

Long-Term Performance of Epicardial versus Transvenous Left Ventricular Leads for Cardiac Resynchronization Therapy
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Transvenous Lead Placement
2.3. Epicardial Left Ventricular Lead Placement
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Population and Baseline Characteristics
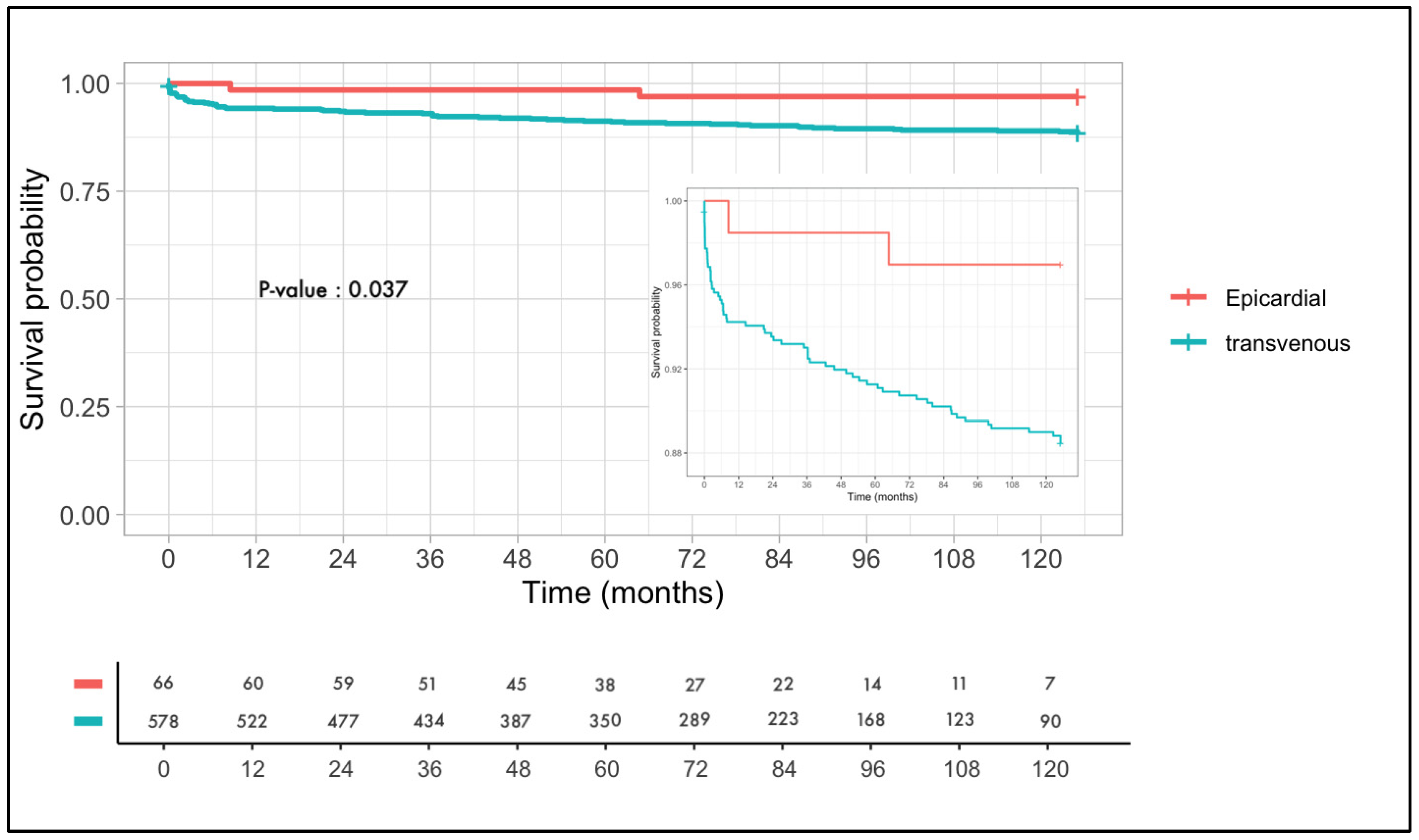
3.2. Lead Failure
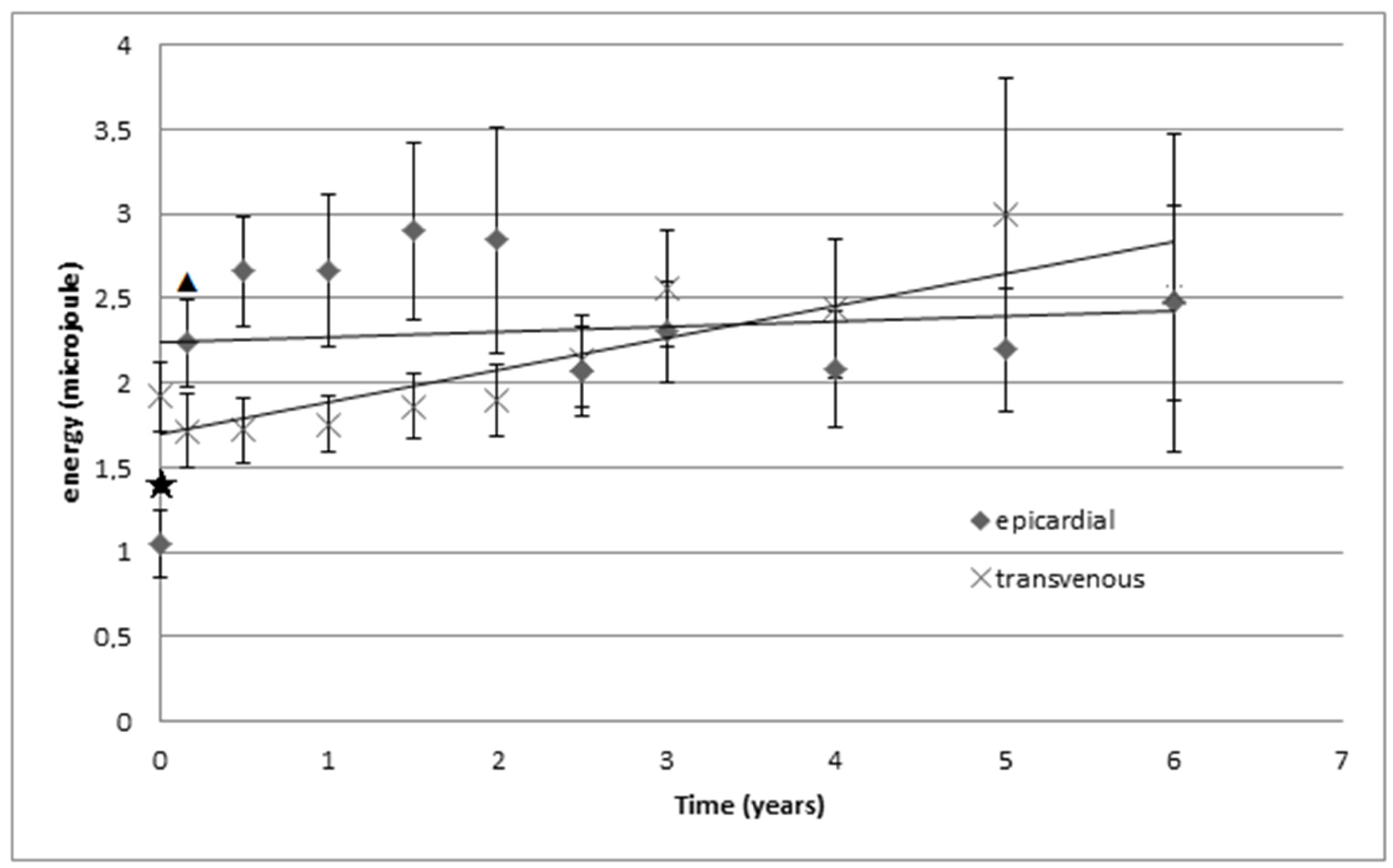
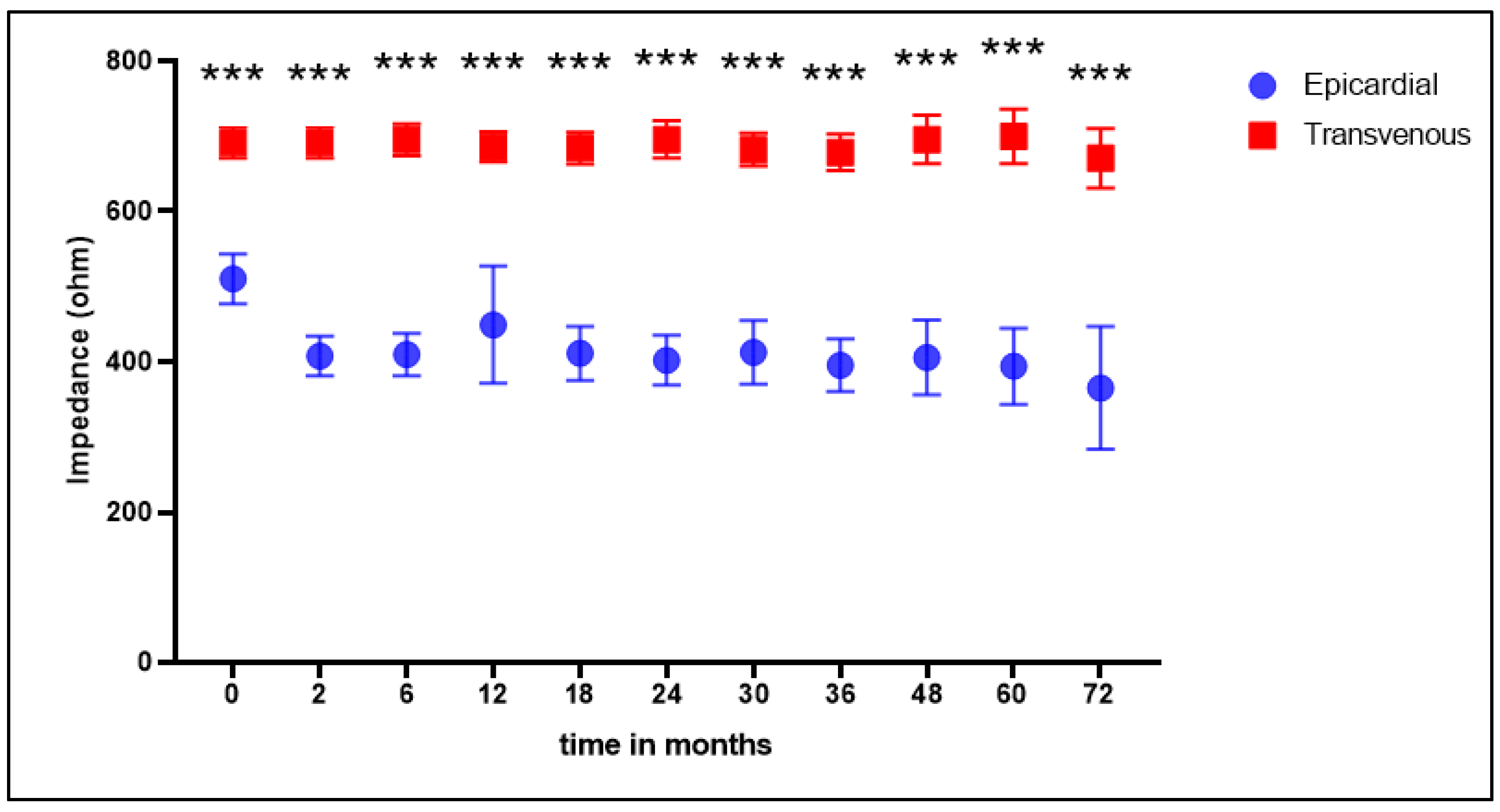
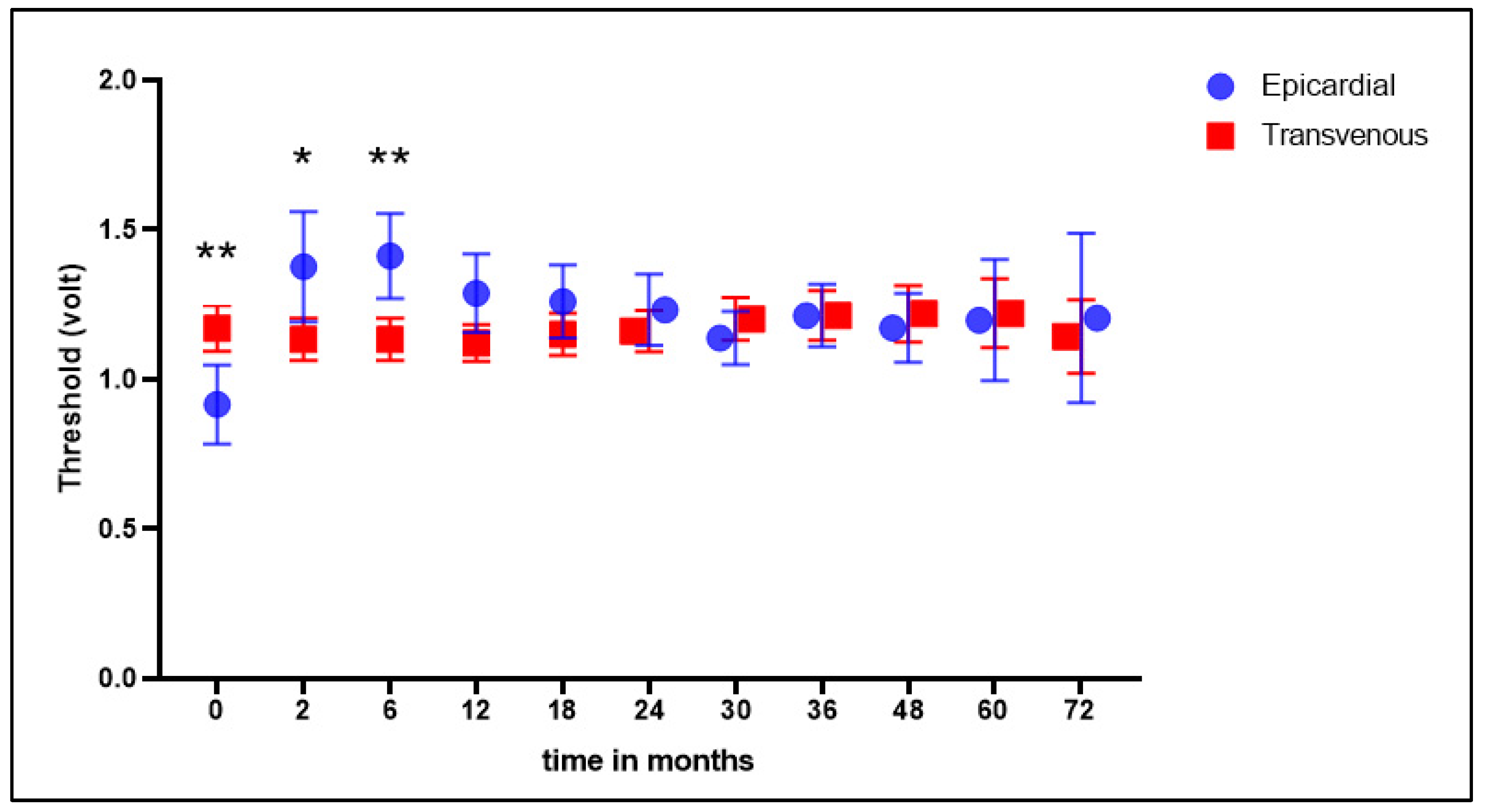
3.3. Electrical Consumption and Stability
4. Discussion
4.1. General
4.2. Comparison of Epicardial versus Transvenous Placed Leads
4.3. Lead Failure
4.4. Energy Consumption
4.5. Epicardial Leads and CRT Response
4.6. Future Perspective
4.7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [PubMed]
- Rad, M.M.; Blaauw, Y.; Dinh, T.; Pison, L.; Crijns, H.J.; Prinzen, F.W.; Vernooy, K. Left ventricular lead placement in the latest activated region guided by coronary venous electroanatomic mapping. Europace 2015, 17, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Gras, D.; Böcker, D.; Lunati, M.; Wellens, H.; Calvert, M.; Freemantle, N.; Gervais, R.; Kappenberger, L.; Tavazzi, L.; Erdmann, E.; et al. Implantation of cardiac resynchronization therapy systems in the CARE-HF trial: Procedural success rate and safety. Europace 2007, 9, 516–522. [Google Scholar] [CrossRef]
- Ahsan, S.Y.; Saberwal, B.; Lambiase, P.D.; Chaubey, S.; Segal, O.R.; Gopalamurugan, A.B.; McCready, J.; Rogers, D.P.; Lowe, M.D.; Chow, A.W. An 8-year single-centre experience of cardiac resynchronisation therapy: Procedural success, early and late complications, and left ventricular lead performance. Europace 2013, 15, 711–717. [Google Scholar] [CrossRef]
- van Gelder, B.M.; Scheffer, M.G.; Meijer, A.; Bracke, F.A. Transseptal endocardial left ventricular pacing: An alternative technique for coronary sinus lead placement in cardiac resynchronization therapy. Heart Rhythm. 2007, 4, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Kassai, I.; Foldesi, C.; Szekely, A.; Szili-Torok, T. Alternative Method for Cardiac Resynchronization: Transapical Lead Implantation. Ann. Thorac. Surg. 2009, 87, 650–652. [Google Scholar] [CrossRef]
- Puglisi, A.; Lunati, M.; Marullo, A.G.; Bianchi, S.; Feccia, M.; Sgreccia, F.; Vicini, I.; Valsecchi, S.; Musumeci, F.; Vitali, E. Limited thoracotomy as a second choice alternative to transvenous implant for cardiac resynchronisation therapy delivery. Eur. Heart J. 2004, 25, 1063–1069. [Google Scholar] [CrossRef]
- Mair, H.; Sachweh, J.; Meuris, B.; Nollert, G.; Schmoeckel, M.; Schuetz, A.; Reichart, B.; Daebritz, S. Surgical epicardial left ventricular lead versus coronary sinus lead placement in biventricular pacing? Eur. J. Cardio-Thoracic Surg. 2005, 27, 235–242. [Google Scholar] [CrossRef]
- Patwala, A.; Woods, P.; Clements, R.; Albouaini, K.; Rao, A.; Goldspink, D.; Tan, L.-B.; Oo, A.; Wright, D. A prospective longitudinal evaluation of the benefits of epicardial lead placement for cardiac resynchronization therapy. Europace 2009, 11, 1323–1329. [Google Scholar] [CrossRef]
- Kamath, G.S.; Balaram, S.; Choi, A.; Kuteyeva, O.; Garikipati, N.V.; Steinberg, J.S.; Mittal, S. Long-Term Outcome of Leads and Patients Following Robotic Epicardial Left Ventricular Lead Placement for Cardiac Resynchronization Therapy. Pacing Clin. Electrophysiol. 2010, 34, 235–240. [Google Scholar] [CrossRef]
- Buiten, M.S.; van der Heijden, A.C.; Klautz, R.J.; Schalij, M.J.; van Erven, L. Epicardial leads in adult cardiac resynchronization therapy recipients: A study on lead performance, durability, and safety. Heart Rhythm. 2015, 12, 533–539. [Google Scholar] [CrossRef]
- Doll, N.; Piorkowski, C.; Czesla, M.; Kallenbach, M.; Rastan, A.J.; Arya, A.; Mohr, F.W. Epicardial versus Transvenous Left Ventricular Lead Placement in Patients Receiving Cardiac Resynchronization Therapy: Results from a Randomized Prospective Study. Thorac. Cardiovasc. Surg. 2008, 56, 256–261. [Google Scholar] [CrossRef]
- Schouwenburg, J.J.; Klinkenberg, T.J.; Maass, A.H.; Mariani, M.A. Video-Assisted Thoracic Placement of Epicardial Leads. J. Card. Surg. 2014, 29, 286–289. [Google Scholar] [CrossRef]
- Kloosterman, M.; Rienstra, M.; Mulder, B.A.; Van Gelder, I.C.; Maass, A.H. Atrial reverse remodelling is associated with outcome of cardiac resynchronization therapy. Europace 2016, 18, 1211–1219. [Google Scholar] [CrossRef]
- Zareba, W.; Klein, H.; Cygankiewicz, I.; Hall, W.J.; McNitt, S.; Brown, M.; Cannom, D.; Daubert, J.P.; Eldar, M.; Gold, M.R.; et al. Effectiveness of Cardiac Resynchronization Therapy by QRS Morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation 2011, 123, 1061–1072. [Google Scholar] [CrossRef]
- Saxon, L.A.; Hayes, D.L.; Gilliam, F.R.; Heidenreich, P.A.; Day, J.; Seth, M.; Meyer, T.E.; Jones, P.W.; Boehmer, J.P. Long-Term Outcome After ICD and CRT Implantation and Influence of Remote Device Follow-Up The ALTITUDE Survival Study. Circulation 2010, 122, 2359–2367. [Google Scholar] [CrossRef]
- Burger, H.; Pecha, S.; Hakmi, S.; Opalka, B.; Schoenburg, M.; Ziegelhoeffer, T. Five-year follow-up of transvenous and epicardial left ventricular leads: Experience with more than 1000 leads. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 74–80. [Google Scholar] [CrossRef]
- Osca, J.; Alonso, P.; Cano, O.; Sánchez, J.M.; Tejada, D.; Andrés, A.; Tello, M.J.S.; Olagüe, J. The Use of Quadripolar Left Ventricular Leads Improves the Hemodynamic Response to Cardiac Resynchronization Therapy. Pacing Clin. Electrophysiol. 2014, 38, 326–333. [Google Scholar] [CrossRef]
- Vollmann, D.; Woronowicz, S.; Kmiec, L.; Jung, K.; Zenker, D.; Seegers, J.; Sossalla, S.; Dorenkamp, M.; Sohns, C.; Lüthje, L.; et al. Passive-fixation lead failure rates and long-term patient mortality in subjects implanted with Sprint Fidelis electrodes. Europace 2014, 16, 258–264. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.-A.; Cleland, J.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Europace 2013, 15, 1070–1118. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, V.F.; Fanggiday, J.; Balt, J.C.; Wijffels, M.C.E.F.; Daeter, E.J.; Kelder, J.C.; Boersma, L.V.A. Effects of epicardial versus transvenous left ventricular lead placement on left ventricular function and cardiac perfusion in cardiac resynchronization therapy: A randomized clinical trial. J. Cardiovasc. Electrophysiol. 2017, 28, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Garikipati, N.V.; Mittal, S.; Chaudhry, F.; Musat, D.L.; Sichrovsky, T.; Preminger, M.; Arshad, A.; Steinberg, J.S. Comparison of Endovascular Versus Epicardial Lead Placement for Resynchronization Therapy. Am. J. Cardiol. 2014, 113, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Rickard, J.; Johnston, D.R.; Price, J.; Tedford, R.; Baranowski, B.; Bassiouny, M.; Cantillon, D.; Grimm, R.A.; Tang, W.W.; Varma, N.; et al. Reverse ventricular remodeling and long-term survival in patients undergoing cardiac resynchronization with surgically versus percutaneously placed left ventricular pacing leads. Heart Rhythm. 2015, 12, 517–523. [Google Scholar] [CrossRef]
- Adelstein, E.; Alam, M.B.; Schwartzman, D.; Jain, S.; Marek, J.; Gorcsan, J.; Saba, S. Effect of echocardiography-guided left ventricular lead placement for cardiac resynchronization therapy on mortality and risk of defibrillator therapy for ventricular arrhythmias in heart failure patients (from the Speckle Tracking Assisted Resynchronization Therapy for Electrode Region [STARTER] trial). Am. J. Cardiol. 2014, 113, 1518–1522. [Google Scholar]
- Kydd, A.C.; Khan, F.Z.; Watson, W.D.; Pugh, P.J.; Virdee, M.S.; Dutka, D.P. Prognostic benefit of optimum left ventricular lead position in cardiac resynchronization therapy: Follow-up of the TARGET Study Cohort (Targeted Left Ventricular Lead Placement to guide Cardiac Resynchronization Therapy). JACC Heart Fail. 2014, 2, 205–212. [Google Scholar] [CrossRef]
- Shan, L.; Buratto, E.; Conaglen, P.; Davis, P.; Yii, M.; Nixon, I.; Newcomb, A. Prophylactic Epicardial Left Ventricular Lead Implantation for Biventricular Pacing During Operations. Ann. Thorac. Surg. 2014, 97, 603–608. [Google Scholar] [CrossRef]
- Quigley, R.L. A hybrid approach to cardiac resynchronization therapy. Ann. Thorac. Cardiovasc. Surg. 2011, 17, 273–276. [Google Scholar] [CrossRef]
- Heckman, L.; Vijayaraman, P.; Luermans, J.; Stipdonk, A.M.W.; Salden, F.; Maass, A.H.; Prinzen, F.W.; Vernooy, K. Novel bradycardia pacing strategies. Heart 2020, 106, 1883–1889. [Google Scholar] [CrossRef]
- Baroni, M.; Preda, A.; Varrenti, M.; Vargiu, S.; Carbonaro, M.; Giordano, F.; Gigli, L.; Mazzone, P. Left bundle branch area pacing over his bundle pacing: How far have we come? J. Clin. Med. 2023, 12, 3251. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Sharma, P.S.; Cano, O.; Ponnusamy, S.S.; Herweg, B.; Zanon, F.; Jastrzebski, M.; Zou, J.; Chelu, M.G.; Vernooy, K.; et al. Comparison of Left Bundle Branch Area Pacing and Biventricular Pacing in Candidates for Resynchronization Therapy. J. Am. Coll. Cardiol. 2023, 82, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Burri, H.; Jastrzebski, M.; Cano, Ó.; Čurila, K.; de Pooter, J.; Huang, W.; Israel, C.; Joza, J.; Romero, J.; Vernooy, K.; et al. EHRA clinical consensus statement on conduction system pacing implantation: Indorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS). Europace 2023, 25, 1208–1236. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transvenous (N = 578) | Epicardial (N = 66) | p-Value | |
|---|---|---|---|
| Age, years | 65.5 ± 11.5 | 63.8 ± 12.2 | 0.13 |
| Male gender, n (%) | 420 (73%) | 41 (62%) | 0.08 |
| Follow up, years | 5.9 ± 3.5 | 5.5 ± 3.1 | 0.94 |
| Body mass index, kg/m2 | 27 ± 5 | 29 ± 6 | 0.12 |
| Diabetes, n (%) | 124 (21) | 17 (27) | 0.30 |
| Coronary artery disease, n (%) | 291 (50) | 28 (42) | 0.19 |
| Hypertension, n (%) | 240 (42) | 37 (56) | 0.02 |
| NYHA class | 2.6 ± 0.6 | 2.5 ± 0.6 | 0.13 |
| LVEF, % | 24.3 ± 8.9 | 25.6 ± 8.9 | 0.42 |
| LBBB, n (%) | 417 (70) | 41 (61) | 0.23 |
| Transvenous (N = 578) | Epicardial (N = 66) | |
|---|---|---|
| Failure | 66 (11%) | 2 (3%) |
| Cause | ||
| Dislocation | 39 (59%) | - |
| Lead fracture | 15 (23%) | - |
| Phrenic nerve stimulation | 7 (10%) | - |
| Infection | 5 (8%) | 1 (50%) |
| Malsensing | 0 (0%) | 1 (50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Maat, G.E.; Mulder, B.A.; Van de Lande, M.E.; Rama, R.S.; Rienstra, M.; Mariani, M.A.; Maass, A.H.; Klinkenberg, T.J. Long-Term Performance of Epicardial versus Transvenous Left Ventricular Leads for Cardiac Resynchronization Therapy. J. Clin. Med. 2023, 12, 5766. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185766
de Maat GE, Mulder BA, Van de Lande ME, Rama RS, Rienstra M, Mariani MA, Maass AH, Klinkenberg TJ. Long-Term Performance of Epicardial versus Transvenous Left Ventricular Leads for Cardiac Resynchronization Therapy. Journal of Clinical Medicine. 2023; 12(18):5766. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185766
Chicago/Turabian Stylede Maat, Gijs E., Bart A. Mulder, Martijn E. Van de Lande, Rajiv S. Rama, Michiel Rienstra, Massimo A. Mariani, Alexander H. Maass, and Theo J. Klinkenberg. 2023. "Long-Term Performance of Epicardial versus Transvenous Left Ventricular Leads for Cardiac Resynchronization Therapy" Journal of Clinical Medicine 12, no. 18: 5766. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185766