
Diagnosis, Classification, and Assessment of the Underlying Etiology of Uveitis by Artificial Intelligence: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
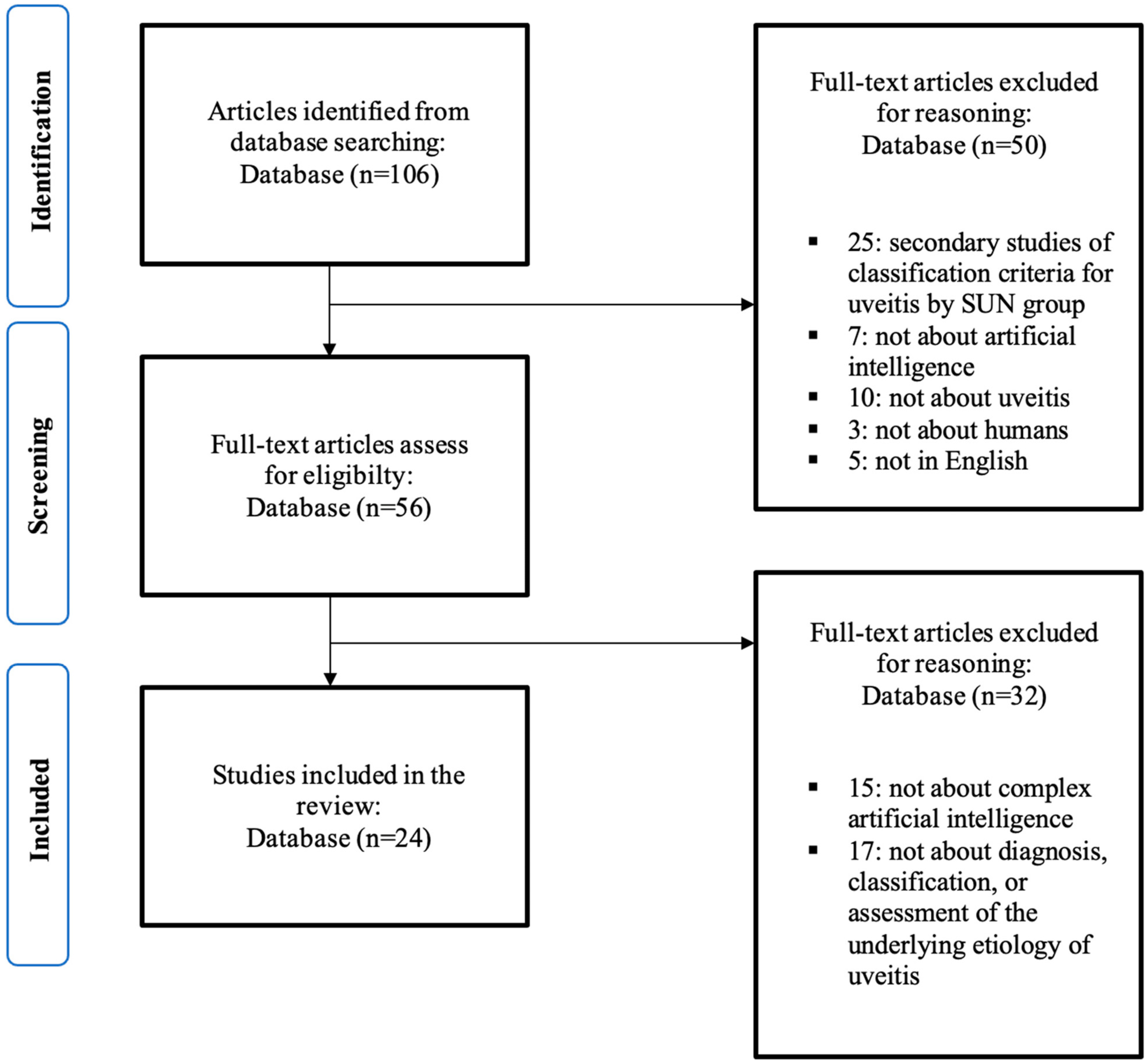
2.1. Search Strategy and Selection Criteria
2.2. Data Collection and Assessment
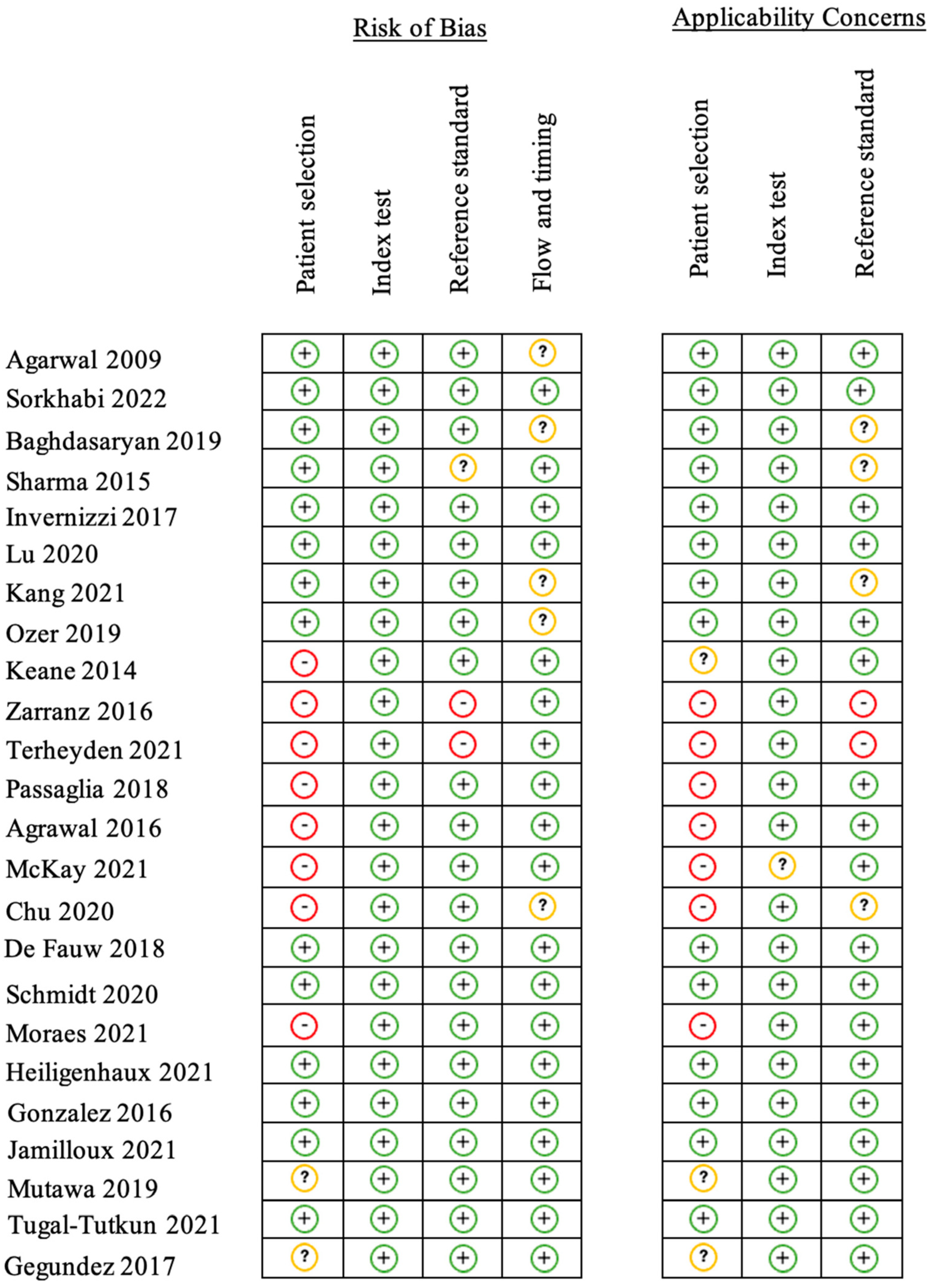
2.3. Risk of Bias Assessment and Outcome Measures
3. Results
3.1. Study Selection, Characteristics, and Risk of Bias
3.2. Diagnosis
3.2.1. Anterior Segment
3.2.2. Vitreous Segment
3.2.3. Posterior Segment
3.3. Classification
3.4. Etiology
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Prete, M.; Dammacco, R.; Fatone, M.C.; Racanelli, V. Autoimmune uveitis: Clinical, pathogenetic, and therapeutic features. Clin. Exp. Med. 2015, 16, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Dick, A.D.; Tundia, N.; Sorg, R.; Zhao, C.; Chao, J.; Joshi, A.; Skup, M. Risk of Ocular Complications in Patients with Noninfectious Intermediate Uveitis, Posterior Uveitis, or Panuveitis. Ophthalmology 2015, 123, 655–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiligenhaus, A.; Rothaus, K.; Pleyer, U. Development of classification criteria for uveitis by the standardization of uveitis nomenclature (SUN) working group. Ophthalmol. Z. Dtsch. Ophthalmol. Ges. 2021, 118, 913–918. [Google Scholar]
- Sève, P.; Cacoub, P.; Bodaghi, B.; Trad, S.; Sellam, J.; Bellocq, D.; Bielefeld, P.; Sène, D.; Kaplanski, G.; Monnet, D.; et al. Uveitis: Diagnostic work-up. A literature review and recommendations from an expert committee. Autoimmun. Rev. 2017, 16, 1254–1264. [Google Scholar] [CrossRef] [Green Version]
- Abad, S.; Sève, P.; Dhote, R.; Brézin, A.P. Guidelines for the management of uveitis in internal medicine. Rev. Med. Interne 2009, 30, 492–500. [Google Scholar] [CrossRef]
- Bodaghi, B.; Cassoux, N.; Wechsler, B.; Hannouche, D.; Fardeau, C.; Papo, T.; Huong, D.L.; Piette, J.C.; LeHoang, P. Chronic severe uveitis: Etiology and visual outcome in 927 patients from a single center. Medicine 2001, 80, 263–270. [Google Scholar] [CrossRef]
- de Parisot, A.; Kodjikian, L.; Errera, M.-H.; Sedira, N.; Heron, E.; Pérard, L.; Cornut, P.-L.; Schneider, C.; Rivière, S.; Ollé, P.; et al. Randomized Controlled Trial Evaluating a Standardized Strategy for Uveitis Etiologic Diagnosis (ULISSE). Am. J. Ophthalmol. 2017, 178, 176–185. [Google Scholar] [CrossRef]
- Seixas, F.L.; Zadrozny, B.; Laks, J.; Conci, A.; Muchaluat Saade, D.C. A Bayesian network decision model for supporting the diagnosis of dementia, Alzheimer׳s disease and mild cognitive impairment. Comput. Biol. Med. 2014, 51, 140–158. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, P.W.; Anderson, N.; Bartels, P.H.; Thompson, D. Expert system support using Bayesian belief networks in the diagnosis of fine needle aspiration biopsy specimens of the breast. J. Clin. Pathol. 1994, 47, 329–336. [Google Scholar] [CrossRef] [Green Version]
- González-López, J.J.; García-Aparicio, M.; Sánchez-Ponce, D.; Muñoz-Sanz, N.; Fernandez-Ledo, N.; Beneyto, P.; Westcott, M.C. Development and validation of a Bayesian network for the differential diagnosis of anterior uveitis. Eye 2016, 30, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Jamilloux, Y.; Romain-Scelle, N.; Rabilloud, M.; Morel, C.; Kodjikian, L.; Maucort-Boulch, D.; Bielefeld, P.; Sève, P. Development and Validation of a Bayesian Network for Supporting the Etiological Diagnosis of Uveitis. J. Clin. Med. 2021, 10, 3398. [Google Scholar] [CrossRef] [PubMed]
- Kras, A.; Celi, L.A.; Miller, J.B. Accelerating ophthalmic AI research: The role of an open access data repository. Curr. Opin. Ophthalmol. 2020, 31, 337. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Ashokkumar, D.; Jacob, S.; Agarwal, A.; Saravanan, Y. High-speed Optical Coherence Tomography for Imaging Anterior Chamber Inflammatory Reaction in Uveitis: Clinical Correlation and Grading. Am. J. Ophthalmol. 2009, 147, 413–416.e3. [Google Scholar] [CrossRef]
- Sorkhabi, M.A.; Potapenko, I.O.; Ilginis, T.; Alberti, M.; Cabrerizo, J. Assessment of Anterior Uveitis through Anterior-Segment Optical Coherence Tomography and Artificial Intelligence-Based Image Analyses. Transl. Vis. Sci. Technol. 2022, 11, 7. [Google Scholar] [CrossRef]
- Baghdasaryan, E.; Tepelus, T.C.; Marion, K.M.; Huang, J.; Huang, P.; Sadda, S.R.; Lee, O.L. Analysis of ocular inflammation in anterior chamber—Involving uveitis using swept-source anterior segment OCT. Int. Ophthalmol. 2018, 39, 1793–1801. [Google Scholar] [CrossRef]
- Sharma, S.; Lowder, C.Y.; Vasanji, A.; Baynes, K.; Kaiser, P.K.; Srivastava, S.K. Automated Analysis of Anterior Chamber Inflammation by Spectral-Domain Optical Coherence Tomography. Ophthalmology 2015, 122, 1464–1470. [Google Scholar] [CrossRef]
- Invernizzi, A.; Marchi, S.; Aldigeri, R.; Mastrofilippo, V.; Viscogliosi, F.; Soldani, A.; Adani, C.; Garoli, E.; Viola, F.; Fontana, L.; et al. Objective Quantification of Anterior Chamber Inflammation: Measuring Cells and Flare by Anterior Segment Optical Coherence Tomography. Ophthalmology 2017, 124, 1670–1677. [Google Scholar] [CrossRef]
- Lu, M.; Wang, X.; Lei, L.; Deng, Y.; Yang, T.; Dai, Y.; Li, Y.; Gan, X.; Hu, Y.; Chen, H.; et al. Quantitative Analysis of Anterior Chamber Inflammation Using the Novel CASIA2 Optical Coherence Tomography. Am. J. Ophthalmol. 2020, 216, 59–68. [Google Scholar] [CrossRef]
- Kang, T.S.; Lee, Y.; Lee, S.; Kim, K.; Lee, W.-S.; Lee, W.; Kim, J.H.; Han, Y.S. Development of fully automated anterior chamber cell analysis based on image software. Sci. Rep. 2021, 11, 10670. [Google Scholar] [CrossRef] [PubMed]
- Ozer, M.D.; Kebapci, F.; Batur, M.; Seven, E.; Tekin, S. In vivo analysis and comparison of anterior segment structures of both eyes in unilateral Fuchs’ uveitis syndrome. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 2019, 257, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Keane, P.A.; Karampelas, M.; Sim, D.A.; Sadda, S.R.; Tufail, A.; Sen, H.N.; Nussenblatt, R.B.; Dick, A.D.; Lee, R.W.; Murray, P.I.; et al. Objective measurement of vitreous inflammation using optical coherence tomography. Ophthalmology 2014, 121, 1706–1714. [Google Scholar] [CrossRef] [Green Version]
- Zarranz-Ventura, J.; Keane, P.A.; Sim, D.A.; Llorens, V.; Tufail, A.; Sadda, S.R.; Dick, A.D.; Lee, R.W.; Denniston, A.K.; Adan, A.; et al. Evaluation of Objective Vitritis Grading Method Using Optical Coherence Tomography: Influence of Phakic Status and Previous Vitrectomy. Am. J. Ophthalmol. 2016, 161, 172–180.e4. [Google Scholar] [CrossRef] [Green Version]
- Terheyden, J.H.; Ometto, G.; Montesano, G.; Wintergerst, M.W.M.; Langner, M.; Liu, X.; Keane, P.A.; Crabb, D.P.; Denniston, A.K.; Finger, R.P. Automated quantification of posterior vitreous inflammation: Optical coherence tomography scan number requirements. Sci. Rep. 2021, 11, 3271. [Google Scholar] [CrossRef]
- Passaglia, C.L.; Arvaneh, T.; Greenberg, E.; Richards, D.; Madow, B. Automated Method of Grading Vitreous Haze in Patients with Uveitis for Clinical Trials. Transl. Vis. Sci. Technol. 2018, 7, 10. [Google Scholar] [CrossRef]
- Agrawal, R.; Salman, M.; Tan, K.A.; Karampelas, M.; Sim, D.A.; Keane, P.A.; Pavesio, C. Choroidal Vascularity Index (CVI)—A Novel Optical Coherence Tomography Parameter for Monitoring Patients with Panuveitis? PLoS ONE 2016, 11, e0146344. [Google Scholar] [CrossRef]
- McKay, K.M.; Chu, Z.; Kim, J.-B.; Legocki, A.; Zhou, X.; Tian, M.; Munk, M.R.; Wang, R.K.; Pepple, K.L. Automated Quantification of Choriocapillaris Lesion Area in Patients with Posterior Uveitis. Am. J. Ophthalmol. 2021, 231, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Chu, Z.; Weinstein, J.E.; Wang, R.K.; Pepple, K.L. Quantitative Analysis of the Choriocapillaris in Uveitis Using En Face Swept-Source Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2020, 218, 17–27. [Google Scholar] [CrossRef]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Vogl, W.-D.; Jampol, L.M.; Bogunović, H. Application of Automated Quantification of Fluid Volumes to Anti–VEGF Therapy of Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 1211–1219. [Google Scholar] [CrossRef]
- Moraes, G.; Fu, D.J.; Wilson, M.; Khalid, H.; Wagner, S.K.; Korot, E.; Ferraz, D.; Faes, L.; Kelly, C.J.; Spitz, T.; et al. Quantitative Analysis of OCT for Neovascular Age-Related Macular Degeneration Using Deep Learning. Ophthalmology 2020, 128, 693–705. [Google Scholar] [CrossRef]
- Mutawa, A.M.; Alzuwawi, M.A. Multilayered rule-based expert system for diagnosing uveitis. Artif. Intell. Med. 2019, 99, 101691. [Google Scholar] [CrossRef]
- Tugal-Tutkun, I.; Onal, S.; Stanford, M.; Akman, M.; Twisk, J.W.; Boers, M.; Oray, M.; Özdal, P.; Kadayifcilar, S.; Amer, R.; et al. An Algorithm for the Diagnosis of Behçet Disease Uveitis in Adults. Ocul. Immunol. Inflamm. 2020, 29, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Gegundez-Fernandez, J.A.; Fernández-Vigo, J.I.; Diaz-Valle, D.; Mendez-Fernandez, R.; Cuiña-Sardiña, R.; Santos-Bueso, E.; Benitez-Del-Castillo, J.M. Uvemaster: A Mobile App-Based Decision Support System for the Differential Diagnosis of Uveitis. Investig. Opthalmol. Vis. Sci. 2017, 58, 3931–3939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abellanas, M.; Elena, M.J.; A Keane, P.; Balaskas, K.; Grewal, D.S.; Carreño, E. Artificial Intelligence and Imaging Processing in Optical Coherence Tomography and Digital Images in Uveitis. Ocul. Immunol. Inflamm. 2022, 30, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, A.S.; Wagner, I.V.; Dorairaj, S.; Checo, L.; Hulzen, R.T. Artificial intelligence in ophthalmology: A multidisciplinary approach. Integr. Med. Res. 2022, 11, 100888. [Google Scholar] [CrossRef]
- Mudie, L.I.; Reddy, A.K.; Patnaik, J.L.; Pecen, P.; Kim, E.; Cole, K.; Palestine, A.G. Evaluation of the SUN Classification Criteria for Uveitides in an Academic Uveitis Practice. Am. J. Ophthalmol. 2022, 241, 57–63. [Google Scholar] [CrossRef]
- Rathinam, S.R.; Babu, M. Algorithmic approach in the diagnosis of uveitis. Indian J. Ophthalmol. 2013, 61, 255–262. [Google Scholar] [CrossRef] [PubMed]
- de la Torre-Díez, I.; Martínez-Pérez, B.; López-Coronado, M.; Díaz, J.R.; López, M.M. Decision support systems and applications in ophthalmology: Literature and commercial review focused on mobile apps. J. Med. Syst. 2015, 39, 174. [Google Scholar] [CrossRef]
- McKay, K.M.; Lim, L.L.; Van Gelder, R.N. Rational laboratory testing in uveitis: A Bayesian analysis. Surv. Ophthalmol. 2021, 66, 802–825. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1 | Uveitis [MeSH Terms] OR uveitides [MeSH Terms] |
| 2 | Algorithms [MeSH Terms] |
| 3 | Artificial intelligence [MeSH Terms] OR Computational Intelligence [MeSH Terms] OR Intelligence, Computational [MeSH Terms] OR Machine Intelligence [MeSH Terms] OR [MeSH Terms] OR Intelligence, Machine [MeSH Terms] OR Computer Reasoning [MeSH Terms] OR Reasoning, Computer [MeSH Terms] OR AI (Artificial Intelligence) [MeSH Terms] OR Computer Vision Systems [MeSH Terms] OR Computer Vision System [MeSH Terms] OR System, Computer Vision [MeSH Terms] OR Systems, Computer Vision [MeSH Terms] OR Vision System, Computer [MeSH Terms] OR Vision Systems, Computer [MeSH Terms] OR Knowledge Acquisition (Computer) [MeSH Terms] OR Acquisition, Knowledge (Computer) [MeSH Terms] OR Knowledge Representation (Computer) [MeSH Terms] OR Knowledge Representations (Computer) [MeSH Terms] OR Representation, Knowledge (Computer) [MeSH Terms] |
| 4 | Decision support systems, Clinical [MeSH Terms] OR Clinical Decision Support Systems [MeSH Terms] OR Clinical Decision Support System [MeSH Terms] OR Clinical Decision Support [MeSH Terms] OR Clinical Decision Supports [MeSH Terms] OR Decision Supports, Clinical [MeSH Terms] OR Support, Clinical Decision [MeSH Terms] OR Supports, Clinical Decision [MeSH Terms] OR Decision Support, Clinical [MeSH Terms] |
| 5 | Bayes Theorem [MeSH Terms] OR Theorem, Bayes [MeSH Terms] OR Bayesian Forecast [MeSH Terms] OR Forecast, Bayesian [MeSH Terms] OR Bayesian Prediction [MeSH Terms] OR Prediction, Bayesian [MeSH Terms] OR Bayesian Estimation [MeSH Terms] OR Estimation, Bayesian [MeSH Terms] OR Bayesian Analysis [MeSH Terms] OR Bayesian Approach [MeSH Terms] OR Approach, Bayesian [MeSH Terms] OR Approachs, Bayesian [MeSH Terms] OR Bayesian Approachs [MeSH Terms] OR Analysis, Bayesian [MeSH Terms] OR Bayesian Method [MeSH Terms] OR Method, Bayesian [MeSH Terms] |
| Study | Methods | Study Factors | Etiology | Diagnostic Performance |
|---|---|---|---|---|
| Gonzalez et al., 2016 [10] | Bayesian belief networks Dataset: 200 cases (anterior uveitis) | Demographic (gender) Ophthalmic (ocular symptoms and signs) Clinical examination (systemic symptoms and signs) Laboratory tests | 11 | Sensitivity (most probable etiology): 64% Sensitivity (two most probable etiologies): 81% |
| Gegundez-Fernandez et al., 2017 (Uvemaster) [35] | Interference method with filtering rules Dataset: 88 cases (all uveitis type) | Demographic (age, gender, immunodeficiency, drugs, trauma or eye surgery, and endemic disease) Ophthalmic (anatomy, chronicity, laterality, granulomatous, vasculitis, papillitis, scleritis, and specific ocular involvement) Clinical examination (skin, mucosal, nervous system, articular, urinary, ear, nose, throat, and digestive and cardiovascular exam) Treatment (steroid response) | 88 | Sensitivity (most probable etiology): 74% Sensitivity (three most probable etiologies): 91% |
| Mutawa et al., 2019 [33] | Rule-based expert system (multilayer rule design) Dataset: 61 cases (case report, all uveitis type) | Ophthalmic (anatomy, chronicity, severity, laterality, granulomatous) Treatment (response to therapy) | 53 | Sensitivity (most probable etiology): 60% Sensitivity (four most probable etiologies): 100% |
| Jamilloux et al., 2021 [11] | Bayesian belief networks Dataset: 877 cases (all uveitis type) | Demographic (Age, sex, and ethnicity) Ophthalmic (Anatomy, laterality, chronicity, vasculitis, granulomatous, and ocular hypertension) | 8 | Sensitivity (most probable etiology): 54% Sensitivity (two most probable etiologies): 85% |
| Type of Outcome | Examples of Indicators |
|---|---|
| Description of patient population | Number of participants Patients or case report Age Sex Ethnicity Co-morbidity |
| Setting, type of unit | Community, primary care, secondary care, tertiary care Mono/multicentric Nationality |
| Study factors | Demographic data Ocular examination data Extraocular examination data Laboratory tests results Response to treatment |
| Etiologies | Number of etiologies Rare etiologies or not? Etiologies with high specific tests? |
| Data collection method | Retrospective Prospective |
| Reference standard | Standard of diagnosis/etiology assessment: detailed description By whom: expert or not? |
| Computing methods | Type of algorithm used? Bayesian belief networks; random forest; interference method with filtering rules; rule-based expert system; tree analysis… |
| Outcome measures | Timepoint Sensitivity Specificity Positive predictive value Area under the receiver operating characteristic curve (AUROC) |
| Validation | Part of the testing cohort (separation before analysis in two parts) External cohort |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacquot, R.; Sève, P.; Jackson, T.L.; Wang, T.; Duclos, A.; Stanescu-Segall, D. Diagnosis, Classification, and Assessment of the Underlying Etiology of Uveitis by Artificial Intelligence: A Systematic Review. J. Clin. Med. 2023, 12, 3746. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12113746
Jacquot R, Sève P, Jackson TL, Wang T, Duclos A, Stanescu-Segall D. Diagnosis, Classification, and Assessment of the Underlying Etiology of Uveitis by Artificial Intelligence: A Systematic Review. Journal of Clinical Medicine. 2023; 12(11):3746. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12113746
Chicago/Turabian StyleJacquot, Robin, Pascal Sève, Timothy L. Jackson, Tao Wang, Antoine Duclos, and Dinu Stanescu-Segall. 2023. "Diagnosis, Classification, and Assessment of the Underlying Etiology of Uveitis by Artificial Intelligence: A Systematic Review" Journal of Clinical Medicine 12, no. 11: 3746. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12113746