
Combined Radiographic Features and Age Can Distinguish Mycoplasma pneumoniae Pneumonia from Other Bacterial Pneumonias: Analysis Using the 16S rRNA Gene Sequencing Data

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Participants
2.2. Diagnostic Criteria for CAP and Atypical Pneumonia
2.3. Sample Collection
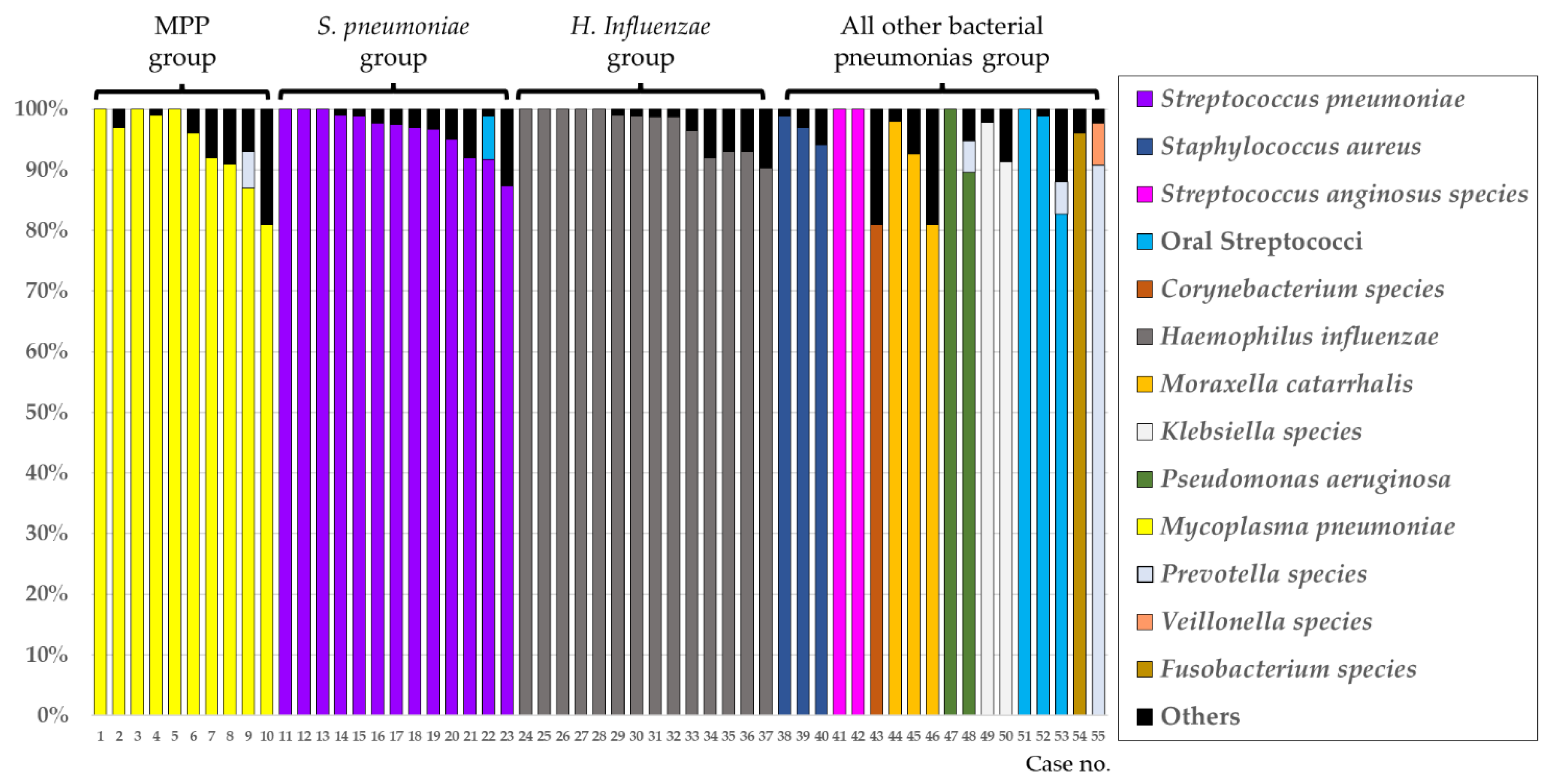
2.4. Evaluation of Lung Bacterial Flora Using the 16S Ribosomal RNA Gene Analysis
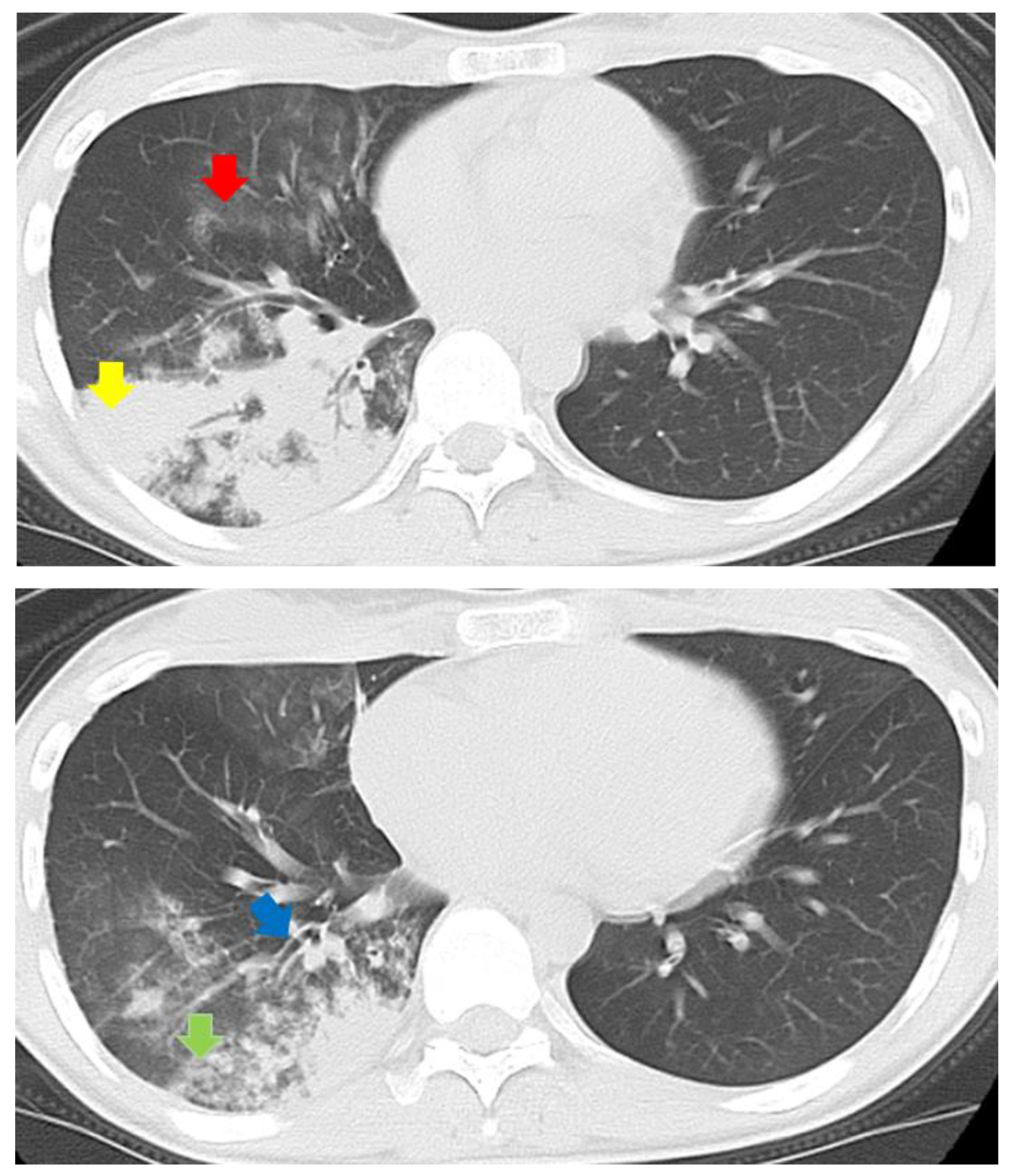
2.5. Evaluation of Chest CT Findings
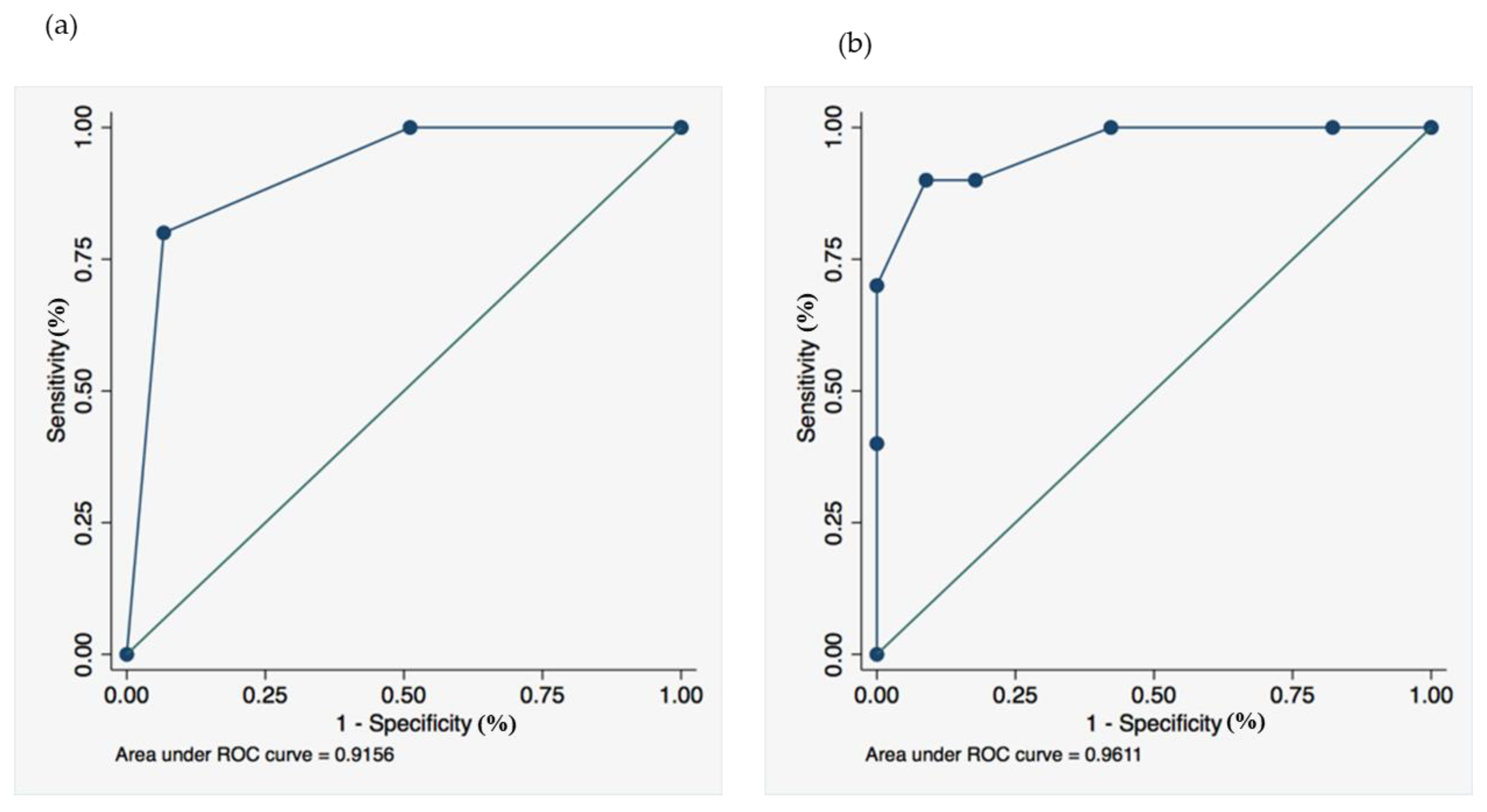
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yanagihara, K.; Kadota, J.; Aoki, N.; Matsumoto, T.; Yoshida, M.; Yagisawa, M.; Oguri, T.; Sato, J.; Ogasawara, K.; Wakamura, T.; et al. Nationwide surveillance of bacterial respiratory pathogens conducted by the surveillance committee of Japanese Society of Chemotherapy, the Japanese Association for Infectious Diseases, and the Japanese Society for Clinical Microbiology in 2010: General view of the pathogens’ antibacterial susceptibility. J. Infect. Chemother. 2015, 21, 410–420. [Google Scholar] [PubMed] [Green Version]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64 (Suppl. 3), iii1–iii55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, T.; Miyashita, N.; Nakahama, C. Clinical differentiation of atypical pneumonia using Japanese guidelines. Respirology 2007, 12, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, N.; Sugiu, T.; Kawai, Y.; Oda, K.; Yamaguchi, T.; Ouchi, K.; Kobashi, Y.; Oka, M. Radiographic features of Mycoplasma pneumoniae pneumonia: Differential diagnosis and performance timing. BMC Med. Imaging 2009, 9, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyashita, N.; Obase, Y.; Ouchi, K.; Kawasaki, K.; Kawai, Y.; Kobashi, Y.; Oka, M. Clinical features of severe Mycoplasma pneumoniae pneumonia in adults admitted to an intensive care unit. J. Med. Microbiol. 2007, 56, 1625–1629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamasaki, K.; Kawanami, T.; Yatera, K.; Fukuda, K.; Noguchi, S.; Nagata, S.; Nishida, C.; Kido, T.; Ishimoto, H.; Taniguchi, H.; et al. Significance of anaerobes and oral bacteria in community-acquired pneumonia. PLoS ONE 2013, 8, e63103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noguchi, S.; Mukae, H.; Kawanami, T.; Yamasaki, K.; Fukuda, K.; Akata, K.; Ishimoto, H.; Taniguchi, H.; Yatera, K. Bacteriological assessment of healthcare-associated pneumonia using a clone library analysis. PLoS ONE 2015, 10, e0124697. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Akata, K.; Yatera, K.; Yamasaki, K.; Kawanami, T.; Naito, K.; Noguchi, S.; Fukuda, K.; Ishimoto, H.; Taniguchi, H.; Mukae, H. The significance of oral streptococci in patients with pneumonia with risk factors for aspiration: The bacterial floral analysis of 16S ribosomal RNA gene using bronchoalveolar lavage fluid. BMC Pulm. Med. 2016, 16, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraya, T.; Ohkuma, K.; Tsukahara, Y.; Watanabe, T.; Kurai, D.; Ishii, H.; Kimura, H.; Goto, H.; Takizawa, H. Correlation between clinical features, high-resolution computed tomography findings, and a visual scoring system in patients with pneumonia due to Mycoplasma pneumoniae. Respir. Investig. 2018, 56, 320–325. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mycoplasma pneumoniae | Streptococcus pneumoniae | Haemophilus influenzae | All Other Bacterial Pneumonias * | p |
|---|---|---|---|---|---|
| (n = 10) | (n = 13) | (n = 14) | (n = 18) | ||
| Age (y); mean ± SD | 30.6 ± 17.0 | 72.9 ± 8.5 | 73.9 ± 11.7 | 65.7 ± 20.5 | <0.001 |
| Sex Female; n (%) | 6 (60) | 5 (38) | 9 (64) | 3 (17) | 0.029 |
| PSI risk | 0.059 | ||||
| 1–3 | 9 (90) | 8 (62) | 5 (36) | 9 (50) | |
| 4 | 0 (0) | 2 (15) | 8 (57) | 6 (33) | |
| 5 | 1 (10) | 3 (23) | 1 (7) | 3 (17) | |
| Comorbid diseases | |||||
| Malignancy | 0 | 3 | 1 | 4 | |
| COPD | 0 | 3 | 4 | 7 | |
| Bronchiectasis | 0 | 0 | 5 | 4 | |
| Interstitial pneumonia | 0 | 0 | 2 | 1 | |
| Cerebrovascular disease | 0 | 0 | 3 | 3 | |
| Diabetes mellitus | 0 | 4 | 3 | 2 | |
| Congestive heart disease | 0 | 0 | 4 | 0 | |
| Chronic kidney disease | 0 | 0 | 2 | 1 | |
| Chronic liver disease | 0 | 1 | 0 | 0 | |
| RA or Sjogren’s syndrome | 0 | 0 | 1 | 0 | |
| WBC (/uL) < 10,000 | 9 (90) | 5 (38) | 7 (50) | 6 (33) | 0.028 |
| The JRS Scoring for atypical pneumonia (≥4) | 9 (90) | 1 (8) | 1 (7) | 2 (11) | <0.001 |
| Chest CT Findings | Mycoplasma pneumoniae | Streptococcus pneumoniae | Haemophilus influenzae | All Other Bacterial Pneumonias * | p |
|---|---|---|---|---|---|
| (n = 10) | (n = 13) | (n = 14) | (n = 18) | ||
| Consolidation | 9 (90) | 10 (77) | 13 (93) | 15 (83) | 0.6572 |
| Grand-glass attenuation | 8 (80) | 5 (38) | 7 (50) | 10 (56) | 0.2515 |
| Centrilobular nodules | 9 (90) | 7 (54) | 8 (57) | 5 (28) | 0.0171 |
| Branchial wall thickening | 10 (100) | 9 (69) | 10 (71) | 11 (61) | 0.1670 |
| Reticular or liner opacity | 0 (0) | 5 (38) | 3 (21) | 2 (11) | 0.0889 |
| Pleural effusion | 5 (50) | 1 (8) | 6 (43) | 3 (17) | 0.0492 |
| Lymphadenopathy | 2 (20) | 5 (38) | 6 (43) | 1 (6) | 0.0627 |
| Variable | β Coefficient | Odds Ratio | 95% Confidence Interval | p | |
|---|---|---|---|---|---|
| Age (years) | |||||
| <60 | 3.95 | 52.2 | 4.97–547.11 | 0.001 | |
| 60 and more than 60 | – | – | – | ||
| CT findings | |||||
| Centrilobular nodules | 2.52 | 12.5 | 1.06–146.52 | 0.0446 | |
| 0 | 1 | |
|---|---|---|
| Age (years) | 60 and more than 60 | <60 |
| Centrilobular nodules | absent | present |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwanaga, Y.; Yamasaki, K.; Nemoto, K.; Akata, K.; Ikegami, H.; Uchimura, K.; Noguchi, S.; Nishida, C.; Kawanami, T.; Fukuda, K.; et al. Combined Radiographic Features and Age Can Distinguish Mycoplasma pneumoniae Pneumonia from Other Bacterial Pneumonias: Analysis Using the 16S rRNA Gene Sequencing Data. J. Clin. Med. 2022, 11, 2201. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082201
Iwanaga Y, Yamasaki K, Nemoto K, Akata K, Ikegami H, Uchimura K, Noguchi S, Nishida C, Kawanami T, Fukuda K, et al. Combined Radiographic Features and Age Can Distinguish Mycoplasma pneumoniae Pneumonia from Other Bacterial Pneumonias: Analysis Using the 16S rRNA Gene Sequencing Data. Journal of Clinical Medicine. 2022; 11(8):2201. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082201
Chicago/Turabian StyleIwanaga, Yuto, Kei Yamasaki, Kazuki Nemoto, Kentaro Akata, Hiroaki Ikegami, Keigo Uchimura, Shingo Noguchi, Chinatsu Nishida, Toshinori Kawanami, Kazumasa Fukuda, and et al. 2022. "Combined Radiographic Features and Age Can Distinguish Mycoplasma pneumoniae Pneumonia from Other Bacterial Pneumonias: Analysis Using the 16S rRNA Gene Sequencing Data" Journal of Clinical Medicine 11, no. 8: 2201. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082201