
Robotic versus Conventional Overground Gait Training in Subacute Stroke Survivors: A Multicenter Controlled Clinical Trial
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
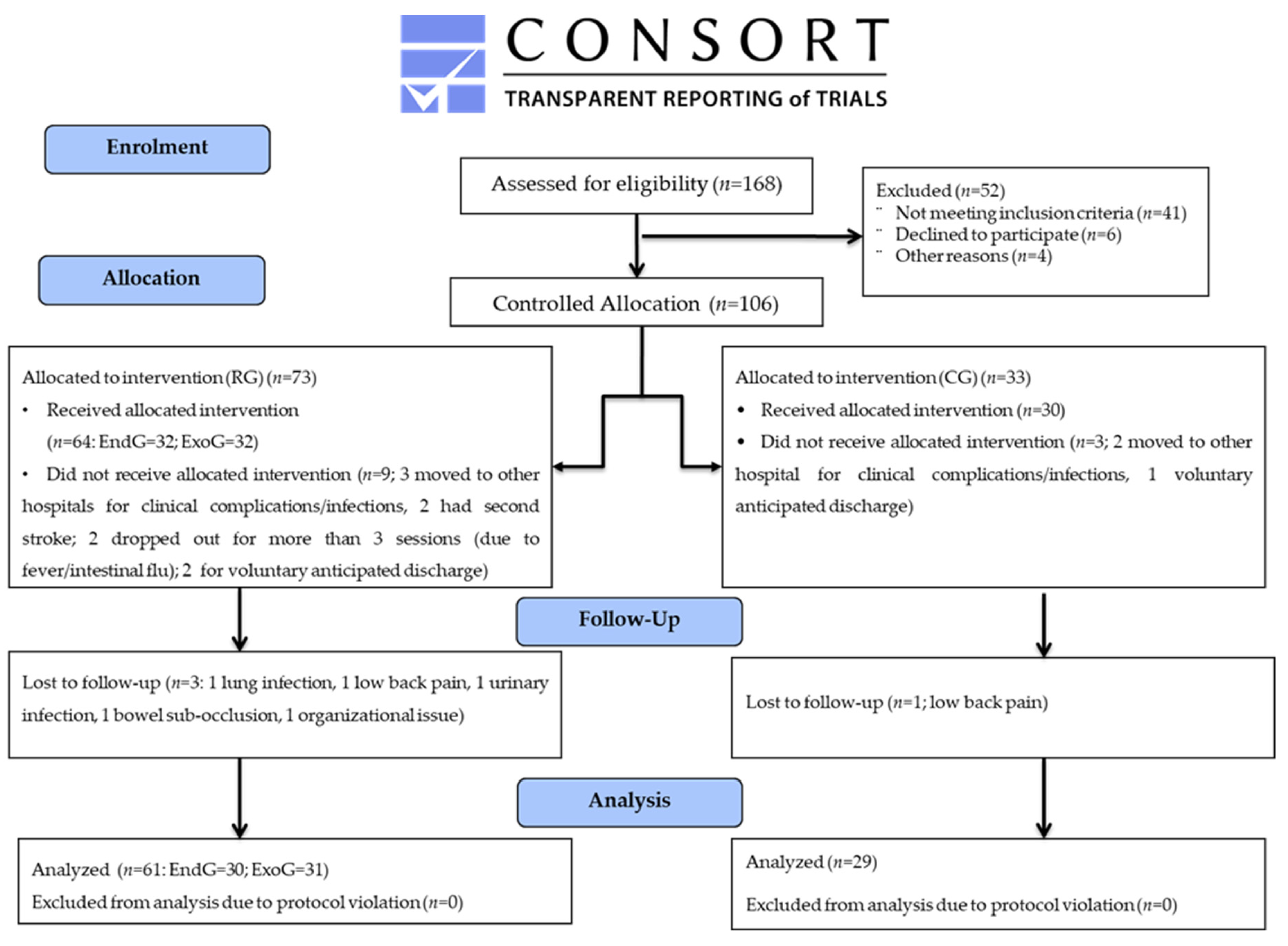
2.1. Study Design
2.2. Participants
2.3. Rehabilitation Intervention
2.3.1. Stationary Robot-Assisted Gait Training
2.3.2. Conventional Overground Gait Training
2.4. Outcome Measures
2.5. Ethical Aspects
2.6. Statistical Analysis
2.7. Data Availability
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thrift, A.G.; Srikanth, V.K.; Nelson, M.R.; Kim, J.; Fitzgerald, S.; Gerraty, R.P.; Bladin, C.F.; Phan, T.G.; Cadilhac, D.A. Risk Factor Management in Survivors of Stroke: A Double-Blind, Cluster-Randomized, Controlled Trial. Int. J. Stroke 2012, 9, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Dobkin, B.H. Rehabilitation after Stroke. N. Engl. J. Med. 2005, 352, 1677–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.-W.; Kim, Y.-N.; Lee, D.-K. Effect of a virtual reality exercise program accompanied by cognitive tasks on the balance and gait of stroke patients. J. Phys. Ther. Sci. 2015, 27, 2175–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Port, I.; Kwakkel, G.; Lindeman, E. Community ambulation in patients with chronic stroke: How is it related to gait speed? J. Rehabil. Med. 2008, 40, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Rosa, M.C.; Marques, A.; Demain, S.; Metcalf, C.D. Fast gait speed and self-perceived balance as valid predictors and discriminators of independent community walking at 6 months post-stroke—A preliminary study. Disabil. Rehabil. 2014, 37, 129–134. [Google Scholar] [CrossRef]
- Vahlberg, B.; Cederholm, T.; Lindmark, B.; Zetterberg, L.; Hellström, K. Factors Related to Performance-Based Mobility and Self-reported Physical Activity in Individuals 1-3 Years after Stroke: A Cross-sectional Cohort Study. J. Stroke Cerebrovasc. Dis. 2013, 22, e426–e434. [Google Scholar] [CrossRef]
- Pihlaja, R.; Uimonen, J.; Mustanoja, S.; Tatlisumak, T.; Poutiainen, E. Post-stroke fatigue is associated with impaired processing speed and memory functions in first-ever stroke patients. J. Psychosom. Res. 2014, 77, 380–384. [Google Scholar] [CrossRef]
- Rand, D.; Eng, J.J.; Liu-Ambrose, T.; Tawashy, A.E. Feasibility of a 6-Month Exercise and Recreation Program to Improve Executive Functioning and Memory in Individuals with Chronic Stroke. Neurorehabilit. Neural Repair 2010, 24, 722–729. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Chollet, F.; Albucher, J.-F. Strategies to Augment Recovery after Stroke. Curr. Treat. Options Neurol. 2012, 14, 531–540. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Glenney, S.S. Minimal Clinically Important Difference for Comfortable Speed as a Measure of Gait Performance in Patients Undergoing Inpatient Rehabilitation after Stroke. J. Phys. Ther. Sci. 2013, 25, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Taqi, M.A.; Vora, N.; Callison, R.C.; Lin, R.; Wolfe, T.J. Past, present, and future of endovascular stroke therapies. Neurology 2012, 79, S213–S220. [Google Scholar] [CrossRef] [Green Version]
- Paolucci, S.; Bragoni, M.; Coiro, P.; De Angelis, D.; Fusco, F.R.; Morelli, D.; Venturiero, V.; Pratesi, L. Quantification of the Probability of Reaching Mobility Independence at Discharge from a Rehabilitation Hospital in Nonwalking Early Ischemic Stroke Patients: A Multivariate Study. Cerebrovasc. Dis. 2008, 26, 16–22. [Google Scholar] [CrossRef]
- Pintado-Izquierdo, S.; Cano-De-La-Cuerda, R.; Ortiz-Gutiérrez, R. Video Game-Based Therapy on Balance and Gait of Patients with Stroke: A Systematic Review. Appl. Sci. 2020, 10, 6426. [Google Scholar] [CrossRef]
- Goffredo, M.; Guanziroli, E.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Damiani, C.; Franceschini, M.; Molteni, F.; et al. Overground wearable powered exoskeleton for gait training in subacute stroke subjects: Clinical and gait assessments. Eur. J. Phys. Rehabil. Med. 2020, 55, 710–721. [Google Scholar] [CrossRef]
- Mazzucchelli, M.; Mazzoleni, D.; Campanini, I.; Merlo, A.; Mazzoli, D.; Melegari, C.; Colombo, V.; Cerulli, S.; Piscitelli, D.; Perin, C.; et al. Evidence-based improvement of gait in post-stroke patients following robot-assisted training: A systematic review. NeuroRehabilitation 2022, 51, 595–608. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; DeRuyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Goffredo, M.; Iacovelli, C.; Russo, E.; Pournajaf, S.; Di Blasi, C.; Galafate, D.; Pellicciari, L.; Agosti, M.; Filoni, S.; Aprile, I.; et al. Stroke Gait Rehabilitation: A Comparison of End-Effector, Overground Exoskeleton, and Conventional Gait Training. Appl. Sci. 2019, 9, 2627. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021, 11, 104. [Google Scholar] [CrossRef]
- Bae, Y.-H.; Ko, Y.J.; Chang, W.H.; Lee, J.H.; Lee, K.B.; Park, Y.J.; Ha, H.G.; Kim, Y.-H. Effects of Robot-assisted Gait Training Combined with Functional Electrical Stimulation on Recovery of Locomotor Mobility in Chronic Stroke Patients: A Randomized Controlled Trial. J. Phys. Ther. Sci. 2014, 26, 1949–1953. [Google Scholar] [CrossRef]
- Sale, P.; Franceschini, M.; Waldner, A.; Hesse, S. Use of the robot assisted gait therapy in rehabilitation of patients with stroke and spinal cord injury. Eur. J. Phys. Rehabil. Med. 2012, 48, 111–121. [Google Scholar] [PubMed]
- Bruni, M.F.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. What does best evidence tell us about robotic gait rehabilitation in stroke patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2018, 48, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, CD006185. [Google Scholar] [CrossRef] [PubMed]
- Haarman, J.A.; Reenalda, J.; Buurke, J.H.; van der Kooij, H.; Rietman, J.S. The effect of ‘device-in-charge’ versus ‘patient-in-charge’ support during robotic gait training on walking ability and balance in chronic stroke survivors: A systematic review. J. Rehabil. Assist. Technol. Eng. 2016, 3, 2055668316676785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickstein, R. Rehabilitation of gait speed after stroke: A critical review of intervention approaches. Neurorehabilit. Neural Repair 2008, 22, 649–660. [Google Scholar] [CrossRef]
- Lissom, L.O.; Lamberti, N.; Lavezzi, S.; Basaglia, N.; Manfredini, F.; Straudi, S. Is robot-assisted gait training intensity a determinant of functional recovery early after stroke? A pragmatic observational study of clinical care. Int. J. Rehabil. Res. 2022, 45, 189–194. [Google Scholar] [CrossRef]
- Lamberti, N.; Manfredini, F.; Lissom, L.O.; Lavezzi, S.; Basaglia, N.; Straudi, S. Beneficial Effects of Robot-Assisted Gait Training on Functional Recovery in Women after Stroke: A Cohort Study. Medicina 2021, 57, 1200. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Cacciola, A.; Bertè, F.; Manuli, A.; Leo, A.; Bramanti, A.; Naro, A.; Milardi, D.; Bramanti, P. Robotic gait rehabilitation and substitution devices in neurological disorders: Where are we now? Neurol. Sci. 2016, 37, 503–514. [Google Scholar] [CrossRef]
- Bowden, M.G.; Balasubramanian, C.K.; Behrman, A.L.; Kautz, S. Validation of a Speed-Based Classification System Using Quantitative Measures of Walking Performance Poststroke. Neurorehabilit. Neural Repair 2008, 22, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Van Hedel, H.J.; Wirz, M.; Dietz, V. Assessing walking ability in subjects with spinal cord injury: Validity and reliability of 3 walking tests. Arch. Phys. Med. Rehabil. 2005, 86, 190–196. [Google Scholar] [CrossRef]
- Fulk, G.D.; Echternach, J.L. Test-Retest Reliability and Minimal Detectable Change of Gait Speed in Individuals Undergoing Rehabilitation after Stroke. J. Neurol. Phys. Ther. 2008, 32, 8–13. [Google Scholar] [CrossRef]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of Walking Handicap in the Stroke Population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Blackburn, M.; Van Vliet, P.; Mockett, S.P. Reliability of Measurements Obtained with the Modified Ashworth Scale in the Lower Extremities of People with Stroke. Phys. Ther. 2002, 82, 25–34. [Google Scholar] [CrossRef]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive Validity and Responsiveness of the Functional Ambulation Category in Hemiparetic Patients after Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical Gait Assessment in the Neurologically Impaired. Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Shelton, F.D.N.A.P.; Volpe, B.T.; Reding, M. Motor Impairment as a Predictor of Functional Recovery and Guide to Rehabilitation Treatment after Stroke. Neurorehabilit. Neural Repair 2001, 15, 229–237. [Google Scholar] [CrossRef]
- Tal, J. Strategy and Statistics in Clinical Trials: A Non-Statisticians Guide to Thinking, Designing and Executing; Academic Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Brody, T. Clinical Trials: Study Design, Endpoints and Biomarkers, Drug Safety, and FDA and ICH Guidelines; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Hey, S.P.; Kimmelman, J. The questionable use of unequal allocation in confirmatory trials. Neurology 2013, 82, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, M.B.; de Oliveira, C.B.; Dos Santos, A.; Garabello Pires, C.; Dylewski, V.; Arida, R.M. A comparative study of conventional physiotherapy versus robot-assisted gait training associated to physiotherapy in individuals with ataxia after stroke. Behav. Neurol. 2018, 2018, 2892065. [Google Scholar] [CrossRef]
- Alingh, J.F.; Fleerkotte, B.M.; Groen, B.E.; Rietman, J.S.; Weerdesteyn, V.; van Asseldonk, E.H.F.; Geurts, A.C.H.; Buurke, J.H. Effect of assist-as-needed robotic gait training on the gait pattern post stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 26. [Google Scholar] [CrossRef]
- Asiri, F.Y. The effectiveness of robotic-assisted gait training on walking speed for stroke survivors: Meta-analysis. Saudi J. Health Sci. 2018, 7, 143. [Google Scholar] [CrossRef]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef] [PubMed]
- Tedla, J.S.; Dixit, S.; Gular, K.; Abohashrh, M. Robotic-Assisted Gait Training Effect on Function and Gait Speed in Subacute and Chronic Stroke Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Neurol. 2019, 81, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Chanubol, R.; Wongphaet, P.; Werner, C.; Chavanich, N.; Panichareon, L. Gait rehabilitation in subacute hemiparetic stroke: Robot-assisted gait training versus conventional physical therapy. J. Neurol. Sci. 2013, 333, e574. [Google Scholar] [CrossRef]
- Chen, S.-C.; Kang, J.-H.; Peng, C.-W.; Hsu, C.-C.; Lin, Y.-N.; Lai, C.-H. Adjustable Parameters and the Effectiveness of Adjunct Robot-Assisted Gait Training in Individuals with Chronic Stroke. Int. J. Environ. Res. Public Health 2022, 19, 8186. [Google Scholar] [CrossRef]
- Baronchelli, F.; Zucchella, C.; Serrao, M.; Intiso, D.; Bartolo, M. The Effect of Robotic Assisted Gait Training with Lokomat® on Balance Control after Stroke: Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 1073. [Google Scholar] [CrossRef]
- Hidler, J.; Nichols, D.; Pelliccio, M.; Brady, K.; Campbell, D.D.; Kahn, J.H.; Hornby, T.G. Multicenter Randomized Clinical Trial Evaluating the Effectiveness of the Lokomat in Subacute Stroke. Neurorehabilit. Neural Repair 2008, 23, 5–13. [Google Scholar] [CrossRef]
- Schwartz, I.; Meiner, Z. Robotic-Assisted Gait Training in Neurological Patients: Who May Benefit? Ann. Biomed. Eng. 2015, 43, 1260–1269. [Google Scholar] [CrossRef]
- Veerbeek, J.; van Wegen, E.; Van Peppen, R.; Van Der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What Is the Evidence for Physical Therapy Poststroke? A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [Green Version]
- Husemann, B.; Müller, F.; Krewer, C.; Heller, S.; Koenig, E. Effects of locomotion training with assistance of a robot-driven gait orthosis in hemiparetic patients after stroke: A randomized controlled pilot study. Stroke 2007, 38, 349–354. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | RG (n = 61) | CG (n = 28) | p-Value |
|---|---|---|---|
| Age (years) | 59 ± 15 | 63.39 ± 12.85 | 0.2 |
| Sex | 0.9 | ||
| Male | 36 (59%) | 18 (64%) | 0.9 |
| Female | 35 (41%) | 10 (36%) | 0.9 |
| Stroke onset (days) | 48 ± 44 | 58.46 ± 43.24 | 0.2 |
| Affected side | 0.9 | ||
| Right | 28 (46%) | 10 (35.7%) | 0.1 |
| Left | 33 (54%) | 18 (64.3%) | 0.1 |
| Etiology | 0.2 | ||
| Ischemic | 53(87%) | 26 (92.86%) | 0.1 |
| Hemorrhagic | 8 (13%) | 2 (7.14%) | 0.2 |
| 10 MWT (m/s) * | 0.43 ± 0.37 | 0.43 ± 0.46 | 0.4 |
| MI-LL [0; 100] | 45 [10; 80] | 43 [1; 84] | 0.2 |
| MAS-LL [0; 12] | 1.8 [0; 6] | 0.5 [0; 5.5] | 0.1 |
| 6 MWT (m) | 102 ± 89 | 122 ± 158 | 0.9 |
| TUG (s) | 23 ± 14 | 23 ± 16 | 0.9 |
| FAC [0; 5] | 1.5 [0; 4.5] | 2 [0; 5] | 0.9 |
| mBI [0; 100] | 47 [11; 80] | 43 [7; 91] | 0.5 |
| Variable | RobotEND-Group (n = 30) | RobotEXO-Group (n = 31) | p-Value |
|---|---|---|---|
| Age (years) | 58.03 ± 14.34 | 59.42 ± 15.51 | 0.2 |
| Sex | 0.9 | ||
| Male | 18 (60%) | 18 (58.06%) | 0.9 |
| Female | 12 (40%) | 23 (41.94%) | 0.8 |
| Stroke onset (days) | 33.30 ± 24.79 | 63.68 ± 49.92 | 0.2 |
| Affected side | 0.9 | ||
| Right | 17 (56.67%) | 11 (35.48%) | 0.1 |
| Left | 13 (43.33%) | 20 (64.52%) | 0.1 |
| Etiology | 0.2 | ||
| Ischemic | 27 (90%) | 26 (83.87%) | 0.1 |
| Hemorrhagic | 3 (10%) | 5 (16.13%) | 0.2 |
| 10 MWT (m/s) * | 0.53 ± 0.38 | 0.33 ± 0.37 | 0.1 |
| MI-LL [0; 100] | 48 [1; 76] | 43 [19; 84] | 0.4 |
| MAS-LL [0; 12] | 2 [0; 6] | 1.5 [0; 5] | 0.2 |
| 6 MWT (m) | 121 ± 88 | 83 ± 90 | 0.8 |
| TUG (s) | 23.38 ± 12.13 | 22.21 ± 16.20 | 0.9 |
| FAC [0; 5] | 2 [0; 5] | 1 [0; 4] | 0.8 |
| mBI [0; 100] | 48.5 [11; 75] | 45 [12; 81] | 0.6 |
| Variable | Group | T0 | T1 | Δ | One-Way ANOVA p-Value (F) |
|---|---|---|---|---|---|
| 10 MWT (m/s) * | CG (n = 28) | 0.43 ± 0.46 | 0.57 ± 0.55 | 0.15 ± 0.26 | <0.0001 (F = 17) |
| RG (n = 61) | 0.43 ± 0.37 | 0.72 ± 0.44 | 0.30 ± 0.05 | ||
| MI-LL [0; 100] | CG (n = 28) | 43 [1; 84] | 76 [1; 100] | 33 [27; 42] | 0.03 (F = 4.87) |
| RG (n = 61) | 45 [10; 80] | 83 [38.5; 97] | 38 [15; 50] | ||
| MAS-LL [0; 12] | CG (n = 28) | 0.5 [0; 5.5] | 0 [0; 4.5] | −0.5 [0.25; 2.6] | 0.7 |
| RG (n = 61) | 1.8 [0; 5.5] | 1 [0; 3] | −0.8 [0; −1.5] | ||
| 6 MWT (m) | CG (n = 28) | 122 ± 156 | 172 ± 163 | 49 ± 26 | <0.0001 (F = 112) |
| RG (n = 61) | 102 ± 89 | 194 ± 110 | 92 ± 13 | ||
| TUG (s) | CG (n = 28) | 23 ± 15.9 | 16.2 ± 7.9 | −6.7 ± 1.5 | <0.0001 (F = 109) |
| RG (n = 61) | 22.8 ± 14.2 | 10.2 ± 5.2 | −12.6 ± 4.81 | ||
| FAC [0; 5] | CG (n = 28) | 2 [0; 5] | 3 [0; 5] | 1.0 [0; 4] | 0.9 |
| RG (n = 61) | 1.5 [0; 4.5] | 3.5 [1; 6] | 2 [1; 3] | ||
| mBI [0; 100] | CG (n = 28) | 43 [7; 91] | 84 [20; 100] | 41 [9; 13] | <0.0001 (F = 22.6) |
| RG (n = 61) | 47 [11.5; 79.5] | 89 [40; 95] | 42 [25; 52] | ||
| WHS [1; 6] | CG (n = 28) | n.a. | 3 [1.5; 4.5] | n.a. | n.a. |
| RG (n = 61) | n.a. | 4 [3; 5] | n.a. |
| Variable | RobotEND-Group (n = 30) | RobotEXO-Group (n = 31) | One-Way ANOVA p-Value (F) |
|---|---|---|---|
| Δ10 MWT (m/s) * | 0.4 ± 0.4 | 0.2 ± 0.3 | 0.0007 (F = 13) |
| ΔMI-LL [0; 100] | 14 [0; 76] | 16 [0; 51] | >0.1 |
| ΔMAS-LL [0; 12] | −1 [−3; 0] | −0.5 [−3; 1.5] | >0.1 |
| Δ6 MWT (m) | 112 ± 11 | 71 ± 89 | >0.1 |
| ΔTUG (s) | −6.84 ± 12.11 | −4.55 ± 10.66 | 0.08 |
| ΔFAC [0; 5] | 1 [0; 4] | 1 [0; 3] | >0.1 |
| ΔmBI [0; 100] | 29 [0; 70] | 23 [−12; 65] | >0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pournajaf, S.; Calabrò, R.S.; Naro, A.; Goffredo, M.; Aprile, I.; Tamburella, F.; Filoni, S.; Waldner, A.; Mazzoleni, S.; Focacci, A.; et al. Robotic versus Conventional Overground Gait Training in Subacute Stroke Survivors: A Multicenter Controlled Clinical Trial. J. Clin. Med. 2023, 12, 439. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12020439
Pournajaf S, Calabrò RS, Naro A, Goffredo M, Aprile I, Tamburella F, Filoni S, Waldner A, Mazzoleni S, Focacci A, et al. Robotic versus Conventional Overground Gait Training in Subacute Stroke Survivors: A Multicenter Controlled Clinical Trial. Journal of Clinical Medicine. 2023; 12(2):439. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12020439
Chicago/Turabian StylePournajaf, Sanaz, Rocco Salvatore Calabrò, Antonino Naro, Michela Goffredo, Irene Aprile, Federica Tamburella, Serena Filoni, Andreas Waldner, Stefano Mazzoleni, Antonella Focacci, and et al. 2023. "Robotic versus Conventional Overground Gait Training in Subacute Stroke Survivors: A Multicenter Controlled Clinical Trial" Journal of Clinical Medicine 12, no. 2: 439. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12020439