
Perioperative Outcomes, Comorbidities, and Complications following Total Shoulder Arthroplasty in Wheelchair Users: A Retrospective Cohort Analysis of a Nationwide Database

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Design
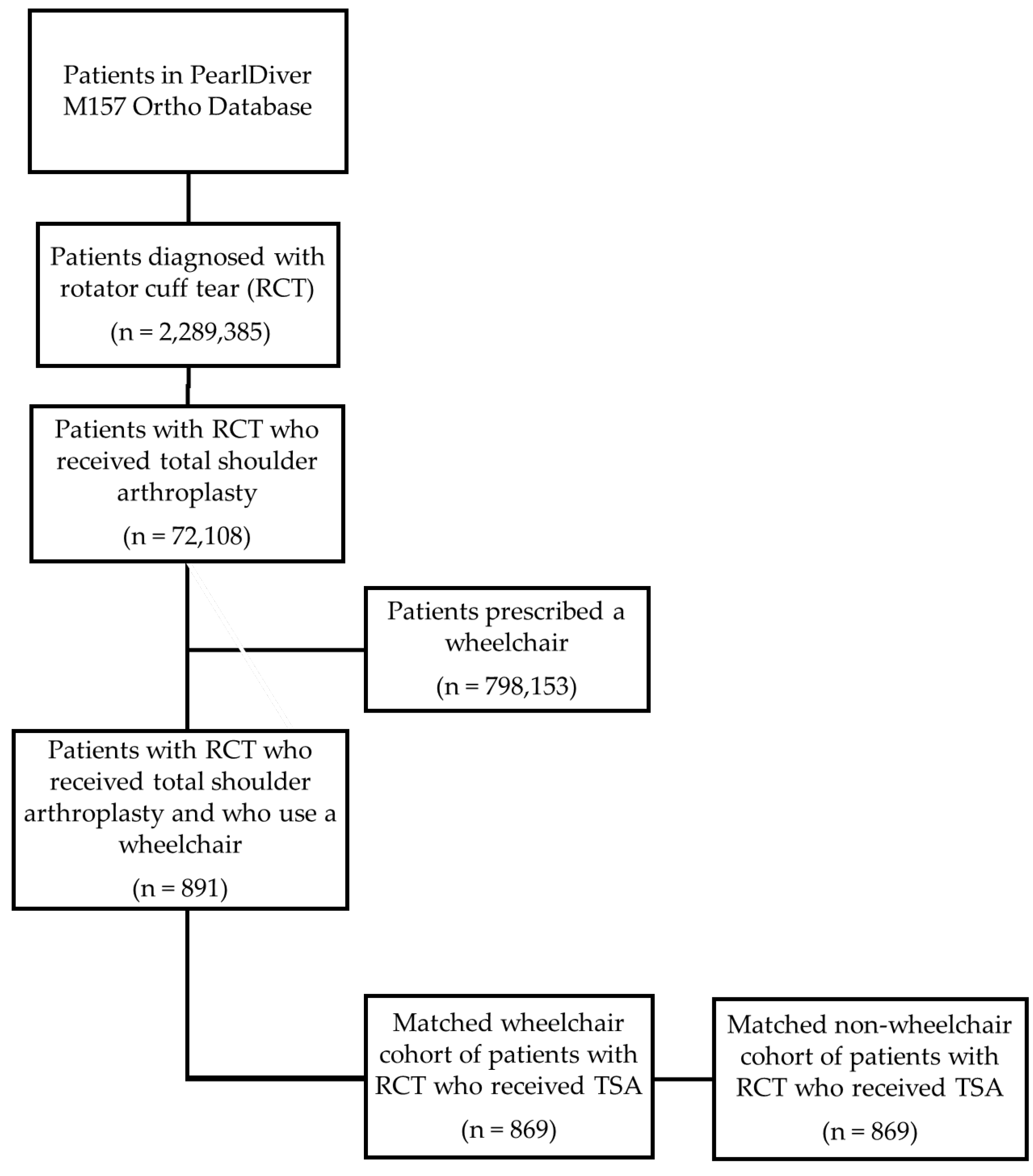
2.2. Creating the Experimental Cohort
2.3. Determining and Comparing the Rates of Readmission, Preoperative Comorbidities, and Postoperative Complications
2.4. Statistical Analysis
3. Results
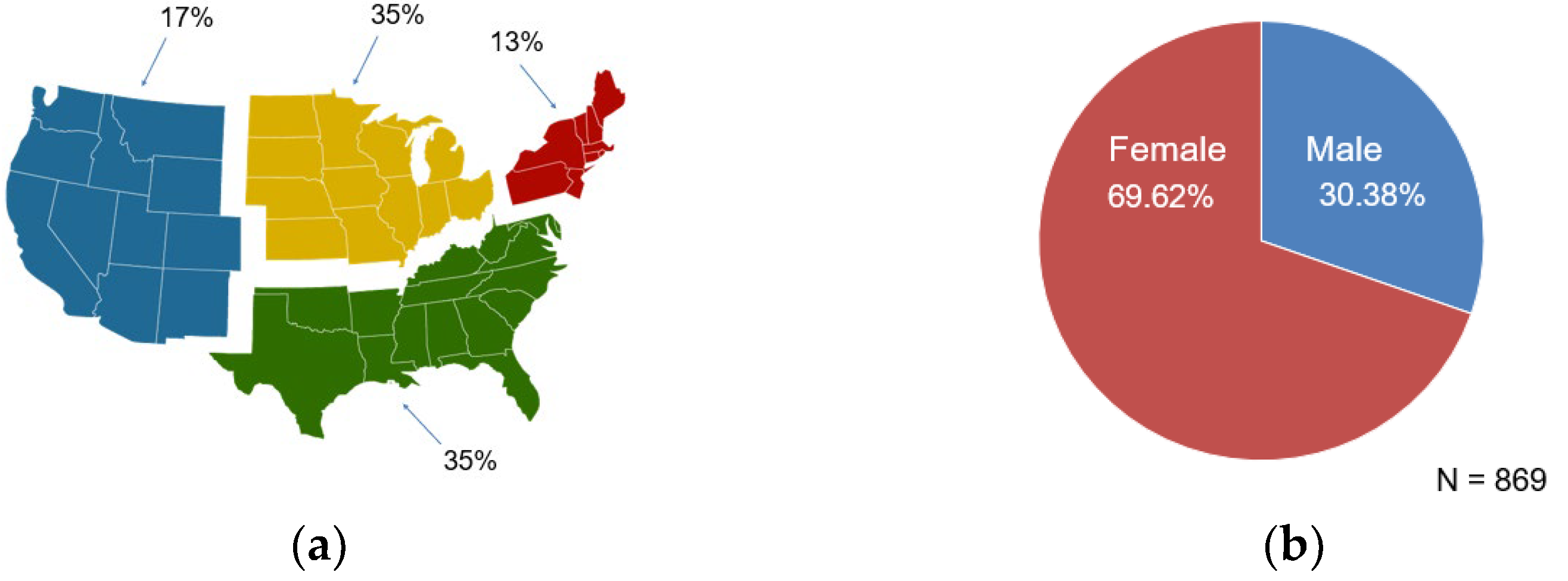
3.1. Demographic Breakdown of Cohorts
3.2. Readmissions
3.3. Postoperative Complications
3.4. Preoperative Comorbidities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karmarkar, A.M.; Dicianno, B.E.; Cooper, R.; Collins, D.M.; Matthews, J.T.; Koontz, A.; Teodorski, E.E.; Cooper, R.A. Demographic profile of older adults using wheeled mobility devices. J. Aging Res. 2011, 2011, 560358. [Google Scholar] [CrossRef] [PubMed]
- Okoro, C.A.; Hollis, N.D.; Cyrus, A.C.; Griffin-Blake, S. Prevalence of Disabilities and Health Care Access by Disability Status and Type Among Adults—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.B.; Higgins, L.D.; Katz, J.N.; Garshick, E. Association of shoulder pain with the use of mobility devices in persons with chronic spinal cord injury. PM R 2010, 2, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.W.; Sloan, R.; Saithna, A. Should we avoid shoulder surgery in wheelchair users? A systematic review of outcomes and complications. Orthop. Traumatol. Surg. Res. 2018, 104, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Bayley, J.C.; Cochran, T.P.; Sledge, C.B. The weight-bearing shoulder. The impingement syndrome in paraplegics. J. Bone Jt. Surg. Am. 1987, 69, 676–678. [Google Scholar] [CrossRef]
- Kulig, K.; Rao, S.S.; Mulroy, S.J.; Newsam, C.J.; Gronley, J.K.; Bontrager, E.L.; Perry, J. Shoulder joint kinetics during the push phase of wheelchair propulsion. Clin. Orthop. Relat. Res. 1998, 354, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Pentland, W.E.; Twomey, L.T. Upper limb function in persons with long term paraplegia and implications for independence: Part I. Paraplegia 1994, 32, 211–218. [Google Scholar] [CrossRef]
- Riley, A.H.; Callahan, C. Shoulder Rehabilitation Protocol and Equipment Fit Recommendations for the Wheelchair Sport Athlete with Shoulder Pain. Sports Med. Arthrosc. Rev. 2019, 27, 67–72. [Google Scholar] [CrossRef]
- Macaulay, A.A.; Greiwe, R.M.; Bigliani, L.U. Rotator cuff deficient arthritis of the glenohumeral joint. Clin. Orthop. Surg. 2010, 2, 196–202. [Google Scholar] [CrossRef]
- Ansok, C.B.; Muh, S.J. Optimal management of glenohumeral osteoarthritis. Orthop. Res. Rev. 2018, 10, 9–18. [Google Scholar] [CrossRef]
- Morgenroth, D.C.; Gellhorn, A.C.; Suri, P. Osteoarthritis in the disabled population: A mechanical perspective. PM R 2012, 4, S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Mohamadi, A.; Chan, J.J.; Claessen, F.M.; Ring, D.; Chen, N.C. Corticosteroid Injections Give Small and Transient Pain Relief in Rotator Cuff Tendinosis: A Meta-analysis. Clin. Orthop. Relat. Res. 2017, 475, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Valiquette, A.M.; Graf, A.R.; Mickschl, D.J.; Zganjar, A.J.; Grindel, S.I. Rotator cuff repair in upper extremity ambulators: An assessment of longitudinal outcomes. JSES Int. 2022, 6, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, B.; Young, J.; Escobedo, E.M. Rotator cuff repairs in individuals with paraplegia. Am. J. Phys. Med. Rehabil. 1997, 76, 316–322. [Google Scholar] [CrossRef]
- Mattei, L.; Mortera, S.; Arrigoni, C.; Castoldi, F. Anatomic shoulder arthroplasty: An update on indications, technique, results and complication rates. Joints 2015, 3, 72–77. [Google Scholar] [CrossRef]
- Akbar, M.; Balean, G.; Brunner, M.; Seyler, T.M.; Bruckner, T.; Munzinger, J.; Grieser, T.; Gerner, H.J.; Loew, M. Prevalence of rotator cuff tear in paraplegic patients compared with controls. J. Bone Jt. Surg. Am. 2010, 92, 23–30. [Google Scholar] [CrossRef]
- Guest, J.; Datta, N.; Jimsheleishvili, G.; Gater, D.R., Jr. Pathophysiology, Classification and Comorbidities after Traumatic Spinal Cord Injury. J. Pers. Med. 2022, 12, 1126. [Google Scholar] [CrossRef]
- Montesinos-Magraner, L.; Serra-Ano, P.; Garcia-Masso, X.; Ramirez-Garceran, L.; Gonzalez, L.M.; Gonzalez-Viejo, M.A. Comorbidity and physical activity in people with paraplegia: A descriptive cross-sectional study. Spinal Cord. 2018, 56, 52–56. [Google Scholar] [CrossRef]
- Selph, S.S.; Skelly, A.C.; Wasson, N.; Dettori, J.R.; Brodt, E.D.; Ensrud, E.; Elliot, D.; Dissinger, K.M.; McDonagh, M. Physical Activity and the Health of Wheelchair Users: A Systematic Review in Multiple Sclerosis, Cerebral Palsy, and Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2021, 102, 2464–2481.e2433. [Google Scholar] [CrossRef]
- Shin, K.C. Physical activity in chronic obstructive pulmonary disease: Clinical impact and risk factors. Korean J. Intern. Med. 2018, 33, 75–77. [Google Scholar] [CrossRef]
- Mallamaci, F.; Pisano, A.; Tripepi, G. Physical activity in chronic kidney disease and the EXerCise Introduction to Enhance Trial. Nephrol. Dial. Transplant. 2020, 35, ii18–ii22. [Google Scholar] [CrossRef]
- Daste, C.; Kirren, Q.; Akoum, J.; Lefevre-Colau, M.M.; Rannou, F.; Nguyen, C. Physical activity for osteoarthritis: Efficiency and review of recommandations. Jt. Bone Spine 2021, 88, 105207. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, B.; Busch, A.; Dunsiger, S. Cigarette smoking among adults with mobility impairments: A US population-based survey. Am. J. Public Health 2014, 104, 1943–1949. [Google Scholar] [CrossRef] [PubMed]
- Weill-Engerer, S.; Meaume, S.; Lahlou, A.; Piette, F.; Saint-Jean, O.; Sachet, A.; Beinis, J.Y.; Gallinari, C.; Grancher, A.S.; Vincent, J.P.; et al. Risk factors for deep vein thrombosis in inpatients aged 65 and older: A case-control multicenter study. J. Am. Geriatr. Soc. 2004, 52, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Stahl, A.; Westerdahl, E. Postoperative Physical Therapy to Prevent Hospital-acquired Pneumonia in Patients over 80 Years Undergoing Hip Fracture Surgery—A Quasi-experimental Study. Clin. Interv. Aging 2020, 15, 1821–1829. [Google Scholar] [CrossRef]
- Rogers, M.A.; Fries, B.E.; Kaufman, S.R.; Mody, L.; McMahon, L.F., Jr.; Saint, S. Mobility and other predictors of hospitalization for urinary tract infection: A retrospective cohort study. BMC Geriatr. 2008, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, V.K.; Fernandez, S.J.; Evans, K.K.; McNish, S.; Banerjee, A.N.; Couch, K.S.; Mete, M.; Shara, N. Postoperative wound dehiscence: Predictors and associations. Wound Repair Regen. 2015, 23, 184–190. [Google Scholar] [CrossRef]
- Chung, A.S.; Makovicka, J.L.; Hydrick, T.; Scott, K.L.; Arvind, V.; Hattrup, S.J. Analysis of 90-Day Readmissions after Total Shoulder Arthroplasty. Orthop. J. Sports Med. 2019, 7, 2325967119868964. [Google Scholar] [CrossRef]
- Schairer, W.W.; Zhang, A.L.; Feeley, B.T. Hospital readmissions after primary shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 1349–1355. [Google Scholar] [CrossRef]
- Lu, Y.; Oeding, J.F.; Parkes, C.; Patel, H.; Berlinberg, E.; Forsythe, B.; Camp, C.L.; Sanchez-Sotelo, J. Incidence and 30- and 90-day readmission rates after primary shoulder arthroplasty in the United States: An analysis using the National Readmissions Database. J. Shoulder Elb. Surg. 2023, 32, 1174–1184. [Google Scholar] [CrossRef]
- Najmanova, K.; Neuhauser, C.; Krebs, J.; Baumberger, M.; Schaefer, D.J.; Sailer, C.O.; Wettstein, R.; Scheel-Sailer, A. Risk factors for hospital acquired pressure injury in patients with spinal cord injury during first rehabilitation: Prospective cohort study. Spinal Cord. 2022, 60, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Bethge, M.; von Groote, P.; Giustini, A.; Gutenbrunner, C. The World Report on Disability: A Challenge for Rehabilitation Medicine. Am. J. Phys. Med. Rehabil. 2014, 93, S4–S11. [Google Scholar] [CrossRef] [PubMed]
- Gologorsky, Y.; Knightly, J.J.; Lu, Y.; Chi, J.H.; Groff, M.W. Improving discharge data fidelity for use in large administrative databases. Neurosurg. Focus 2014, 36, E2. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Range (Years) | Number of Patients in Each Age Range | Percentage of Patients in Each Age Range |
|---|---|---|
| 35–39 | * | * |
| 40–44 | * | * |
| 45–49 | 11 | 1.27% |
| 50–54 | 28 | 3.22% |
| 55–59 | 74 | 8.52% |
| 60–64 | 127 | 14.61% |
| 65–69 | 159 | 18.30% |
| 70–74 | 194 | 22.32% |
| 75–79 | 211 | 24.28% |
| 80+ | 56 | 6.44% |
| Mean age + SD: 75.1 ± 4.1 | ||
| Wheelchair Users (n = 869) | Non-Wheelchair Users (n = 869) | Odds Ratio | 95% CI | p-Value | |||
|---|---|---|---|---|---|---|---|
| Readmissions following TSA | 209 | 24.05% | 83 | 9.55% | 2.9988 | 2.2788, 3.9462 | <0.0001 |
| Comorbidity | Readmission Within 1 Year (n = 209) | No Readmission (n = 660) | p-Value | ||
|---|---|---|---|---|---|
| Osteoarthritis | 79 | 37.80% | 296 | 44.85% | 0.0367 * |
| Rheumatoid arthritis | 17 | 8.13% | 34 | 5.15% | 0.0565 |
| Asthma | 36 | 17.22% | 114 | 17.27% | 0.4936 |
| Hypertension | 171 | 81.82% | 530 | 80.30% | 0.3144 |
| Ischemic heart disease | 16 | 7.66% | 38 | 5.76% | 0.0114 * |
| Pulmonary heart disease | 35 | 16.75% | 52 | 7.88% | 0.0002 * |
| Obesity | 83 | 39.71% | 251 | 38.03% | 0.3315 |
| Diabetes | 92 | 44.02% | 272 | 41.21% | 0.2367 |
| Coronary artery disease | 67 | 32.06% | 202 | 30.61% | 0.3462 |
| Chronic kidney disease | 60 | 28.71% | 150 | 22.73% | 0.0392 * |
| Tobacco use | 69 | 33.01% | 243 | 36.82% | 0.1589 |
| Myocardial infarction | 26 | 12.44% | 61 | 9.24% | 0.0898 |
| Anemia | 11 | 5.26% | 26 | 3.94% | 0.2044 |
| Arrhythmia | 76 | 36.36% | 192 | 29.09% | 0.0236 * |
| Arthroplasty | Wheelchair Users (n = 869) | Non-Wheelchair Users (n = 869) | OR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|---|
| Postoperative complications | |||||||
| Urinary tract infection | 291 | 33.49% | 108 | 12.43% | 3.5475 | 2.7742, 4.5365 | <0.0001 * |
| Pneumonia | 148 | 17.03% | 49 | 5.64% | 3.4351 | 2.4495, 4.8174 | <0.0001 * |
| Acute kidney injury | 170 | 19.56% | 44 | 5.06% | 4.5601 | 3.2247, 6.4484 | <0.0001 * |
| Deep vein thrombosis | 31 | 3.57% | 18 | 2.07% | 1.7489 | 0.9708, 3.1506 | 0.0180 * |
| Wound disruption | 24 | 2.76% | 11 | 1.27% | 2.2154 | 1.0784, 4.5511 | 0.0076 * |
| Preoperative comorbidities | |||||||
| Myocardial infarction | 99 | 11.39% | 50 | 5.75% | 2.1060 | 1.4781, 3.0005 | <0.0001 * |
| Anemia | 48 | 5.52% | 19 | 2.19% | 2.6156 | 1.5245, 4.4876 | 0.0001 * |
| Arrhythmia | 288 | 33.14% | 147 | 16.92% | 2.4346 | 1.9408, 3.0542 | <0.0001 * |
| Opioid use | 646 | 74.34% | 674 | 77.56% | 0.8381 | 0.6723, 1.0448 | 0.0581 |
| Osteoarthritis | 425 | 48.91% | 275 | 31.65% | 2.0676 | 1.7008, 2.5134 | <0.0001 * |
| Rheumatoid arthritis | 58 | 6.67% | 31 | 3.57% | 1.9333 | 1.2369, 3.0217 | 0.0009 * |
| Asthma | 163 | 18.76% | 95 | 10.93% | 1.8810 | 1.4320, 2.4710 | <0.0001 * |
| Hypertension | 725 | 83.43% | 576 | 66.28% | 2.5611 | 2.0399, 3.2153 | <0.0001 * |
| Ischemic heart disease | 65 | 7.48% | 21 | 2.42% | 3.2646 | 1.9774, 5.3897 | <0.0001 * |
| Pulmonary heart disease | 100 | 11.51% | 40 | 4.60% | 2.6951 | 1.8438, 3.9393 | <0.0001 * |
| Obesity | 367 | 42.23% | 203 | 23.36% | 2.3985 | 1.9502, 2.9499 | <0.0001 * |
| Diabetes | 384 | 44.19% | 210 | 24.17% | 2.4846 | 2.0240, 3.0501 | <0.0001 * |
| COPD | 281 | 32.34% | 135 | 15.54% | 2.5983 | 2.0600, 3.2773 | <0.0001 * |
| Coronary artery disease | 286 | 32.91% | 178 | 20.48% | 1.9044 | 1.5326, 2.3663 | <0.0001 * |
| Chronic kidney disease | 235 | 27.04% | 126 | 14.50% | 2.1857 | 1.7177, 2.7813 | <0.0001 * |
| Tobacco use | 346 | 39.82% | 228 | 26.24% | 1.8599 | 1.5179, 2.2790 | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prabhu, K.; Nasr, A.J.; Kasitinon, D.; Cabrera, A.; Lin, Y.-S. Perioperative Outcomes, Comorbidities, and Complications following Total Shoulder Arthroplasty in Wheelchair Users: A Retrospective Cohort Analysis of a Nationwide Database. J. Clin. Med. 2023, 12, 5799. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185799
Prabhu K, Nasr AJ, Kasitinon D, Cabrera A, Lin Y-S. Perioperative Outcomes, Comorbidities, and Complications following Total Shoulder Arthroplasty in Wheelchair Users: A Retrospective Cohort Analysis of a Nationwide Database. Journal of Clinical Medicine. 2023; 12(18):5799. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185799
Chicago/Turabian StylePrabhu, Kevin, Andrew J. Nasr, Donald Kasitinon, Alison Cabrera, and Yen-Sheng Lin. 2023. "Perioperative Outcomes, Comorbidities, and Complications following Total Shoulder Arthroplasty in Wheelchair Users: A Retrospective Cohort Analysis of a Nationwide Database" Journal of Clinical Medicine 12, no. 18: 5799. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12185799