
A Therapeutic Pathway in Patients with Chronic Coronary Syndromes: Proposal for Optimization

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Subjects and Methods
3. Results
3.1. Study Population
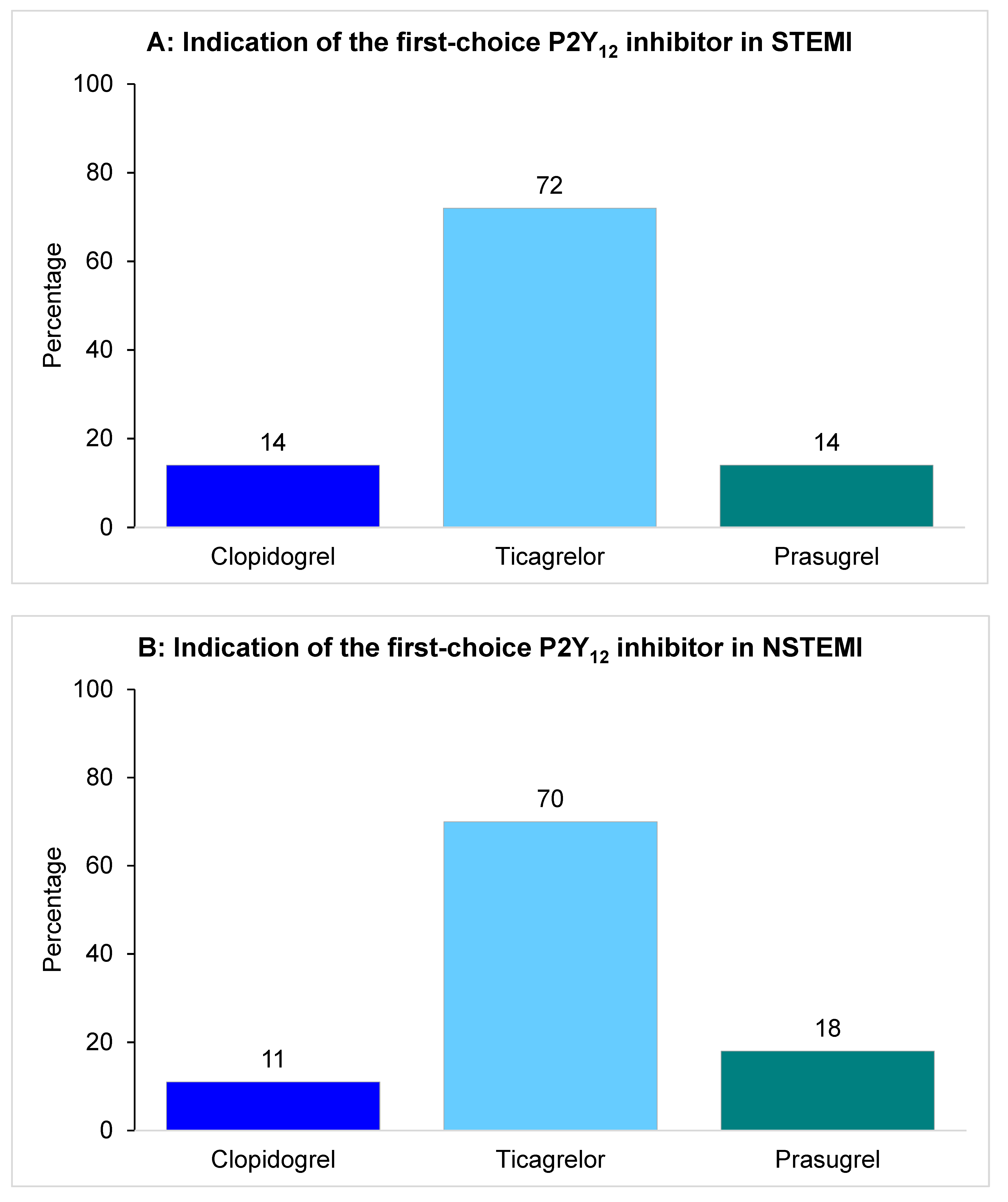
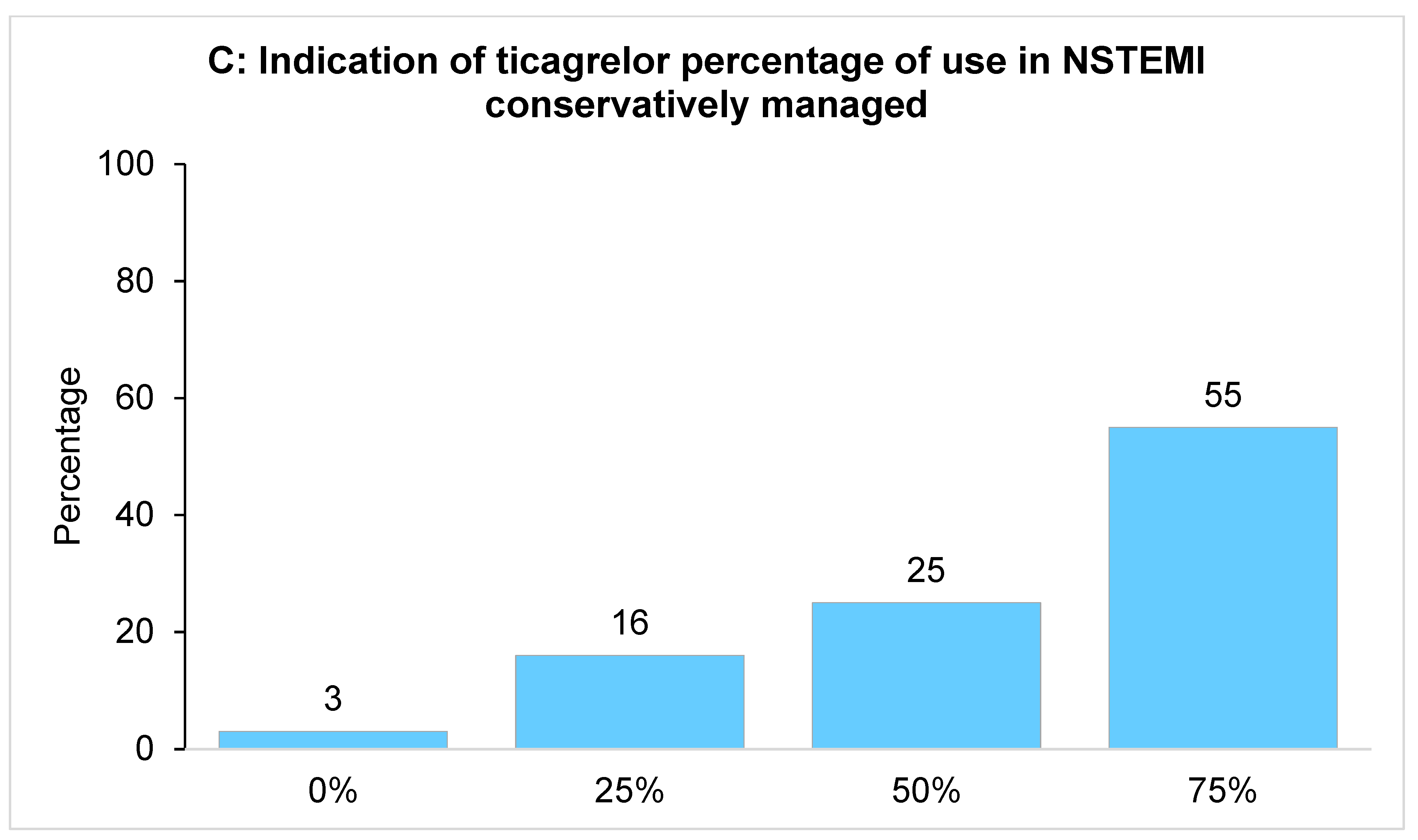
3.2. In-Hospital P2Y12 Inhibitor Management
3.3. Follow-Up of CCS Patients and Long-Term DAPT Prescription
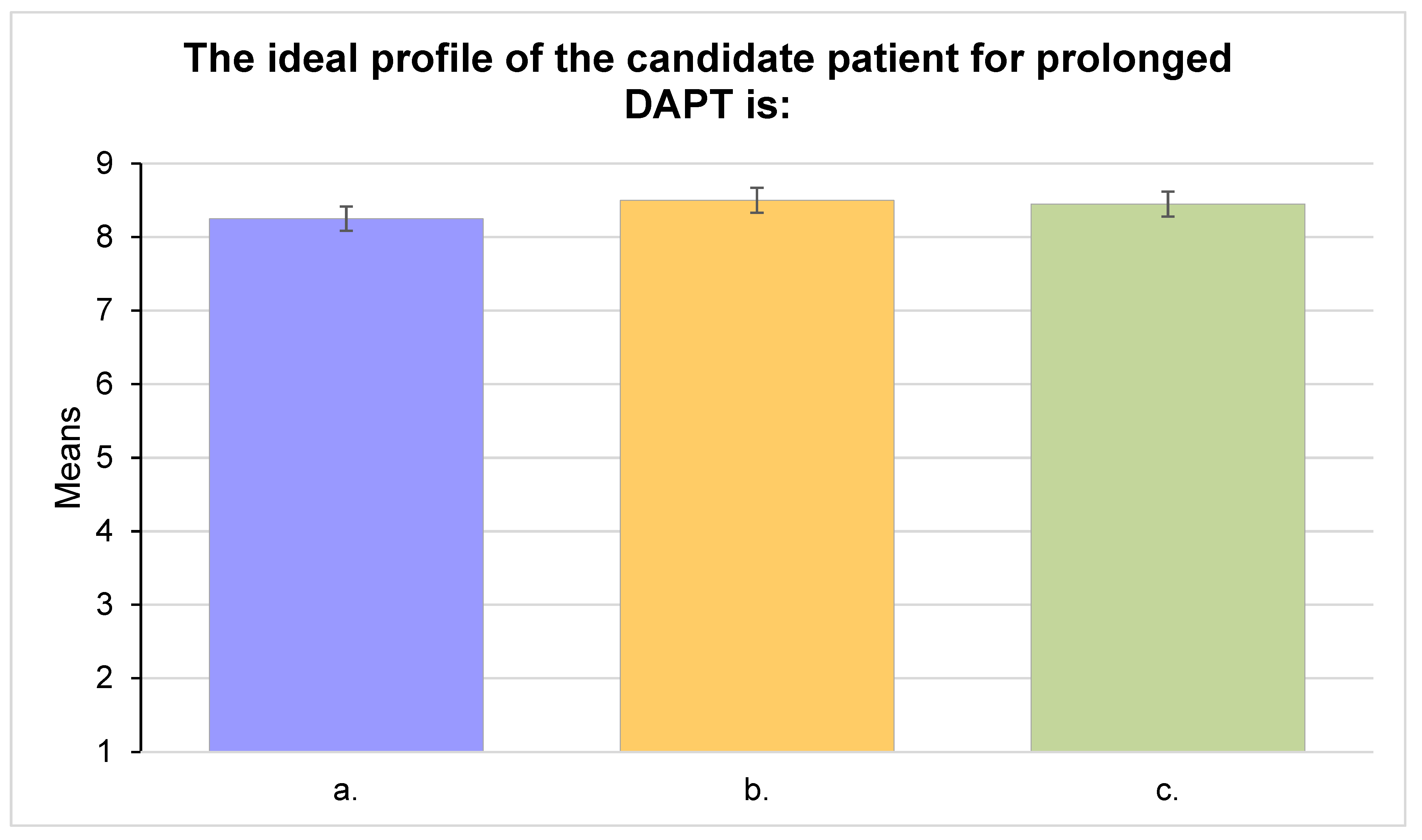
3.4. Identification of Long-Term DAPT Candidates
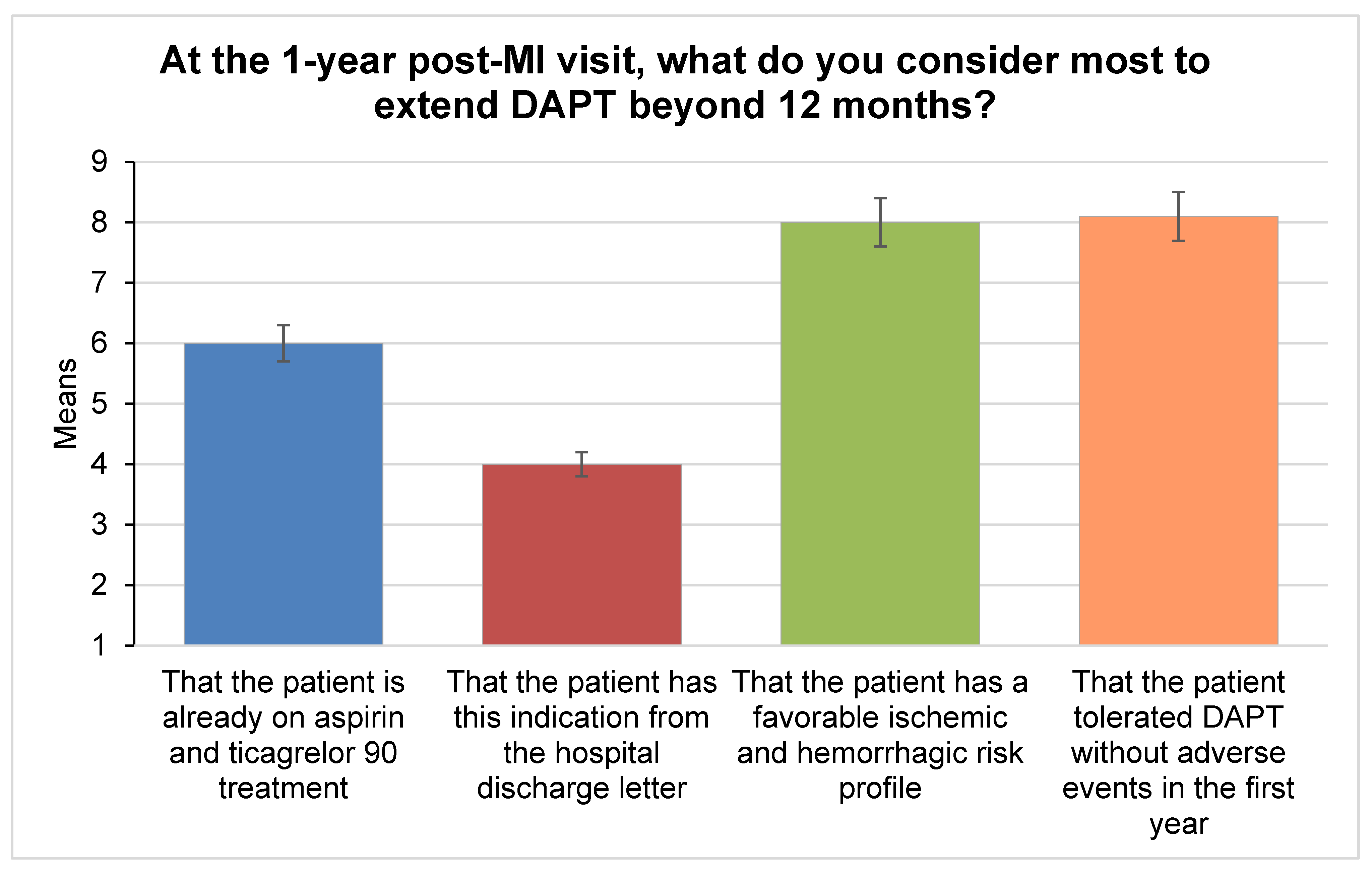
3.5. Outpatient Management at the One-Year Visit
- A patient with post-MI CCS, without high hemorrhagic risk, multivessel
- A patient with post-MI CCS, without high hemorrhagic risk, at high residual ischemic risk by clinical characteristics (diabetes mellitus, chronic renal failure, recurrent acute events, multivessel atherosclerosis)
- A patient with post-MI CCS, without high hemorrhagic risk, at high residual ischemic risk by procedural characteristics of percutaneous revascularization (main stem disease; three or more lesions; implantation of three or more stents; bifurcation treatment with two stents, treatment of chronic occlusions or venous grafts, total stent length >60 mm)
4. Discussion
- Ticagrelor is still considered as the first choice P2Y12 inhibitor in ACS patients, irrespective of the presentation (STEMI vs. NSTEMI) or the management (invasive vs. conservative);
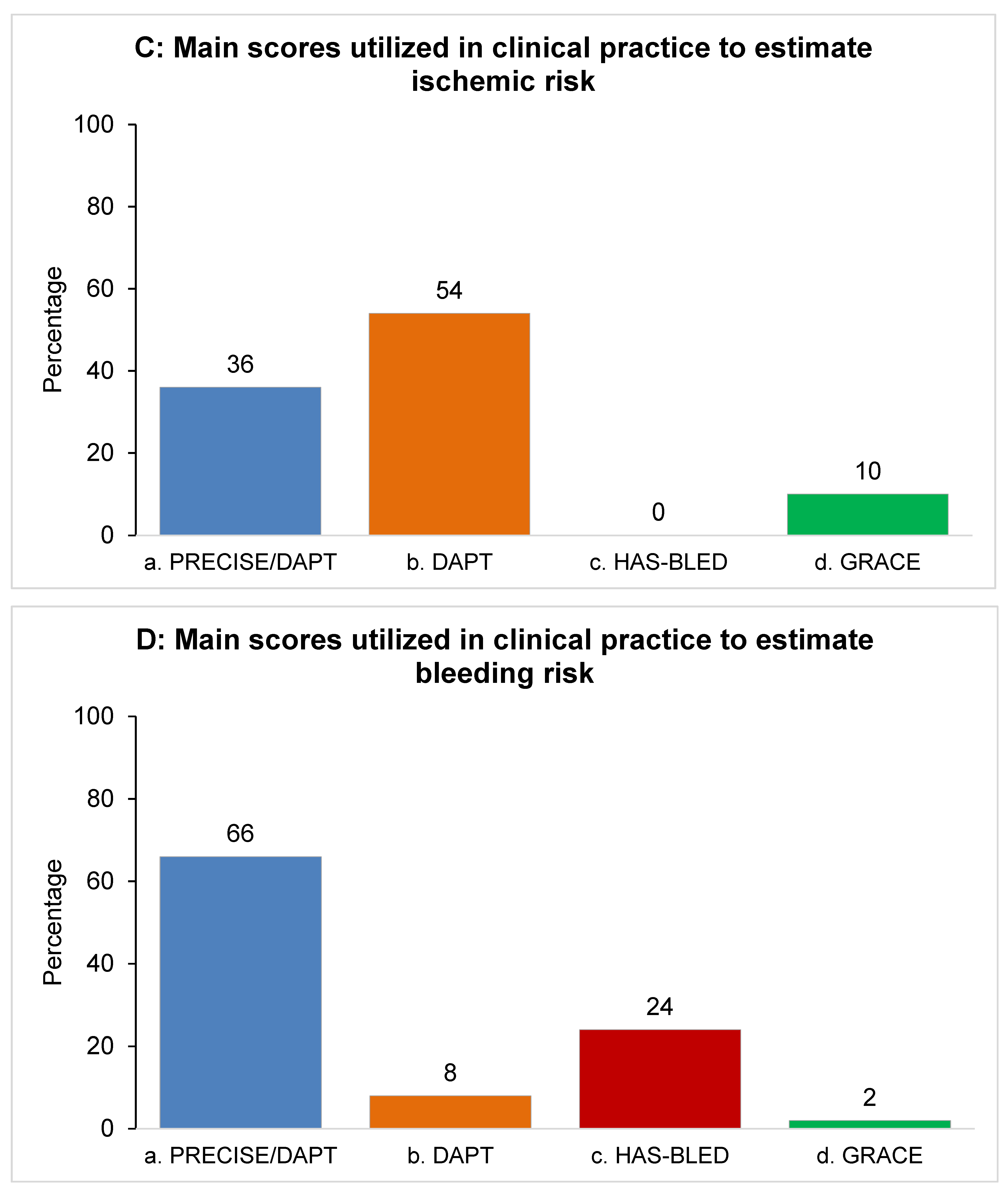
- Prolonged DAPT regimens after one year are acknowledged as important strategies by more than two-thirds of respondents, and scores to estimate ischemic and bleeding risks were declared to be frequently utilized in clinical practice;
- When clinically indicated, the switch from one P2Y12 inhibitor to another does not represent a barrier to prolong DAPT with ticagrelor 60 mg.
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Task Force Members; Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar] [CrossRef]
- Piironen, M.; Ukkola, O.; Huikuri, H.; Havulinna, A.S.; Koukkunen, H.; Mustonen, J.; Ketonen, M.; Lehto, S.; Airaksinen, J.; Kesaeniemi, Y.A.; et al. Trends in long-term prognosis after acute coronary syndrome. Eur. J. Prev. Cardiol. 2017, 24, 274–280. [Google Scholar] [CrossRef]
- Ziada, K.M.; Moliterno, D.J. Dual antiplatelet therapy: Is it time to cut the cord with aspirin? JAMA 2019, 321, 2409–2411. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bhatt, D.L.; Cohen, M.; Steg, P.G.; Storey, R.F.; Jensen, E.C.; Magnani, G.; Bansilal, S.; Fish, M.P.; Im, K.; et al. Long-term use of ticagrelor in patients with prior myocardial infarction. N. Engl. J. Med. 2015, 372, 1791–1800. [Google Scholar] [CrossRef] [Green Version]
- De Luca, L.; Colivicchi, F.; Meessen, J.; Uguccioni, M.; Piscione, F.; Bernabò, P.; Lardieri, G.; Granatelli, A.; Gabrielli, D.; Gulizia, M.M.; et al. How do cardiologists select patients for dual antiplatelet therapy continuation beyond 1 year after a myocardial infarction? Insights from the EYESHOT Post-MI Study. Clin. Cardiol. 2019, 42, 1113–1120. [Google Scholar] [CrossRef] [Green Version]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar]
- Cassese, S.; Byrne, R.A.; Tada, T.; King, L.A.; Kastrati, A. Clinical impact of extended dual antiplatelet therapy after percutaneous coronary interventions in the drug-eluting stent era: A meta-analysis of randomized trials. Eur. Heart J. 2012, 33, 3078–3087. [Google Scholar] [CrossRef] [Green Version]
- Dellborg, M.; Bonaca, M.P.; Storey, R.F.; Steg, P.G.; Im, K.A.; Cohen, M.; Bhatt, D.L.; Ophuis, T.O.; Budaj, A.; Hamm, C.; et al. Efficacy and safety with ticagrelor in patients with prior myocardial infarction in the approved European label: Insights from PEGASUS-TIMI 54. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Cesaro, A.; Taglialatela, V.; Gragnano, F.; Moscarella, E.; Fimiani, F.; Conte, M.; Barletta, V.; Monda, E.; Limongelli, G.; Severino, S.; et al. Low-Dose Ticagrelor in Patients with High Ischemic Risk and Previous Myocardial Infarction: A Multicenter Prospective Real-World Observational Study. J. Cardiovasc. Pharmacol. 2020, 76, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Rossini, R.; Oltrona Visconti, L.; Musumeci, G.; Filippi, A.; Pedretti, R.; Lettieri, C.; Buffoli, F.; Campana, M.; Capodanno, D.; Castiglioni, B.; et al. A multidisciplinary consensus document on follow-up strategies for patients treated with percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2015, 85, E129–E139. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Hansson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R. The RAND/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001; Available online: https://www.rand.org/pubs/monograph_reports/MR1269.html (accessed on 6 December 2021).
- Linstone, H.; Turoff, M. (Eds.) The Delphi Method. Techniques and Applications; Addison-Wesley Publishing Company: Reading, MA, USA, 1995; pp. 1–616. [Google Scholar]
- Jones, J.; Hunter, D. Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef]
- Rowe, G.; Wright, G. The Delphi technique as a forecasting tool: Issues and analysis. Int. J. Forecast. 1999, 15, 353–375. [Google Scholar] [CrossRef]
- Graham, B.; Regehr, G.; Wright, J.G. Delphi as a method to establish consensus for diagnostic criteria. J. Clin. Epidemiol. 2003, 56, 1150–1156. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Schüpke, S.; Neumann, F.J.; Menichelli, M.; Mayer, K.; Bernlochner, I.; Wöhrle, J.; Richardt, G.; Liebetrau, C.; Witzenbichler, B.; Antoniucci, D.; et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2019, 381, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Angoulvant, D.; Sabouret, P.; Savage, M.P. NSTE-ACS ESC Guidelines Recommend Prasugrel as the Preferred P2Y12 Inhibitor: A Contrarian View. Am. J. Cardiovasc. Drugs 2021, 21, 483–486. [Google Scholar] [CrossRef]
- Timmis, A.; Rapsomaniki, E.; Chung, S.C.; Rodriguez, M.P.; Moayyeri, A.; Stogiannis, D.; Shah, A.D.; Pasea, L.; Denaxas, S.; Emmas, C.; et al. Prolonged dual antiplatelet therapy in stable coronary disease: Comparative observational study of benefits and harms in unselected versus trial populations. BMJ 2016, 353, i3163. [Google Scholar] [CrossRef] [Green Version]
- Cesaro, A.; Gragnano, F.; Calabrò, P.; Moscarella, E.; Santelli, F.; Fimiani, F.; Patti, G.; Cavallari, I.; Antonucci, E.; Cirillo, P.; et al. Prevalence and clinical implications of eligibility criteria for prolonged dual antithrombotic therapy in patients with PEGASUS and COMPASS phenotypes: Insights from the START-ANTIPLATELET registry. Int. J. Cardiol. 2021, 345, 7–13. [Google Scholar] [CrossRef]
- Perrone Filardi, P.; Caldarola, P.; Colivicchi, F.; Mugelli, A.; Varbella, F.; Paolillo, S. Strategie antitrombotiche a lungo termine nel paziente post-infarto [Long-term antithrombotic strategies in post-myocardial infarction patients]. G. Ital. Cardiol. 2019, 20 (Suppl. 1), e1–e11. [Google Scholar] [CrossRef]
- Urban, P.; Mehran, R.; Colleran, R.; Angiolillo, D.J.; Byrne, R.A.; Capodanno, D.; Cuisset, T.; Cutlip, D.; Eerdmans, P.; Eikelboom, J.; et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 2019, 40, 2632–2653. [Google Scholar] [CrossRef] [Green Version]
- Gragnano, F.; Spirito, A.; Corpataux, N.; Vaisnora, L.; Galea, R.; Gargiulo, G.; Siontis, G.C.; Praz, F.; Lanz, J.; Billinger, M.; et al. Impact of clinical presentation on bleeding risk after percutaneous coronary intervention and implications for the ARC-HBR definition. EuroIntervention 2021, 17, e898–e909. [Google Scholar] [CrossRef]
- Yeh, R.W.; Secemsky, E.A.; Kereiakes, D.J.; Normand, S.-L.; Gershlick, A.H.; Cohen, D.J.; Spertus, J.A.; Steg, P.G.; Cutlip, D.E.; Rinaldi, M.J.; et al. Development and Validation of a Prediction Rule for Benefit and Harm of Dual Antiplatelet Therapy beyond 1 Year after Percutaneous Coronary Intervention. JAMA 2016, 315, 1735–1749. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; van Klaveren, D.; James, S.; Heg, D.; Räber, L.; Feres, F.; Pilgrim, T.; Hong, M.K.; Kim, H.S.; Colombo, A.; et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: A pooled analysis of individual-patient datasets from clinical trials. Lancet 2017, 389, 1025–1034. [Google Scholar] [CrossRef]
- Crisci, M.; Gragnano, F.; Di Maio, M.; Diana, V.; Moscarella, E.; Pariggiano, I.; Di Maio, D.; Concilio, C.; Taglialatela, V.; Fimiani, F.; et al. Improving Adherence to Ticagrelor in Patients After Acute Coronary Syndrome: Results from the PROGRESS Trial. Curr. Vasc. Pharmacol. 2020, 18, 294–301. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q1 | Q2 | |
|---|---|---|
| N = 122 | N = 87 | |
| Age, years | 41.8 ± 8.8 | 42.1 ± 8.6 |
| Overall working experience, years | 16.6 ± 8.4 | 16.6 ± 8.4 |
| Experience in cardiovascular disease treatment, years | 15 ± 8.4 | 15.1 ± 8.5 |
| Main occupation | ||
| Cath lab | 56 (46%) | 37 (42%) |
| Coronary Intensive Care Unit/Ward | 50 (41%) | 38 (48%) |
| Out-patient service | 16 (13%) | 12 (11%) |
| Place of work | ||
| University | 29 (24%) | |
| Public hospital | 89 (73%) | |
| Private hospital | 15 (12%) | |
| Hub hospital | 40 (33%) | |
| Spoke hospital | 17 (14%) | |
| Out-of-hospital ambulatory | 9 (7%) |
| Item | Median | IQR | IPRAS | Assessment |
|---|---|---|---|---|
| 17. How would you define a patient with CCS? | ||||
| 17.c. Asymptomatic patient (and/or with stabilized symptomatology) | 7 | 4 | 4.60 | appropriate |
| 17.e. Patient with elective revascularization for more than one year | 7 | 4 | 6.10 | appropriate |
| 17.f. Patient more than 1 year after MI with no further events | 8 | 3 | 6.10 | appropriate |
| 18. Do you consider CCS to be a dynamic disease? | 9 | 2 | 7.08 | appropriate |
| 27. At the 1-year post-MI visit. what element do you most consider to extend DAPT beyond 12 months? | ||||
| 27.c. That he has a favourable ischemic and hemorrhagic risk profile | 9 | 1 | 7.60 | appropriate |
| 27.d. That he tolerated DAPT without adverse events in the first year | 9 | 1 | 7.60 | appropriate |
| 28. The ideal profile of the candidate patient for prolonged DAPT is: | ||||
| 28.a. A patient with CCS post IM. without high hemorrhagic risk. multivessel | 9 | 1 | 7.60 | appropriate |
| 28.b. A patient with post-MI CCS. without high hemorrhagic risk. at high residual ischemic risk by clinical characteristics (diabetes mellitus. chronic renal failure. recurrent acute events. multivessel atherosclerosis) | 9 | 1 | 8.35 | appropriate |
| 28.c. A patient with post-MI CCS. without high hemorrhagic risk. at high residual ischemic risk by procedural characteristics of percutaneous revascularization (main stem lesions; three or more lesions; implantation of three or more stents; bifurcation treatment with two stents; treatment of chronic occlusions or venous grafts; total stent length >60 mm) | 9 | 1 | 8.35 | appropriate |
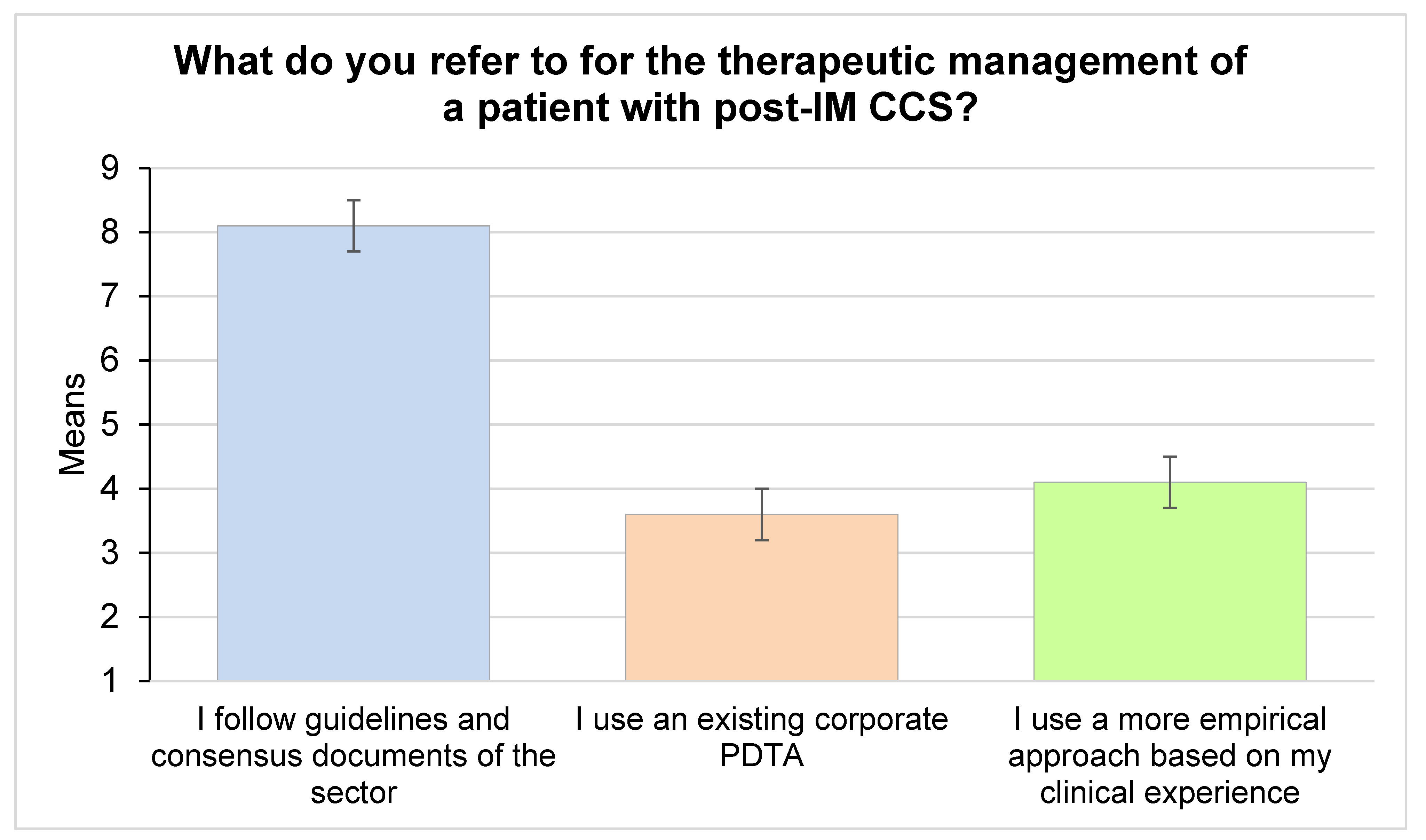
| 32. What do you refer to for the therapeutic management of a patient with post-MI CCS? | ||||
| 32.a. I follow guidelines and consensus documents of the sector | 9 | 1 | 7.60 | appropriate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Caterina, R.; Calabrò, P.; Campo, G.; Rossini, R.; Giubilato, S. A Therapeutic Pathway in Patients with Chronic Coronary Syndromes: Proposal for Optimization. J. Clin. Med. 2022, 11, 2091. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082091
De Caterina R, Calabrò P, Campo G, Rossini R, Giubilato S. A Therapeutic Pathway in Patients with Chronic Coronary Syndromes: Proposal for Optimization. Journal of Clinical Medicine. 2022; 11(8):2091. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082091
Chicago/Turabian StyleDe Caterina, Raffaele, Paolo Calabrò, Gianluca Campo, Roberta Rossini, and Simona Giubilato. 2022. "A Therapeutic Pathway in Patients with Chronic Coronary Syndromes: Proposal for Optimization" Journal of Clinical Medicine 11, no. 8: 2091. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082091