
Comparison of Antero-Lateral Thigh Flap and Vastus Lateralis Muscle Flap for the Treatment of Extensive Scalp Defects—A Retrospective Cohort Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Acquisition
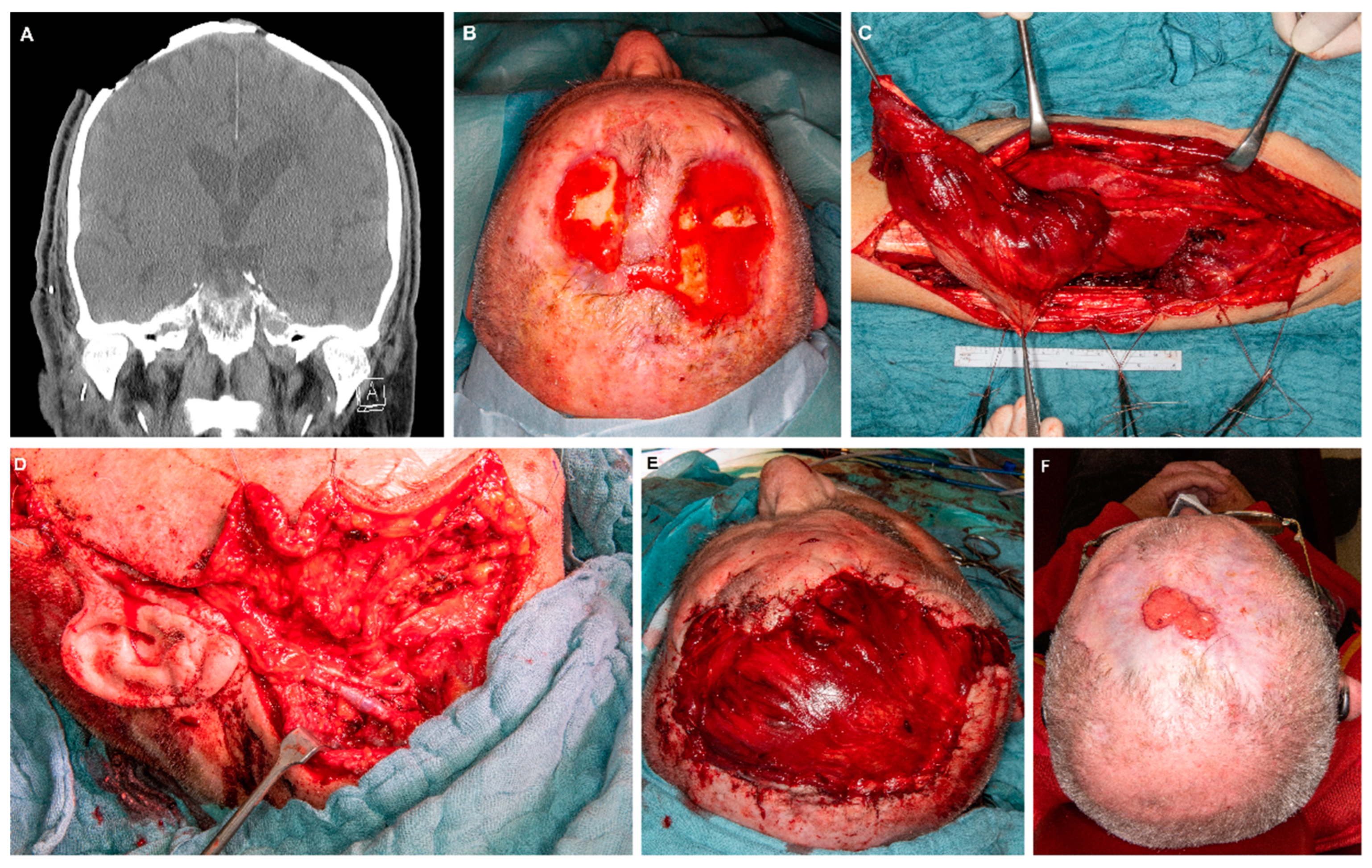
2.2. Surgical Procedures
2.3. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Surgical Procedures and Perioperative Management
3.3. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwarcinski, J.; Boughton, P.; van Gelder, J.; Damodaran, O.; Doolan, A.; Ruys, A. Clinical evaluation of rapid 3D print-formed implants for surgical reconstruction of large cranial defects. ANZ J. Surg. 2021, 91, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.S. The reconstructive ladder. An orthoplastic approach. Orthop. Clin. N. Am. 1993, 24, 393–409. [Google Scholar] [CrossRef]
- Urken, M.L.; Weinberg, H.; Buchbinder, D.; Moscoso, J.F.; Lawson, W.; Catalano, P.J.; Biller, H.F. Microvascular free flaps in head and neck reconstruction. Report of 200 cases and review of complications. Arch. Otolaryngol. Head. Neck Surg. 1994, 120, 633–640. [Google Scholar] [CrossRef] [PubMed]
- McConnel, F.M.; Pauloski, B.R.; Logemann, J.A.; Rademaker, A.W.; Colangelo, L.; Shedd, D.; Carroll, W.; Lewin, J.; Johnson, J. Functional results of primary closure vs flaps in oropharyngeal reconstruction: A prospective study of speech and swallowing. Arch. Otolaryngol. Head. Neck Surg. 1998, 124, 625–630. [Google Scholar] [CrossRef]
- Tanaka, Y.; Matsumoto, K.; Song, S.; Tajima, S.; Ohmura, T. Reconstruction of a cranial bone defect with hydroxyapatite and free flap transfer. J. Craniofac. Surg. 1997, 8, 141–145. [Google Scholar] [CrossRef]
- Baumeister, S.; Peek, A.; Friedman, A.; Levin, L.S.; Marcus, J.R. Management of postneurosurgical bone flap loss caused by infection. Plast. Reconstr. Surg. 2008, 122, 195e–208e. [Google Scholar] [CrossRef]
- Weitz, J.; Spaas, C.; Wolff, K.D.; Meyer, B.; Shiban, E.; Ritschl, L.M. A Standard Algorithm for Reconstruction of Scalp Defects With Simultaneous Free Flaps in an Interdisciplinary Two-Team Approach. Front. Oncol. 2019, 9, 1130. [Google Scholar] [CrossRef]
- Zhou, W.; Zhang, W.B.; Yu, Y.; Wang, Y.; Mao, C.; Guo, C.B.; Yu, G.Y.; Peng, X. Risk factors for free flap failure: A retrospective analysis of 881 free flaps for head and neck defect reconstruction. Int. J. Oral. Maxillofac. Surg. 2017, 46, 941–945. [Google Scholar] [CrossRef]
- Mucke, T.; Rau, A.; Weitz, J.; Ljubic, A.; Rohleder, N.; Wolff, K.D.; Mitchell, D.A.; Kesting, M.R. Influence of irradiation and oncologic surgery on head and neck microsurgical reconstructions. Oral Oncol. 2012, 48, 367–371. [Google Scholar] [CrossRef]
- Iblher, N.; Ziegler, M.C.; Penna, V.; Eisenhardt, S.U.; Stark, G.B.; Bannasch, H. An algorithm for oncologic scalp reconstruction. Plast. Reconstr. Surg. 2010, 126, 450–459. [Google Scholar] [CrossRef]
- Steiner, D.; Horch, R.E.; Eyupoglu, I.; Buchfelder, M.; Arkudas, A.; Schmitz, M.; Ludolph, I.; Beier, J.P.; Boos, A.M. Reconstruction of composite defects of the scalp and neurocranium-a treatment algorithm from local flaps to combined AV loop free flap reconstruction. World J. Surg. Oncol. 2018, 16, 217. [Google Scholar] [CrossRef] [PubMed]
- Goertz, O.; von der Lohe, L.; Martinez-Olivera, R.; Daigeler, A.; Harati, K.; Hirsch, T.; Lehnhardt, M.; Kolbenschlag, J. Microsurgical Reconstruction of Extensive Oncological Scalp Defects. Front. Surg. 2015, 2, 44. [Google Scholar] [CrossRef] [PubMed]
- Lamaris, G.A.; Knackstedt, R.; Couto, R.A.; Abedi, N.; Durand, P.; Gastman, B. The Anterolateral Thigh Flap as the Flap of Choice for Scalp Reconstruction. J. Craniofac. Surg. 2017, 28, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Simunovic, F.; Eisenhardt, S.U.; Penna, V.; Thiele, J.R.; Stark, G.B.; Bannasch, H. Microsurgical reconstruction of oncological scalp defects in the elderly. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 912–919. [Google Scholar] [CrossRef]
- Nassif, T.M.; Vidal, L.; Bovet, J.L.; Baudet, J. The parascapular flap: A new cutaneous microsurgical free flap. Plast. Reconstr. Surg. 1982, 69, 591–600. [Google Scholar] [CrossRef]
- van Driel, A.A.; Mureau, M.A.M.; Goldstein, D.P.; Gilbert, R.W.; Irish, J.C.; Gullane, P.J.; Neligan, P.C.; Hofer, S.O.P. Aesthetic and oncologic outcome after microsurgical reconstruction of complex scalp and forehead defects after malignant tumor resection: An algorithm for treatment. Plast. Reconstr. Surg. 2010, 126, 460–470. [Google Scholar] [CrossRef]
- Krishna, B.V.; Green, M.F. Extended role of latissimus dorsi myocutaneous flap in reconstruction of the neck. Br. J. Plast. Surg. 1980, 33, 233–236. [Google Scholar] [CrossRef]
- Patel, R.S.; Makitie, A.A.; Goldstein, D.P.; Gullane, P.J.; Brown, D.; Irish, J.; Gilbert, R.W. Morbidity and functional outcomes following gastro-omental free flap reconstruction of circumferential pharyngeal defects. Head Neck 2009, 31, 655–663. [Google Scholar] [CrossRef]
- Carlson, G.W.; Thourani, V.H.; Codner, M.A.; Grist, W.J. Free gastro-omental flap reconstruction of the complex, irradiated pharyngeal wound. Head Neck 1997, 19, 68–71. [Google Scholar] [CrossRef]
- Schipper, J.; Boedeker, C.C.; Horch, R.E.; Ridder, G.J.; Maier, W. The free vastus lateralis flap for reconstruction in ablative oncologic head and neck surgery. Eur. J. Surg. Oncol. 2006, 32, 103–107. [Google Scholar] [CrossRef]
- Sardesai, M.G.; Yoo, J.H.; Franklin, J.H.; Fung, K. Vastus lateralis muscle-only free flap: Defining its role in head and neck reconstruction. J. Otolaryngol. Head Neck Surg. 2008, 37, 230–234. [Google Scholar] [PubMed]
- Nelson, J.A.; Serletti, J.M.; Wu, L.C. The vastus lateralis muscle flap in head and neck reconstruction: An alternative flap for soft tissue defects. Ann. Plast. Surg. 2010, 64, 28–30. [Google Scholar] [CrossRef]
- Wolff, K.D. Indications for the vastus lateralis flap in oral and maxillofacial surgery. Br. J. Oral. Maxillofac. Surg. 1998, 36, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Wolff, K.D.; Grundmann, A. The free vastus lateralis flap: An anatomic study with case reports. Plast. Reconstr. Surg. 1992, 89, 469–475, discussion 476–467. [Google Scholar] [CrossRef]
- Wolff, K.D.; Howaldt, H.P. Three years of experience with the free vastus lateralis flap: An analysis of 30 consecutive reconstructions in maxillofacial surgery. Ann. Plast. Surg. 1995, 34, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, F.; Oatari, M.; Matsuda, K.; Uehara, M.; Sato, S.; Kato, A. Algorithm for reconstruction of composite cranial defects using the fascial component of free anterolateral thigh flaps. J. Craniofac. Surg. 2013, 24, 1631–1635. [Google Scholar] [CrossRef]
- Sharabi, S.E.; Hatef, D.A.; Koshy, J.C.; Jain, A.; Cole, P.D.; Hollier, L.H., Jr. Is primary thinning of the anterolateral thigh flap recommended? Ann. Plast. Surg. 2010, 65, 555–559. [Google Scholar] [CrossRef]
- Cigna, E.; Minni, A.; Barbaro, M.; Attanasio, G.; Sorvillo, V.; Malzone, G.; Chen, H.C.; Ribuffo, D. An experience on primary thinning and secondary debulking of anterolateral thigh flap in head and neck reconstruction. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1095–1101. [Google Scholar]
- Wolff, K.D.; Kesting, M.; Loffelbein, D.; Holzle, F. Perforator-based anterolateral thigh adipofascial or dermal fat flaps for facial contour augmentation. J. Reconstr. Microsurg. 2007, 23, 497–503. [Google Scholar] [CrossRef]
- Hansen, S.L.; Foster, R.D.; Dosanjh, A.S.; Mathes, S.J.; Hoffman, W.Y.; Leon, P. Superficial temporal artery and vein as recipient vessels for facial and scalp microsurgical reconstruction. Plast. Reconstr. Surg. 2007, 120, 1879–1884. [Google Scholar] [CrossRef]
- Seth, I.; Hewitt, L.; Yabe, T.; Dunn, M.; Wykes, J.; Clark, J.R.; Ashford, B. Assessment of post-surgical donor-site morbidity in vastus lateralis free flap for head and neck reconstructive surgery: An observational study. ANZ J. Surg. 2021, 91, 2738–2743. [Google Scholar] [CrossRef] [PubMed]
- Klinkenberg, M.; Fischer, S.; Kremer, T.; Hernekamp, F.; Lehnhardt, M.; Daigeler, A. Comparison of anterolateral thigh, lateral arm, and parascapular free flaps with regard to donor-site morbidity and aesthetic and functional outcomes. Plast. Reconstr. Surg. 2013, 131, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.; Ayeni, O.; Thoma, A. A systematic review of anterolateral thigh flap donor site morbidity. Can. J. Plast. Surg. 2012, 20, 17–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ID | Gender | Age | Reason for Surgery | Prior RT | Used Flap |
|---|---|---|---|---|---|
| 1 | female | 66 | Wound healing disorder (cerebral aneurysm) | No | ALT |
| 2 | male | 96 | Cutaneous SCC | No | ALT |
| 3 | male | 27 | Wound healing disorder (Glioma) | Yes | VL |
| 4 | male | 78 | Cutaneous SCC | No | VL |
| 5 | female | 54 | Melanoma | No | ALT |
| 6 | female | 40 | Wound healing disorder (cerebral aneurysm) | No | VL |
| 7 | male | 78 | Cutaneous SCC | Yes | ALT |
| 8 | female | 80 | Wound healing disorder (Osteomyelitis) | No | ALT |
| 9 | male | 95 | Cutaneous SCC | No | VL |
| 10 | male | 78 | Cutaneous SCC | No | ALT |
| 11 | male | 75 | Cutaneous pleomorphic sarcoma | No | VL |
| 12 | female | 62 | Wound healing disorder (Osteoradionecrosis) | Yes | VL |
| 13 | male | 77 | Cutaneous SCC | No | ALT |
| 14 | female | 40 | Wound healing disorder (Meningioma) | Yes | VL |
| 15 | female | 33 | Wound healing disorder (Glioma) | Yes | VL |
| 16 | female | 65 | Wound healing disorder (cerebral aneurysm) | No | VL |
| 17 | male | 66 | Meningioma | No | ALT |
| 18 | male | 71 | Wound healing disorder (Osteoradionecrosis) | Yes | VL |
| 19 | male | 78 | Cutaneous SCC | No | ALT |
| 20 | male | 60 | Wound healing disorder (Meningioma) | Yes | ALT |
| Medical History of Patients | n (%) | |
|---|---|---|
| Reasons for Cranial Defects | ||
| Wound healing disorder | 10 (50%) | |
| Cerebral aneurysm/SAH | 3 (30%) | |
| Glioma | 2 (20%) | |
| Osteomyelitis | 1 (10%) | |
| Meningioma | 2 (20%) | |
| Osteoradionecrosis | 2 (20%) | |
| Tumors | 10 (50%) | |
| Cutaneous squamous cell carcinoma (SCC) | 8 (80%) | |
| Malignant melanoma | 1 (10%) | |
| Meningioma | 1 (10%) | |
| Relevant comorbidities | ||
| Cardiovascular | 8 (40%) | |
| Metabolic | 9 (45%) | |
| Prior treatment | ||
| 1–3 operations | 6 (30%) | |
| >3 operations | 14 (70%) | |
| Prior radiotherapy | 7 (35%) | |
| Arteries | ALT Flap | VL Flap | Total |
| Superficial temporal artery | 4 (80%) | 1 (20%) | 5 (25%) |
| Facial artery | 4 (50%) | 4 (50%) | 8 (40%) |
| Superior thyroid artery | 2 (40%) | 3 (60%) | 5 (25%) |
| Lingual artery | - | 2 (100%) | 2 (10%) |
| Veins | ALT Flap | VL Flap | Total |
| Superficial temporal vein | 4 (80%) | 1 (20%) | 5 (25%) |
| Facial vein | 1 (20%) | 4 (80%) | 5 (25%) |
| Internal jugular vein | 4 (50%) | 4 (50%) | 8 (40%) |
| External jugular vein | 1 (50%) | 1 (50%) | 2 (10%) |
| Parameter | ALT Flap | VL Flap | p-Value | |
|---|---|---|---|---|
| Indication for surgery | Tumor | 6 (60%) | 4 (40%) | 0.371 |
| Wound healing disorder | 4 (40%) | 6 (60%) | ||
| Closure of donor site | Primary closure | 8 (80%) | 10 (100%) | 0.136 |
| Secondary closure | 2 (20%) | - | ||
| Flap revision | Yes | 1 (10%) | - | 0.305 |
| No | 9 (90%) | 10 (100%) | ||
| Major complications | Yes | 2 (20%) | 2 (20%) | 1.0 |
| No | 8 (80%) | 8 (80%) | ||
| Hospitalization, surgery time and defect sizes | p-Value | |||
| Mean surgery time (minutes) | 288 (±81) | 258 (±59) | 0.351 | |
| Hospitalization—ICU (days) | 10 (±20) | 5 (±7) | 0.476 | |
| Hospitalization (days) | 22 (±17) | 14 (±5) | 0.180 | |
| Mean defect sizes | 154 ± 61 | 152 ± 21 | 0.962 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moratin, J.; Dao Trong, P.; Semmelmayer, K.; Mrosek, J.; Zittel, S.; Bleymehl, M.; Ristow, O.; Freudlsperger, C.; Hoffmann, J.; Engel, M. Comparison of Antero-Lateral Thigh Flap and Vastus Lateralis Muscle Flap for the Treatment of Extensive Scalp Defects—A Retrospective Cohort Study. J. Clin. Med. 2023, 12, 6208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12196208
Moratin J, Dao Trong P, Semmelmayer K, Mrosek J, Zittel S, Bleymehl M, Ristow O, Freudlsperger C, Hoffmann J, Engel M. Comparison of Antero-Lateral Thigh Flap and Vastus Lateralis Muscle Flap for the Treatment of Extensive Scalp Defects—A Retrospective Cohort Study. Journal of Clinical Medicine. 2023; 12(19):6208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12196208
Chicago/Turabian StyleMoratin, Julius, Philip Dao Trong, Karl Semmelmayer, Jan Mrosek, Sven Zittel, Moritz Bleymehl, Oliver Ristow, Christian Freudlsperger, Jürgen Hoffmann, and Michael Engel. 2023. "Comparison of Antero-Lateral Thigh Flap and Vastus Lateralis Muscle Flap for the Treatment of Extensive Scalp Defects—A Retrospective Cohort Study" Journal of Clinical Medicine 12, no. 19: 6208. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12196208