
Long-Term Outcomes of a Kahook Dual Blade Procedure Combined with Phacoemulsification in Japanese Patients with Open-Angle Glaucoma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Technique
2.3. Postoperative Care and Data Collection
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Demographic and Clinical Characteristics
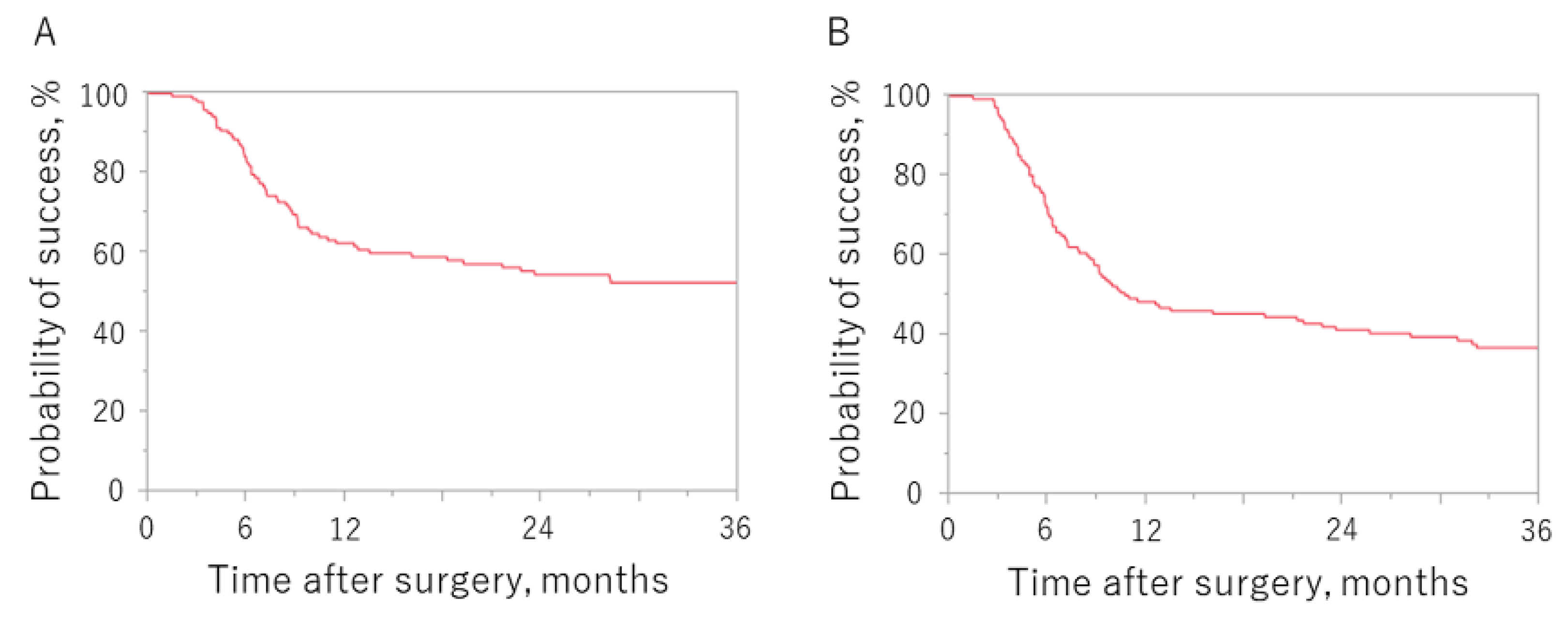
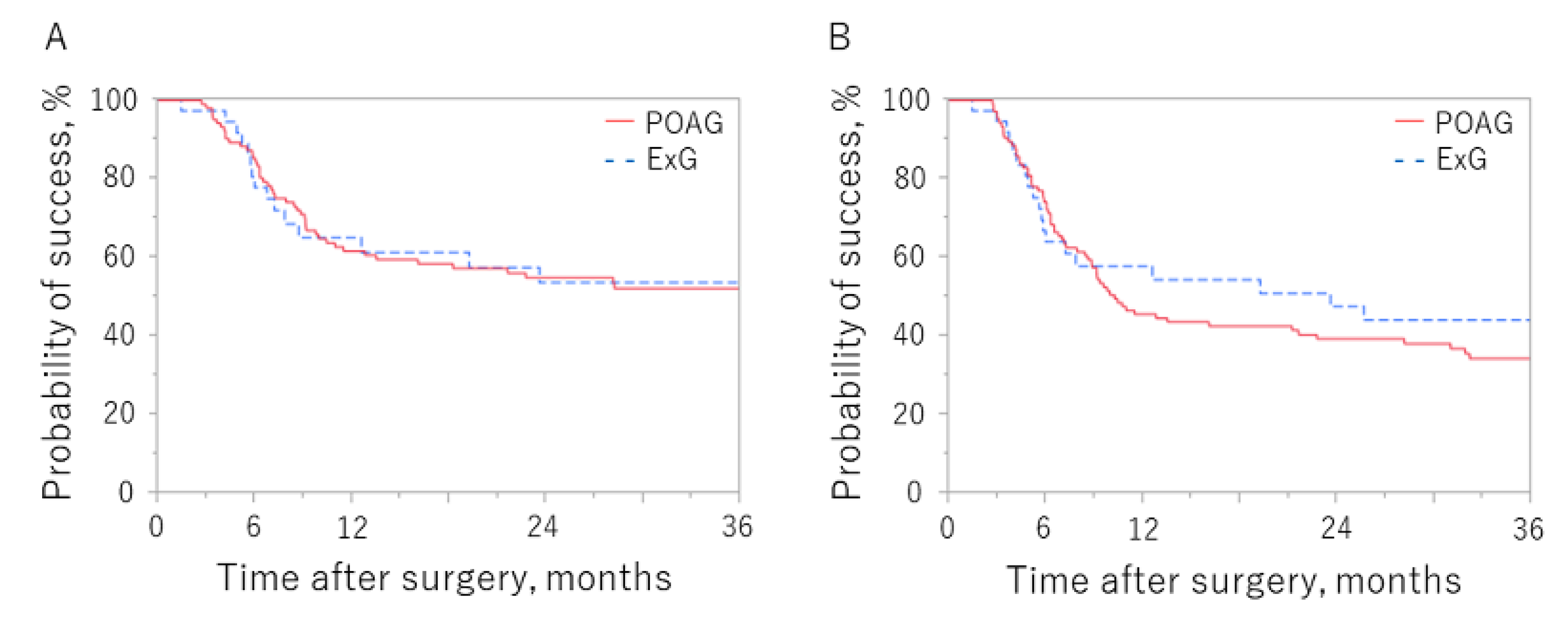
3.2. Primary Outcome
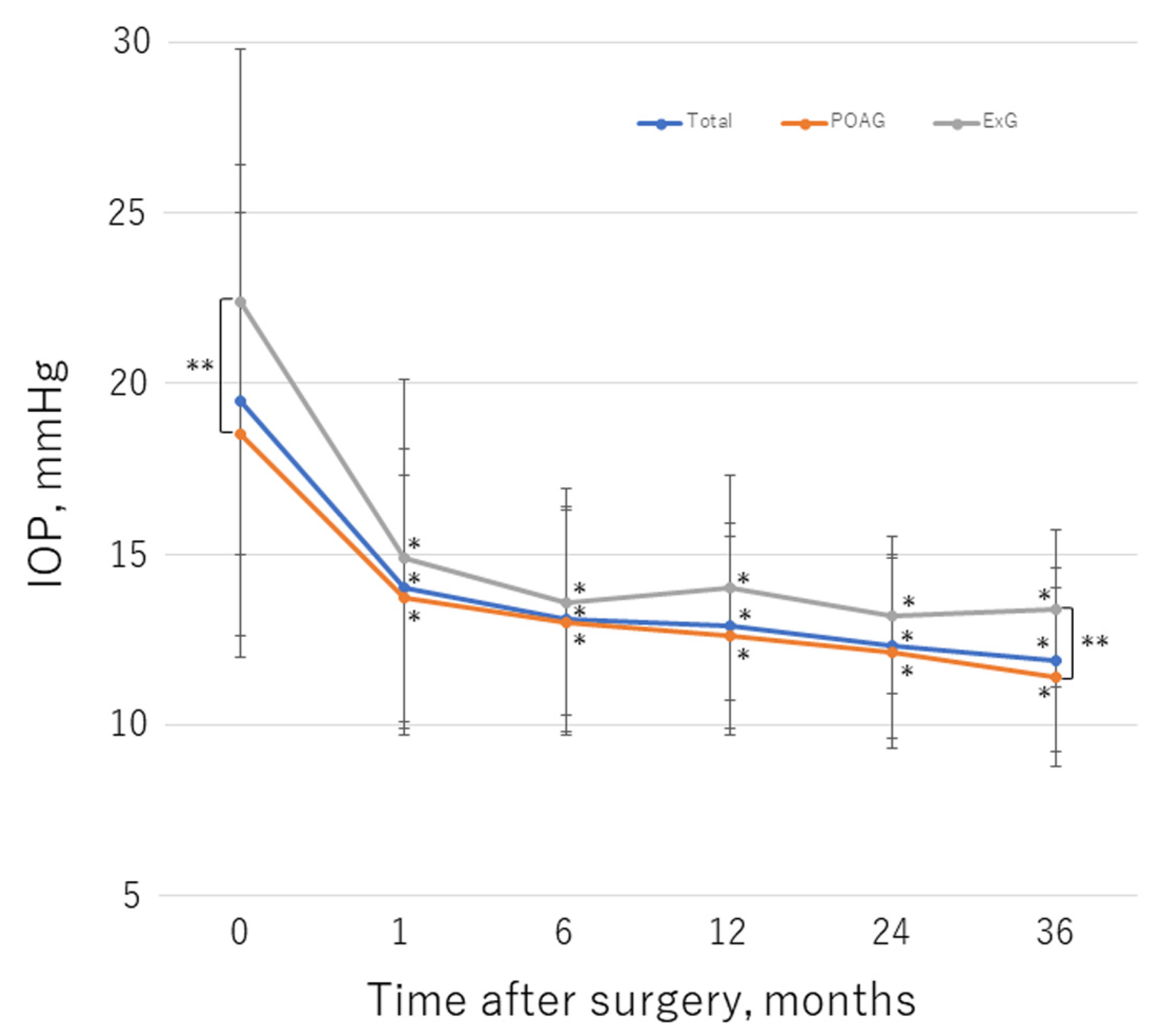
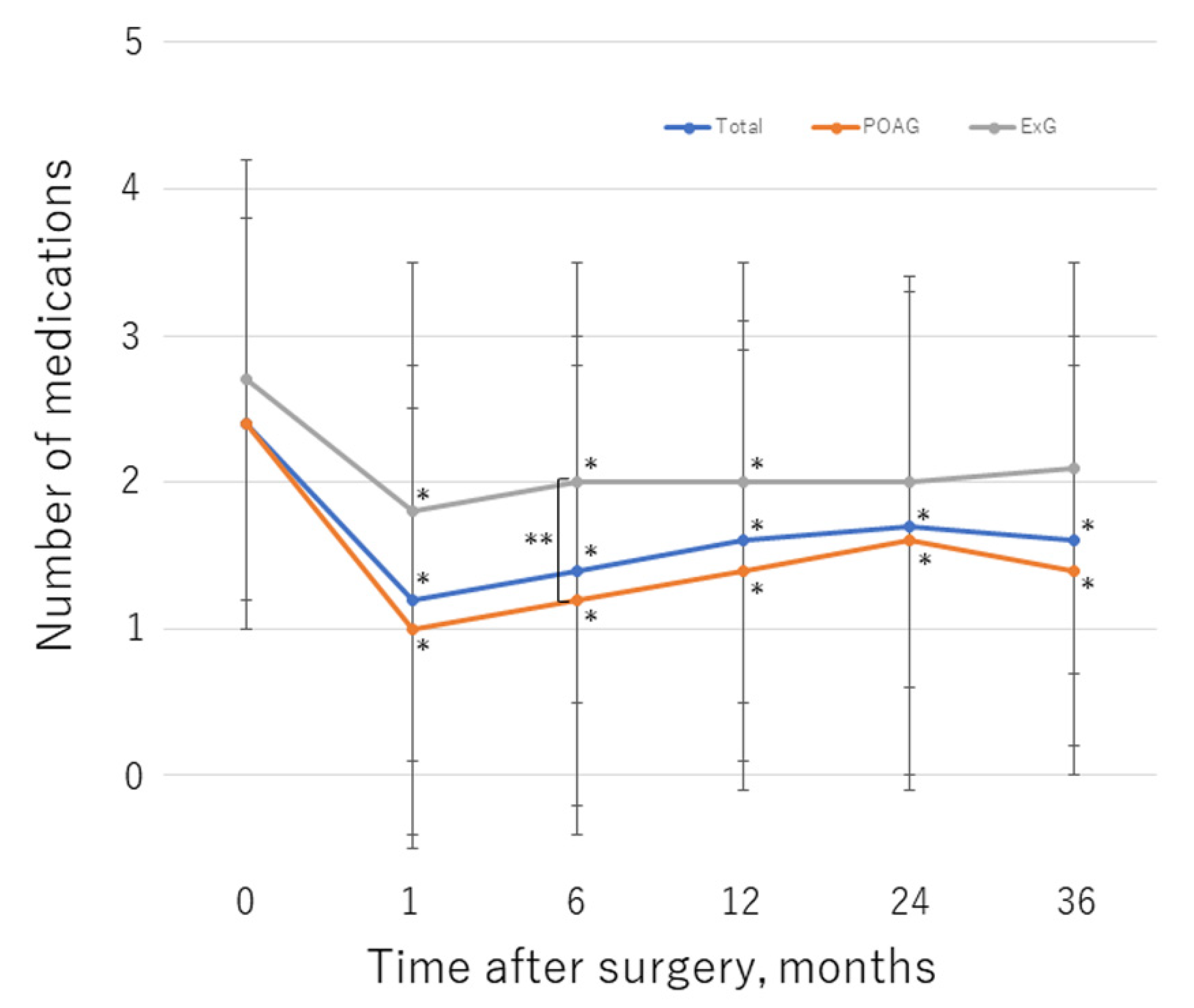
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tanihara, H.; Negi, A.; Akimoto, M.; Terauchi, H.; Okudaira, A.; Kozaki, J.; Takeuchi, A.; Nagata, M. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch. Ophthalmol. 1993, 111, 1653–1661. [Google Scholar] [CrossRef]
- Chihara, E.; Nishida, A.; Kodo, M.; Yoshimura, N.; Matsumura, M.; Yamamoto, M.; Tsukada, T. Trabeculotomy ab externo: An alternative treatment in adult patients with primary open-angle glaucoma. Ophthalmic. Surg. 1993, 24, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Iwao, K.; Inatani, M.; Tanihara, H. Success rates of trabeculotomy for steroid-induced glaucoma: A comparative, multicenter, retrospective cohort study. Am. J. Ophthalmol. 2011, 151, 1047–1056.e1. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Ishigooka, H.; Muto, T.; Tanihara, H.; Nagata, M. Long-term outcome of trabeculotomy for the treatment of developmental glaucoma. Arch. Ophthalmol. 2004, 122, 1122–1128. [Google Scholar] [CrossRef] [Green Version]
- Honjo, M.; Tanihara, H.; Negi, A.; Hangai, M.; Taniguchi, T.; Honda, Y.; Mizoguchi, T.; Matsumura, M.; Nagata, M. Trabeculotomy ab externo, cataract extraction, and intraocular lens implantation: Preliminary report. J. Cataract Refract. Surg. 1996, 22, 601–606. [Google Scholar] [CrossRef]
- Tanito, M.; Ohira, A.; Chihara, E. Surgical outcome of combined trabeculotomy and cataract surgery. J. Glaucoma 2001, 10, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Broadway, D.C.; Grierson, I.; Hitchings, R.A. Local effects of previous conjunctival incisional surgery and the subsequent outcome of filtration surgery. Am. J. Ophthalmol. 1998, 125, 805–818. [Google Scholar] [CrossRef]
- Broadway, D.C.; Chang, L.P. Trabeculectomy, risk factors for failure and the preoperative state of the conjunctiva. J. Glaucoma. 2001, 10, 237–249. [Google Scholar] [CrossRef]
- Iwao, K.; Inatani, M.; Ogata-Iwao, M.; Takihara, Y.; Tanihara, H. Restricted post-trabeculectomy bleb formation by conjunctival scarring. Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1095–1101. [Google Scholar] [CrossRef]
- Iwasaki, K.; Arimura, S.; Takamura, Y.; Inatani, M. Clinical practice preferences for glaucoma surgery in Japan: A survey of Japan Glaucoma Society specialists. Jpn. J. Ophthalmol. 2020, 64, 385–391. [Google Scholar] [CrossRef]
- Richter, G.M.; Coleman, A.L. Minimally invasive glaucoma surgery: Current status and future prospects. Clin. Ophthalmol. 2016, 10, 189–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yook, E.; Vinod, K.; Panarelli, J.F. Complications of micro-invasive glaucoma surgery. Curr. Opin. Ophthalmol. 2018, 29, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Rosdahl, J.A.; Gupta, D. Prospective studies of minimally invasive glaucoma surgeries: Systematic review and quality assessment. Clin. Ophthalmol. 2020, 14, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seibold, L.K.; SooHoo, J.R.; Ammar, D.A.; Kahook, M.Y. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. Am. J. Ophthalmol. 2013, 155, 524–529.e2. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, K.; Takamura, Y.; Orii, Y.; Arimura, S.; Inatani, M. Performances of glaucoma operations with Kahook Dual Blade or iStent combined with phacoemulsification in Japanese open angle glaucoma patients. Int. J. Ophthalmol. 2020, 13, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, M.D.; Seibold, L.K.; Radcliffe, N.M.; Dorairaj, S.K.; Aref, A.A.; Román, J.J.; Lazcano-Gomez, G.S.; Darlington, J.K.; Abdullah, S.; Jasek, M.C. Goniotomy with a single-use dual blade: Short-term results. J. Cataract Refract. Surg. 2017, 43, 1197–1201. [Google Scholar] [CrossRef]
- Dorairaj, S.K.; Seibold, L.K.; Radcliffe, N.M.; Aref, A.A.; Jimenez-Román, J.; Lazcano-Gomez, G.S.; Darlington, J.K.; Mansouri, K.; Berdahl, J.P. 12-month outcomes of goniotomy performed using the kahook dual blade combined with cataract surgery in eyes with medically treated glaucoma. Adv. Ther. 2018, 35, 1460–1469. [Google Scholar] [CrossRef] [Green Version]
- Hirabayashi, M.T.; King, J.T.; Lee, D.; An, J.A. Outcome of phacoemulsification combined with excisional goniotomy using the Kahook Dual Blade in severe glaucoma patients at 6 months. Clin. Ophthalmol. 2019, 13, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Ansari, E.; Loganathan, D. 12-month clinical outcomes of combined phacoemulsification and ab interno trabeculectomy for open-angle glaucoma in the United Kingdom. PLoS ONE 2021, 16, e0252826. [Google Scholar] [CrossRef]
- Dorairaj, S.K.; Kahook, M.Y.; Williamson, B.K.; Seibold, L.K.; ElMallah, M.K.; Singh, I.P. A multicenter retrospective comparison of goniotomy versus trabecular bypass device implantation in glaucoma patients undergoing cataract extraction. Clin. Ophthalmol. 2018, 12, 791–797. [Google Scholar] [CrossRef] [Green Version]
- ElMallah, M.K.; Seibold, L.K.; Kahook, M.Y.; Williamson, B.K.; Singh, I.P.; Dorairaj, S.K.; KDB Goniotomy Study Group. 12-month retrospective comparison of Kahook Dual Blade excisional goniotomy with istent trabecular bypass device implantation in glaucomatous eyes at the time of cataract surgery. Adv. Ther. 2019, 36, 2515–2527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falkenberry, S.; Singh, I.P.; Crane, C.J.; Haider, M.A.; Morgan, M.G.; Grenier, C.P.; Brubaker, J.W.; Balasubramani, G.K.; Dorairaj, S. Excisional goniotomy vs trabecular microbypass stent implantation: A prospective randomized clinical trial in eyes with mild to moderate open-angle glaucoma. J. Cataract Refract. Surg. 2020, 46, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Al Habash, A.; Albuainain, A. Long term outcome of combined phacoemulsification and excisional goniotomy with the Kahook Dual Blade in different subtypes of glaucoma. Sci. Rep. 2021, 11, 10660. [Google Scholar] [CrossRef] [PubMed]
- Omoto, T.; Sugiura, A.; Fujishiro, T.; Asano-Shimizu, K.; Sugimoto, K.; Sakata, R.; Murata, H.; Asaoka, R.; Honjo, M.; Aihara, M. Twelve-month surgical outcome and prognostic factors of stand-alone ab interno trabeculotomy in Japanese patients with open-angle glaucoma. PLoS ONE 2021, 16, e0245015. [Google Scholar] [CrossRef] [PubMed]
- Wakil, S.M.; Birnbaum, F.; Vu, D.M.; McBurney-Lin, S.; ElMallah, M.K.; Tseng, H. Efficacy and safety of a single-use dual blade goniotomy: 18-month results. J. Cataract Refract. Surg. 2020, 46, 1408–1415. [Google Scholar] [CrossRef]
- Takihara, Y.; Inatani, M.; Fukushima, M.; Iwao, K.; Iwao, M.; Tanihara, H. Trabeculectomy with mitomycin C for neovascular glaucoma: Prognostic factors for surgical failure. Am. J. Ophthalmol. 2009, 147, 912–918. [Google Scholar] [CrossRef]
- Sieck, E.G.; Epstein, R.S.; Kennedy, J.B.; SooHoo, J.R.; Pantcheva, M.B.; Patnaik, J.L.; Wagner, B.D.; Lynch, A.M.; Kahook, M.Y.; Seibold, L.K. Outcomes of Kahook Dual Blade goniotomy with and without phacoemulsification cataract extraction. Ophthalmol. Glaucoma 2018, 1, 75–81. [Google Scholar] [CrossRef]
- Salinas, L.; Chaudhary, A.; Berdahl, J.P.; Lazcano-Gomez, G.S.; Williamson, B.K.; Dorairaj, S.K.; Seibold, L.K.; Smith, S.; Aref, A.A.; Darlington, J.K.; et al. Goniotomy using the Kahook Dual Blade in severe and refractory glaucoma: 6-month outcomes. J. Glaucoma 2018, 27, 849–855. [Google Scholar] [CrossRef]
- Ong, A.Y.; Shalchi, Z. Outcomes of cataract surgery in pseudoexfoliation syndrome in England: 10-year retrospective cohort study. J. Cataract Refract. Surg. 2021, 47, 165–171. [Google Scholar] [CrossRef]
- Vesti, E.; Kivela, T. Exfoliation syndrome and exfoliation glaucoma. Prog. Retin. Eye Res. 2000, 19, 345–368. [Google Scholar] [CrossRef]
- Topouzis, F.; Harris, A.; Wilson, M.R.; Koskosas, A.; Founti, P.; Yu, F.; Anastasopoulos, E.; Pappas, T.; Coleman, A.L. Increased likelihood of glaucoma at the same screening intraocular pressure in subjects with pseudoexfoliation: The Thessaloniki Eye Study. Am. J. Ophthalmol. 2009, 148, 606–613.e1. [Google Scholar] [CrossRef]
- Jea, S.Y.; Francis, B.A.; Vakili, G.; Filippopoulos, T.; Rhee, D.J. Ab interno trabeculectomy versus trabeculectomy for open-angle glaucoma. Ophthalmology 2012, 119, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, M.; Shoji, N. Effectiveness and limitations of minimally invasive glaucoma surgery targeting Schlemm’s canal. Jpn. J. Ophthalmol. 2021, 65, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Kawaji, T.; Inatani, M.; Kameda, T.; Yoshimura, N.; Tanihara, H. Simultaneous increases in multiple proinflammatory cytokines in the aqueous humor in pseudophakic glaucomatous eyes. J. Cataract Refract. Surg. 2012, 38, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.L.; Wong, E.Y.M.; Walton, D.S. Goniosurgery for glaucoma complicating chronic childhood uveitis. Arch. Ophthalmol. 2004, 122, 838–844. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | POAG | ExG | p-Value | |
|---|---|---|---|---|
| Eyes, n | 148 | 110 | 38 | |
| Age (years) | 76.9 ± 7.2 | 76.1 ± 7.4 | 79.0 ± 6.2 | 0.08 |
| Sex, n (%) | 0.09 | |||
| Male | 71 (48) | 48 (44) | 23 (61) | |
| Female | 77 (52) | 62 (56) | 15 (39) | |
| Glaucoma type, n (%) | NA | |||
| POAG | 110 (74) | NA | NA | |
| ExG | 38 (26) | NA | NA | |
| Severity, n (%) | 0.24 | |||
| Mild | 36 (24) | 29 (26) | 7 (18) | |
| Moderate | 28 (19) | 23 (21) | 5 (13) | |
| Severe | 84 (57) | 58 (53) | 26 (69) | |
| BCVA (logMAR) | 0.53 ± 0.46 | 0.56 ± 051 | 0.44 ± 0.27 | 0.42 |
| Spherical equivalent (diopters) | −2.6 ± 5.3 | −3.0 ± 5.8 | −1.6 ± 3.3 | 0.57 |
| Axial length (mm) | 24.0 ± 2.1 | 24.1 ± 2.2 | 23.8 ± 1.7 | 0.54 |
| Visual field MD (dB) | −14.9 ± 9.3 | −14.3 ± 9.3 | −16.8 ± 9.4 | 0.17 |
| Total | POAG | ExG | p-Value | |
|---|---|---|---|---|
| Preoperative | ||||
| IOP (mmHg) | 19.5 ± 6.9 | 18.5 ± 6.5 | 22.4 ± 7.4 | <0.01 |
| Medications, n | 2.4 ± 1.4 | 2.4 ± 1.4 | 2.7 ± 1.5 | >0.99 |
| Eyes, n | 148 | 110 | 38 | |
| 1 month | ||||
| IOP (mmHg) | 14.0 ± 4.1 | 13.7 ± 3.6 | 14.9 ± 5.2 | >0.99 |
| Medications, n | 1.2 ± 1.6 | 1.0 ± 1.5 | 1.8 ± 1.7 | 0.052 |
| Eyes, n | 148 | 110 | 38 | |
| 6 months | ||||
| IOP (mmHg) | 13.1 ± 3.3 | 13.0 ± 3.3 | 13.6 ± 3.3 | >0.99 |
| Medications, n | 1.4 ± 1.6 | 1.2 ± 1.6 | 2.0 ± 1.5 | 0.039 |
| Eyes, n | 138 | 102 | 36 | |
| 12 months | ||||
| IOP (mmHg) | 12.9 ± 3.0 | 12.6 ± 2.9 | 14.0 ± 3.3 | 0.39 |
| Medications, n | 1.6 ± 1.5 | 1.4 ± 1.5 | 2.0 ± 1.5 | 0.50 |
| Eyes, n | 122 | 94 | 28 | |
| 24 months | ||||
| IOP (mmHg) | 12.3 ± 2.7 | 12.1 ± 2.8 | 13.2 ± 2.3 | 0.71 |
| Medications, n | 1.7 ± 1.7 | 1.6 ± 1.7 | 2.0 ± 1.4 | >0.99 |
| Eyes, n | 109 | 86 | 23 | |
| 36 months | ||||
| IOP (mmHg) | 11.9 ± 2.7 | 11.4 ± 2.6 | 13.4 ± 2.3 | 0.014 |
| Medications, n | 1.6 ± 1.4 | 1.4 ± 1.4 | 2.1 ± 1.4 | 0.28 |
| Eyes, n | 93 | 70 | 23 | |
| IOP reduction in baseline at 36 months (%) | 28.0 ± 20.8 | 28.7 ± 20.1 | 26.0 ± 23.3 | 0.47 |
| IOP reduction ≥20% in baseline at final visit, n (%) | 105 (71) | 81 (74) | 24 (63) | 0.22 |
| Medication-free at 12 months, n (%) | 47 (39) | 41 (44) | 6 (21) | 0.046 |
| Medication-free at 24 months, n (%) | 39 (36) | 35 (41) | 4 (17) | 0.051 |
| Medication-free at 36 months, n (%) | 32 (34) | 28 (40) | 4 (17) | 0.075 |
| Using ≥1 fewer medications from baseline at final visit, n (%) | 83 (56) | 67 (61) | 16 (42) | 0.058 |
| n (%) | Total | POAG | ExG | p-Value |
|---|---|---|---|---|
| Hyphema | 21 (14.2) | 15 (13.6) | 6 (15.8) | 0.79 |
| IOP spikes | 19 (12.8) | 10 (9.1) | 9 (23.7) | 0.045 |
| Additional glaucoma surgery | 6 (4.1) | 2 (1.8) | 4 (10.5) | 0.038 |
| Criterion | ||||
|---|---|---|---|---|
| A | B | |||
| RR (95% CI) | p-Value | RR (95% CI) | p-Value | |
| Sex (Male/Female) | 0.93 (0.52–1.65) | 0.81 | 0.86 (0.53–1.39) | 0.55 |
| Age per year | 0.97 (0.93–1.01) | 0.13 | 0.97 (0.94–1.00) | 0.08 |
| Axial length per mm | 1.04 (0.89–1.19) | 0.63 | 1.04 (0.92–1.16) | 0.54 |
| Visual field MD per dB | 0.99 (0.96–1.03) | 0.7 | 0.98 (0.96–1.01) | 0.23 |
| Glaucoma type (POAG/ExG) | 0.74 (0.39–1.48) | 0.38 | 1.32 (0.76–2.37) | 0.33 |
| Preoperative IOP per mmHg | 0.89 (0.83–0.95) | <0.01 | 1.02 (0.98–1.06) | 0.31 |
| Preoperative glaucoma medication per each | 1.04 (0.85–1.27) | 0.72 | 1.05 (0.89–1.24) | 0.57 |
| IOP spikes | 1.41 (0.64–2.87) | 0.38 | 1.46 (0.73–2.71) | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwasaki, K.; Kakimoto, H.; Orii, Y.; Arimura, S.; Takamura, Y.; Inatani, M. Long-Term Outcomes of a Kahook Dual Blade Procedure Combined with Phacoemulsification in Japanese Patients with Open-Angle Glaucoma. J. Clin. Med. 2022, 11, 1354. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051354
Iwasaki K, Kakimoto H, Orii Y, Arimura S, Takamura Y, Inatani M. Long-Term Outcomes of a Kahook Dual Blade Procedure Combined with Phacoemulsification in Japanese Patients with Open-Angle Glaucoma. Journal of Clinical Medicine. 2022; 11(5):1354. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051354
Chicago/Turabian StyleIwasaki, Kentaro, Hiroshi Kakimoto, Yusuke Orii, Shogo Arimura, Yoshihiro Takamura, and Masaru Inatani. 2022. "Long-Term Outcomes of a Kahook Dual Blade Procedure Combined with Phacoemulsification in Japanese Patients with Open-Angle Glaucoma" Journal of Clinical Medicine 11, no. 5: 1354. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051354