
Usefulness of Multi-Organ Point-of-Care Ultrasound as a Complement to the Decision-Making Process in Internal Medicine


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
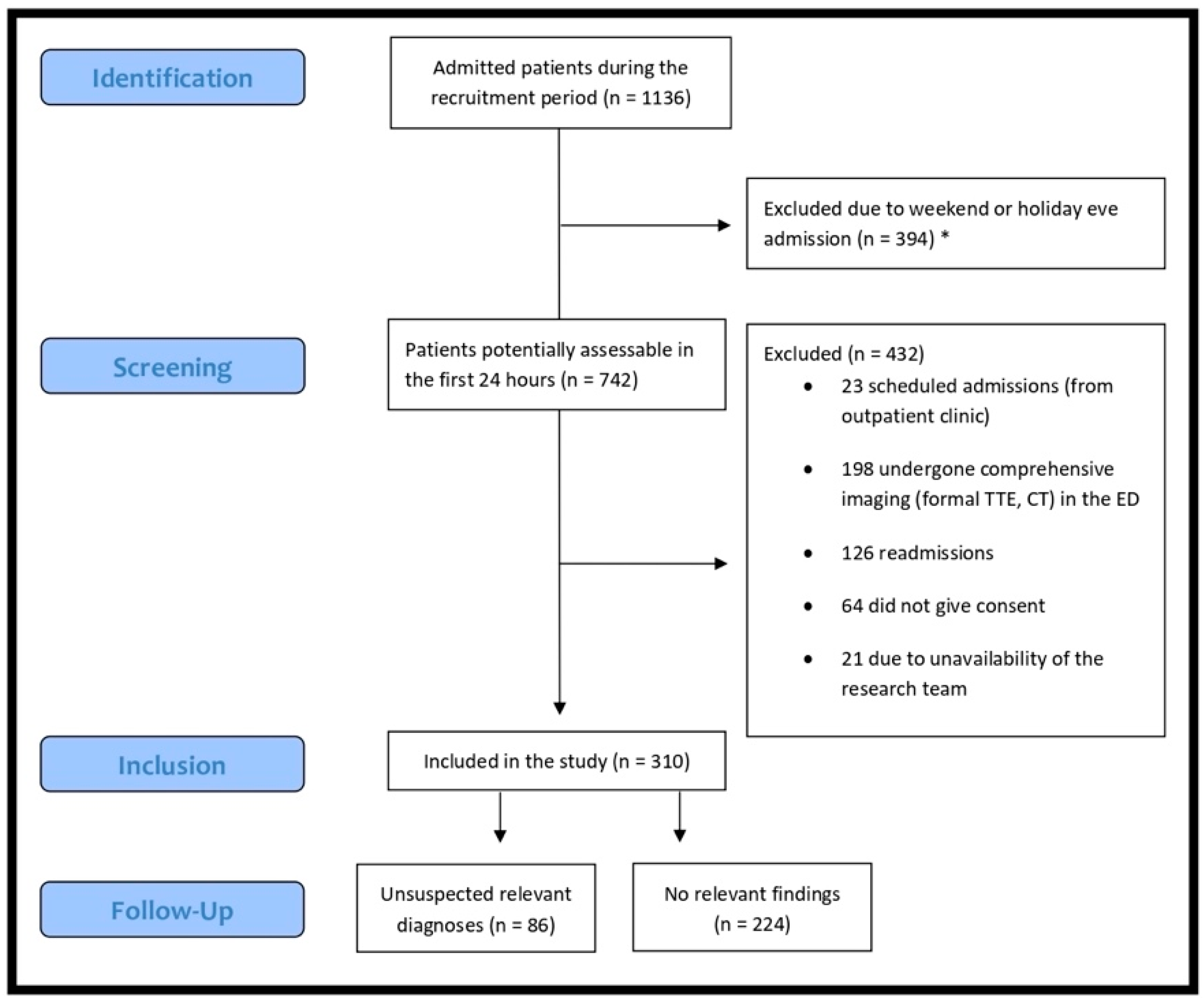
2.1. Patient Selection
2.2. Epidemiological, Clinical, Laboratory and Radiological Data Assessment
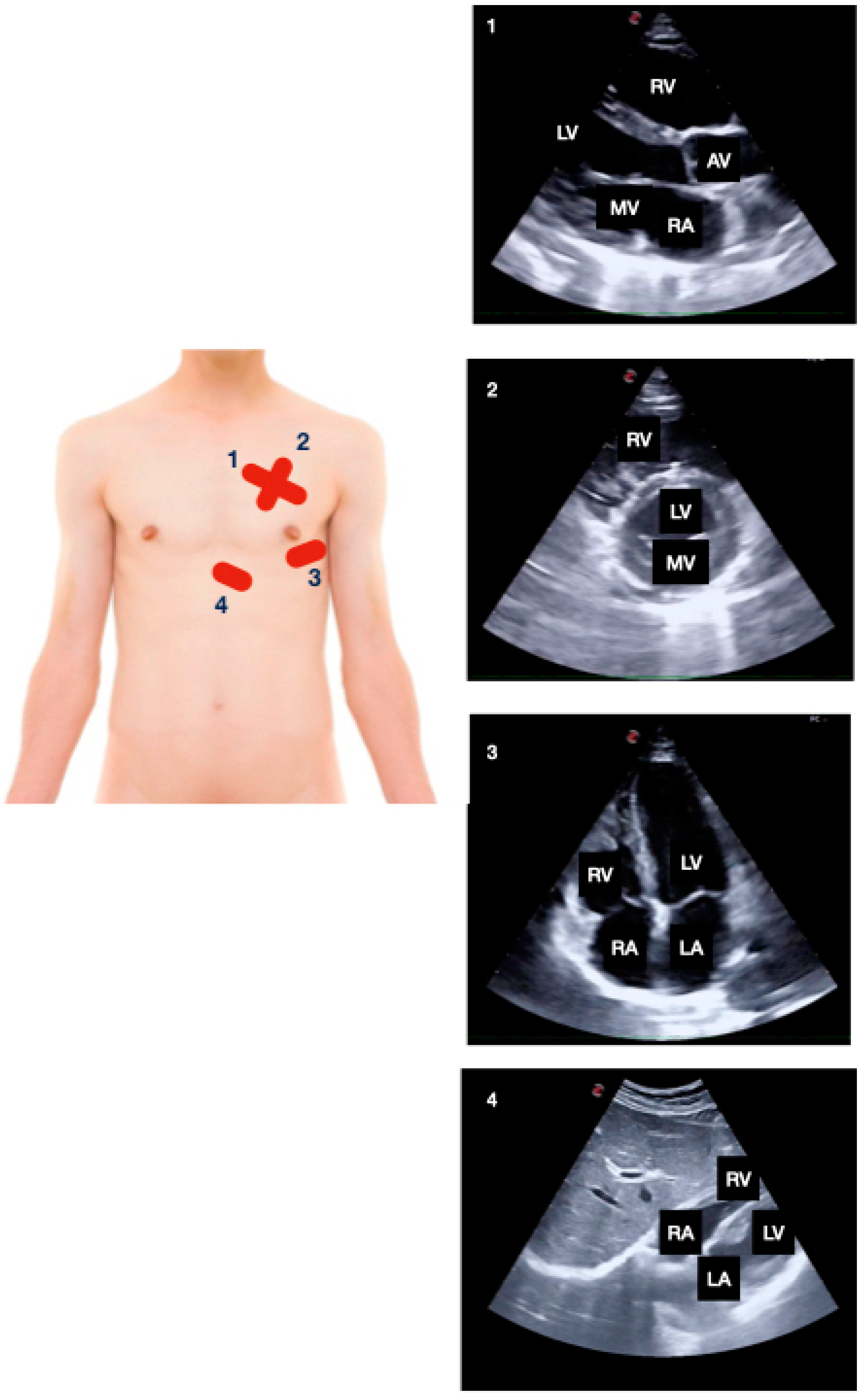
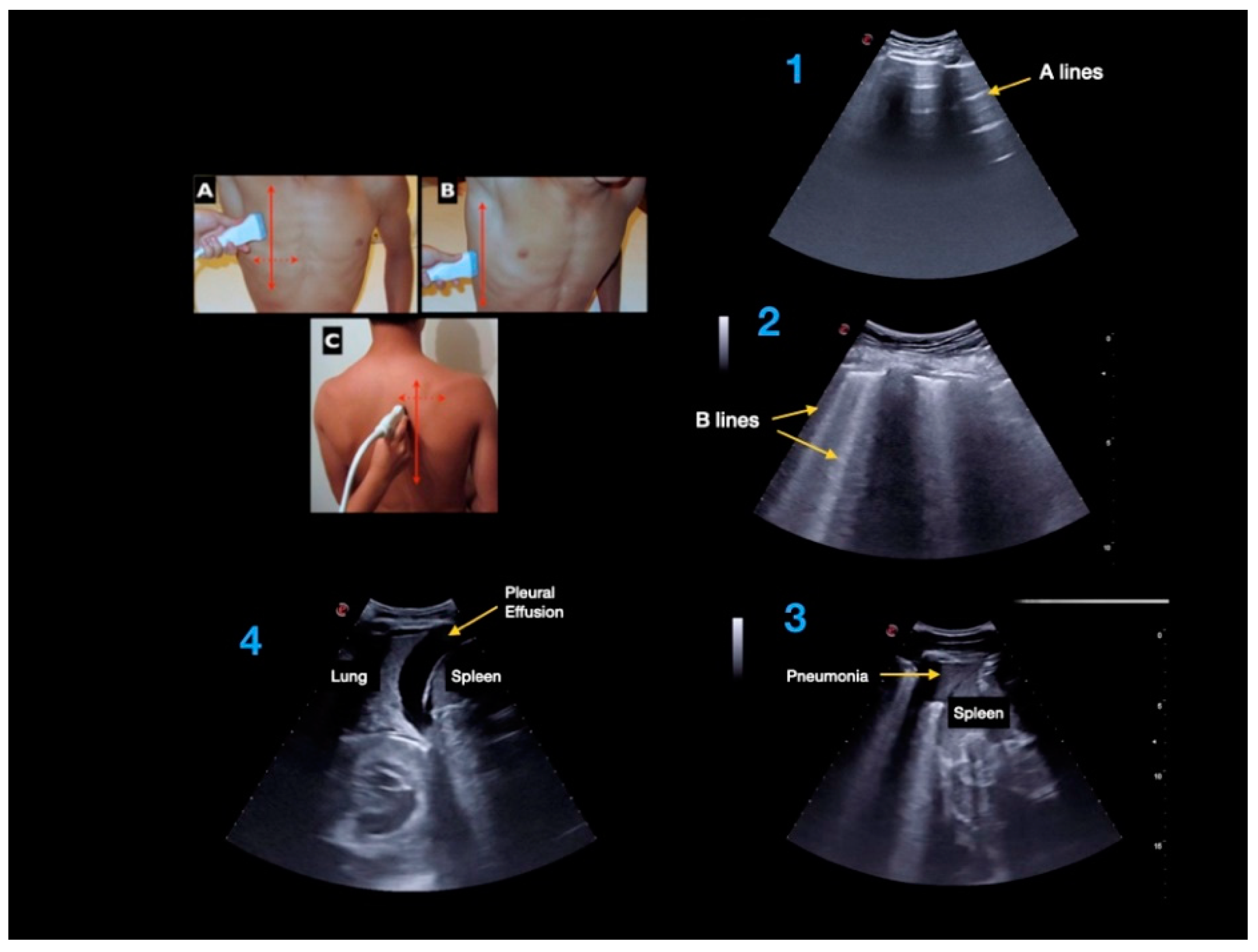
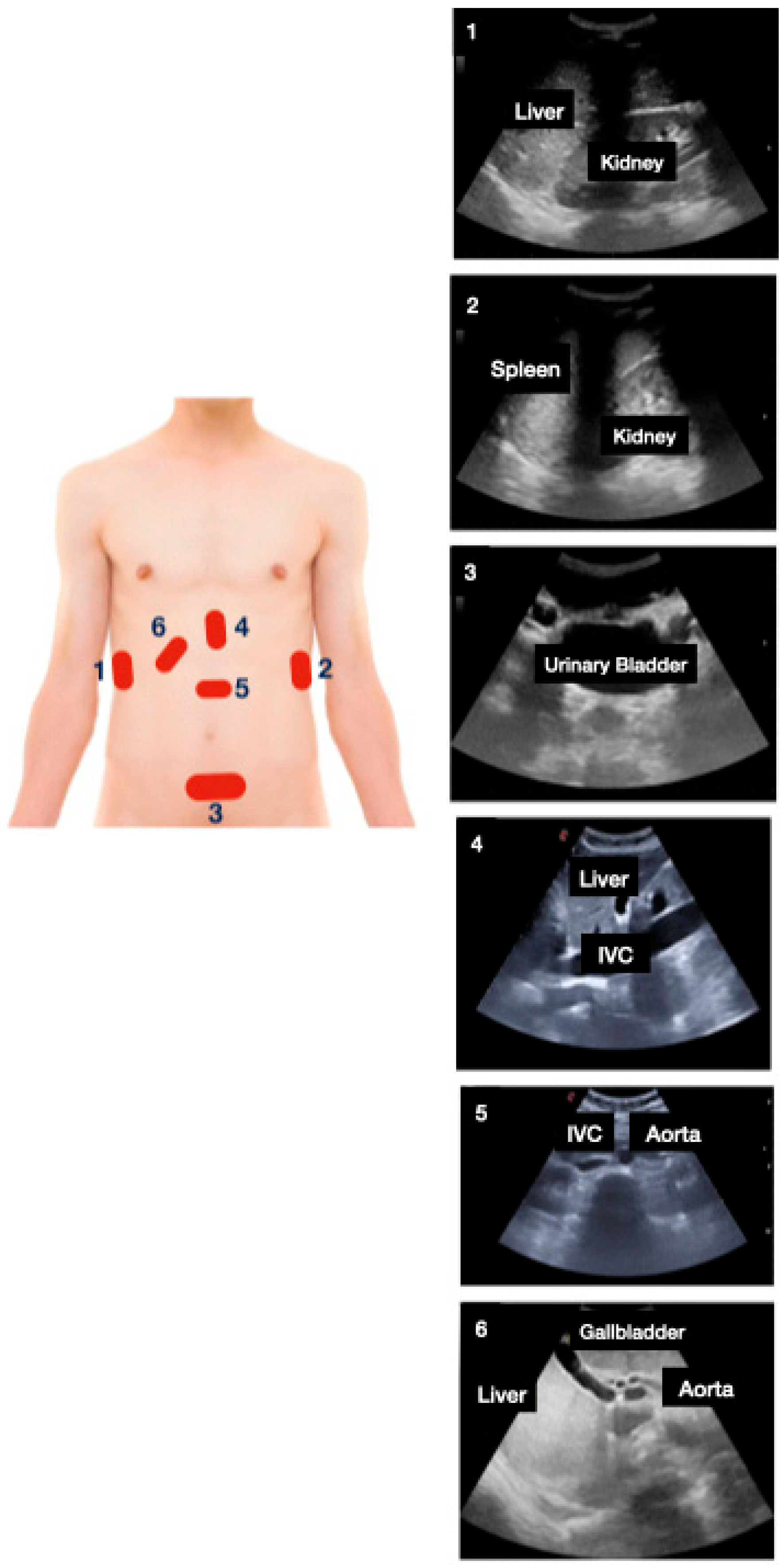
2.3. Ultrasound Data Collection
2.4. Outcome Measures and Definitions
2.5. Statistical Analysis
3. Results
4. Discussion
- Dyspnea is a very common reason for admission and multiorgan PoCUS might be especially useful [24,25,26,27]. In fact, acute heart failure and the detection of a significant cardiac abnormality (valvular heart disease, left ventricular systolic dysfunction, pulmonary hypertension) have accounted for a very high percentage of unsuspected diagnoses made by PoCUS.
- The high prevalence of relevant cardiac abnormalities, especially significant valve disease, is related to aging and frequently seen in admitted patients to the internal medicine wards.
- Lung ultrasound has allowed the diagnosis of a significant percentage of pneumonia and complicated pleural effusion. Especially in older patients, chest X-ray might not be accurate, and it can be difficult to visualize pneumonia located in the lower posterior regions of the lungs or whether a pleural effusion is complicated (i.e., presence of fibrous tracts) [28,29].
- Acute urinary retention is relatively common, and predominantly affects older men.
- It is important to explore the abdominal aorta in the presence of cardiovascular risk factors (i.e., smoking) [30].
- Excessive volume intake can lead to a systemic venous congestion in a short time, especially in malnourished individuals (i.e., low albumin levels). Lung ultrasound can aid in detecting signs of early congestion.
- As expected, older patients have higher probabilities of exhibiting unsuspected diagnoses through multi-organ PoCUS. The same happens with the level of dependency, although it is very likely that age might act as a cofounding factor.
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kimura, B.J.; Shaw, D.J.; Amundson, S.A.; Phan, J.N.; Blanchard, D.G.; DeMaria, A.N. Cardiac Limited Ultrasound Examination Techniques to Augment the Bedside Cardiac Physical Examination. J. Ultrasound. Med. 2015, 34, 1683–1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, B.J. Point-of-care cardiac ultrasound techniques in the physical examination: Better at the bedside. Heart 2017, 103, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Kobal, S.L.; Trento, L.; Baharami, S.; Tolstrup, K.; Naqvi, T.Z.; Cercek, B.; Neuman, Y.; Mirocha, J.; Kar, S.; Forrester, J.S.; et al. Comparison of effectiveness of hand-carried ultrasound to bedside cardiovascular physical examination. Am. J. Cardiol. 2005, 96, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Thomas, F.; Flint, N.; Setareh-Shenas, S.; Rader, F.; Kobal, S.L.; Siegel, R.J. Accuracy and Efficacy of Hand-Held Echocardiography in Diagnosing Valve Disease: A Systematic Review. Am. J. Med. 2018, 131, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Nelson, W.G.; Rosen, A.; Pronovost, P.J. Reengineering the Physical Examination for the New Millennium. JAMA 2016, 315, 2391–2392. [Google Scholar] [CrossRef] [PubMed]
- Narula, J.; Chandrashekhar, Y.; Braunwald, E. Time to Add a Fifth Pillar to Bedside Physical Examination: Inspection, Palpation, Percussion, Auscultation, and Insonation. JAMA Cardiol. 2018, 3, 346–350. [Google Scholar] [CrossRef]
- Perera, P.; Mailhot, T.; Riley, D.; Mandavia, D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med. Clin. N. Am. 2010, 28, 29–56. [Google Scholar] [CrossRef] [PubMed]
- Milne, J.; Atkinson, P.; Lewis, D.; Fraser, J.; Diegelmann, L.; Olszynski, P.; Stander, M.; Lamprecht, H. Sonography in Hypotension and Cardiac Arrest (SHoC): Rates of Abnormal Findings in Undifferentiated Hypotension and During Cardiac Arrest as a Basis for Consensus on a Hierarchical Point of Care Ultrasound Protocol. Cureus 2016, 8, e564. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [Green Version]
- Russell, F.M.; Ehrman, R.; Cosby, K.; Ansari, A.; Tseeng, S.; Christain, E.; Bailitz, J. Diagnosing acute heart failure in patients with undifferentiated dyspnea: A lung and cardiac ultrasound (LuCUS) protocol. Acad. Emerg. Med. 2015, 22, 182–191. [Google Scholar] [CrossRef] [Green Version]
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavattone, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, J.H.; Frederiksen, C.A.; Juhl-Olsen, P.; Sloth, E. Perioperative use of focus assessed transthoracic echocardiography (FATE). Anesth. Analg. 2012, 115, 1029–1032. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Goudie, A.; Chiorean, L.; Cui, X.W.; Gilja, O.H.; Dong, Y.; Abramowicz, J.S.; Vinayak, S.; Westerway, S.C.; Nolsøe, C.P.; et al. Point of Care Ultrasound: A WFUMB Position Paper. Ultrasound. Med. Biol. 2017, 43, 49–58. [Google Scholar] [CrossRef] [PubMed]
- García de Casasola, G.; Casado López, I.; Torres-Macho, J. Clinical ultrasonography in the decision-making process in medicine point-of-care ultrasound in clinical decision making. Rev. Clin. Esp. 2020, 220, 49–56. [Google Scholar] [CrossRef]
- Zieleskiewicz, L.; Lopez, A.; Hraiech, S.; Baumstarck, K.; Pastene, B.; Di Bisceglie, M.; Coiffard, B.; Duclos, G.; Boussuges, A.; Bobbia, X.; et al. Bedside POCUS during ward emergencies is associated with improved diagnosis and outcome: An observational, prospective, controlled study. Crit. Care 2021, 25, 34. [Google Scholar] [CrossRef]
- Weile, J.; Frederiksen, C.A.; Laursen, C.B.; Graumann, O.; Sloth, E.; Kirkegaard, H. Point-of-care ultrasound induced changes in management of unselected patients in the emergency department—A prospective single-blinded observational trial. Scand. J. Trauma. Resusc. Emerg. Med. 2020, 28, 47. [Google Scholar] [CrossRef]
- Weile, J.; Laursen, C.B.; Frederiksen, C.A.; Graumann, O.; Sloth, E.; Kirkegaard, H. Point-of-care ultrasound findings in unselected patients in an emergency department-results from a prospective observational trial. BMC Emerg. Med. 2018, 18, 60. [Google Scholar] [CrossRef] [Green Version]
- Killu, K.; Coba, V.; Mendez, M.; Reddy, S.; Adrzejewski, T.; Huang, Y.; Ede, J.; Horst, M. Model Point-of-Care Ultrasound Curriculum in an Intensive Care Unit Fellowship Program and Its Impact on Patient Management. Crit. Care Res. Pract. 2014, 2014, 934796. [Google Scholar] [CrossRef] [Green Version]
- Denault, A.; Canty, D.J. Whole-body ultrasound in the intensive care unit. ICU Manag. Pract. 2018, 18, 244–252. [Google Scholar]
- Tavares, J.; Ivo, R.; Gonzalez, F.; Lamas, T.; Mendes, J.J. Global Ultrasound Check for the Critically lll (GUCCI)-a new systematized protocol unifying point-of-care ultrasound in critically ill patients based on clinical presentation. Open Access Emerg. Med. 2019, 11, 133–145. [Google Scholar] [CrossRef] [Green Version]
- Cid-Serra, X.; Hoang, W.; El-Ansary, D.; Canty, D.; Royse, A.; Royse, C. Clinical Impact of Point-of-Care Ultrasound in Internal Medicine Inpatients: A Systematic Review. Ultrasound. Med. Biol 2022, 48, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Riishede, M.; Lassen, A.T.; Baatrup, G.; Pietersen, P.I.; Jacobsen, N.; Jeschke, K.N.; Laursen, C.B. Point-of-care ultrasound of the heart and lungs in patients with respiratory failure: A pragmatic randomized controlled multicenter trial. Scand. J. Trauma. Resusc. Emerg. Med. 2021, 29, 60. [Google Scholar] [CrossRef] [PubMed]
- Zare, M.A.; Bahmani, A.; Fathi, M.; Arefi, M.; Hossein Sarbazi, A.; Teimoori, M. Role of point-of-care ultrasound study in early disposition of patients with undifferentiated acute dyspnea in emergency department: A multi-center prospective study. J. Ultrasound. 2021. [Google Scholar] [CrossRef]
- Kirschner, J.M.; Hunter, B.R. In acute dyspnea with diagnostic uncertainty, ACP suggests POCUS may be added to the standard diagnostic pathway. Ann Intern. Med. 2021, 174, JC99. [Google Scholar] [CrossRef] [PubMed]
- Staub, L.J.; Mazzali Biscaro, R.R.; Kaszubowski, E.; Maurici, R. Lung Ultrasound for the Emergency Diagnosis of Pneumonia, Acute Heart Failure, and Exacerbations of Chronic Obstructive Pulmonary Disease/Asthma in Adults: A Systematic Review and Meta-analysis. J. Emerg. Med. 2019, 56, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; DeSanto, K.; Platz, E.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults With Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Zanobetti, M.; Scorpiniti, M.; Gigli, C.; Nazerian, P.; Vanni, S.; Innocenti, F.; Stefanone, V.T.; Savinelli, C.; Coppa, A.; Bigiarini, S.; et al. Point-of-Care Ultrasonography for Evaluation of Acute Dyspnea in the ED. Chest 2017, 151, 1295–1301. [Google Scholar] [CrossRef]
- Orso, D.; Guglielmo, N.; Copetti, R. Lung ultrasound in diagnosing pneumonia in the emergency department: A systematic review and meta-analysis. Eur. J. Emerg. Med. 2018, 25, 312–321. [Google Scholar] [CrossRef]
- Alzahrani, S.A.; Al-Salamah, M.A.; Al-Madani, W.H.; Elbarbary, M.A. Systematic review and meta-analysis for the use of ultrasound versus radiology in diagnosing of pneumonia. Crit Ultrasound. J. 2017, 9, 6. [Google Scholar] [CrossRef] [Green Version]
- Lahoz, C.; Gracia, C.E.; García, L.R.; Bellmunt-Montoya, S.; Hernando Ángel, B.; Heredero Álvaro, F.; Tembra, M.S.; Velasco, M.B.; Guijarro, C.; Ruiz, E.B.; et al. Recomendaciones de la guía para el diagnóstico y tratamiento del aneurisma de aorta abdominal. Clin. Investig. Arterioscler. 2015, 27, 159–165. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Gender (male)—N (%) | 149 (48.7) |
| Age (years) mean (SD) | 70.5 (18) |
| Past Medical History | N (%) |
| Diabetes mellitus—N (%) | 32 (10.3) |
| Body mass index (kg/m2) mean (SD) | 27.6 (5.6) |
| Smoking habit—N (%) | 59 (19.2) |
| Excessive alcohol consumption (>20 g/day)—N (%) | 32 (10.3%) |
| Barthel index mean (SD) | 78 (29) |
| Moderate to high disability (Barthel index < 60)—N (%) | 86 (27.7%) |
| Physical Exam | |
| SBP (mmHg) mean (SD) | 130 (21) |
| DBP (mmHg) mean (SD) | 71 (14) |
| Heart rate (bpm) mean (SD) | 82 (16) |
| SO2 (%) mean (SD) | 94 (3) |
| Reason for Admission | N (%) * |
|---|---|
| Lower respiratory tract infection | 91 (29.3) |
| Acute heart failure | 52 (16.8) |
| UTI | 35 (11.3) |
| COPD exacerbation | 28 (9) |
| Infectious diseases (non-respiratory or UTI) | 11 (3.5) |
| Chronic respiratoria exacerbation (non-COPD) | 9 (2.9) |
| VTE disease | 8 (2.6) |
| Gastrointestinal pathology (hepatitis, cholecystitis, cholangitis) | 7 (2.3) |
| Cardiac arrythmia | 4 (1.3) |
| Cerebrovascular disease | 3 (1) |
| Other diagnosis | 92 (29.6) |
| Final Diagnosis | N (%) |
|---|---|
| Significant valvular disease (unknown) | 15 (4.8) |
| Heart failure | 14 (4.5) |
| Pneumonia | 14 (4.5) |
| Acute urinary retention | 10 (3.2) |
| Congestive status | 9 (2.9) |
| Severe pulmonary hypertension (unknown) | 8 (2.6) |
| Moderate to severe systolic dysfunction (unknown) | 5 (1.6) |
| Abdominal aorta aneurism | 5 (1.6) |
| Hydronephrosis | 7 (2.2) |
| Lung interstitial disease (unknown) | 4 (1.3) |
| Complicated pleural effusion (empyema) | 4 (1.3) |
| Moderate to severe pericardial effusion | 4 (1.3) |
| Metastatic liver | 3 (0.9) |
| Oher diagnosis | 10 (3.2) |
| Age Stratification | N (%) | Unsuspected Diagnosis | Risk (%) | Relative Risk | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| <56 | 64 (20.6) | 11 | 17.1 | 1 | ||
| 56–69 | 65 (21.0) | 15 | 23.07 | 1.32 | 0.7 | 2.65 |
| 70–79 | 62 (20.0) | 17 | 27.42 | 1.57 | 0.8 | 3.08 |
| 79–87 | 59 (19.0) | 16 | 27.11 | 1.55 | 0.8 | 3.07 |
| 87–100 | 60 (19.4) | 30 | 50 | 2.91 | 1.61 | 5.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casado-López, I.; Tung-Chen, Y.; Torres-Arrese, M.; Luordo-Tedesco, D.; Mata-Martínez, A.; Casas-Rojo, J.M.; Montero-Hernández, E.; García De Casasola-Sánchez, G. Usefulness of Multi-Organ Point-of-Care Ultrasound as a Complement to the Decision-Making Process in Internal Medicine. J. Clin. Med. 2022, 11, 2256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082256
Casado-López I, Tung-Chen Y, Torres-Arrese M, Luordo-Tedesco D, Mata-Martínez A, Casas-Rojo JM, Montero-Hernández E, García De Casasola-Sánchez G. Usefulness of Multi-Organ Point-of-Care Ultrasound as a Complement to the Decision-Making Process in Internal Medicine. Journal of Clinical Medicine. 2022; 11(8):2256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082256
Chicago/Turabian StyleCasado-López, Irene, Yale Tung-Chen, Marta Torres-Arrese, Davide Luordo-Tedesco, Arantzazu Mata-Martínez, Jose Manuel Casas-Rojo, Esther Montero-Hernández, and Gonzalo García De Casasola-Sánchez. 2022. "Usefulness of Multi-Organ Point-of-Care Ultrasound as a Complement to the Decision-Making Process in Internal Medicine" Journal of Clinical Medicine 11, no. 8: 2256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11082256