
Robotic Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis

 ,
,  , , , , , ,
, , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Searches
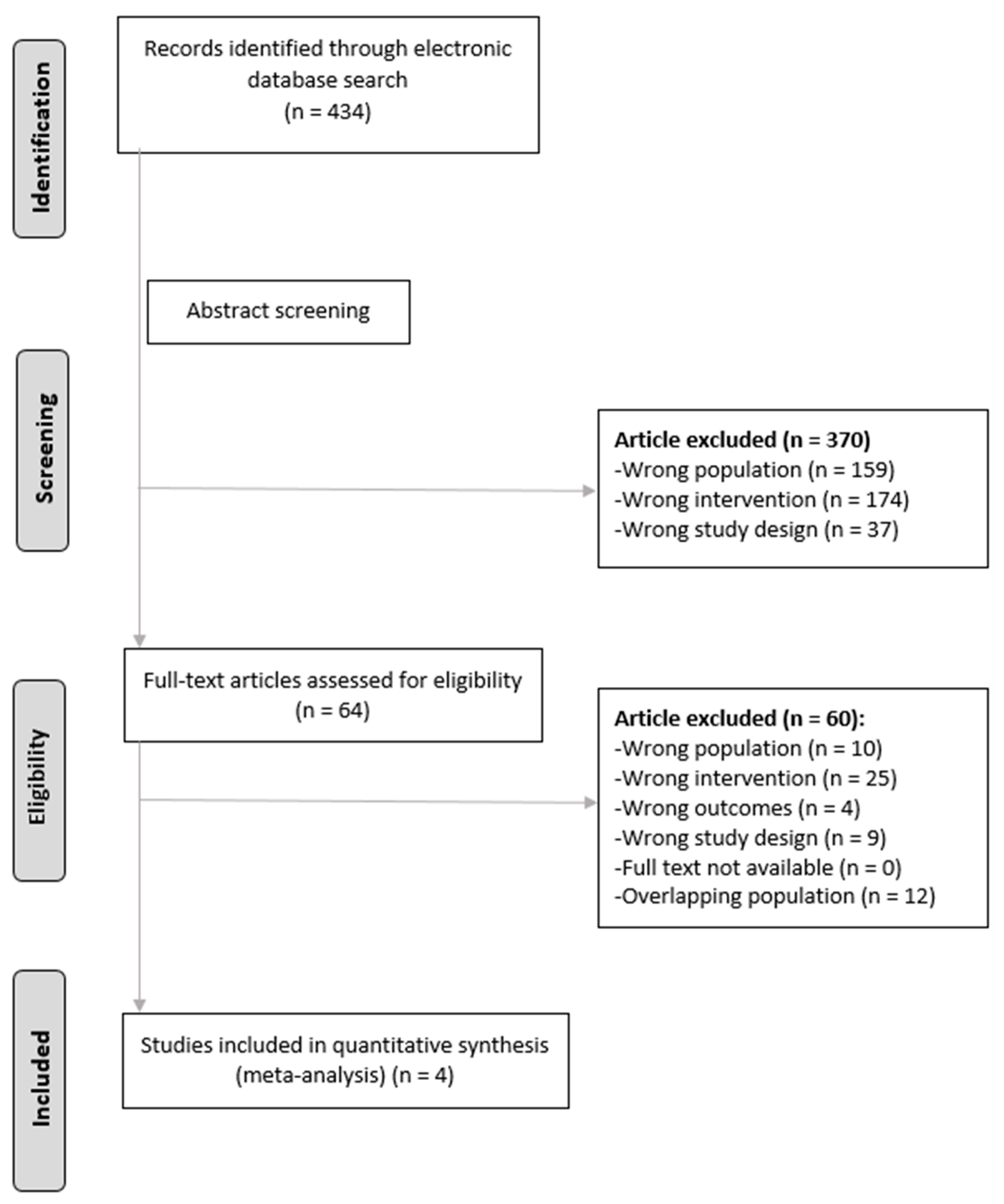
2.3. Study Selection
2.4. Data Collection and Management
2.5. Author Contact
2.6. Risk of Bias in Individual Studies
2.7. Statistical Analyses
2.8. Online Resource
3. Results
3.1. Overall Characteristics
3.2. Studies Reporting Outcomes of Donors
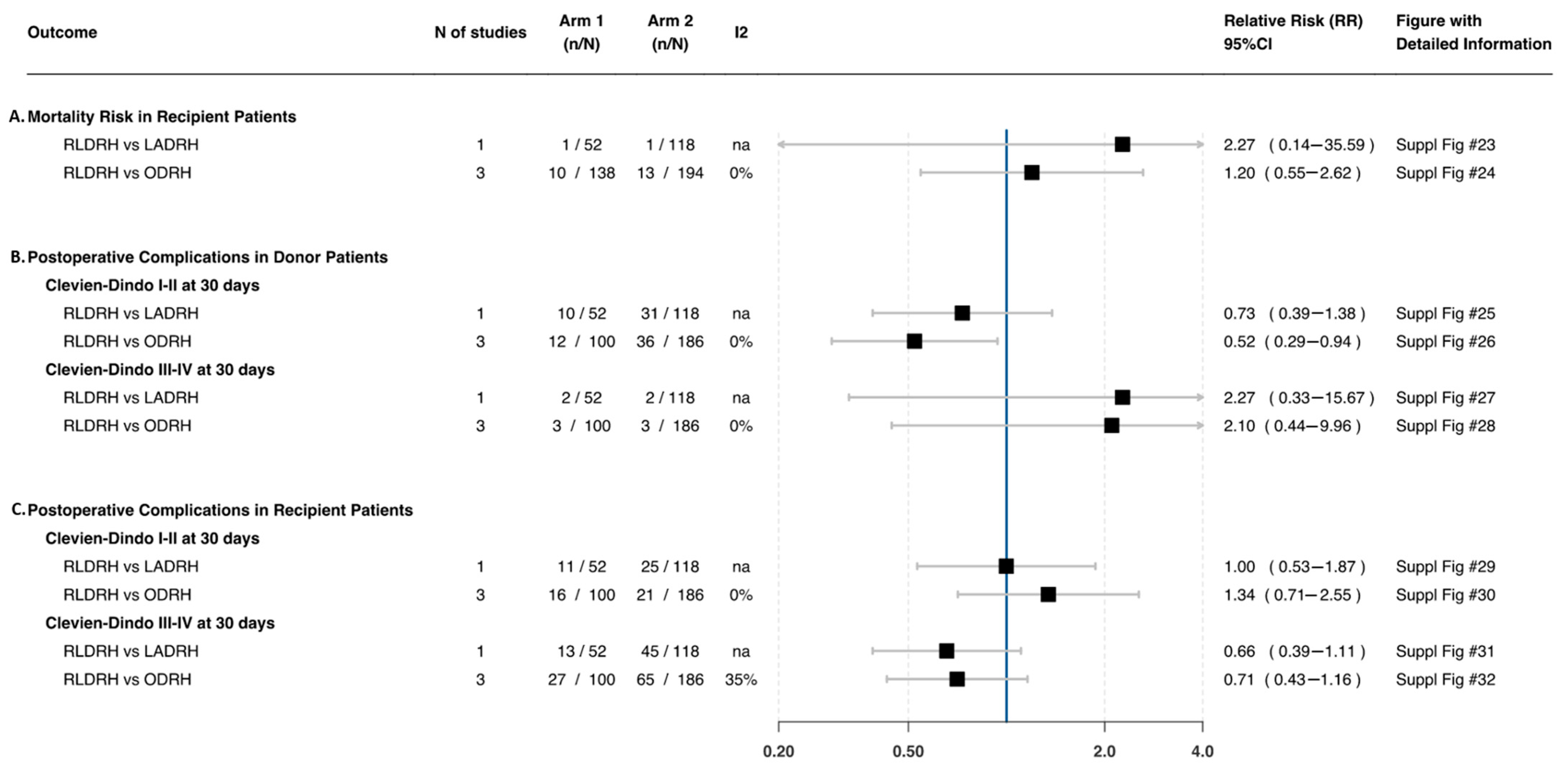
3.2.1. Patient Important Outcomes
Clavien–Dindo Complications I–II
Clavien–Dindo Complications III–IV
Mortality
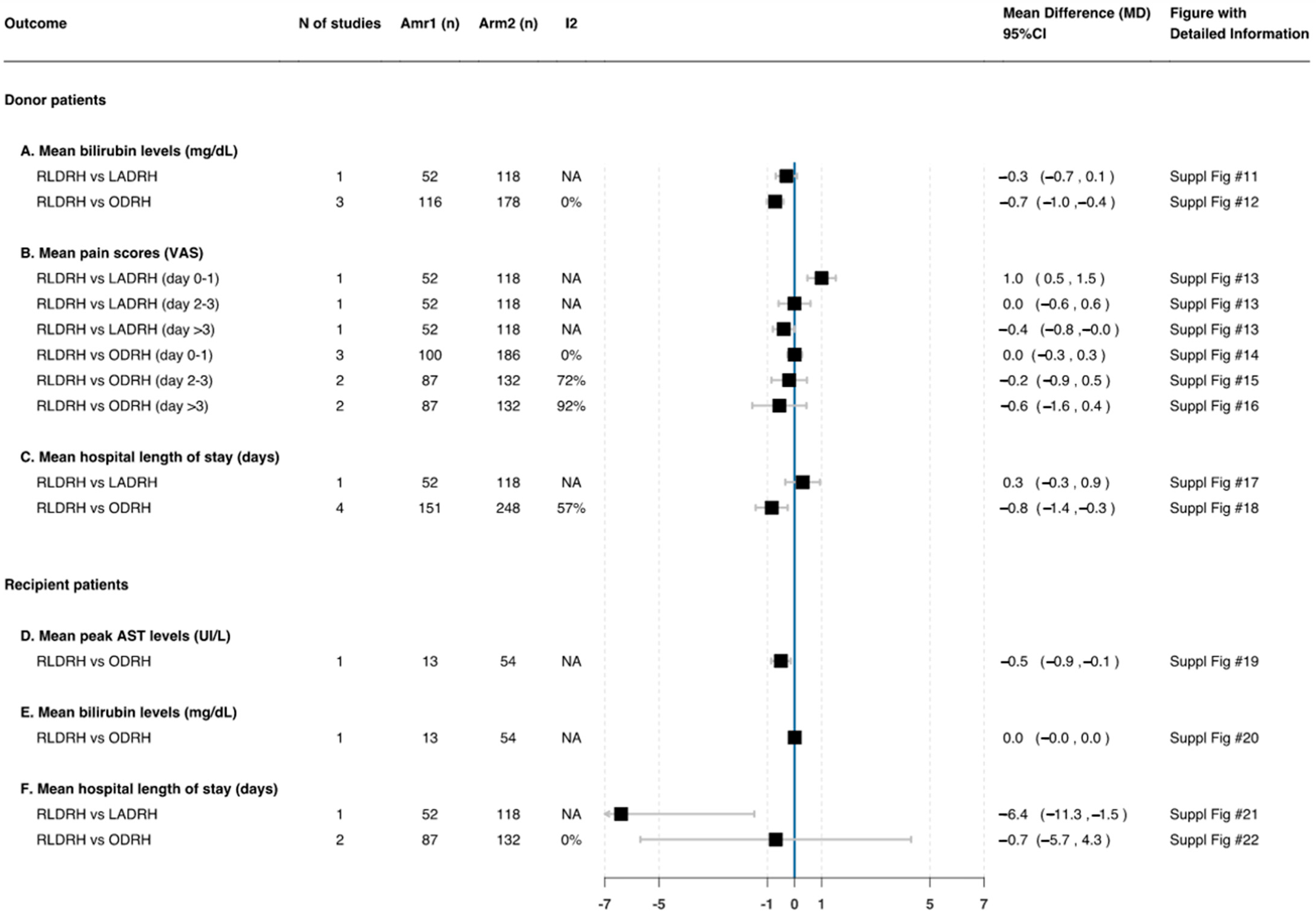
Postoperative Pain (Visual Analogue Scale)
3.2.2. Secondary Outcomes
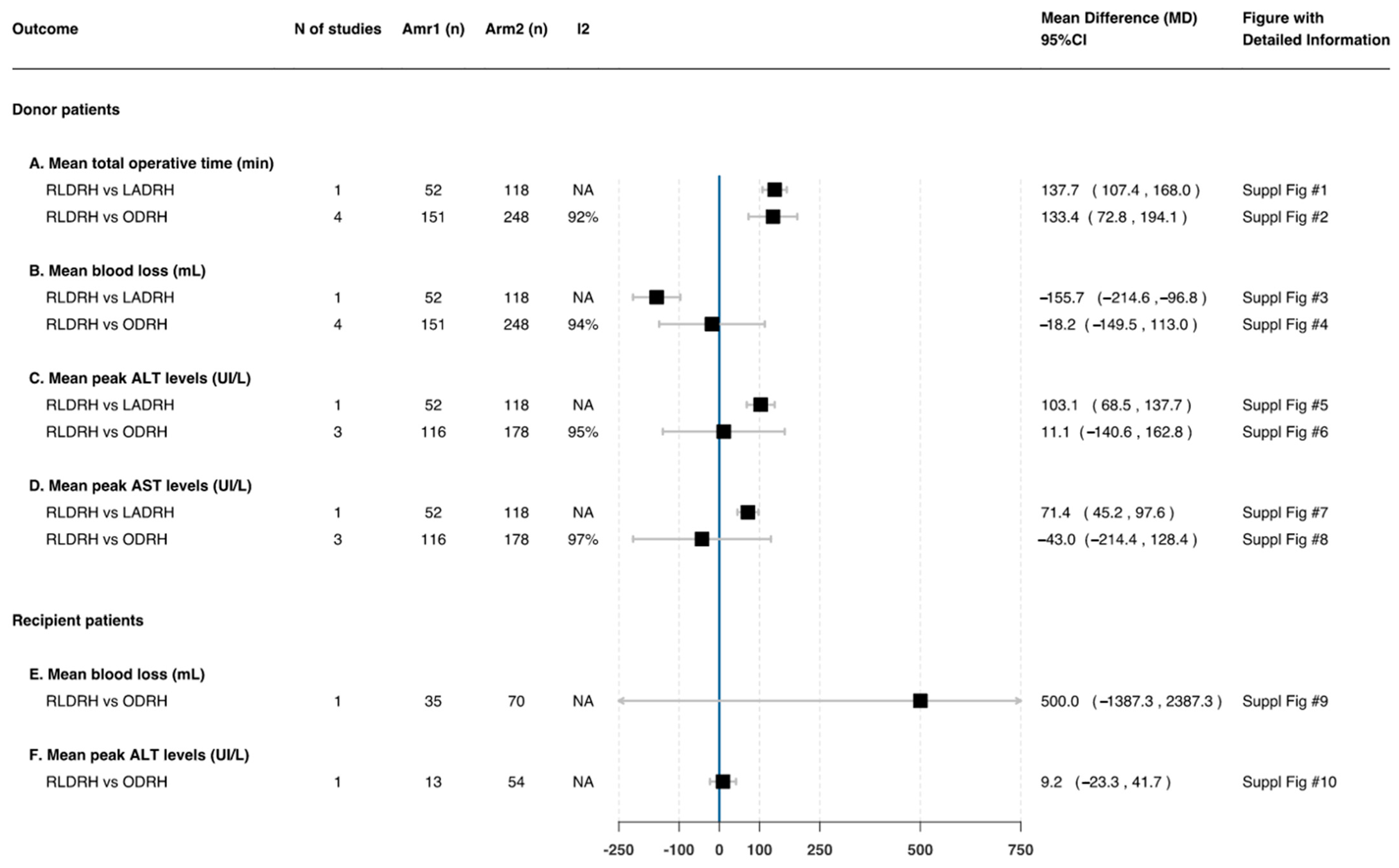
Operative Time (Min)
Estimated Blood Loss (mL)
Postoperative Liver Function
Length of Hospital Stay (Days)
3.3. Studies Reporting Outcomes of Recipients
3.3.1. Patient Important Outcomes
Clavien–Dindo Complications I–II
Clavien–Dindo Complications III–IV
Mortality
3.3.2. Secondary Outcomes
Estimated Blood Loss (mL)
Postoperative Liver Function
Length of Hospital Stay (Days)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Åberg, F. Quality of life after liver transplantation. Best Pract. Res. Clin. Gastroenterol. 2020, 46–47, 101684. [Google Scholar] [CrossRef] [PubMed]
- Goldaracena, N.; Barbas, A.S. Living donor liver transplantation. Curr. Opin. Organ. Transpl. 2019, 24, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Soubrane, O.; Eguchi, S.; Uemoto, S.; Kwon, C.H.D.; Wakabayashi, G.; Han, H.S.; Kim, K.H.; Troisi, R.I.; Cherqui, D.; Rotellar, F.; et al. Minimally Invasive Donor Hepatectomy for Adult Living Donor Liver Transplantation. Ann. Surg. 2022, 275, 166–174. [Google Scholar] [CrossRef]
- Gruttadauria, S.; Pagano, D.; Cintorino, D.; Arcadipane, A.; Traina, M.; Volpes, R.; Luca, A.; Vizzini, G.; Gridelli, B.; Spada, M. Right hepatic lobe living donation: A 12 years single Italian center experience. World J. Gastroenterol. 2013, 19, 6353–6359. [Google Scholar] [CrossRef] [PubMed]
- Buell, J.F.; Cherqui, D.; Geller, D.A.; O’Rourke, N.; Iannitti, D.; Dagher, I.; Koffron, A.J.; Thomas, M.; Gayet, B.; Han, H.S.; et al. The international position on laparoscopic liver surgery: The Louisville Statement, 2008. Ann. Surg. 2009, 250, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Cherqui, D.; Soubrane, O.; Husson, E.; Barshasz, E.; Vignaux, O.; Ghimouz, M.; Branchereau, S.; Chardot, C.; Gauthier, F.; Fagniez, P.L.; et al. Laparoscopic living donor hepatectomy for liver transplantation in children. Lancet 2002, 359, 392–396. [Google Scholar] [CrossRef]
- Scatton, O.; Katsanos, G.; Boillot, O.; Goumard, C.; Bernard, D.; Stenard, F.; Perdigao, F.; Soubrane, O. Pure laparoscopic left lateral sectionectomy in living donors: From innovation to development in France. Ann. Surg. 2015, 261, 506–512. [Google Scholar] [CrossRef]
- Zhang, W.; Xu, L.; Zhang, J.; Che, X. Safety and feasibility of laparoscopic living donor right hepatectomy for adult liver transplantation: A meta-analysis. HPB 2021, 23, 344–358. [Google Scholar] [CrossRef]
- Chen, P.-D.; Wu, C.-Y.; Wu, Y.-M. Use of robotics in liver donor right hepatectomy. Hepato. Surg. Nutr. 2017, 6, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Giulianotti, P.C.; Coratti, A.; Angelini, M.; Sbrana, F.; Cecconi, S.; Balestracci, T.; Caravaglios, G. Robotics in general surgery. Arch. Surg. 2003, 138, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Lincango-Naranjo, E.; Garces-Delgado, E.; Solis-Pazmino, P.; Alexander-Leon, H.; Restrepo-Rodas, G.; Mancero-Montalvo, R.; Ponce, C.J.; Cadena-Semanate, R.; Vargas-Cordova, R.; Herrera-Cevallos, G.; et al. Outcomes of Robotic Living Donor Right Hepatectomy in Liver Transplant Recipients: A Systematic Review and Meta-analysis—ATC Abstracts. Am. J. Transpl. 2021, 21 (Suppl. 3), 774. Available online: https://atcmeetingabstracts.com/abstract/outcomes-of-robotic-living-donor-right-hepatectomy-in-liver-transplant-recipients-a-systematic-review-and-meta-analysis/ (accessed on 29 August 2021).
- Lincango-Naranjo, E.; Garces-Delgado, E.; Solis-Pazmino, P.; Alexander-Leon, H.; Vargas-Cordova, R.; Vallejo, S.; Liu-Sanchez, C.; Guerron, A.D.; Ponce, O.J.; Moris, D. Safety of Robotic Living Donor Right Hepatectomy (RLDRH) in Donor Patients: A Systematic Review and Meta-analysis. J. Am. Coll. Surg. 2021, 233, e195. [Google Scholar] [CrossRef]
- Lincango-Naranjo, E.; Garces-Delgado, E.; Ponce-Ontaneda, C.; Restrepo-Rodas, G.; Mancero-Montalvo, R.; Cadena-Semanate, R.; Leon, H.; Vargas-Cordova, R.; Herrera-Cevallos, G.; Vallejo, S.; et al. Robotic Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis. PROSPERO 2020 CRD42020214313. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020214313 (accessed on 10 November 2019).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, 50931. [Google Scholar] [CrossRef] [PubMed]
- DistillerSR: Systematic Review and Literature Review Software by Evidence Partners. Available online: https://www.evidencepartners.com/products/distillersr-systematic-review-software/ (accessed on 10 November 2019).
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rho, S.Y.; Lee, J.G.; Joo, D.J.; Kim, M.S.; Kim, S.I.; Han, D.H.; Choi, J.S.; Choi, G.H. Outcomes of Robotic Living Donor Right Hepatectomy From 52 Consecutive Cases: Comparison With Open and Laparoscopy-assisted Donor Hepatectomy. Ann. Surg. 2022, 275, e433–e442. [Google Scholar] [CrossRef]
- CLARITY Group at McMaster University. Tool to Assess Risk of Bias in Cohort Studies. Available online: https://www.evidencepartners.com/wp-content/uploads/2017/09/Tool-to-Assess-Risk-of-Bias-in-Cohort-Studies.pdf (accessed on 1 May 2021).
- Solis-Pazmino, P.; Baiu, I.; Lincango-Naranjo, E.; Trope, W.; Prokop, L.; Ponce, O.J.; Shrager, J.B. Impact of the Surgical Approach to Thymectomy Upon Complete Stable Remission Rates in Myasthenia Gravis: A Meta-analysis. Neurology 2021, 97, e357–e368. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Comuting. 2020. Available online: https://www.r-project.org (accessed on 1 May 2021).
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Mesiar, R.; Špirková, J. Weighted means and weighting functions. Kybernetika 2006, 42, 151–160. [Google Scholar]
- Karagöz, D. Weighted standard deviation method for X and S control charts. Commun. Fac. Sci. Univ. Ank. Ser. A1 Math. Stat. 2019, 68, 1377–1386. [Google Scholar] [CrossRef] [Green Version]
- Binoj, S.T.; Mathew, J.S.; Nair, K.; Mallick, S.; Chandran, B.; Menon, R.; Unnikrishnan, G.; Balakrishnan, D.; Sudheer, O.V.; Sudhindran, S. 260 Robotic Donor Right Hepatectomy: Is It Just Flaunting the Scar? Gastroenterology 2020, 158, S-1263. [Google Scholar] [CrossRef]
- Chen, P.D.; Wu, C.Y.; Hu, R.H.; Ho, C.M.; Lee, P.H.; Lai, H.S.; Lin, M.T.; Wu, Y.M. Robotic liver donor right hepatectomy: A pure, minimally invasive approach. Liver Transpl. 2016, 22, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Broering, D.C.; Elsheikh, Y.; Alnemary, Y.; Zidan, A.; Elsarawy, A.; Saleh, Y.; Alabbad, S.; Sturdevant, M.; Wu, Y.M.; Troisi, R.I. Robotic Versus Open Right Lobe Donor Hepatectomy for Adult Living Donor Liver Transplantation: A Propensity Score-Matched Analysis. Liver Transpl. 2020, 26, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Abu Hilal, M.; Aldrighetti, L.; Dagher, I.; Edwin, B.; Troisi, R.I.; Alikhanov, R.; Aroori, S.; Belli, G.; Besselink, M.; Briceno, J.; et al. The Southampton Consensus Guidelines for Laparoscopic Liver Surgery: From Indication to Implementation. Ann. Surg. 2018, 268, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shehta, A.; Han, H.S.; Yoon, Y.S.; Cho, J.Y.; Choi, Y. Laparoscopic liver resection for hepatocellular carcinoma in cirrhotic patients: 10-year single-center experience. Surg. Endosc. 2016, 30, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.I.; Kim, K.H.; Kang, S.H.; Kim, W.J.; Shin, M.H.; Lee, S.K.; Jung, D.H.; Park, G.C.; Ahn, C.S.; Moon, D.B. Pure Laparoscopic Versus Open Right Hepatectomy for Hepatocellular Carcinoma in Patients with Cirrhosis. Ann. Surg. 2017, 265, 856–863. [Google Scholar] [CrossRef]
- Kornaropoulos, M.; Moris, D.; Beal, E.W.; Makris, M.C.; Mitrousias, A.; Petrou, A.; Felekouras, E.; Michalinos, A.; Vailas, M.; Schizas, D.; et al. Total robotic pancreaticoduodenectomy: A systematic review of the literature. Surg. Endosc. 2017, 31, 4382–4392. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Moris, D.; Vagios, S.; Merath, K.; Pawlik, T.M. Safety and oncologic outcomes of robotic liver resections: A systematic review. J. Surg. Oncol. 2018, 117, 1517–1530. [Google Scholar] [CrossRef]
- Machairas, N.; Papaconstantinou, D.; Tsilimigras, D.I.; Moris, D.; Prodromidou, A.; Paspala, A.; Spartalis, E.; Kostakis, I.D. Comparison between robotic and open liver resection: A systematic review and meta-analysis of short-term outcomes. Updates Surg. 2019, 71, 39–48. [Google Scholar] [CrossRef]
- Moris, D.; Burkhart, R.A.; Beal, E.W.; Pawlik, T.M. Laparoscopic hepatectomy for hepatocellular carcinoma: Are oncologic outcomes truly superior to an open approach? Hepato. Surg. Nutr. 2017, 6, 200–202. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.K.; Suh, K.S.; Kim, K.A.; Lee, J.M.; Cho, J.H.; Yi, N.J.; Lee, K.W. Pure Laparoscopic Versus Open Left Hepatectomy Including the Middle Hepatic Vein for Living Donor Liver Transplantation. Liver Transpl. 2020, 26, 370–378. [Google Scholar] [CrossRef]
- Hong, S.K.; Tan, M.Y.; Worakitti, L.; Lee, J.M.; Cho, J.H.; Yi, N.J.; Lee, K.W.; Suh, K.S. Pure Laparoscopic Versus Open Right Hepatectomy in Live Liver Donors. Ann. Surg. 2022, 275, e206–e212. [Google Scholar] [CrossRef] [PubMed]
- Song, J.L.; Yang, J.; Wu, H.; Yan, L.N.; Wen, T.F.; Wei, Y.G.; Yang, J.Y. Pure laparoscopic right hepatectomy of living donor is feasible and safe: A preliminary comparative study in China. Surg. Endosc. 2018, 32, 4614–4623. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kang, S.H.; Jung, D.H.; Yoon, Y.I.; Kim, W.J.; Shin, M.H.; Lee, S.G. Initial outcomes of pure laparoscopic living donor right hepatectomy in an experienced adult living donor liver transplant center. Transplantation 2017, 101, 1106–1110. [Google Scholar] [CrossRef]
- Hong, S.K.; Suh, K.S.; Yoon, K.C.; Lee, J.M.; Cho, J.H.; Yi, N.J.; Lee, K.W. The learning curve in pure laparoscopic donor right hepatectomy: A cumulative sum analysis. Surg. Endosc. 2019, 33, 3741–3748. [Google Scholar] [CrossRef]
- Samstein, B.; Griesemer, A.; Cherqui, D.; Mansour, T.; Pisa, J.; Yegiants, A.; Fox, A.N.; Guarrera, J.V.; Kato, T.; Halazun, K.J.; et al. Fully Laparoscopic Left-Sided Donor Hepatectomy Is Safe and Associated With Shorter Hospital Stay and Earlier Return To Work: A Comparative Study. Liver Transpl. 2015, 21, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Abecassis, M.M.; Fisher, R.A.; Olthoff, K.M.; Freise, C.E.; Rodrigo, D.R.; Samstein, B.; Kam, I.; Merion, R.M.; A2ALL Study Group. Complications of living donor hepatic lobectomy-A comprehensive report. Am. J. Transpl. 2012, 12, 1208–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghobrial, R.M.; Freise, C.E.; Trotter, J.F.; Tong, L.; Ojo, A.O.; Fair, J.H.; Fisher, R.A.; Emond, J.C.; Koffron, A.J.; Pruett, T.L.; et al. Donor Morbidity After Living Donation for Liver Transplantation. Gastroenterology 2008, 135, 468–476. [Google Scholar] [CrossRef] [Green Version]
- Coelho, F.F.; Bernardo, W.M.; Kruger, J.A.P.; Jeismann, V.B.; Fonseca, G.M.; Macacari, R.L.; Cesconetto, D.M.; D’Albuquerque, L.A.C.; Cecconello, I.; Herman, P. Laparoscopy-assisted versus open and pure laparoscopic approach for liver resection and living donor hepatectomy: A systematic review and meta-analysis. HPB 2018, 20, 687–694. [Google Scholar] [CrossRef] [Green Version]
- Tsung, A.; Geller, D.A.; Sukato, D.C.; Sabbaghian, S.; Tohme, S.; Steel, J.; Marsh, W.; Reddy, S.K.; Bartlett, D.L. Robotic versus laparoscopic hepatectomy: A matched comparison. Ann. Surg. 2014, 259, 549–555. [Google Scholar] [CrossRef]
- Montalti, R.; Scuderi, V.; Patriti, A.; Vivarelli, M.; Troisi, R.I. Robotic versus laparoscopic resections of posterosuperior segments of the liver: A propensity score-matched comparison. Surg. Endosc. 2016, 30, 1004–1013. [Google Scholar] [CrossRef]
- Zhang, L.; Yuan, Q.; Xu, Y.; Wang, W. Comparative clinical outcomes of robotassisted liver resection versus laparoscopic liver resection: A meta-analysis. PLoS ONE 2020, 15, e0240593. [Google Scholar] [CrossRef]
- Ziogas, I.A.; Giannis, D.; Esagian, S.M.; Economopoulos, K.P.; Tohme, S.; Geller, D.A. Laparoscopic versus robotic major hepatectomy: A systematic review and meta-analysis. Surg. Endosc. 2021, 35, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.H.D.; Choi, G.S.; Kim, J.M.; Cho, C.W.; Rhu, J.; Soo Kim, G.; Sinn, D.H.; Joh, J.W. Laparoscopic Donor Hepatectomy for Adult Living Donor Liver Transplantation Recipients. Liver Transpl. 2018, 24, 1545–1553. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Country | Study Design | Conference Abstracts | Study Period | Setting | Sample Size (n) | Robotic (n) | Laparoscopic (n) | Open (n) |
|---|---|---|---|---|---|---|---|---|---|
| Rho et al., 2020 | South Korea | Retrospective | NA | March 2016 to March 2019 | Single center | 232 | 52 | 62 | 118 |
| Broering et al., 2020 | Saudi Arabia | Retrospective | NA | January 2015 to July 2019 | Single center | 105 | 35 | NA | 70 |
| Binoj et al., 2020 | India | Prospective | American Association for the Study of Liver Diseases Congress 2020 | NR | NR | 113 | 51 | NA | 62 |
| Chen et al., 2016 | China | Retrospective | NA | June 2005 to September 2012 | Single center | 67 | 13 | NA | 54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lincango Naranjo, E.P.; Garces-Delgado, E.; Siepmann, T.; Mirow, L.; Solis-Pazmino, P.; Alexander-Leon, H.; Restrepo-Rodas, G.; Mancero-Montalvo, R.; Ponce, C.J.; Cadena-Semanate, R.; et al. Robotic Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2603. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092603
Lincango Naranjo EP, Garces-Delgado E, Siepmann T, Mirow L, Solis-Pazmino P, Alexander-Leon H, Restrepo-Rodas G, Mancero-Montalvo R, Ponce CJ, Cadena-Semanate R, et al. Robotic Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(9):2603. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092603
Chicago/Turabian StyleLincango Naranjo, Eddy P., Estefany Garces-Delgado, Timo Siepmann, Lutz Mirow, Paola Solis-Pazmino, Harold Alexander-Leon, Gabriela Restrepo-Rodas, Rafael Mancero-Montalvo, Cristina J. Ponce, Ramiro Cadena-Semanate, and et al. 2022. "Robotic Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 9: 2603. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11092603