- Bosetti, M.; Borrone, A.; Follenzi, A.; Messaggio, F.; Tremolada, C.; Cannas, M. Human lipoaspirate as autologous injectable active scaffold for one-step repair of cartilage defects. Cell Transplant. 2016, 25, 1043–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Yu, X.; Yang, Q.; Liu, X.; Fang, J.; Dai, X. Autologous micro-fragmented adipose tissue as stem cell-based natural scaffold for cartilage defect repair. Cell Transplant. 2019, 28, 1709–1720. [Google Scholar] [CrossRef]
- Filardo, G.; Tschon, M.; Perdisa, F.; Brogini, S.; Cavallo, C.; Desando, G.; Giavaresi, G.; Grigolo, B.; Martini, L.; Aldini, N.N.; et al. Micro-fragmentation is a valid alternative to cell expansion and enzymatic digestion of adipose tissue for the treatment of knee osteoarthritis: A comparative preclinical study. Knee Surg. Sports Traumatol. Arthrosc. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, B.; Shaw, I.; Lesme, H.; Yong, L.; Khan, N.; Tremolada, C.; Péault, B. Higher pericyte content and secretory activity of microfragmented human adipose tissue compared to enzymatically derived stromal vascular fraction. Stem Cells Transl. Med. 2018, 7, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Nava, S.; Sordi, V.; Pascucci, L.; Tremolada, C.; Ciusani, E.; Zeira, O.; Cadei, M.; Soldati, G.; Pessina, A.; Parati, E.; et al. Long-lasting anti-inflammatory activity of human microfragmented adipose tissue. Stem Cells Int. 2019, 2019, 1–13. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Age (years) | 54.0 ± 9.0 |
| Gender (F/M) | 105/97 |
| BMI | 26.8 ± 4.2 |
| BMI category (Normal weight/Overweight/Obese) | 70/94/38 |
| Smokers (yes/former/no) | 24/69/109 |
| Diagnosis | |
| Monolateral/Bilateral | 188/14 |
| Treated for OA (yes/no) | 154/48 |
| Kellgren–Lawrence grade (0/1/2/3/4) | 25/80/46/32/19 |
| Comorbidities (yes/no) | 77/125 |
| Hypertension | 46 |
| Thyroid disorders | 23 |
| Diabetes | 10 |
| Arthritis | 7 |
| Cardiovascular disease | 4 |
| Fibromyalgia | 1 |
| Sport | |
| Sport Activity (None/Recreational/Competitive) | 43/154/3 |
| Hours/week sport activity * | 3.53 ± 3.3 |
| Previous and Current Treatments/Surgeries at Baseline | |
| Previous surgeries (yes/no) | 109/93 |
| Previous injections (yes/no) | 97/105 |
| In treatment with painkillers (yes/no) | 74/128 |
| Painkiller administrations per month | 7.0 ± 9.9 |
| In treatment with physical therapy (yes/no) ** | 115/87 |
| Follow-Up | KOOS Pain Score | p Value vs. Baseline |
|---|---|---|
| Baseline | 63.9 (47.2–77.8) | - |
| 6-month | 80.6 (69.4–91.7) | p < 0.001 |
| 12-month | 83.3 (66.7–93.7) | p < 0.001 |
| 24-month | 83.3 (68.7–94.4) | p < 0.001 |
| Change vs. Reference | p Value | Model Covariates | |
|---|---|---|---|
| KOOS | |||
| Thyroid disease | −14.4 ± 4.9 | p = 0.003 | Diabetes, KOOS at baseline |
| Diabetes | −12.5 ± 6.7 | p = 0.064 | Thyroid disease, KOOS at baseline |
| KL grade 4 | −21.05 ± 10.3 | p = 0.043 | KOOS at baseline |
| Previous ACL reconstruction | +10.0 ± 4.0 | p = 0.013 | KOOS at baseline |
| VAS | |||
| Previous PRP injections | −1.83 ± 0.70 | p = 0.010 | VAS at baseline, follow-up time |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Screpis, D.; Natali, S.; Farinelli, L.; Piovan, G.; Iacono, V.; de Girolamo, L.; Viganò, M.; Zorzi, C. Autologous Microfragmented Adipose Tissue for the Treatment of Knee Osteoarthritis: Real-World Data at Two Years Follow-Up. J. Clin. Med. 2022, 11, 1268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051268
Screpis D, Natali S, Farinelli L, Piovan G, Iacono V, de Girolamo L, Viganò M, Zorzi C. Autologous Microfragmented Adipose Tissue for the Treatment of Knee Osteoarthritis: Real-World Data at Two Years Follow-Up. Journal of Clinical Medicine. 2022; 11(5):1268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051268
Chicago/Turabian StyleScrepis, Daniele, Simone Natali, Luca Farinelli, Gianluca Piovan, Venanzio Iacono, Laura de Girolamo, Marco Viganò, and Claudio Zorzi. 2022. "Autologous Microfragmented Adipose Tissue for the Treatment of Knee Osteoarthritis: Real-World Data at Two Years Follow-Up" Journal of Clinical Medicine 11, no. 5: 1268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051268