
The Limitations of Periapical X-ray Assessment in Endodontic Diagnosis—A Systematic Review

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Articles that are published in English or use English as a second language;
- Articles that use histopathology as a gold standard for periapical diagnosis;
- Articles that have used periapical X-ray as the main imaging technique or that include periapical X-ray as a comparative study to other imaging investigations;
- Articles that perform study on living organisms: human beings or animals;
- Articles that relate the histopathological diagnosis to the imaging investigation;
- Studies that approach distinctly the imaging assessment (if the assessment has been performed using various techniques—OPG, periapical, CBCT).
2.2. Exclusion Criteria
- Studies performed on human or animal cadavers (simulated tissue for X-ray exposure is not an accurate assessment);
- Studies that do not use histopathology as a gold standard in diagnosis;
- Book chapters, personal opinions, letters, narratives, commentaries and conference abstracts;
- Studies that could not be found published in English;
- Studies that use other imaging techniques to assess the periapical status (OPG/CBCT);
- Induced pathology was not accepted (intra-oral exposed pulp for a defined period of time).
2.3. Study Selection
2.4. Data Collection Process
3. Results

{kind=link}
{kind=link}
| Reason for Exclusion | Article (Author and Year) |
|---|---|
| The study was performed on cadavers and/or used simulated tissue for X-ray exposure | (Trope et al., 1989) (Green et al., 1997) (Barthel, Zimmer and Trope, 2004) (Kanagasingam, Hussaini et al., 2017) (Leonardi Dutra et al., 2016) (Kanagasingam, Lim et al., 2017) (Holtzmann et al., 1998) [29,30,31,32,33,34,35] |
| The study did not use histopathology as a gold standard method for diagnosis confirmation | (Estrela et al., 2008) (Tsai et al., 2012) (Low et al., 2008) (Halse, Molven and Fristad, 2002) (Lofthag-Hansen et al., 2007) (Tikku et al., 2010) [36,37,38,39,40,41] |
| The study did not use periapical X-ray for imaging assessment or did not clearly mention the X-ray type included in the Materials and Methods section or elsewhere in the article text (OPG/CBCT) | (Lin, Louis M. et al., 1991) (Becconsall-Ryan, Tong and Love, 2010) (Carrillo, Celia et al., 2008) (Simon et al., 2006) (Cotti et al., 2003) (Natkin, Oswald and Carnes, 1984) (Rud, Andreasen, 1972) (Seltzer, S., Bender, Smith, Freedman and Nazimov, 1967a) (Seltzer, S., Bender, Smith, Freedman and Nazimov, 1967b) (Yanagisawa, 1980) (Akinyamoju, O Gbadebo and Adeyemi, 2014) (Penarrocha et al., 2011) (Schulz et al., 2009) (Carrillo, C. et al., 2008) (Block et al., 1976) (Baumann, Rossman, 1956) (Bhaskar, 1966) (Lalonde, 1970) (Kizil, Energin, 1990) (Linenberg, Waldron and DeLaune, 1964) (Alotaibi et al., 2020) [25,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] |
| The study induced the pathological status of the periapical tissue | (Tanomaru-Filho et al., 2009) (López et al., 2014) (Paula-Silva et al., 2009) [22,62,63] |
| The study is a narrative review | (Hamood, 2001) (Lin, L. M., Huang and Rosenberg, 2007) [64,65] |
| The study does not contain information that could be linked to the reviewed subject | (Spatafore et al., 1990) (Teixeira-Salum et al., 2010) (Seltzer, Samuel, 1999) (Gallego Romero et al., 2002) (Ricucci, D., Lin and Spangberg, 2009) (Laux et al., 2000) (Patel et al., 2009) [66,67,68,69,70,71,72] |
| The study did not differentiate between OPG, CBCT or periapical X-ray when performing the imaging analysis and its correlation to the histological status | (Croitoru et al., 2016) (Syrjänen et al., 1982) [73,74] |
| Study Selected for Review | Type of Study Perfomed | Sample Size | Details Abouth the PA X-ray Assessment | Details Abouth the Histological Assessment | Results |
|---|---|---|---|---|---|
| (O Gbadebo, Akinyamoju and Sulaiman, 2014) [26] | Retrospective study | 19 patients | Diagnosis verified by Endodontic Consultants | Results verified by Oral Pathologists | Quantitative measures and quantitative analysis |
| (Kruse et al., 2017) [9] | Follow-up study | 19 patients/19 teeth | Imaging assessment was performed by three observers (two Endodontists, one Oral Radiologist), and when the result had three different versions, a single result was agreed by consesus | Samples were cut at 3–4 µm and analysed by one Oral Pathologist | Quantitative measures and quantitative analysis |
| (Bornstein et al., 2015) [23] | Follow-up study | 62 patients/62 teeth | Imaging assessment was performed by four blinded observers (two Oral Surgeons and two Residents in Oral Surgery) | Two experienced investigators diagnosed the samples, and the disagreement was solved by debate and consensus | Quantitative measures and quantitative analysis |
| (Berar et al., 2016) [75] | Case study | 60 patients/60 teeth | PA X-rays were assessed by two observers | Perfomed using a Leica DM750 Microscope | Quantitative measures and quantitative analysis |
| (Rózyło-Kalinowska, 2007) [24] | Retrospective study | 221 digital X-rays | Digora ver. 2.0 (Soredex—Orion Company, Finland), Dimaxis ver. 2.4.4 (Planmeca, Finland) and Emago ver. 3.42 (Oral Diagnostic Systems, ACTA, Holland) were the software used for density measurements | Not mentioned | Quantitative measures and quantitative analysis |
| (Shrout, Hall and Hildebolt, 1993) [76] | Case study | 10 biopsies of periapical lesions | Regions of interest were digitaly drawn on each X-ray for histogram analysis and cumulative percent histogram calculation | Samples were assessed by two board-certified Oral Pathologists | Quantitative measures and quantitative analysis |
| (White et al., 1994) [77] | Case study | 55 periapical lesions were histologicaly examined | NIH Image was used for X-ray measurements | Histology was assessed by one to three board-certified Oral Pathologist(s) | Quantitative measures and quantitative analysis |
| (Correa et al., 2017) [78] | Descriptive study | 14 samples of apical lesions | VixWin Platinum (version 3.3, Gendex INC, USA) was used for the imaging measurements | Not mentioned | Quantitative measures and quantitative analysis |
| (Çalışkan et al., 2016) [28] | Retrospective study | 93 teeth | Two blinded, trained observers investigated the X-rays in special conditions | Serial sectioning was performed in 4 µm thickness and examined by 1 Oral Pathologist | Quantitative measures and quantitative analysis |
| (Ricucci, Mannocci and Pitt Ford, 2006) [15] | Case study | 57 teeth | Two blinded, trained observers investigated the X-rays in special conditions | Serial sectioning was performed (150–600) in 4–5 µm thickness | Quantitative measures and quantitative analysis |
| (Ricucci, Siqueira, 2010) [79] | Retrospective study | 71 samples | Lesions were divided into 2: ≤5 mm and >5 mm, and no other information was available | Serial sectioning was performed in 4–5 µm thickness, and the assessment was separately performed by two evaluators | Quantitative measures and quantitative analysis |
| (Priebe, Lazansky and Wuehrmann, 1954) [80] | Prospective study | 101 patients | The ø of the apical rarefaction was ≲1 cm, and the imaging assessment was performed independently by four observers (two Oral Surgery Teachers and two Dental Roentgenology Teachers) | Microscopic serial sectioning was performed obtaining > 16,000 sections assessed by a Pathologist | Quantitative measures and quantitative analysis |
| (Gundappa, Ng and Whaites, 2006) [81] | Comparative in vivo pilot study | 15 patients | Three observers (two expert dental Radiologists and one Endodontist) examined the images on day 1, day 7 and day 14 to minimise errors | The biopsies were processed for routine histopathological assessment | Quantitative measures and quantitative analysis |
| (Mortensen, Winther and Birn, 1970) [82] | Research article | 396 periapical lesions were histologically examined | All X-rays were reassessed by one of the authors to minimise subjectivity | The specimens were processed for routine histologic assessment | Quantitative measures and quantitative analysis |
| (Zain, Roswati and Ismail, 1989a) [83] | Retrospective study | 69 cases | The measurements of the radiolucency were performed by operators respecting a defined criteria and a standard protocol | The lesions were reassessed respecting the general criteria | Quantitative measures and quantitative analysis |
| (Cunningham, Penick, 1968) [84] | Cross-sectional study | 41 lesions | The roentgenograms were assessed by two investigators after the injection of the contrast agent | The specimens were examined by an Oral Pathologist | Qualtitative measures and qualtitative analysis |
| STUDIES | (Kruse et al., 2017) [9] | (Ricucci, Mannocci & Pitt Ford, 2006) [15] | (Bornstein et al., 2015) [23] | (Rózyło-Kalinowska, 2007) [24] | (O Gbadebo, Akinyamoju & Sulaiman, 2014) [26] | (Çalışkan et al., 2016) [28] | (Berar et al., 2016) [75] | (Shrout, Hall & Hildebolt, 1993) [76] | (White et al., 1994) [77] | (Correa et al., 2017) [78] | (Ricucci, Siqueira, 2010) [79] | (Priebe, Lazansky & Wuehrmann, 1954) [80] | (Gundappa, Ng & Whaites, 2006) [81] | (Mortensen, Winther & Birn, 1970) [82] | (Zain, Roswati & Ismail, 1989) [83] | (Cunningham, Penick, 1968) [84] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quality measures | ||||||||||||||||
| Was the research objective clear? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the methodology described in detail? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | N | Y |
| Was the histology assessment protocol described? | Y | Y | Y | N | N | Y | Y | Y | N | N | Y | Y | Y | Y | Y | N |
| Was the imaging assessment protocol described? | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | N | Y | Y | Y | Y |
| Was it stated how subjects were attained? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the subjects clearly defined? | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the method of allocation, or similarity between groups described? | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A |
| Were diagnostic tools compared on any variables? | Y | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | N |
| Were the outcome measures clearly defined? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N |
| Were the outcome measures objective? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N/A |
| Were the outcome assessors blinded? | Y | N | Y | N | N | N/A | N/A | N | N | N | N | N | N | N | N | Y |
| Were the participants blinded? | N/A | N | N/A | N/A | N/A | N/A | N/A | N/A | N | N | N | N/A | N/A | N | N/A | N |
| Was the statistical analysis appropriate? | Y | Y | Y | Y | Y | Y | Y | N/A | Y | Y | Y | Y | Y | Y | Y | N/A |
| Was the sample size for each group given? | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | N/A |
| Was there a sample size justification? | N/A | N | N/A | N | N | N/A | N/A | N/A | N | N | N | N | N | Y | Y | N/A |
| Was the statistical significance defined? | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | N | N/A |
| Was drop-out rate given? | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N | N/A | N | N/A | Y | N/A | N/A |
| Was drop-out rate <10%? | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N | N/A | N/A |
| Were drop-outs accounted for? | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A |
| Quality score | 17 | 14.5 | 15 | 11.5 | 12.5 | 20.5 | 13.5 | 11.5 | 11 | 12.5 | 13.5 | 11 | 15.5 | 14.5 | 13.5 | 10.5 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Messer, H.H. Clinical judgement and decision making in endodontics. Aust. Endod. J. 1999, 25, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Pigg, M.; Broden, J.; Fransson, H.; EndoReCo; the Foresight Research Consortium; Vareman, N. How do we and how should we deal with uncertainty in endodontics? Int. Endod. J. 2022, 55, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.; Freeman, R. Reflective practice and experiential learning: Tools for continuing professional development. Dent. Update 2004, 31, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Bennett, G.W.; Tan, J.; Abbott, P.V. Diagnostic procedures employed by dental practitioners in Australia with a focus on endodontic diagnostic procedures. Aust. Dent. J. 2017, 62, 337–344. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, M. WHO surgical safety checklist cuts post-surgical deaths by 22%, US study finds. BMJ 2017, 357, j1935. [Google Scholar] [CrossRef]
- Iacopino, A.M. The influence of “new science” on dental education: Current concepts, trends, and models for the future. J. Dent. Educ. 2007, 71, 450–462. [Google Scholar] [CrossRef]
- Wenteler, G.L.; Sathorn, C.; Parashos, P. Factors influencing root canal retreatment strategies by general practitioners and specialists in Australia. Int. Endod. J. 2015, 48, 417–427. [Google Scholar] [CrossRef]
- Alim-Uysal, B.A.; Dincer, A.N.; Yurtgezen, B.; Guneser, M.B. Does the Endodontic Education Level Affect Decision-Making for Endodontically Treated Teeth with Apical Periodontitis? A Web-Based Survey. Int. Dent. J. 2021, 71, 477–483. [Google Scholar] [CrossRef]
- Kruse, C.; Spin-Neto, R.; Reibel, J.; Wenzel, A.; Kirkevang, L.-L. Diagnostic validity of periapical radiography and CBCT for assessing periapical lesions that persist after endodontic surgery. Dentomaxillofac. Radiol. 2017, 46, 20170210. [Google Scholar] [CrossRef]
- Patil, S.; Rao, R.; Patil, S. Deep Sections, a Guiding Path for Accurate Diagnosis in Histopathology—A Retrospective Study. J. Adv. Oral Res. 2013, 4, 15–20. [Google Scholar] [CrossRef]
- Buchanan, A.; Hancock, R.; Kalathingal, S. The role of software in quality assurance for indirect digital intraoral imaging. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kal, B.I.; Baksi, B.G.; Dundar, N.; Sen, B.H. Effect of various digital processing algorithms on the measurement accuracy of endodontic file length. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.L.; Wadhwani, C.P.; Abramovitch, K.; Rice, D.D.; Kattadiyil, M.T. Effect of image sharpening on radiographic image quality. J. Prosthet. Dent. 2018, 120, 927–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gormez, O.; Yilmaz, H.H. Image post-processing in dental practice. Eur. J. Dent. 2009, 3, 343–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricucci, D.; Mannocci, F.; Pitt Ford, T.R. A study of periapical lesions correlating the presence of a radiopaque lamina with histological findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 389–394. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- Patel, S.; Arias, A.; Whitworth, J.; Mannocci, F. Outcome of endodontic treatment—The elephant in the room. Int. Endod. J. 2020, 53, 291–297. [Google Scholar] [CrossRef]
- Gorni, F.G.; Gagliani, M.M. The outcome of endodontic retreatment: A 2-yr follow-up. J. Endod. 2004, 30, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ng, Y.L.; Mann, V.; Gulabivala, K. Outcome of secondary root canal treatment: A systematic review of the literature. Int. Endod. J. 2008, 41, 1026–1046. [Google Scholar] [CrossRef]
- Appel, D.; Schafer, E.; Appel, C. Success rate of orthograde endodontic retreatment after failed apicectomy—A retrospective study. Int. Endod. J. 2023, 56, 819–826. [Google Scholar] [CrossRef]
- Izaz, S.; Mandava, P.; Bolla, N.; Dasari, B. Atypical anatomy of maxillary second premolar with three roots and four canals. J. Conserv. Dent. 2017, 20, 370–373. [Google Scholar] [CrossRef] [PubMed]
- De Paula-Silva, F.W.G.; Wu, M.-K.; Leonardo, M.R.; da Silva, L.A.B.; Wesselink, P.R. Accuracy of Periapical Radiography and Cone-Beam Computed Tomography Scans in Diagnosing Apical Periodontitis Using Histopathological Findings as a Gold Standard. J. Endod. 2009, 35, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.M.; Bingisser, A.C.; Reichart, P.A.; Sendi, P.; Bosshardt, D.D.; von Arx, T. Comparison between Radiographic (2-dimensional and 3-dimensional) and Histologic Findings of Periapical Lesions Treated with Apical Surgery. J. Endod. 2015, 41, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Rozylo-Kalinowska, I. Digital radiography density measurements in differentiation between periapical granulomas and radicular cysts. Med. Sci. Monit. 2007, 13 (Suppl. S1), 129–136. [Google Scholar]
- Akinyamoju, A.O.; Gbadebo, S.O.; Adeyemi, B.F. Periapical lesions of the jaws: A review of 104 cases in ibadan. Ann. Ib. Postgrad. Med. 2014, 12, 115–119. [Google Scholar]
- Gbadebo, S.O.; Akinyamoju, A.O.; Sulaiman, A.O. Periapical Pathology: Comparison of Clinical Diagnosis and Histopathological Findings. J. West Afr. Coll. Surg. 2014, 4, 74–88. [Google Scholar]
- McGrath, C.; Zhang, W.; Lo, E.C. A review of the effectiveness of oral health promotion activities among elderly people. Gerodontology 2009, 26, 85–96. [Google Scholar] [CrossRef]
- Çalışkan, M.K.; Kaval, M.E.; Tekin, U.; Ünal, T. Radiographic and histological evaluation of persistent periapical lesions associated with endodontic failures after apical microsurgery. Int. Endod. J. 2015, 49, 1011–1019. [Google Scholar] [CrossRef]
- Trope, M.; Pettigrew, J.; Petras, J.; Barnett, F.; Tronstad, L. Differentiation of radicular cyst and granulomas using computerized tomography. Dent. Traumatol. 1989, 5, 69–72. [Google Scholar] [CrossRef]
- Green, T.L.; Walton, R.E.; Taylor, J.K.; Merrell, P. Radiographic and histologic periapical findings of root canal treated teeth in cadaver. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 707–711. [Google Scholar] [CrossRef]
- Barthel, C.; Zimmer, S.; Trope, M. Relationship of Radiologic and Histologic Signs of Inflammation in Human Root-filled Teeth. J. Endod. 2004, 30, 75–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanagasingam, S.; Hussaini, H.M.; Soo, I.; Baharin, S.; Ashar, A.; Patel, S. Accuracy of single and parallax film and digital periapical radiographs in diagnosing apical periodontitis—A cadaver study. Int. Endod. J. 2017, 50, 427–436. [Google Scholar] [CrossRef]
- Leonardi Dutra, K.; Haas, L.; Porporatti, A.L.; Flores-Mir, C.; Nascimento Santos, J.; Mezzomo, L.A.; Corrêa, M.; De Luca Canto, G. Diagnostic Accuracy of Cone-beam Computed Tomography and Conventional Radiography on Apical Periodontitis: A Systematic Review and Meta-analysis. J. Endod. 2016, 42, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Kanagasingam, S.; Lim, C.X.; Yong, C.P.; Mannocci, F.; Patel, S. Diagnostic accuracy of periapical radiography and cone beam computed tomography in detecting apical periodontitis using histopathological findings as a reference standard. Int. Endod. J. 2017, 50, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Holtzmann, D.J.; Johnson, W.T.; Southard, T.E.; Khademi, J.A.; Chang, P.J.; Rivera, E.M. Storage-phosphor computed radiography versus film radiography in the detection of pathologic periradicular bone loss in cadavers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Estrela, C.; Bueno, M.R.; Leles, C.R.; Azevedo, B.; Azevedo, J.R. Accuracy of Cone Beam Computed Tomography and Panoramic and Periapical Radiography for Detection of Apical Periodontitis. J. Endod. 2008, 34, 273–279. [Google Scholar] [CrossRef]
- Tsai, P.; Torabinejad, M.; Rice, D.; Azevedo, B. Accuracy of Cone-Beam Computed Tomography and Periapical Radiography in Detecting Small Periapical Lesions. J. Endod. 2012, 38, 965–970. [Google Scholar] [CrossRef]
- Low, K.M.T.; Dula, K.; Bürgin, W.; von Arx, T. Comparison of Periapical Radiography and Limited Cone-Beam Tomography in Posterior Maxillary Teeth Referred for Apical Surgery. J. Endod. 2008, 34, 557–562. [Google Scholar] [CrossRef]
- Halse, A.; Molven, O.; Fristad, I. Diagnosing periapical lesions—Disagreement and borderline cases. Int. Endod. J. 2002, 35, 703–709. [Google Scholar] [CrossRef]
- Lofthag-Hansen, S.; Huumonen, S.; Gröndahl, K.; Gröndahl, H.-G. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 114–119. [Google Scholar] [CrossRef]
- Tikku, A.P.; Kumar, S.; Loomba, K.; Chandra, A.; Verma, P.; Aggarwal, R. Use of ultrasound, color Doppler imaging and radiography to monitor periapical healing after endodontic surgery. J. Oral Sci. 2010, 52, 411–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.M.; Pascon, E.A.; Skribner, J.; Gängler, P.; Langeland, K. Clinical, radiographic, and histologic study of endodontic treatment failures. Oral Surg. Oral Med. Oral Pathol. 1991, 71, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Becconsall-Ryan, K.; Tong, D.; Love, R.M. Radiolucent inflammatory jaw lesions: A twenty-year analysis. Int. Endod. J. 2010, 43, 859–865. [Google Scholar] [CrossRef]
- Carrillo, C.; Peñarrocha, M.; Bagán, J.V.; Vera, F. Relationship Between Histological Diagnosis and Evolution of 70 Periapical Lesions at 12 Months, Treated by Periapical Surgery. J. Oral Maxillofac. Surg. 2008, 66, 1606–1609. [Google Scholar] [CrossRef]
- Simon, J.H.S.; Enciso, R.; Malfaz, J.-M.; Roges, R.; Bailey-Perry, M.; Patel, A. Differential Diagnosis of Large Periapical Lesions Using Cone-Beam Computed Tomography Measurements and Biopsy. J. Endod. 2006, 32, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Cotti, E.; Campisi, G.; Ambu, R.; Dettori, C. Ultrasound real-time imaging in the differential diagnosis of periapical lesions. Int. Endod. J. 2003, 36, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Natkin, E.; Oswald, R.J.; Carnes, L.I. The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas. Oral Surg. Oral Med. Oral Pathol. 1984, 57, 82–94. [Google Scholar] [CrossRef]
- Rud, J.; Andreasen, J.O. A study of failures after endodontic surgery by radiographic, histologic and stereomicroscopic methods. Int. J. Oral Surg. 1972, 1, 311–328. [Google Scholar] [CrossRef]
- Seltzer, S.; Bender, I.B.; Smith, J.; Freedman, I.; Nazimov, H. Endodontic failures—An analysis based on clinical, roentgenographic, and histologic findings: Part I. Oral Surg. Oral Med. Oral Pathol. 1967, 23, 500–516. [Google Scholar] [CrossRef]
- Seltzer, S.; Bender, I.B.; Smith, J.; Freedman, I.; Nazimov, H. Endodontic failures—An analysis based on clinical, roentgenographic, and histologic findings: Part II. Oral Surg. Oral Med. Oral Pathol. 1967, 23, 517–530. [Google Scholar] [CrossRef]
- Yanagisawa, S. Pathologic study of periapical lesions 1. Periapical granulomas: Clinical, histopathologic and immunohistopathologic studies. J. Oral Pathol. Med. 1980, 9, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha, M.; Carrillo, C.; Peñarrocha, M.; Peñarrocha, D.; von Arx, T.; Vera, F. Symptoms Before Periapical Surgery Related to Histologic Diagnosis and Postoperative Healing at 12 Months for 178 Periapical Lesions. J. Oral Maxillofac. Surg. 2011, 69, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; von Arx, T.; Altermatt, H.J.; Bosshardt, D. Histology of Periapical Lesions Obtained During Apical Surgery. J. Endod. 2009, 35, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, C.; Penarrocha, M.; Ortega, B.; Martí, E.; Bagán, J.V.; Vera, F. Correlation of Radiographic Size and the Presence of Radiopaque Lamina with Histological Findings in 70 Periapical Lesions. J. Oral Maxillofac. Surg. 2008, 66, 1600–1605. [Google Scholar] [CrossRef]
- Block, R.M.; Bushell, A.; Rodrigues, H.; Langeland, K. A histopathologic, histobacteriologic, and radiographic study of periapical endodontic surgical specimens. Oral Surg. Oral Med. Oral Pathol. 1976, 42, 656–678. [Google Scholar] [CrossRef]
- Baumann, L.; Rossman, S.R. Clinical, roentgenologic, and histopathologic findings in teeth with apical radiolucent areas. Oral Surg. Oral Med. Oral Pathol. 1956, 9, 1330–1336. [Google Scholar] [CrossRef]
- Bhaskar, S.N. Oral surgery—Oral pathology conference no. 17, Walter Reed Army Medical Center. Oral Surg. Oral Med. Oral Pathol. 1966, 21, 657–671. [Google Scholar] [CrossRef]
- Lalonde, E.R. A New Rationale for the Management of Periapical Granulomas and Cysts: An Evaluation of Histopathological and Radiographic Findings. J. Am. Dent. Assoc. 1970, 80, 1056–1059. [Google Scholar] [CrossRef]
- Kizil, Z.; Energin, K. An evaluation of radiographic and histopathological findings in periapical lesions. J. Marmara Univ. Dent. Fac. 1990, 1, 16–23. [Google Scholar]
- Linenberg, W.B.; Waldron, C.A.; DeLaune, G.F. A clinical, roentgenographic, and histopathologic evaluation of periapical lesions. Oral Surg. Oral Med. Oral Pathol. 1964, 17, 467–472. [Google Scholar] [CrossRef]
- Alotaibi, O.; Alswayyed, S.; Alshagroud, R.; AlSheddi, M. Evaluation of concordance between clinical and histopathological diagnoses in periapical lesions of endodontic origin. J. Dent. Sci. 2020, 15, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Tanomaru-Filho, M.; Jorge, E.G.; Duarte, M.A.H.; Gonçalves, M.; Guerreiro-Tanomaru, J.M. Comparative radiographic and histological analyses of periapical lesion development. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 442–447. [Google Scholar] [CrossRef] [PubMed]
- López, F.U.; Kopper, P.M.P.; Cucco, C.; Della Bona, A.; de Figueiredo, J.A.P.; Vier-Pelisser, F.V. Accuracy of Cone-beam Computed Tomography and Periapical Radiography in Apical Periodontitis Diagnosis. J. Endod. 2014, 40, 2057–2060. [Google Scholar] [CrossRef] [PubMed]
- Hamood, E. The Evaluation of Success and Failure of Endodontic Treatments. Aust. Endod. J. 2001, 27, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.M.; Huang, G.T.J.; Rosenberg, P.A. Proliferation of Epithelial Cell Rests, Formation of Apical Cysts, and Regression of Apical Cysts after Periapical Wound Healing. J. Endod. 2007, 33, 908–916. [Google Scholar] [CrossRef]
- Spatafore, C.M.; Griffin, J.A.; Keyes, G.G.; Wearden, S.; Skidmore, A.E. Periapical biopsy report: An analysis over a 10-year period. J. Endod. 1990, 16, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Teixeira-Salum, T.B.; Rodrigues, D.B.R.; Gervásio, A.M.; Souza, C.J.A.; Rodrigues, V., Jr.; Loyola, A.M. Distinct Th1, Th2 and Treg cytokines balance in chronic periapical granulomas and radicular cysts. J. Oral Pathol. Med. 2010, 39, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Seltzer, S. Long-term radiographic and histological observations of endodontically treated teeth. J. Endod. 1999, 25, 818–822. [Google Scholar] [CrossRef] [PubMed]
- Gallego Romero, D.; Torres Lagares, D.; GarcIa Calderon, M.; Romero Ruiz, M.M.; Infante Cossio, P.; Gutierrez Perez, J.L. Differential diagnosis and therapeutic approach to periapical cysts in daily dental practice. Med. Oral 2002, 7, 54–62. [Google Scholar] [PubMed]
- Ricucci, D.; Lin, L.M.; Spångberg, L.S.W. Wound healing of apical tissues after root canal therapy: A long-term clinical, radiographic, and histopathologic observation study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 609–621. [Google Scholar] [CrossRef]
- Laux, M.; Abbott, P.V.; Pajarola, G.; Nair, P.N.R. Apical inflammatory root resorption: A correlative radiographic and histological assessment. Int. Endod. J. 2000, 33, 483–493. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Whaites, E.; Ford, T.P. New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int. Endod. J. 2009, 42, 447–462. [Google Scholar] [CrossRef] [PubMed]
- Croitoru, I.C.; Craitoiu, S.; Petcu, C.M.; Mihailescu, O.A.; Pascu, R.M.; Bobic, A.G.; Forna, D.A.; Craitoiu, M.M. Clinical, imagistic and histopathological study of chronic apical periodontitis. Rom. J. Morphol. Embryol. 2016, 57, 719–728. [Google Scholar] [PubMed]
- Syrjänen, S.; Tammisalo, E.; Lilja, R.; Syrjänen, K. Radiological Interpretation of the Periapical Cysts and Granulomas. Dentomaxillofac. Radiol. 1982, 11, 89–92. [Google Scholar] [CrossRef]
- Berar, A.M.; Bondor, C.I.; Matros, L.; Campian, R.S. Radiological, histological and immunohistochemical evaluation of periapical inflammatory lesions. Rom. J. Morphol. Embryol. 2016, 57, 419–425. [Google Scholar] [PubMed]
- Shrout, M.K.; Hall, J.M.; Hildebolt, C.E. Differentiation of periapical granulomas and radicular cysts by digital radiometric analysis. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 356–361. [Google Scholar] [CrossRef]
- White, S.C.; Sapp, J.P.; Seto, B.G.; Mankovich, N.J. Absence of radiometric differentiation between periapical cysts and granulomas. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 650–654. [Google Scholar] [CrossRef]
- Correa, C.P.; García, L.B.; del Río, E.P.; Caballero, A.D. Correlation of clinical, radiographic and histological diagnoses of apical dental lesions. Rev. Odontológica Mex. 2017, 21, e21–e28. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F. Biofilms and Apical Periodontitis: Study of Prevalence and Association with Clinical and Histopathologic Findings. J. Endod. 2010, 36, 1277–1288. [Google Scholar] [CrossRef]
- Priebe, W.A.; Lazansky, J.P.; Wuehrmann, A.H. The value of the roentgenographic film in the differential diagnosis of periapical lesions. Oral Surg. Oral Med. Oral Pathol. 1954, 7, 979–983. [Google Scholar] [CrossRef]
- Gundappa, M.; Ng, S.Y.; Whaites, E.J. Comparison of ultrasound, digital and conventional radiography in differentiating periapical lesions. Dentomaxillofacial Radiol. 2006, 35, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, H.; Winther, J.E.; Birn, H. Periapical granulomas and cysts. Eur. J. Oral Sci. 1970, 78, 241–250. [Google Scholar] [CrossRef]
- Zain, R.B.; Roswati, N.; Ismail, K. Radiographic evaluation of lesion sizes of histologically diagnosed periapical cysts and granulomas. Ann. Dent. 1989, 48, 3–5, 46. [Google Scholar]
- Cunningham, C.J.; Penick, E.C. Use of a roentgenographic contrast medium in the differential diagnosis of periapical lesions. Oral Surg. Oral Med. Oral Pathol. 1968, 26, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Nagendrareddy, S.G.; Raju, M.S.; Krishnojirao, D.R.J.; Rastogi, R.; Mohan, R.P.S.; Gupta, S. Ultrasonography with color Doppler and power Doppler in the diagnosis of periapical lesions. Indian J. Radiol. Imaging 2011, 21, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Kronfeld, R. Histopathology of the Teeth: And Their Surrounding Structures; Lea & Febiger: Philadelphia, PA, USA, 1939. [Google Scholar]
- Reit, C.; Petersson, K.; Molven, O. Diagnosis of pulpal and periapical disease. In Textbook of Endodontology; Munksgaard, B., Ed.; John Wiley & Sons: Oxford, UK, 2003; pp. 9–18. [Google Scholar]
- Cotti, E.; Campisi, G.; Garau, V.; Puddu, G. A new technique for the study of periapical bone lesions: Ultrasound real time imaging. Int. Endod. J. 2002, 35, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Glickman, G.N. AAE Consensus Conference on Diagnostic Terminology: Background and perspectives. J. Endod. 2009, 35, 1619–1620. [Google Scholar] [CrossRef]
- Nair, P.R.; Pajarola, G.; Schroeder, H.E. Types and incidence of human periapical lesions obtained with extracted teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 81, 93–102. [Google Scholar] [CrossRef]
- Stockdale, C.R.; Chandler, N.P. The nature of the periapical lesion—A review of 1108 cases. J. Dent. 1988, 16, 123–129. [Google Scholar] [CrossRef]
- Abbott, P.V. Classification, diagnosis and clinical manifestations of apical periodontitis. Endod. Top. 2004, 8, 36–54. [Google Scholar] [CrossRef]
- Shoha, R.R.; Dowson, J.; Richards, A.G. Radiographic interpretation of experimentally produced bony lesions. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 294–303. [Google Scholar] [CrossRef]
- Bender, I.; Seltzer, S. Roentgenographic and Direct Observation of Experimental Lesions in Bone: I. J. Endod. 2003, 29, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N.R. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Rice, D.D.; Maktabi, O.; Oyoyo, U.; Abramovitch, K. Prevalence and Size of Periapical Radiolucencies Using Cone-beam Computed Tomography in Teeth without Apparent Intraoral Radiographic Lesions: A New Periapical Index with a Clinical Recommendation. J. Endod. 2018, 44, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Olcay, K.; Ataoglu, H.; Belli, S. Evaluation of Related Factors in the Failure of Endodontically Treated Teeth: A Cross-sectional Study. J. Endod. 2018, 44, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Gulabivala, K.; Ng, Y.-L. Preface. In Endodontics; Elsevier: Amsterdam, The Netherlands, 2014; p. vii. [Google Scholar] [CrossRef]
- Mainkar, A.; Kim, S.G. Diagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-analysis. J. Endod. 2018, 44, 694–702. [Google Scholar] [CrossRef]
- Prince, C.N.; Annapurna, C.S.; Sivaraj, S.; Ali, I.M. Ultrasound imaging in the diagnosis of periapical lesions. J. Pharm. Bioallied Sci. 2012, 4, S369–S372. [Google Scholar] [CrossRef]
- Parvathy, V.; Kumar, R.; James, E.; George, S. Ultrasound imaging versus conventional histopathology in diagnosis of periapical lesions of endodontic origin: A comparative evaluation. Indian J. Dent. Res. 2014, 25, 54. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Absence of evidence is not evidence of absence. BMJ 1995, 311, 485. [Google Scholar] [CrossRef] [Green Version]
- Wasserstein, R.L.; Lazar, N.A. The ASA Statement on p-Values: Context, Process, and Purpose. Am. Stat. 2016, 70, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Bender, I.; Seltzer, S. Roentgenographic and Direct Observation of Experimental Lesions in Bone: II. J. Endod. 2003, 29, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Vier, F.V.; Figueiredo, J.A.P. Internal apical resorption and its correlation with the type of apical lesion. Int. Endod. J. 2004, 37, 730–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodersen, J.; Schwartz, L.M.; Heneghan, C.; O’Sullivan, J.W.; Aronson, J.K.; Woloshin, S. Overdiagnosis: What it is and what it isn’t. BMJ Evid.-Based Med. 2018, 23, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, N. Nonsurgical management of periapical lesions: A prospective study. Oral Surg. Oral Med. Oral Pathol. 1988, 66, 365–371. [Google Scholar] [CrossRef]
- Iandolo, A.; Pantaleo, G.; Malvano, M.; Simeone, M.; Amato, M. Nonsurgical management of complex endodontic cases with several periapical lesions: A case series. G. Ital. Endod. 2016, 30, 101–110. [Google Scholar] [CrossRef]
- Torabinejad, M.; White, S.N. Endodontic treatment options after unsuccessful initial root canal treatment. J. Am. Dent. Assoc. 2016, 147, 214–220. [Google Scholar] [CrossRef]


| Normal Apical Tissues | Teeth with Normal Periradicular Tissues That Are Not Sensitive to Percussion or Palpation Testing. The Lamina Dura Surrounding the Root Is Intact, and the Periodontal Ligament Space Is Uniform. |
|---|---|
| Symptomatic apical periodontitis | Inflammation, usually of the apical periodontium, producing clinical symptoms including a painful response to biting and/or percussion or palpation. It might or might not be associated with an apical radiolucent area. |
| Asymptomatic apical periodontitis | Inflammation and destruction of apical periodontium that is of pulpal origin, appears as an apical radiolucent area, and does not produce clinical symptoms. |
| Acute apical abscess | An inflammatory reaction to pulpal infection and necrosis characterized by rapid onset, spontaneous pain, tenderness of the tooth to pressure, pus formation and swelling of associated tissues. |
| Chronic apical abscess | An inflammatory reaction to pulpal infection and necrosis characterized by gradual onset, little or no discomfort, and the intermittent discharge of pus through an associated sinus tract. |
| Condensing osteitis | Diffuse radiopaque lesion representing a localized bony reaction to a low-grade inflammatory stimulus, usually seen at apex of tooth. |
| Periapical Abscess | Periapical Granuloma | Periapical Cyst |
|---|---|---|
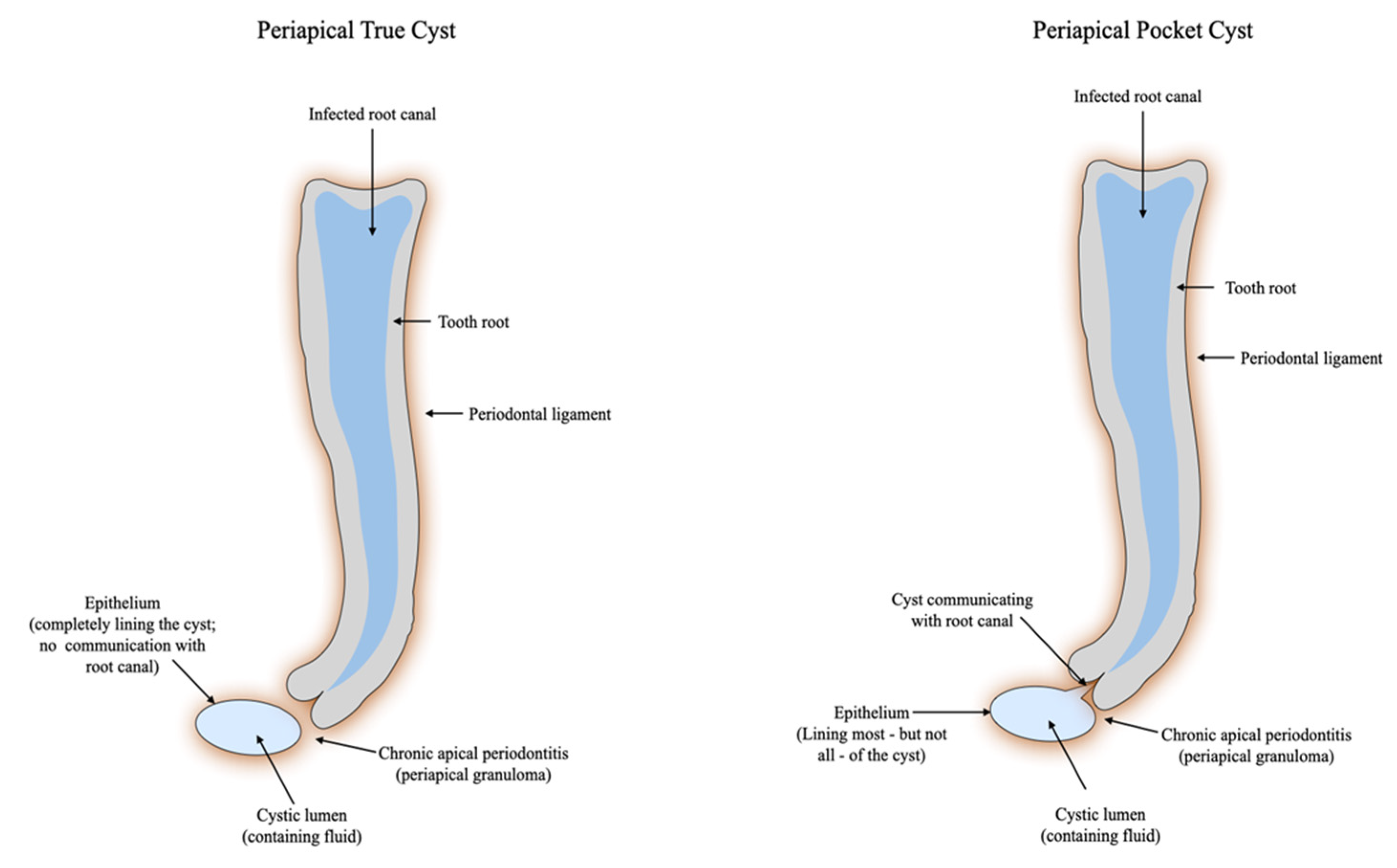
| Epithelialized abscess | Epithelialized granuloma | Apical true cyst |
| Non-epithelialized abscess | Non-epithelialized granuloma | Apical pocket cyst |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gliga, A.; Imre, M.; Grandini, S.; Marruganti, C.; Gaeta, C.; Bodnar, D.; Dimitriu, B.A.; Foschi, F. The Limitations of Periapical X-ray Assessment in Endodontic Diagnosis—A Systematic Review. J. Clin. Med. 2023, 12, 4647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12144647
Gliga A, Imre M, Grandini S, Marruganti C, Gaeta C, Bodnar D, Dimitriu BA, Foschi F. The Limitations of Periapical X-ray Assessment in Endodontic Diagnosis—A Systematic Review. Journal of Clinical Medicine. 2023; 12(14):4647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12144647
Chicago/Turabian StyleGliga, Alexandru, Marina Imre, Simone Grandini, Crystal Marruganti, Carlo Gaeta, Dana Bodnar, Bogdan Alexandru Dimitriu, and Federico Foschi. 2023. "The Limitations of Periapical X-ray Assessment in Endodontic Diagnosis—A Systematic Review" Journal of Clinical Medicine 12, no. 14: 4647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12144647