
The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus

 , , and
, , and
Abstract
:1. Introduction
2. Epidemiology
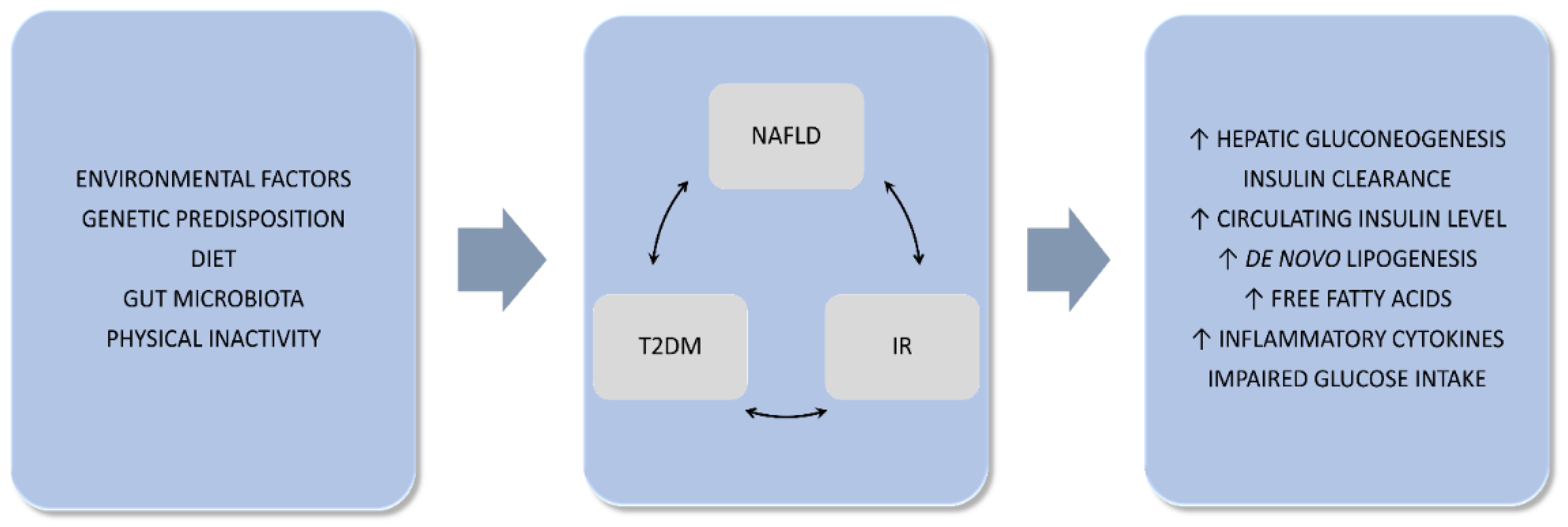
3. Common Pathogenesis
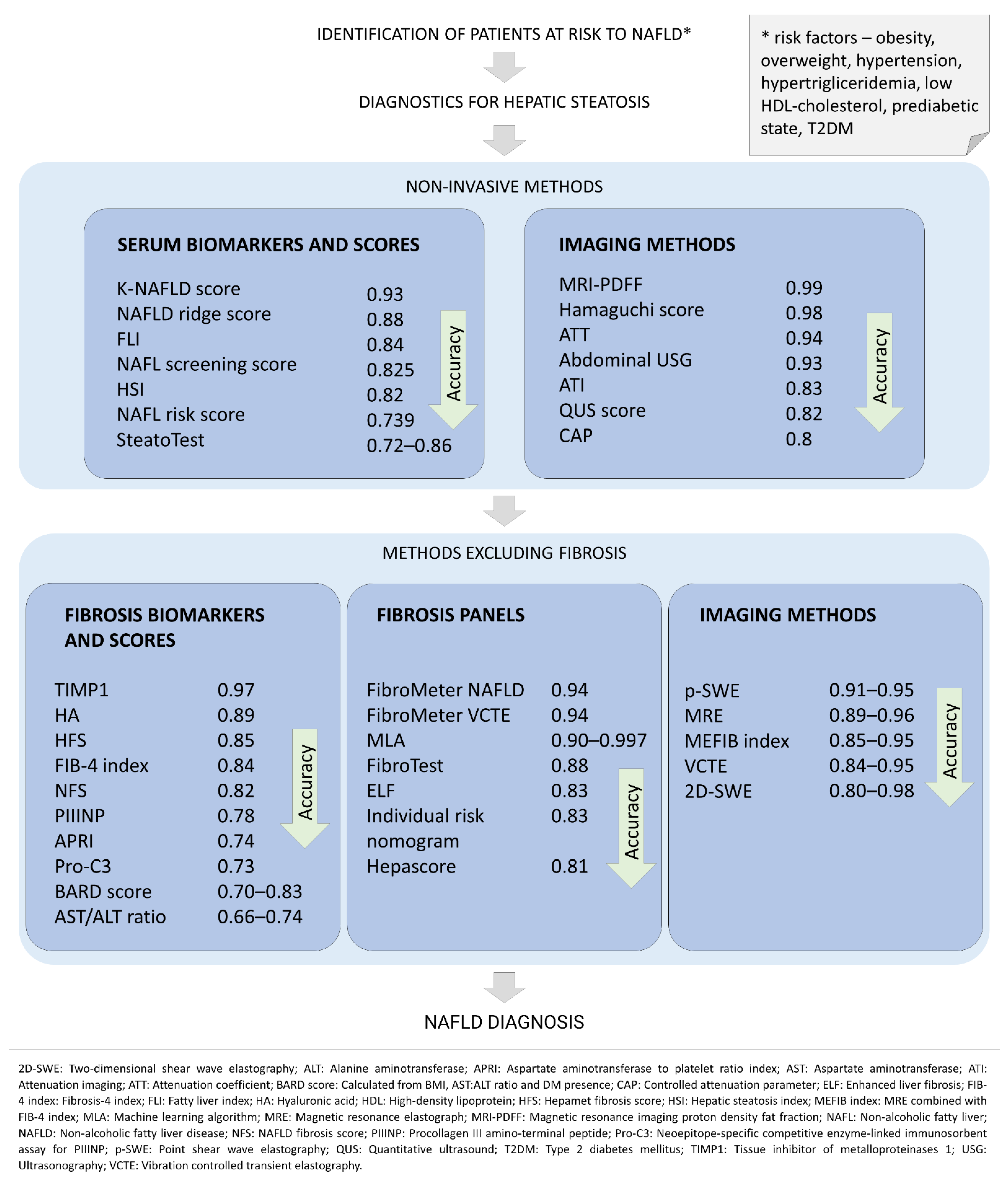
4. Diagnosis
5. Complications
6. NAFLD Pharmacotherapy with Hypoglycemic Agents
6.1. Metformin
6.2. Thiazolidinediones (TZDs)
6.3. GLP-1 Agonists and DPP-4 Inhibitors
6.4. Others
7. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thaler, H. The fatty liver and its pathogenetic relation to liver cirrhosis. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 1962, 335, 180–210. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD Diagnostic Criteria in Real World. Liver Int. Off. J. Int. Assoc. Study Liver 2020, 40, 2082–2089. [Google Scholar] [CrossRef]
- Marchesini, G.; Brizi, M.; Morselli-Labate, A.M.; Bianchi, G.; Bugianesi, E.; McCullough, A.J.; Forlani, G.; Melchionda, N. Association of Nonalcoholic Fatty Liver Disease with Insulin Resistance. Am. J. Med. 1999, 107, 450–455. [Google Scholar] [CrossRef]
- Liebe, R.; Esposito, I.; Bock, H.H.; Vom Dahl, S.; Stindt, J.; Baumann, U.; Luedde, T.; Keitel, V. Diagnosis and Management of Secondary Causes of Steatohepatitis. J. Hepatol. 2021, 74, 1455–1471. [Google Scholar] [CrossRef] [PubMed]
- Kneeman, J.M.; Misdraji, J.; Corey, K.E. Secondary Causes of Nonalcoholic Fatty Liver Disease. Ther. Adv. Gastroenterol. 2012, 5, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Kim, W.R.; Kim, H.J.; Therneau, T.M. Association between Noninvasive Fibrosis Markers and Mortality among Adults with Nonalcoholic Fatty Liver Disease in the United States. Hepatology 2013, 57, 1357–1365. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Adams, L.A.; Canbay, A.; Syn, W.-K. Extrahepatic Complications of Nonalcoholic Fatty Liver Disease. Hepatology 2014, 59, 1174–1197. [Google Scholar] [CrossRef]
- Kasturiratne, A.; Weerasinghe, S.; Dassanayake, A.S.; Rajindrajith, S.; de Silva, A.P.; Kato, N.; Wickremasinghe, A.R.; de Silva, H.J. Influence of Non-Alcoholic Fatty Liver Disease on the Development of Diabetes Mellitus. J. Gastroenterol. Hepatol. 2013, 28, 142–147. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Tran, T.; Everhart, J.E. Diabetes Increases the Risk of Chronic Liver Disease and Hepatocellular Carcinoma. Gastroenterology 2004, 126, 460–468. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Rodella, S.; Tessari, R.; Zenari, L.; Lippi, G.; Arcaro, G. Nonalcoholic Fatty Liver Disease Is Independently Associated with an Increased Incidence of Cardiovascular Events in Type 2 Diabetic Patients. Diabetes Care 2007, 30, 2119–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leite, N.C.; Villela-Nogueira, C.A.; Pannain, V.L.N.; Bottino, A.C.; Rezende, G.F.M.; Cardoso, C.R.L.; Salles, G.F. Histopathological Stages of Nonalcoholic Fatty Liver Disease in Type 2 Diabetes: Prevalences and Correlated Factors. Liver Int. Off. J. Int. Assoc. Study Liver 2011, 31, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sanyal, A.J. The Global NAFLD Epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef]
- Bambha, K.; Belt, P.; Abraham, M.; Wilson, L.A.; Pabst, M.; Ferrell, L.; Unalp-Arida, A.; Bass, N. Ethnicity and Nonalcoholic Fatty Liver Disease. Hepatology 2012, 55, 769–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazo, M.; Clark, J.M. The Epidemiology of Nonalcoholic Fatty Liver Disease: A Global Perspective. Semin. Liver Dis. 2008, 28, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Vilgrain, V.; Angulo, P. Noninvasive Evaluation of NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 666–675. [Google Scholar] [CrossRef]
- Mitra, S.; De, A.; Chowdhury, A. Epidemiology of Non-Alcoholic and Alcoholic Fatty Liver Diseases. Transl. Gastroenterol. Hepatol. 2020, 5, 16. [Google Scholar] [CrossRef]
- Chen, Y.-Y.; Yeh, M.M. Non-Alcoholic Fatty Liver Disease: A Review with Clinical and Pathological Correlation. J. Formos. Med. Assoc. 2021, 120, 68–77. [Google Scholar] [CrossRef]
- Dufour, J.-F.; Scherer, R.; Balp, M.-M.; McKenna, S.J.; Janssens, N.; Lopez, P.; Pedrosa, M. The Global Epidemiology of Nonalcoholic Steatohepatitis (NASH) and Associated Risk Factors—A Targeted Literature Review. Endocr. Metab. Sci. 2021, 3, 100089. [Google Scholar] [CrossRef]
- Wong, R.J.; Liu, B.; Bhuket, T. Significant Burden of Nonalcoholic Fatty Liver Disease with Advanced Fibrosis in the US: A Cross-Sectional Analysis of 2011–2014 National Health and Nutrition Examination Survey. Aliment. Pharmacol. Ther. 2017, 46, 974–980. [Google Scholar] [CrossRef] [Green Version]
- Rinella, M.; Charlton, M. The Globalization of Nonalcoholic Fatty Liver Disease: Prevalence and Impact on World Health. Hepatology 2016, 64, 19–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazo, M.; Hernaez, R.; Eberhardt, M.S.; Bonekamp, S.; Kamel, I.; Guallar, E.; Koteish, A.; Brancati, F.L.; Clark, J.M. Prevalence of Nonalcoholic Fatty Liver Disease in the United States: The Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Epidemiol. 2013, 178, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Schouten, J.N.L.; Hansen, B.E.; van Rooij, F.J.A.; Hofman, A.; Stricker, B.H.; Janssen, H.L.A. Prevalence and Risk Factors of Non-Alcoholic Fatty Liver Disease in the Elderly: Results from the Rotterdam Study. J. Hepatol. 2012, 57, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, J.-H.; Choi, J.-M.; Moon, S.Y.; Suh, Y.J.; Shin, J.-Y.; Shin, H.C.; Park, S.K. The Clinical Availability of Non Alcoholic Fatty Liver Disease as an Early Predictor of the Metabolic Syndrome in Korean Men: 5-Year’s Prospective Cohort Study. Atherosclerosis 2013, 227, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Yasutake, K.; Kohjima, M.; Kotoh, K.; Nakashima, M.; Nakamuta, M.; Enjoji, M. Dietary Habits and Behaviors Associated with Nonalcoholic Fatty Liver Disease. World J. Gastroenterol. 2014, 20, 1756–1767. [Google Scholar] [CrossRef]
- Zeb, I.; Katz, R.; Nasir, K.; Ding, J.; Rezaeian, P.; Budoff, M.J. Relation of Nonalcoholic Fatty Liver Disease to the Metabolic Syndrome: The Multi-Ethnic Study of Atherosclerosis. J. Cardiovasc. Comput. Tomogr. 2013, 7, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Paschos, P.; Paletas, K. Non Alcoholic Fatty Liver Disease and Metabolic Syndrome. Hippokratia 2009, 13, 9–19. [Google Scholar]
- Kotronen, A.; Westerbacka, J.; Bergholm, R.; Pietiläinen, K.H.; Yki-Järvinen, H. Liver Fat in the Metabolic Syndrome. J. Clin. Endocrinol. Metab. 2007, 92, 3490–3497. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Takeda, N.; Nakagawa, T.; Taniguchi, H.; Fujii, K.; Omatsu, T.; Nakajima, T.; Sarui, H.; Shimazaki, M.; et al. The Metabolic Syndrome as a Predictor of Nonalcoholic Fatty Liver Disease. Ann. Intern. Med. 2005, 143, 722–728. [Google Scholar] [CrossRef]
- Moretto, M.; Kupski, C.; Mottin, C.C.; Repetto, G.; Garcia Toneto, M.; Rizzolli, J.; Berleze, D.; de Souza Brito, C.L.; Casagrande, D.; Colossi, F. Hepatic Steatosis in Patients Undergoing Bariatric Surgery and Its Relationship to Body Mass Index and Co-Morbidities. Obes. Surg. 2003, 13, 622–624. [Google Scholar] [CrossRef]
- Basaranoglu, M.; Neuschwander-Tetri, B.A. Nonalcoholic Fatty Liver Disease: Clinical Features and Pathogenesis. Gastroenterol. Hepatol. 2006, 2, 282–291. [Google Scholar]
- Van Vliet-Ostaptchouk, J.V.; Nuotio, M.-L.; Slagter, S.N.; Doiron, D.; Fischer, K.; Foco, L.; Gaye, A.; Gögele, M.; Heier, M.; Hiekkalinna, T.; et al. The Prevalence of Metabolic Syndrome and Metabolically Healthy Obesity in Europe: A Collaborative Analysis of Ten Large Cohort Studies. BMC Endocr. Disord. 2014, 14, 9. [Google Scholar] [CrossRef] [Green Version]
- Kopylov, U.; Ben-Horin, S.; Lahat, A.; Segev, S.; Avidan, B.; Carter, D. Obesity, Metabolic Syndrome and the Risk of Development of Colonic Diverticulosis. Digestion 2012, 86, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Li, J.; Ying, M.; Wei, F.; Xie, X. Diabetes Increases Morbidities of Colonic Diverticular Disease and Colonic Diverticular Hemorrhage: A Systematic Review and Meta-Analysis. Am. J. Ther. 2017, 24, e213–e221. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Falchuk, K.R. Diverticulosis and Diverticulitis. Mayo Clin. Proc. 2016, 91, 1094–1104. [Google Scholar] [CrossRef]
- Pantic, I.; Lugonja, S.; Rajovic, N.; Dumic, I.; Milovanovic, T. Colonic Diverticulosis and Non-Alcoholic Fatty Liver Disease: Is There a Connection? Medicina 2021, 58, 38. [Google Scholar] [CrossRef]
- Milovanovic, T.; Pantic, I.; Dragasevic, S.; Lugonja, S.; Dumic, I.; Rajilic-Stojanovic, M. The Interrelationship Among Non-Alcoholic Fatty Liver Disease, Colonic Diverticulosis and Metabolic Syndrome. J. Gastrointestin. Liver Dis. 2021, 30, 274–282. [Google Scholar] [CrossRef]
- Wah-Kheong, C.; Khean-Lee, G. Epidemiology of a Fast Emerging Disease in the Asia-Pacific Region: Non-Alcoholic Fatty Liver Disease. Hepatol. Int. 2013, 7, 65–71. [Google Scholar] [CrossRef]
- Kwon, Y.-M.; Oh, S.-W.; Hwang, S.; Lee, C.; Kwon, H.; Chung, G.E. Association of Nonalcoholic Fatty Liver Disease with Components of Metabolic Syndrome According to Body Mass Index in Korean Adults. Am. J. Gastroenterol. 2012, 107, 1852–1858. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Yeung, D.K.-W.; Lau, T.K.-T.; Chan, C.K.-M.; Chim, A.M.-L.; Abrigo, J.M.; Chan, R.S.-M.; Woo, J.; Tse, Y.-K.; et al. Incidence of Non-Alcoholic Fatty Liver Disease in Hong Kong: A Population Study with Paired Proton-Magnetic Resonance Spectroscopy. J. Hepatol. 2015, 62, 182–189. [Google Scholar] [CrossRef]
- Kalra, S.; Vithalani, M.; Gulati, G.; Kulkarni, C.M.; Kadam, Y.; Pallivathukkal, J.; Das, B.; Sahay, R.; Modi, K.D. Study of Prevalence of Nonalcoholic Fatty Liver Disease (NAFLD) in Type 2 Diabetes Patients in India (SPRINT). J. Assoc. Physicians India 2013, 61, 448–453. [Google Scholar] [PubMed]
- Ortiz-Lopez, C.; Lomonaco, R.; Orsak, B.; Finch, J.; Chang, Z.; Kochunov, V.G.; Hardies, J.; Cusi, K. Prevalence of Prediabetes and Diabetes and Metabolic Profile of Patients with Nonalcoholic Fatty Liver Disease (NAFLD). Diabetes Care 2012, 35, 873–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blachier, M.; Leleu, H.; Peck-Radosavljevic, M.; Valla, D.-C.; Roudot-Thoraval, F. The Burden of Liver Disease in Europe: A Review of Available Epidemiological Data. J. Hepatol. 2013, 58, 593–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Seo, M.H.; Shin, H.C.; Ryoo, J.-H. Clinical Availability of Nonalcoholic Fatty Liver Disease as an Early Predictor of Type 2 Diabetes Mellitus in Korean Men: 5-Year Prospective Cohort Study. Hepatology 2013, 57, 1378–1383. [Google Scholar] [CrossRef]
- Kosmalski, M.; Kasznicki, J.; Drzewoski, J. Relationship between Ultrasound Features of Nonalcoholic Fatty Liver Disease and Cardiometabolic Risk Factors in Patients with Newly Diagnosed Type 2 Diabetes. Pol. Arch. Med. Wewn. 2013, 123, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Bian, H.; Xia, M.; Yan, H.; Chang, X.; Yao, X.; Rao, S.; Zeng, M.; Gao, X. Liver disease spectrum in hospitalized type 2 diabetes and related risk factors analysis of non-alcoholic fatty liver disease. Zhonghua Yi Xue Za Zhi 2013, 93, 270–274. [Google Scholar]
- Williamson, R.M.; Price, J.F.; Glancy, S.; Perry, E.; Nee, L.D.; Hayes, P.C.; Frier, B.M.; Van Look, L.A.F.; Johnston, G.I.; Reynolds, R.M.; et al. Prevalence of and Risk Factors for Hepatic Steatosis and Nonalcoholic Fatty Liver Disease in People with Type 2 Diabetes: The Edinburgh Type 2 Diabetes Study. Diabetes Care 2011, 34, 1139–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, W.; Ye, L.; Liu, A.; Wen, S.W.; Deng, J.; Wu, X.; Lai, Z. Prevalence of Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus: A Meta-Analysis. Medicine 2017, 96, e8179. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The Global Epidemiology of NAFLD and NASH in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Saponaro, C.; Gaggini, M.; Gastaldelli, A. Nonalcoholic Fatty Liver Disease and Type 2 Diabetes: Common Pathophysiologic Mechanisms. Curr. Diabetes Rep. 2015, 15, 607. [Google Scholar] [CrossRef]
- Williams, K.H.; Shackel, N.A.; Gorrell, M.D.; McLennan, S.V.; Twigg, S.M. Diabetes and Nonalcoholic Fatty Liver Disease: A Pathogenic Duo. Endocr. Rev. 2013, 34, 84–129. [Google Scholar] [CrossRef] [PubMed]
- Fruci, B.; Giuliano, S.; Mazza, A.; Malaguarnera, R.; Belfiore, A. Nonalcoholic Fatty Liver: A Possible New Target for Type 2 Diabetes Prevention and Treatment. Int. J. Mol. Sci. 2013, 14, 22933–22966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, S.-Y.; Pan, X.-Y.; Song, K.-X.; Huang, Y.-Y.; Li, F.; Cheng, X.-Y.; Qu, S. Differential Patterns of Insulin Secretion and Sensitivity in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease versus Patients with Type 2 Diabetes Mellitus Alone. Lipids Health Dis. 2014, 13, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finucane, F.M.; Sharp, S.J.; Hatunic, M.; Sleigh, A.; De Lucia Rolfe, E.; Aihie Sayer, A.; Cooper, C.; Griffin, S.J.; Wareham, N.J. Liver Fat Accumulation Is Associated with Reduced Hepatic Insulin Extraction and Beta Cell Dysfunction in Healthy Older Individuals. Diabetol. Metab. Syndr. 2014, 6, 43. [Google Scholar] [CrossRef] [Green Version]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The Multiple-Hit Pathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Browning, J.D.; Szczepaniak, L.S.; Dobbins, R.; Nuremberg, P.; Horton, J.D.; Cohen, J.C.; Grundy, S.M.; Hobbs, H.H. Prevalence of Hepatic Steatosis in an Urban Population in the United States: Impact of Ethnicity. Hepatology 2004, 40, 1387–1395. [Google Scholar] [CrossRef]
- Ekstedt, M.; Franzén, L.E.; Mathiesen, U.L.; Thorelius, L.; Holmqvist, M.; Bodemar, G.; Kechagias, S. Long-Term Follow-up of Patients with NAFLD and Elevated Liver Enzymes. Hepatology 2006, 44, 865–873. [Google Scholar] [CrossRef]
- Kashyap, S.R.; Defronzo, R.A. The Insulin Resistance Syndrome: Physiological Considerations. Diabetes Vasc. Dis. Res. 2007, 4, 13–19. [Google Scholar] [CrossRef]
- Kahn, B.B.; Flier, J.S. Obesity and Insulin Resistance. J. Clin. Investig. 2000, 106, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Katagiri, H.; Yamada, T.; Oka, Y. Adiposity and Cardiovascular Disorders: Disturbance of the Regulatory System Consisting of Humoral and Neuronal Signals. Circ. Res. 2007, 101, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Ahmadieh, H.; Azar, S.T. Liver Disease and Diabetes: Association, Pathophysiology, and Management. Diabetes Res. Clin. Pract. 2014, 104, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.N.A.; Maglio, C.; Pirazzi, C.; Burza, M.A.; Adiels, M.; Burch, L.; Donnelly, L.A.; Colhoun, H.; Doney, A.S.; Dillon, J.F.; et al. Paradoxical Lower Serum Triglyceride Levels and Higher Type 2 Diabetes Mellitus Susceptibility in Obese Individuals with the PNPLA3 148M Variant. PLoS ONE 2012, 7, e39362. [Google Scholar] [CrossRef] [PubMed]
- Dubuquoy, C.; Burnol, A.-F.; Moldes, M. PNPLA3, a Genetic Marker of Progressive Liver Disease, Still Hiding Its Metabolic Function? Clin. Res. Hepatol. Gastroenterol. 2013, 37, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Masarone, M.; Rosato, V.; Aglitti, A.; Bucci, T.; Caruso, R.; Salvatore, T.; Sasso, F.C.; Tripodi, M.F.; Persico, M. Liver Biopsy in Type 2 Diabetes Mellitus: Steatohepatitis Represents the Sole Feature of Liver Damage. PLoS ONE 2017, 12, e0178473. [Google Scholar] [CrossRef] [PubMed]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of Human Gut Microbiome Correlates with Metabolic Markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Dao, M.C.; Everard, A.; Aron-Wisnewsky, J.; Sokolovska, N.; Prifti, E.; Verger, E.O.; Kayser, B.D.; Levenez, F.; Chilloux, J.; Hoyles, L.; et al. Akkermansia Muciniphila and Improved Metabolic Health during a Dietary Intervention in Obesity: Relationship with Gut Microbiome Richness and Ecology. Gut 2016, 65, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The Gut-Liver Axis in Liver Disease: Pathophysiological Basis for Therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Lin, A.; Kong, M.; Yao, X.; Yin, M.; Xia, H.; Ma, J.; Liu, H. Intestinal Microbiome and NAFLD: Molecular Insights and Therapeutic Perspectives. J. Gastroenterol. 2020, 55, 142–158. [Google Scholar] [CrossRef] [Green Version]
- Dong, T.S.; Jacobs, J.P. Nonalcoholic Fatty Liver Disease and the Gut Microbiome: Are Bacteria Responsible for Fatty Liver? Exp. Biol. Med. 2019, 244, 408–418. [Google Scholar] [CrossRef]
- Menni, C.; Jackson, M.A.; Pallister, T.; Steves, C.J.; Spector, T.D.; Valdes, A.M. Gut Microbiome Diversity and High-Fibre Intake Are Related to Lower Long-Term Weight Gain. Int. J. Obes. 2017, 41, 1099–1105. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Zhang, F.; Ding, X.; Wu, G.; Lam, Y.Y.; Wang, X.; Fu, H.; Xue, X.; Lu, C.; Ma, J.; et al. Gut Bacteria Selectively Promoted by Dietary Fibers Alleviate Type 2 Diabetes. Science 2018, 359, 1151–1156. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Jiang, X.; Cao, M.; Ge, J.; Bao, Q.; Tang, L.; Chen, Y.; Li, L. Altered Fecal Microbiota Correlates with Liver Biochemistry in Nonobese Patients with Non-Alcoholic Fatty Liver Disease. Sci. Rep. 2016, 6, 32002. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Zheng, R.-D.; Sun, X.-Q.; Ding, W.-J.; Wang, X.-Y.; Fan, J.-G. Gut Microbiota Dysbiosis in Patients with Non-Alcoholic Fatty Liver Disease. Hepatobiliary Pancreat. Dis. Int 2017, 16, 375–381. [Google Scholar] [CrossRef]
- Mollica, M.P.; Mattace Raso, G.; Cavaliere, G.; Trinchese, G.; De Filippo, C.; Aceto, S.; Prisco, M.; Pirozzi, C.; Di Guida, F.; Lama, A.; et al. Butyrate Regulates Liver Mitochondrial Function, Efficiency, and Dynamics in Insulin-Resistant Obese Mice. Diabetes 2017, 66, 1405–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vadder, F.; Kovatcheva-Datchary, P.; Zitoun, C.; Duchampt, A.; Bäckhed, F.; Mithieux, G. Microbiota-Produced Succinate Improves Glucose Homeostasis via Intestinal Gluconeogenesis. Cell Metab. 2016, 24, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Fan, C.; Li, P.; Lu, Y.; Chang, X.; Qi, K. Short Chain Fatty Acids Prevent High-Fat-Diet-Induced Obesity in Mice by Regulating G Protein-Coupled Receptors and Gut Microbiota. Sci. Rep. 2016, 6, 37589. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.J.; Zheng, L.; Campbell, E.L.; Saeedi, B.; Scholz, C.C.; Bayless, A.J.; Wilson, K.E.; Glover, L.E.; Kominsky, D.J.; Magnuson, A.; et al. Crosstalk between Microbiota-Derived Short-Chain Fatty Acids and Intestinal Epithelial HIF Augments Tissue Barrier Function. Cell Host Microbe 2015, 17, 662–671. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Yin, J.; Zhang, J.; Ward, R.E.; Martin, R.J.; Lefevre, M.; Cefalu, W.T.; Ye, J. Butyrate Improves Insulin Sensitivity and Increases Energy Expenditure in Mice. Diabetes 2009, 58, 1509–1517. [Google Scholar] [CrossRef] [Green Version]
- Mattace Raso, G.; Simeoli, R.; Russo, R.; Iacono, A.; Santoro, A.; Paciello, O.; Ferrante, M.C.; Canani, R.B.; Calignano, A.; Meli, R. Effects of Sodium Butyrate and Its Synthetic Amide Derivative on Liver Inflammation and Glucose Tolerance in an Animal Model of Steatosis Induced by High Fat Diet. PLoS ONE 2013, 8, e68626. [Google Scholar]
- Canfora, E.E.; Meex, R.C.R.; Venema, K.; Blaak, E.E. Gut Microbial Metabolites in Obesity, NAFLD and T2DM. Nat. Rev. Endocrinol. 2019, 15, 261–273. [Google Scholar] [CrossRef]
- Palermo, A.; Maggi, D.; Maurizi, A.R.; Pozzilli, P.; Buzzetti, R. Prevention of Type 2 Diabetes Mellitus: Is It Feasible? Diabetes Metab. Res. Rev. 2014, 30 (Suppl. S1), 4–12. [Google Scholar] [CrossRef] [PubMed]
- Vrieze, A.; Van Nood, E.; Holleman, F.; Salojärvi, J.; Kootte, R.S.; Bartelsman, J.F.W.M.; Dallinga-Thie, G.M.; Ackermans, M.T.; Serlie, M.J.; Oozeer, R.; et al. Transfer of Intestinal Microbiota from Lean Donors Increases Insulin Sensitivity in Individuals with Metabolic Syndrome. Gastroenterology 2012, 143, 913–916.e7. [Google Scholar] [CrossRef]
- Erridge, C. Diet, Commensals and the Intestine as Sources of Pathogen-Associated Molecular Patterns in Atherosclerosis, Type 2 Diabetes and Non-Alcoholic Fatty Liver Disease. Atherosclerosis 2011, 216, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Firneisz, G. Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus: The Liver Disease of Our Age? World J. Gastroenterol. 2014, 20, 9072–9089. [Google Scholar]
- Wójcik-Cichy, K.; Koślińska-Berkan, E.; Piekarska, A. The Influence of NAFLD on the Risk of Atherosclerosis and Cardiovascular Diseases. Clin. Exp. Hepatol. 2018, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Colak, Y.; Senates, E.; Yesil, A.; Yilmaz, Y.; Ozturk, O.; Doganay, L.; Coskunpinar, E.; Kahraman, O.T.; Mesci, B.; Ulasoglu, C.; et al. Assessment of Endothelial Function in Patients with Nonalcoholic Fatty Liver Disease. Endocrine 2013, 43, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Salvi, P.; Ruffini, R.; Agnoletti, D.; Magnani, E.; Pagliarani, G.; Comandini, G.; Praticò, A.; Borghi, C.; Benetos, A.; Pazzi, P. Increased Arterial Stiffness in Nonalcoholic Fatty Liver Disease: The Cardio-GOOSE Study. J. Hypertens. 2010, 28, 1699–1707. [Google Scholar] [CrossRef]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic Syndrome and Risk of Incident Cardiovascular Events and Death: A Systematic Review and Meta-Analysis of Longitudinal Studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-Alcoholic Fatty Liver Disease and Risk of Incident Cardiovascular Disease: A Meta-Analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced Incidence of Type 2 Diabetes in Patients with Chronic Hepatitis C Virus Infection Cleared by Direct-Acting Antiviral Therapy: A Prospective Study. Diabetes Obes. Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Narciso, V.; Nevola, R.; Rinaldi, L.; Calvaruso, V.; Staiano, L.; Di Marco, V.; et al. Impact of Hepatitis C Virus Clearance by Direct-Acting Antiviral Treatment on the Incidence of Major Cardiovascular Events: A Prospective Multicentre Study. Atherosclerosis 2020, 296, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Sasso, F.C.; Pafundi, P.C.; Caturano, A.; Galiero, R.; Vetrano, E.; Nevola, R.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Di Marco, V.; et al. Impact of Direct Acting Antivirals (DAAs) on Cardiovascular Events in HCV Cohort with Pre-Diabetes. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, K.L.; Smith, C.I.; Schwarzenberg, S.J.; Jessurun, J.; Boldt, M.D.; Parks, E.J. Sources of Fatty Acids Stored in Liver and Secreted via Lipoproteins in Patients with Nonalcoholic Fatty Liver Disease. J. Clin. Investig. 2005, 115, 1343–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eguchi, Y.; Eguchi, T.; Mizuta, T.; Ide, Y.; Yasutake, T.; Iwakiri, R.; Hisatomi, A.; Ozaki, I.; Yamamoto, K.; Kitajima, Y.; et al. Visceral Fat Accumulation and Insulin Resistance Are Important Factors in Nonalcoholic Fatty Liver Disease. J. Gastroenterol. 2006, 41, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.J.; Samuel, V.T.; Petersen, K.F.; Shulman, G.I. The Role of Hepatic Lipids in Hepatic Insulin Resistance and Type 2 Diabetes. Nature 2014, 510, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.F.; Dufour, S.; Savage, D.B.; Bilz, S.; Solomon, G.; Yonemitsu, S.; Cline, G.W.; Befroy, D.; Zemany, L.; Kahn, B.B.; et al. The Role of Skeletal Muscle Insulin Resistance in the Pathogenesis of the Metabolic Syndrome. Proc. Natl. Acad. Sci. USA 2007, 104, 12587–12594. [Google Scholar] [CrossRef] [Green Version]
- Asrih, M.; Jornayvaz, F.R. Metabolic Syndrome and Nonalcoholic Fatty Liver Disease: Is Insulin Resistance the Link? Mol. Cell. Endocrinol. 2015, 418 Pt 1, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahima, R.S.; Lazar, M.A. Adipokines and the Peripheral and Neural Control of Energy Balance. Mol. Endocrinol. 2008, 22, 1023–1031. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Della Corte, C.; Mosca, A.; Majo, F.; Lucidi, V.; Panera, N.; Giglioni, E.; Monti, L.; Stronati, L.; Alisi, A.; Nobili, V. Nonalcoholic Fatty Pancreas Disease and Nonalcoholic Fatty Liver Disease: More than Ectopic Fat. Clin. Endocrinol. 2015, 83, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Alempijevic, T.; Dragasevic, S.; Zec, S.; Popovic, D.; Milosavljevic, T. Non-Alcoholic Fatty Pancreas Disease. Postgrad. Med. J. 2017, 93, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, T.D.; Alexakis, K.; Mavrikaki, V.; Mikhailidis, D.P. Nonalcoholic Fatty Pancreas Disease: Role in Metabolic Syndrome, “Prediabetes” Diabetes and Atherosclerosis. Dig. Dis. Sci. 2022, 67, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Y.; Ou, H.-Y.; Chen, M.-F.; Chang, T.-C.; Chang, C.-J. Enigmatic Ectopic Fat: Prevalence of Nonalcoholic Fatty Pancreas Disease and Its Associated Factors in a Chinese Population. J. Am. Heart Assoc. 2014, 3, e000297. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Kim, S.H.; Jun, D.W.; Han, J.H.; Jang, E.C.; Park, J.Y.; Son, B.K.; Kim, S.H.; Jo, Y.J.; Park, Y.S.; et al. Clinical Implications of Fatty Pancreas: Correlations between Fatty Pancreas and Metabolic Syndrome. World J. Gastroenterol. 2009, 15, 1869–1875. [Google Scholar] [CrossRef]
- Van Geenen, E.-J.M.; Smits, M.M.; Schreuder, T.C.M.A.; van der Peet, D.L.; Bloemena, E.; Mulder, C.J.J. Nonalcoholic Fatty Liver Disease Is Related to Nonalcoholic Fatty Pancreas Disease. Pancreas 2010, 39, 1185–1190. [Google Scholar] [CrossRef]
- Uygun, A.; Kadayifci, A.; Demirci, H.; Saglam, M.; Sakin, Y.S.; Ozturk, K.; Polat, Z.; Karslioglu, Y.; Bolu, E. The Effect of Fatty Pancreas on Serum Glucose Parameters in Patients with Nonalcoholic Steatohepatitis. Eur. J. Intern. Med. 2015, 26, 37–41. [Google Scholar] [CrossRef]
- Ou, H.-Y.; Wang, C.-Y.; Yang, Y.-C.; Chen, M.-F.; Chang, C.-J. The Association between Nonalcoholic Fatty Pancreas Disease and Diabetes. PLoS ONE 2013, 8, e62561. [Google Scholar] [CrossRef] [Green Version]
- Prasun, P. Mitochondrial Dysfunction in Metabolic Syndrome. Biochim. Biophys. Acta-Mol. Basis Dis. 2020, 1866, 165838. [Google Scholar] [CrossRef]
- Begriche, K.; Massart, J.; Robin, M.-A.; Bonnet, F.; Fromenty, B. Mitochondrial Adaptations and Dysfunctions in Nonalcoholic Fatty Liver Disease. Hepatology 2013, 58, 1497–1507. [Google Scholar] [CrossRef]
- Patterson, R.E.; Kalavalapalli, S.; Williams, C.M.; Nautiyal, M.; Mathew, J.T.; Martinez, J.; Reinhard, M.K.; McDougall, D.J.; Rocca, J.R.; Yost, R.A.; et al. Lipotoxicity in Steatohepatitis Occurs despite an Increase in Tricarboxylic Acid Cycle Activity. Am. J. Physiol. Endocrinol. Metab. 2016, 310, E484–E494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Z.; Tseng, Y.; White, M.F. Insulin Signaling Meets Mitochondria in Metabolism. Trends Endocrinol. Metab. 2010, 21, 589–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, M.; Mosaoa, R.; Graham, G.T.; Kasprzyk-Pawelec, A.; Gadre, S.; Parasido, E.; Catalina-Rodriguez, O.; Foley, P.; Giaccone, G.; Cheema, A.; et al. Inhibition of the Mitochondrial Citrate Carrier, Slc25a1, Reverts Steatosis, Glucose Intolerance, and Inflammation in Preclinical Models of NAFLD/NASH. Cell Death Differ. 2020, 27, 2143–2157. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Zhao, H. Role of Carnitine in Non-Alcoholic Fatty Liver Disease and Other Related Diseases: An Update. Front. Med. 2021, 8, 689042. [Google Scholar] [CrossRef]
- Harrison, S.A.; Di Bisceglie, A.M. Advances in the Understanding and Treatment of Nonalcoholic Fatty Liver Disease. Drugs 2003, 63, 2379–2394. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.; Caussy, C.; Imajo, K.; Chen, J.; Singh, S.; Kaulback, K.; Le, M.-D.; Hooker, J.; Tu, X.; Bettencourt, R.; et al. Magnetic Resonance vs. Transient Elastography Analysis of Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 630–637.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwenzer, N.F.; Springer, F.; Schraml, C.; Stefan, N.; Machann, J.; Schick, F. Non-Invasive Assessment and Quantification of Liver Steatosis by Ultrasound, Computed Tomography and Magnetic Resonance. J. Hepatol. 2009, 51, 433–445. [Google Scholar] [CrossRef]
- Lomonaco, R.; Sunny, N.E.; Bril, F.; Cusi, K. Nonalcoholic Fatty Liver Disease: Current Issues and Novel Treatment Approaches. Drugs 2013, 73, 1–14. [Google Scholar] [CrossRef]
- Bohte, A.E.; van Werven, J.R.; Bipat, S.; Stoker, J. The Diagnostic Accuracy of US, CT, MRI and 1H-MRS for the Evaluation of Hepatic Steatosis Compared with Liver Biopsy: A Meta-Analysis. Eur. Radiol. 2011, 21, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Cheah, M.C.; McCullough, A.J.; Goh, G.B.-B. Current Modalities of Fibrosis Assessment in Non-Alcoholic Fatty Liver Disease. J. Clin. Transl. Hepatol. 2017, 5, 261–271. [Google Scholar] [CrossRef] [Green Version]
- Yokoo, T.; Shiehmorteza, M.; Hamilton, G.; Wolfson, T.; Schroeder, M.E.; Middleton, M.S.; Bydder, M.; Gamst, A.C.; Kono, Y.; Kuo, A.; et al. Estimation of Hepatic Proton-Density Fat Fraction by Using MR Imaging at 3.0 T. Radiology 2011, 258, 749–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, A.; Tan, J.; Sun, M.; Hamilton, G.; Bydder, M.; Wolfson, T.; Gamst, A.C.; Middleton, M.; Brunt, E.M.; Loomba, R.; et al. Nonalcoholic Fatty Liver Disease: MR Imaging of Liver Proton Density Fat Fraction to Assess Hepatic Steatosis. Radiology 2013, 267, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graffy, P.M.; Pickhardt, P.J. Quantification of Hepatic and Visceral Fat by CT and MR Imaging: Relevance to the Obesity Epidemic, Metabolic Syndrome and NAFLD. Br. J. Radiol. 2016, 89, 20151024. [Google Scholar] [CrossRef] [Green Version]
- Petroff, D.; Blank, V.; Newsome, P.N.; Shalimar; Voican, C.S.; Thiele, M.; de Lédinghen, V.; Baumeler, S.; Chan, W.K.; Perlemuter, G.; et al. Assessment of Hepatic Steatosis by Controlled Attenuation Parameter Using the M and XL Probes: An Individual Patient Data Meta-Analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 185–198. [Google Scholar] [CrossRef]
- De Lédinghen, V.; Wong, G.L.-H.; Vergniol, J.; Chan, H.L.-Y.; Hiriart, J.-B.; Chan, A.W.-H.; Chermak, F.; Choi, P.C.-L.; Foucher, J.; Chan, C.K.-M.; et al. Controlled Attenuation Parameter for the Diagnosis of Steatosis in Non-Alcoholic Fatty Liver Disease. J. Gastroenterol. Hepatol. 2016, 31, 848–855. [Google Scholar] [CrossRef]
- Lee, H.W.; Park, S.Y.; Kim, S.U.; Jang, J.Y.; Park, H.; Kim, J.K.; Lee, C.K.; Chon, Y.E.; Han, K.-H. Discrimination of Nonalcoholic Steatohepatitis Using Transient Elastography in Patients with Nonalcoholic Fatty Liver Disease. PLoS ONE 2016, 11, e0157358. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.-K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.-H.; Wong, V.W.-S.; et al. FibroScan-AST (FAST) Score for the Non-Invasive Identification of Patients with Non-Alcoholic Steatohepatitis with Significant Activity and Fibrosis: A Prospective Derivation and Global Validation Study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, L.; Aggarwal, S.; Shalimar; Yadav, R.; Dattagupta, S.; Garg, H.; Agarwal, S. Bariatric Surgery in Nonalcoholic Fatty Liver Disease (NAFLD): Impact Assessment Using Paired Liver Biopsy and Fibroscan. Obes. Surg. 2021, 31, 617–626. [Google Scholar] [CrossRef]
- Caussy, C.; Alquiraish, M.H.; Nguyen, P.; Hernandez, C.; Cepin, S.; Fortney, L.E.; Ajmera, V.; Bettencourt, R.; Collier, S.; Hooker, J.; et al. Optimal Threshold of Controlled Attenuation Parameter with MRI-PDFF as the Gold Standard for the Detection of Hepatic Steatosis. Hepatology 2018, 67, 1348–1359. [Google Scholar] [CrossRef] [Green Version]
- Sasso, M.; Audière, S.; Kemgang, A.; Gaouar, F.; Corpechot, C.; Chazouillères, O.; Fournier, C.; Golsztejn, O.; Prince, S.; Menu, Y.; et al. Liver Steatosis Assessed by Controlled Attenuation Parameter (CAP) Measured with the XL Probe of the FibroScan: A Pilot Study Assessing Diagnostic Accuracy. Ultrasound Med. Biol. 2016, 42, 92–103. [Google Scholar] [CrossRef]
- Garg, H.; Aggarwal, S.; Shalimar; Yadav, R.; Datta Gupta, S.; Agarwal, L.; Agarwal, S. Utility of Transient Elastography (Fibroscan) and Impact of Bariatric Surgery on Nonalcoholic Fatty Liver Disease (NAFLD) in Morbidly Obese Patients. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2018, 14, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Festi, D.; Schiumerini, R.; Marzi, L.; Di Biase, A.R.; Mandolesi, D.; Montrone, L.; Scaioli, E.; Bonato, G.; Marchesini-Reggiani, G.; Colecchia, A. Review Article: The Diagnosis of Non-Alcoholic Fatty Liver Disease—Availability and Accuracy of Non-Invasive Methods. Aliment. Pharmacol. Ther. 2013, 37, 392–400. [Google Scholar] [CrossRef]
- Miyake, T.; Kumagi, T.; Furukawa, S.; Tokumoto, Y.; Hirooka, M.; Abe, M.; Hiasa, Y.; Matsuura, B.; Onji, M. Non-Alcoholic Fatty Liver Disease: Factors Associated with Its Presence and Onset. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. S4), 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahlman, H.; Ahlund, L.; Dahlström, A.; Nilsson, O.; Skolnik, G.; Tisell, L.E.; Tylén, U. Use of a Somatostatin Analogue in Association with Surgery and Hepatic Arterial Embolisation in the Treatment of the Carcinoid Syndrome. Br. J. Cancer 1987, 56, 840–842. [Google Scholar] [CrossRef] [Green Version]
- Tada, T.; Kumada, T.; Toyoda, H.; Kobayashi, N.; Sone, Y.; Oguri, T.; Kamiyama, N. Utility of Attenuation Coefficient Measurement Using an Ultrasound-Guided Attenuation Parameter for Evaluation of Hepatic Steatosis: Comparison with MRI-Determined Proton Density Fat Fraction. Am. J. Roentgenol. 2019, 212, 332–341. [Google Scholar] [CrossRef]
- Pirmoazen, A.M.; Khurana, A.; El Kaffas, A.; Kamaya, A. Quantitative Ultrasound Approaches for Diagnosis and Monitoring Hepatic Steatosis in Nonalcoholic Fatty Liver Disease. Theranostics 2020, 10, 4277–4289. [Google Scholar] [CrossRef]
- Janes, C.H.; Lindor, K.D. Outcome of Patients Hospitalized for Complications after Outpatient Liver Biopsy. Ann. Intern. Med. 1993, 118, 96–98. [Google Scholar] [CrossRef]
- Oki, Y.; Ono, M.; Hyogo, H.; Ochi, T.; Munekage, K.; Nozaki, Y.; Hirose, A.; Masuda, K.; Mizuta, H.; Okamoto, N.; et al. Evaluation of Postprandial Hypoglycemia in Patients with Nonalcoholic Fatty Liver Disease by Oral Glucose Tolerance Testing and Continuous Glucose Monitoring. Eur. J. Gastroenterol. Hepatol. 2018, 30, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhang, X.; Lin, H.; Liang, L.Y.; Wong, G.L.; Wong, V.W. Non-Invasive Tests of Non-Alcoholic Fatty Liver Disease. Chin. Med. J. 2022. [Google Scholar] [CrossRef]
- Nakahara, T.; Hyogo, H.; Yoneda, M.; Sumida, Y.; Eguchi, Y.; Fujii, H.; Ono, M.; Kawaguchi, T.; Imajo, K.; Aikata, H.; et al. Type 2 Diabetes Mellitus Is Associated with the Fibrosis Severity in Patients with Nonalcoholic Fatty Liver Disease in a Large Retrospective Cohort of Japanese Patients. J. Gastroenterol. 2014, 49, 1477–1484. [Google Scholar] [CrossRef] [Green Version]
- Stepanova, M.; Rafiq, N.; Makhlouf, H.; Agrawal, R.; Kaur, I.; Younoszai, Z.; McCullough, A.; Goodman, Z.; Younossi, Z.M. Predictors of All-Cause Mortality and Liver-Related Mortality in Patients with Non-Alcoholic Fatty Liver Disease (NAFLD). Dig. Dis. Sci. 2013, 58, 3017–3023. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Abraham, M.; Unalp, A.; Wilson, L.; Lavine, J.; Doo, E.; Bass, N.M. Association between Diabetes, Family History of Diabetes, and Risk of Nonalcoholic Steatohepatitis and Fibrosis. Hepatology 2012, 56, 943–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashiba, M.; Ono, M.; Hyogo, H.; Ikeda, Y.; Masuda, K.; Yoshioka, R.; Ishikawa, Y.; Nagata, Y.; Munekage, K.; Ochi, T.; et al. Glycemic Variability Is an Independent Predictive Factor for Development of Hepatic Fibrosis in Nonalcoholic Fatty Liver Disease. PLoS ONE 2013, 8, e76161. [Google Scholar] [CrossRef] [Green Version]
- Lv, W.-S.; Sun, R.-X.; Gao, Y.-Y.; Wen, J.-P.; Pan, R.-F.; Li, L.; Wang, J.; Xian, Y.-X.; Cao, C.-X.; Zheng, M. Nonalcoholic Fatty Liver Disease and Microvascular Complications in Type 2 Diabetes. World J. Gastroenterol. 2013, 19, 3134–3142. [Google Scholar] [CrossRef]
- Cakır, E.; Ozbek, M.; Colak, N.; Cakal, E.; Delıbaşi, T. Is NAFLD an Independent Risk Factor for Increased IMT in T2DM? Minerva Endocrinol. 2012, 37, 187–193. [Google Scholar] [PubMed]
- Trojak, A.; Waluś-Miarka, M.; Woźniakiewicz, E.; Małecki, M.T.; Idzior-Waluś, B. Nonalcoholic Fatty Liver Disease Is Associated with Low HDL Cholesterol and Coronary Angioplasty in Patients with Type 2 Diabetes. Med. Sci. Monit. 2013, 19, 1167–1172. [Google Scholar]
- Targher, G.; Bertolini, L.; Padovani, R.; Rodella, S.; Tessari, R.; Zenari, L.; Day, C.; Arcaro, G. Prevalence of Nonalcoholic Fatty Liver Disease and Its Association with Cardiovascular Disease among Type 2 Diabetic Patients. Diabetes Care 2007, 30, 1212–1218. [Google Scholar] [CrossRef] [Green Version]
- Idilman, I.S.; Akata, D.; Hazirolan, T.; Doganay Erdogan, B.; Aytemir, K.; Karcaaltincaba, M. Nonalcoholic Fatty Liver Disease Is Associated with Significant Coronary Artery Disease in Type 2 Diabetic Patients: A Computed Tomography Angiography Study 2. J. Diabetes 2015, 7, 279–286. [Google Scholar] [CrossRef]
- Bonapace, S.; Perseghin, G.; Molon, G.; Canali, G.; Bertolini, L.; Zoppini, G.; Barbieri, E.; Targher, G. Nonalcoholic Fatty Liver Disease Is Associated with Left Ventricular Diastolic Dysfunction in Patients with Type 2 Diabetes. Diabetes Care 2012, 35, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Bonapace, S.; Valbusa, F.; Bertolini, L.; Pichiri, I.; Mantovani, A.; Rossi, A.; Zenari, L.; Barbieri, E.; Targher, G. Nonalcoholic Fatty Liver Disease Is Associated with Aortic Valve Sclerosis in Patients with Type 2 Diabetes Mellitus. PLoS ONE 2014, 9, e88371. [Google Scholar] [CrossRef]
- Targher, G.; Valbusa, F.; Bonapace, S.; Bertolini, L.; Zenari, L.; Rodella, S.; Zoppini, G.; Mantovani, W.; Barbieri, E.; Byrne, C.D. Non-Alcoholic Fatty Liver Disease Is Associated with an Increased Incidence of Atrial Fibrillation in Patients with Type 2 Diabetes. PLoS ONE 2013, 8, e57183. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jeon, M.; Lee, J.; Han, J.; Oh, S.J.; Jung, T.; Nam, S.J.; Kil, W.H.; Lee, J.E. Induction of Fibronectin in Response to Epidermal Growth Factor Is Suppressed by Silibinin through the Inhibition of STAT3 in Triple Negative Breast Cancer Cells. Oncol. Rep. 2014, 32, 2230–2236. [Google Scholar] [CrossRef] [PubMed]
- Tziomalos, K.; Giampatzis, V.; Bouziana, S.D.; Spanou, M.; Papadopoulou, M.; Pavlidis, A.; Kostaki, S.; Bozikas, A.; Savopoulos, C.; Hatzitolios, A.I. Association between Nonalcoholic Fatty Liver Disease and Acute Ischemic Stroke Severity and Outcome. World J. Hepatol. 2013, 5, 621–626. [Google Scholar] [CrossRef]
- Jenks, S.J.; Conway, B.R.; Hor, T.J.; Williamson, R.M.; McLachlan, S.; Robertson, C.; Morling, J.R.; Strachan, M.W.J.; Price, J.F. Hepatic Steatosis and Non-Alcoholic Fatty Liver Disease Are Not Associated with Decline in Renal Function in People with Type 2 Diabetes. Diabet. Med. 2014, 31, 1039–1046. [Google Scholar] [CrossRef]
- Kim, B.-Y.; Jung, C.-H.; Mok, J.-O.; Kang, S.K.; Kim, C.-H. Prevalences of Diabetic Retinopathy and Nephropathy Are Lower in Korean Type 2 Diabetic Patients with Non-Alcoholic Fatty Liver Disease. J. Diabetes Investig. 2014, 5, 170–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziolkowska, S.; Binienda, A.; Jabłkowski, M.; Szemraj, J.; Czarny, P. The Interplay between Insulin Resistance, Inflammation, Oxidative Stress, Base Excision Repair and Metabolic Syndrome in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2021, 22, 11128. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Salmon, J.; Healy, G.N.; Shaw, J.E.; Jolley, D.; Zimmet, P.Z.; Owen, N. Association of Television Viewing with Fasting and 2-h Postchallenge Plasma Glucose Levels in Adults without Diagnosed Diabetes. Diabetes Care 2007, 30, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Al-Jiffri, O.; Al-Sharif, F.M.; Abd El-Kader, S.M.; Ashmawy, E.M. Weight Reduction Improves Markers of Hepatic Function and Insulin Resistance in Type-2 Diabetic Patients with Non-Alcoholic Fatty Liver. Afr. Health Sci. 2013, 13, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Kistler, K.D.; Brunt, E.M.; Clark, J.M.; Diehl, A.M.; Sallis, J.F.; Schwimmer, J.B. Physical Activity Recommendations, Exercise Intensity, and Histological Severity of Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2011, 106, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.E.; Elliott, E.J.; Naughton, G.A. Exercise for Type 2 Diabetes Mellitus. Cochrane Database Syst. Rev. 2006, 3, CD002968. [Google Scholar] [CrossRef]
- Snowling, N.J.; Hopkins, W.G. Effects of Different Modes of Exercise Training on Glucose Control and Risk Factors for Complications in Type 2 Diabetic Patients: A Meta-Analysis. Diabetes Care 2006, 29, 2518–2527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzetto, L.; Prinster, A.; Annuzzi, G.; Costagliola, L.; Mangione, A.; Vitelli, A.; Mazzarella, R.; Longobardo, M.; Mancini, M.; Vigorito, C.; et al. Liver Fat Is Reduced by an Isoenergetic MUFA Diet in a Controlled Randomized Study in Type 2 Diabetic Patients. Diabetes Care 2012, 35, 1429–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, H.; Qin, Y.-L.; Shi, Z.-Y.; Chen, J.-H.; Zeng, M.-J.; Zhou, W.; Chen, R.-Q.; Chen, Z.-Y. Effects of Alternate-Day Fasting on Body Weight and Dyslipidaemia in Patients with Non-Alcoholic Fatty Liver Disease: A Randomised Controlled Trial. BMC Gastroenterol. 2019, 19, 219. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Chou, W.; Sears, D.D.; Patterson, R.E.; Webster, N.J.G.; Ellies, L.G. Time-Restricted Feeding Improves Insulin Resistance and Hepatic Steatosis in a Mouse Model of Postmenopausal Obesity. Metabolism 2016, 65, 1743–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, K.E.; Haller, D.L.; Sargeant, C.; Levenson, J.L.; Puri, P.; Sanyal, A.J. Readiness for Behaviour Change in Non-Alcoholic Fatty Liver Disease: Implications for Multidisciplinary Care Models. Liver Int. Off. J. Int. Assoc. Study Liver 2015, 35, 936–943. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.A.; Kelleni, M.; Geddawy, A. Nonalcoholic Fatty Liver Disease: Current and Potential Therapies. Life Sci. 2013, 92, 114–118. [Google Scholar] [CrossRef]
- Duseja, A.; Das, A.; Dhiman, R.K.; Chawla, Y.K.; Thumburu, K.T.; Bhadada, S.; Bhansali, A. Metformin Is Effective in Achieving Biochemical Response in Patients with Nonalcoholic Fatty Liver Disease (NAFLD) Not Responding to Lifestyle Interventions. Ann. Hepatol. 2007, 6, 222–226. [Google Scholar] [CrossRef]
- Shyangdan, D.; Clar, C.; Ghouri, N.; Henderson, R.; Gurung, T.; Preiss, D.; Sattar, N.; Fraser, A.; Waugh, N. Insulin Sensitisers in the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review. Health Technol. Assess. 2011, 15, 1–110. [Google Scholar] [CrossRef] [Green Version]
- Haukeland, J.W.; Konopski, Z.; Eggesbø, H.B.; von Volkmann, H.L.; Raschpichler, G.; Bjøro, K.; Haaland, T.; Løberg, E.M.; Birkeland, K. Metformin in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Controlled Trial. Scand. J. Gastroenterol. 2009, 44, 853–860. [Google Scholar] [CrossRef]
- Linden, M.A.; Fletcher, J.A.; Morris, E.M.; Meers, G.M.; Kearney, M.L.; Crissey, J.M.; Laughlin, M.H.; Booth, F.W.; Sowers, J.R.; Ibdah, J.A.; et al. Combining Metformin and Aerobic Exercise Training in the Treatment of Type 2 Diabetes and NAFLD in OLETF Rats. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E300–E310. [Google Scholar] [CrossRef] [Green Version]
- Vuppalanchi, R.; Chalasani, N. Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Selected Practical Issues in Their Evaluation and Management. Hepatology 2009, 49, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Duvnjak, M.; Tomasic, V.; Gomercic, M.; Smircic Duvnjak, L.; Barsic, N.; Lerotic, I. Therapy of Nonalcoholic Fatty Liver Disease: Current Status. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 57–66. [Google Scholar]
- Shadid, S.; Jensen, M.D. Effect of Pioglitazone on Biochemical Indices of Non-Alcoholic Fatty Liver Disease in Upper Body Obesity. Clin. Gastroenterol. Hepatol. 2003, 1, 384–387. [Google Scholar] [CrossRef]
- Saryusz-Wolska, M.; Szymańska-Garbacz, E.; Jabłkowski, M.; Białkowska, J.; Pawłowski, M.; Kwiecińska, E.; Omulecka, A.; Borkowska, A.; Ignaczak, A.; Loba, J.; et al. Rosiglitazone Treatment in Nondiabetic Subjects with Nonalcoholic Fatty Liver Disease. Pol. Arch. Med. Wewn. 2011, 121, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Lutchman, G.; Modi, A.; Kleiner, D.E.; Promrat, K.; Heller, T.; Ghany, M.; Borg, B.; Loomba, R.; Liang, T.J.; Premkumar, A.; et al. The Effects of Discontinuing Pioglitazone in Patients with Nonalcoholic Steatohepatitis. Hepatology 2007, 46, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.; Fu, J. Pioglitazone for NAFLD Patients with Prediabetes or Type 2 Diabetes Mellitus: A Meta-Analysis. Front. Endocrinol. 2021, 12, 428. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Charlotte, F.; Bernhardt, C.; Giral, P.; Halbron, M.; Lenaour, G.; Hartmann-Heurtier, A.; Bruckert, E.; Poynard, T. Long-Term Efficacy of Rosiglitazone in Nonalcoholic Steatohepatitis: Results of the Fatty Liver Improvement by Rosiglitazone Therapy (FLIRT 2) Extension Trial. Hepatology 2010, 51, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Omer, Z.; Cetinkalp, S.; Akyildiz, M.; Yilmaz, F.; Batur, Y.; Yilmaz, C.; Akarca, U. Efficacy of Insulin-Sensitizing Agents in Nonalcoholic Fatty Liver Disease. Eur. J. Gastroenterol. Hepatol. 2010, 22, 18–23. [Google Scholar] [CrossRef]
- Colca, J.R.; McDonald, W.G.; Adams, W.J. MSDC-0602K, a Metabolic Modulator Directed at the Core Pathology of Non-Alcoholic Steatohepatitis. Expert Opin. Investig. Drugs 2018, 27, 631–636. [Google Scholar] [CrossRef]
- Cuthbertson, D.J.; Irwin, A.; Gardner, C.J.; Daousi, C.; Purewal, T.; Furlong, N.; Goenka, N.; Thomas, E.L.; Adams, V.L.; Pushpakom, S.P.; et al. Improved Glycaemia Correlates with Liver Fat Reduction in Obese, Type 2 Diabetes, Patients given Glucagon-like Peptide-1 (GLP-1) Receptor Agonists. PLoS ONE 2012, 7, e50117. [Google Scholar] [CrossRef]
- Fan, H.; Pan, Q.; Xu, Y.; Yang, X. Exenatide Improves Type 2 Diabetes Concomitant with Non-Alcoholic Fatty Liver Disease. Arq. Bras. Endocrinol. Metabol. 2013, 57, 702–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, N.; Kuang, H.Y.; Hao, M.; Gao, X.Y.; Lin, W.J.; Zou, W. Benefits of Exenatide on Obesity and Non-Alcoholic Fatty Liver Disease with Elevated Liver Enzymes in Patients with Type 2 Diabetes. Diabetes Metab. Res. Rev. 2014, 30, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Houlihan, D.D.; Rowe, I.A.; Clausen, W.H.O.; Elbrønd, B.; Gough, S.C.L.; Tomlinson, J.W.; Newsome, P.N. Safety and Efficacy of Liraglutide in Patients with Type 2 Diabetes and Elevated Liver Enzymes: Individual Patient Data Meta-Analysis of the LEAD Program. Aliment. Pharmacol. Ther. 2013, 37, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, T.; Hyogo, H.; Ochi, H.; Fujino, H.; Kan, H.; Naeshiro, N.; Honda, Y.; Miyaki, D.; Kawaoka, T.; Tsuge, M.; et al. Efficacy and Safety of Sitagliptin for the Treatment of Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus. Hepatogastroenterology 2014, 61, 323–328. [Google Scholar]
- Deng, X.-L.; Ma, R.; Zhu, H.-X.; Zhu, J. Short Article: A Randomized-Controlled Study of Sitagliptin for Treating Diabetes Mellitus Complicated by Nonalcoholic Fatty Liver Disease. Eur. J. Gastroenterol. Hepatol. 2017, 29, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Ohki, T.; Isogawa, A.; Iwamoto, M.; Ohsugi, M.; Yoshida, H.; Toda, N.; Tagawa, K.; Omata, M.; Koike, K. The Effectiveness of Liraglutide in Nonalcoholic Fatty Liver Disease Patients with Type 2 Diabetes Mellitus Compared to Sitagliptin and Pioglitazone. Sci. World J. 2012, 2012, 496453. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycaemia in Type 2 Diabetes: A Patient-Centered Approach. Position Statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012, 55, 1577–1596. [Google Scholar] [CrossRef]
- Chatran, M.; Pilehvar-Soltanahmadi, Y.; Dadashpour, M.; Faramarzi, L.; Rasouli, S.; Jafari-gharabaghlou, D.; Asbaghi, N.; Zarghami, N.; Zarghami, N.; Street, G.; et al. Synergistic Anti-Proliferative Effects of Metformin and Silibinin Combination on T47D Breast Cancer Cells via HTERT and Cyclin D1 Inhibition. Drug Res. 2018, 68, 710–716. [Google Scholar] [CrossRef] [Green Version]
- Fraser, A.; Harris, R.; Sattar, N.; Ebrahim, S.; Davey Smith, G.; Lawlor, D.A. Alanine Aminotransferase, Gamma-Glutamyltransferase, and Incident Diabetes: The British Women’s Heart and Health Study and Meta-Analysis. Diabetes Care 2009, 32, 741–750. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.; Mittendorfer, B.; Eagon, J.C.; Patterson, B.; Grant, L.; Feirt, N.; Seki, E.; Brenner, D.; Korenblat, K.; McCrea, J. Gastric Bypass Surgery Improves Metabolic and Hepatic Abnormalities Associated with Nonalcoholic Fatty Liver Disease. Gastroenterology 2006, 130, 1564–1572. [Google Scholar] [CrossRef]
- Viana, E.C.; Araujo-Dasilio, K.L.; Miguel, G.P.S.; Bressan, J.; Lemos, E.M.; Moyses, M.R.; de Abreu, G.R.; de Azevedo, J.L.M.C.; Carvalho, P.S.; Passos-Bueno, M.R.S.; et al. Gastric Bypass and Sleeve Gastrectomy: The Same Impact on IL-6 and TNF-α. Prospective Clinical Trial. Obes. Surg. 2013, 23, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Bower, G.; Toma, T.; Harling, L.; Jiao, L.R.; Efthimiou, E.; Darzi, A.; Athanasiou, T.; Ashrafian, H. Bariatric Surgery and Non-Alcoholic Fatty Liver Disease: A Systematic Review of Liver Biochemistry and Histology. Obes. Surg. 2015, 25, 2280–2289. [Google Scholar] [CrossRef] [PubMed]
- Praveen Raj, P.; Gomes, R.M.; Kumar, S.; Senthilnathan, P.; Karthikeyan, P.; Shankar, A.; Palanivelu, C. The Effect of Surgically Induced Weight Loss on Nonalcoholic Fatty Liver Disease in Morbidly Obese Indians: “NASHOST” Prospective Observational Trial. Surg. Obes. Relat. Dis. 2015, 11, 1315–1322. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Medications | cART in HIV, chemotherapy, amiodarone, methotrexate, tamoxifen, corticosteroids, tetracyclines, valproic acid, amphetamines, acetylsalicylic acid |
| Genetic causes | haemochromatosis, alpha-1 antitrypsin deficiency, Wilson’s disease, congenital lipodystrophy, abetalipoproteinaemia, hypobetalipoproteinaemia, familial hyperlipidaemia, lysosomal acid lipase deficiency, glycogen storage diseases, hereditary fructose intolerance, urea cycle disorders, citrin deficiency |
| Environmental causes | lead, arsenic, mercury, cadmium, herbicides, pesticides, polychlorinated biphenyls, chloroalkenes |
| Nutritional/gastroenterological causes | severe surgical weight loss, starvation, malnutrition, total parenteral nutrition, microbiome changes, coeliac disease, pancreatectomy, short bowel syndrome |
| Other causes | Chronic HCV infection, hypothyroidism, polycystic ovary syndrome, hypothalamic or pituitary dysfunction, growth hormone deficiency, HELLP syndrome, acute fatty liver of pregnancy, celiac disease, Wilson’s disease, hepatitis C virus, Amanita phalloides mushrooms, phosphorous poisoning, petrochemicals, Bacillus cereus toxin |
| Index | Factors |
|---|---|
| AST/ALT ratio | AST, ALT |
| APRI (AST to platelet ratio index) | AST, upper normal limit for ALT, PLT |
| FibroTest | Age, gender, total bilirubin, haptoglobin, GGT, α2-macroglobulin, apolipoprotein-A |
| FibroMax | Age, gender, total bilirubin, haptoglobin, GGT, α2-macroglobulin, apolipoprotein-A, ALT, AST, TCH, TG, fasting glucose, weight, height |
| FibroMeter | HA, PLT, prothrombin index, α2-macroglobulin |
| BARD | BMI, AST/ALT ratio, diabetes mellitus |
| NFS (NAFLD fibrosis score) | Age, hyperglycemia, BMI, PLT, albumin, AST/ALT ratio |
| FIB-4 (fibrosis 4 index) | Age, AST, ALT, PLT |
| HepatoScore | Age, gender, bilirubin, GGT, HA, α2-macroglobulin |
| OELF (Original European Liver Fibrosis panel) | Age, TIMP 1, HA, P3NP |
| ELF (European Liver Fibrosis panel) | HA, P3NP, TIMP-1 |
| NIKEI (Noninvasive Koeln–Essen-index) | Age, AST, AST/ALT ratio, total bilirubin |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmalski, M.; Ziółkowska, S.; Czarny, P.; Szemraj, J.; Pietras, T. The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. J. Clin. Med. 2022, 11, 1375. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051375
Kosmalski M, Ziółkowska S, Czarny P, Szemraj J, Pietras T. The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2022; 11(5):1375. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051375
Chicago/Turabian StyleKosmalski, Marcin, Sylwia Ziółkowska, Piotr Czarny, Janusz Szemraj, and Tadeusz Pietras. 2022. "The Coexistence of Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus" Journal of Clinical Medicine 11, no. 5: 1375. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051375