
Increasing Soluble P-Selectin Levels Predict Higher Peripheral Atherosclerotic Plaque Progression
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
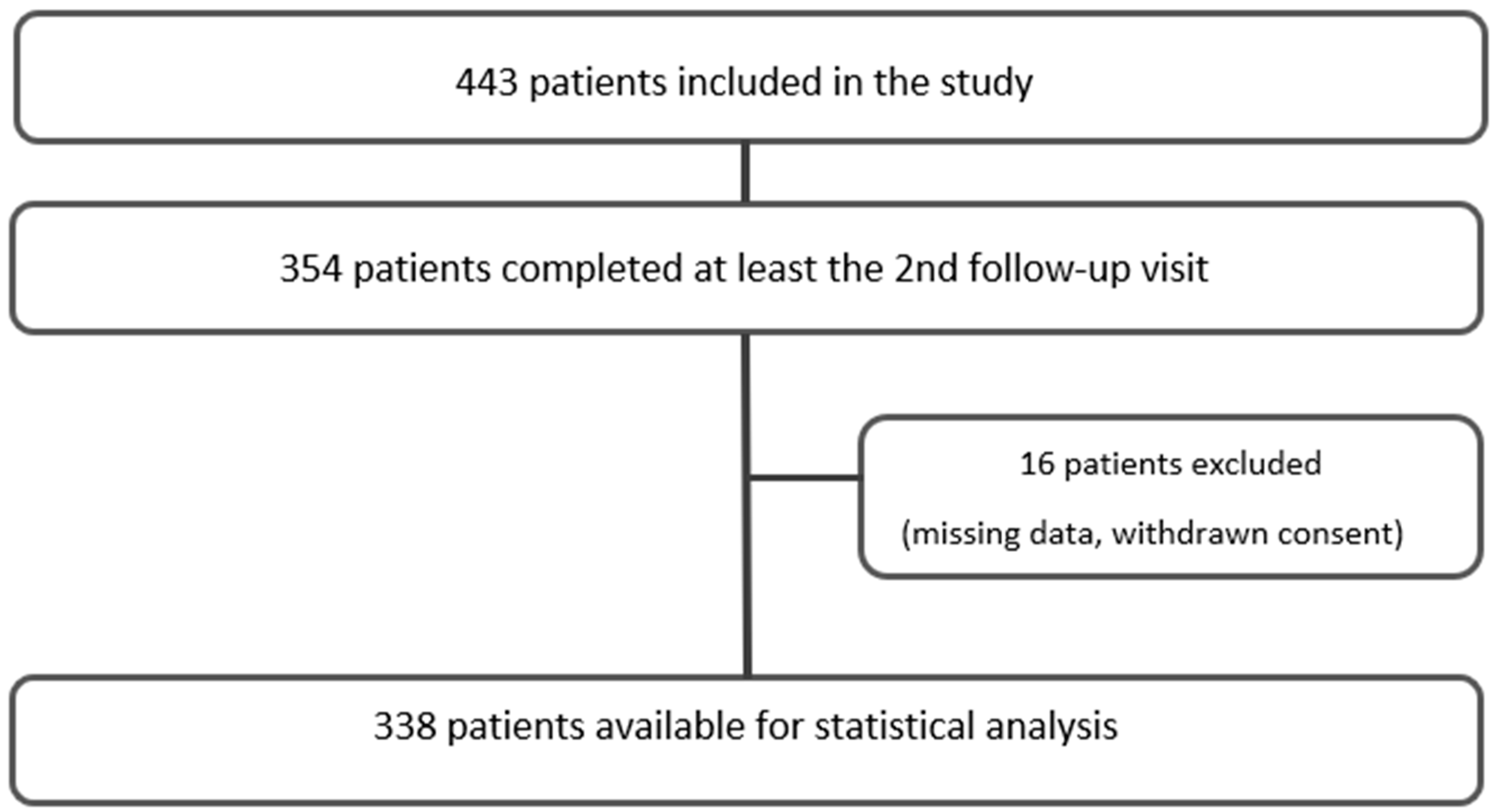
2.1. Study Design
2.2. Ultrasound Imaging, Routine Laboratory, and Additional Examination
2.3. Statistical Analysis
2.4. Ethical Issues
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Wu, W.-K.; Melnichenko, A.A.; Wetzker, R.; Sukhorukov, V.; Markin, A.M.; Khotina, V.A.; Orekhov, A.N. Signaling Pathways and Key Genes Involved in Regulation of foam Cell Formation in Atherosclerosis. Cells 2020, 9, 584. [Google Scholar] [CrossRef] [PubMed]
- Kouhpeikar, H.; Delbari, Z.; Sathyapalan, T.; Simental-Mendía, L.E.; Jamialahmadi, T.; Sahebkar, A. The Effect of Statins through Mast Cells in the Pathophysiology of Atherosclerosis: A Review. Curr. Atheroscler. Rep. 2020, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, C.; Delgado, P.; Busse, C.E.; Sanz-Bravo, A.; Martos-Folgado, I.; Bonzon-Kulichenko, E.; Ferrarini, A.; Gonzalez-Valdes, I.B.; Mur, S.M.; Roldán-Montero, R.; et al. ALDH4A1 is an atherosclerosis auto-antigen targeted by protective antibodies. Nature 2021, 589, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Beverly, J.K.; Budoff, M.J. Atherosclerosis: Pathophysiology of insulin resistance, hyperglycemia, hyperlipidemia, and inflammation. J. Diabetes 2020, 12, 102–104. [Google Scholar] [CrossRef]
- Marschang, P.; Friedrich, G.J.; Ditlbacher, H.; Stoeger, A.; Nedden, D.Z.; Kirchmair, R.; Dienstl, A.; Pachinger, O.; Patsch, J.R. Reduction of soluble P-selectin by statins is inversely correlated with the progression of coronary artery disease. Int. J. Cardiol. 2006, 106, 183–190. [Google Scholar] [CrossRef]
- Hoefer, I.E.; Steffens, S.; Ala-Korpela, M.; Bäck, M.; Badimon, L.; Bochaton-Piallat, M.-L.; Boulanger, C.M.; Caligiuri, G.; Dimmeler, S.; Egido, J.; et al. Novel methodologies for biomarker discovery in atherosclerosis. Eur. Heart J. 2015, 36, 2635–2642. [Google Scholar] [CrossRef]
- Ferri, N.; Paoletti, R.; Corsini, A. Biomarkers for atherosclerosis: Pathophysiological role and pharmacological modulation. Curr. Opin. Infect. Dis. 2006, 17, 495–501. [Google Scholar] [CrossRef]
- Sakurai, S.; Kitamura, A.; Cui, R.; Yamagishi, K.; Tanigawa, T.; Iso, H. Relationships of Soluble E-Selectin and High-Sensitivity C-Reactive Protein with Carotid Atherosclerosis in Japanese Men. J. Atheroscler. Thromb. 2009, 16, 339–345. [Google Scholar] [CrossRef]
- Hobbs, F.; Piepoli, M.; Hoes, A.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.; Cooney, M.; Corra, U.; Cosyns, B.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Purdy, M.; Obi, A.; Myers, D.; Wakefield, T. P- and E-selectin in venous thrombosis and non-venous pathologies. J. Thromb. Haemost. 2022, 20, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Hisada, Y.; Mackman, N. Cancer-associated pathways and biomarkers of venous thrombosis. Blood 2017, 130, 1499–1506. [Google Scholar] [CrossRef]
- Agrati, C.; Sacchi, A.; Tartaglia, E.; Vergori, A.; Gagliardini, R.; Scarabello, A.; Bibas, M. The Role of P-Selectin in COVID-19 Coagulopathy: An Updated Review. Int. J. Mol. Sci. 2021, 22, 7942. [Google Scholar] [CrossRef]
- Johnson, R.C.; Chapman, S.M.; Dong, Z.M.; Ordovas, J.M.; Mayadas, T.N.; Herz, J.; Hynes, R.O.; Schaefer, E.J.; Wagner, D.D. Absence of P-selectin delays fatty streak formation in mice. J. Clin. Investig. 1997, 99, 1037–1043. [Google Scholar] [CrossRef]
- Tardif, J.-C.; Tanguay, J.-F.; Wright, S.R.; Duchatelle, V.; Petroni, T.; Grégoire, J.C.; Ibrahim, R.; Heinonen, T.M.; Robb, S.; Bertrand, O.F.; et al. Effects of the P-Selectin Antagonist Inclacumab on Myocardial Damage After Percutaneous Coronary Intervention for Non–ST-Segment Elevation Myocardial Infarction:: Results of the SELECT-ACS trial. J. Am. Coll. Cardiol. 2013, 61, 2048–2055. [Google Scholar] [CrossRef]
- Johnson-Tidey, R.R.; McGregor, J.L.; Taylor, P.R.; Poston, R.N. Increase in the adhesion molecule P-selectin in endothelium overlying atherosclerotic plaques. Coexpression with intercellular adhesion molecule-1. Am. J. Pathol. 1994, 144, 952–961. [Google Scholar]
- Ridker, P.M.; Buring, J.E.; Rifai, N. Soluble P-selectin and the risk of future cardiovascular events. Circulation 2001, 103, 491–495. [Google Scholar] [CrossRef]
- Wang, T.; Sun, C.; Hu, L.; Gao, E.; Li, C.; Wang, H.; Sun, D. Sirt6 stabilizes atherosclerosis plaques by promoting macrophage autophagy and reducing contact with endothelial cells. Biochem. Cell Biol. 2020, 98, 120–129. [Google Scholar] [CrossRef]
- Carnevale, R.; Sciarretta, S.; Valenti, V.; di Nonno, F.; Calvieri, C.; Nocella, C.; Frati, G.; Forte, M.; D’amati, G.; Pignataro, M.G.; et al. Low-grade endotoxaemia enhances artery thrombus growth via Toll-like receptor 4: Implication for myocardial infarction. Eur. Heart J. 2020, 41, 3156–3165. [Google Scholar] [CrossRef]
- Lorenz, M.W.; von Kegler, S.; Steinmetz, H.; Markus, H.S.; Sitzer, M. Carotid Intima-Media Thickening Indicates a Higher Vascular Risk Across a Wide Age Range: Prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke 2006, 37, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Polak, J.F.; Pencina, M.J.; Pencina, K.M.; O’Donnell, C.J.; Wolf, P.A.; D’Agostino, R.B., Sr. Carotid-Wall Intima–Media Thickness and Cardiovascular Events. N. Engl. J. Med. 2011, 365, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Morioka, T.; Mori, K.; Emoto, M. Is Stiffness Parameter β Useful for the Evaluation of Atherosclerosis?~ Its Clinical Implications, Limitations, and Future Perspectives. J. Atheroscler. Thromb. 2021, 28, 435–453. [Google Scholar] [CrossRef]
- Willeit, P.; Tschiderer, L.; Allara, E.; Reuber, K.; Seekircher, L.; Gao, L.U.; Liao, X.; Lonn, E.; Gerstein, H.C.; Yusuf, S.; et al. Carotid intima-media thickness progression as surrogate marker for cardiovascular risk: Meta-analysis of 119 clinical trials involving 100,667 patients. Circulation 2021, 142, 621–642. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Carotid plaque, compared with carotid intima-media thickness, more accurately predicts coronary artery disease events: A meta-analysis. Atherosclerosis 2012, 220, 128–133. [Google Scholar] [CrossRef]
- Sillesen, H.; Muntendam, P.; Adourian, A.; Entrekin, R.; Garcia, M.; Falk, E.; Fuster, V. Carotid Plaque Burden as a Measure of Subclinical Atherosclerosis: Comparison with Other Tests for Subclinical Arterial Disease in the High Risk Plaque BioImage Study. JACC Cardiovasc. Imaging 2012, 5, 681–689. [Google Scholar] [CrossRef]
- Schreinlechner, M.; Noflatscher, M.; Lener, D.; Bauer, A.; Kirchmair, R.; Marschang, P.; Theurl, M. NGAL Correlates with Femoral and Carotid Plaque Volume Assessed by Sonographic 3D Plaque Volumetry. J. Clin. Med. 2020, 9, 2811. [Google Scholar] [CrossRef]
- Sommer, P.; Schreinlechner, M.; Noflatscher, M.; Lener, D.; Mair, F.; Theurl, M.; Kirchmair, R.; Marschang, P. High baseline fetuin-A levels are associated with lower atherosclerotic plaque progression as measured by 3D ultrasound. Atheroscler. Plus 2021, 45, 10–17. [Google Scholar] [CrossRef]
- Noflatscher, M.; Schreinlechner, M.; Sommer, P.; Kerschbaum, J.; Berggren, K.; Theurl, M.; Kirchmair, R.; Marschang, P. Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound. J. Clin. Med. 2018, 8, 32. [Google Scholar] [CrossRef]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011) An Update on Behalf of the Advisory Board of the 3rd, 4th and 5th Watching the Risk Symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [PubMed]
- Tscharre, M.; Farhan, S.; Bruno, V.; Rohla, M.; Egger, F.; Weiss, T.W.; Hübl, W.; Willheim, M.; Wojta, J.; Geppert, A.; et al. Impact of platelet turnover on long-term adverse cardiovascular outcomes in patients undergoing percutaneous coronary intervention. Eur. J. Clin. Investig. 2019, 49, e13157. [Google Scholar] [CrossRef]
- Berg, D.D.; Yeh, R.W.; Mauri, L.; Morrow, D.A.; Kereiakes, D.J.; Cutlip, D.E.; Gao, Q.; Jarolim, P.; Michelson, A.D.; Frelinger, A.L.; et al. Biomarkers of platelet activation and cardiovascular risk in the DAPT trial. J. Thromb. Thrombolysis 2021, 51, 675–681. [Google Scholar] [CrossRef]
- Shen, L.; Yang, T.; Xia, K.; Yan, Z.; Tan, J.; Li, L.; Qin, Y.; Shi, W. P-selectin (CD62P) and soluble TREM-like transcript-1 (sTLT-1) are associated with coronary artery disease: A case control study. BMC Cardiovasc. Disord. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wassel, C.L.; Berardi, C.; Pankow, J.S.; Larson, N.B.; Decker, P.A.; Hanson, N.Q.; Tsai, M.Y.; Criqui, M.H.; Allison, M.A.; Bielinski, S.J. Soluble P-selectin predicts lower extremity peripheral artery disease incidence and change in the ankle brachial index: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2015, 239, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Hally, K.E.; Parker, O.M.; Brunton-O’Sullivan, M.M.; Harding, S.A.; Larsen, P.D. Linking Neutrophil Extracellular Traps and Platelet Activation: A Composite Biomarker Score for Predicting Outcomes after Acute Myocardial Infarction. Arthritis Res. Ther. 2021, 121, 1637–1649. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration. C-Reactive Protein, Fibrinogen, and Cardiovascular Disease Prediction. N. Engl. J. Med. 2012, 367, 1310–1320. [Google Scholar] [CrossRef]
- Lee, M.; Lee, K.; Kim, D.-W.; Cho, J.S.; Kim, T.-S.; Kwon, J.; Kim, C.J.; Park, C.S.; Kim, H.Y.; Yoo, K.-D.; et al. Relationship of Serial High-Sensitivity C-Reactive Protein Changes to Long-term Clinical Outcomes in Stabilised Patients After Myocardial Infarction. Can. J. Cardiol. 2021, 38, 92–101. [Google Scholar] [CrossRef]
- Ibanez, B.; Fernández-Ortiz, A.; Fernández-Friera, L.; García-Lunar, I.; Andrés, V.; Fuster, V. Progression of Early Subclinical Atherosclerosis (PESA) Study: JACC Focus Seminar 7/8. J. Am. Coll. Cardiol. 2021, 78, 156–179. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Population (n = 338) | Low-TPP (n = 256) | High-TPP (n = 82) | p-Value | |
|---|---|---|---|---|
| Age, years | 63.1 (±10.1) | 62.0 (±10.4) | 66.6 (±8.1) | <0.001 |
| Female, n (%) | 144 (42.6) | 122 (47.7) | 22 (26.8) | <0.001 |
| Body mass index, kg/m2 | 25.3 (4.7) | 25.2 (4.4) | 26.2 (4.3) | n.s. |
| Hypertension, n (%) | 218 (64.5) | 154 (60.2) | 64 (78.0) | 0.003 |
| Family history for CVD, n (%) | 78 (23.1) | 61 (23.8) | 17 (20.7) | n.s. |
| Smoking, pack years | 12.3 (±19.6) | 11.4 (±19.06) | 15.2 (±21.8) | n.s. |
| Hyperlipidemia, n (%) | 295 (87.3) | 224 (87.5) | 71 (86.6) | n.s. |
| Diabetes mellitus, n (%) | 47 (13.9) | 36 (14.1) | 11 (13.4) | n.s. |
| hsCRP, mg/dL | 0.17 (0.29) | 0.17 (0.32) | 0.17 (0.27) | n.s. |
| sP-selectin, µg/mL | 40.0 (24) | 41.0 (25.1) | 36.3 (20) | n.s. |
| Total cholesterol, mg/dL | 196.5 (±46.4) | 198 (±48.8) | 189 (±37.5) | n.s. |
| LDL-cholesterol, mg/dL | 115.0 (55.75) | 119 (59.0) | 106 (46.0) | n.s. |
| HDL-cholesterol, mg/dL | 58.0 (26.75) | 58.0 (28.0) | 58.0 (26.0) | n.s. |
| Triglyceride mg/dL | 128.0 (85.0) | 132 (88) | 118 (76) | n.s. |
| eGFR, mL/min/1.73 m2 | 76.6 (±15.5) | 77.59 (±15.9) | 73.53 (±13.9) | n.s. |
| Antiplatelet therapy, n (%) | 157 (46.4) | 118 (46.1) | 39 (47.6) | n.s. |
| Lipid lowering therapy | 192 (56.8) | 144 (56.3) | 48 (58.5) | n.s. |
| Antihypertensive therapy | 195 (57.7) | 139 (54.3) | 56 (68.3) | 0.02 |
| ESC SCORE | 3.0 (3.0) | 2.0 (3.0) | 4.0 (2.5) | <0.001 |
| CAD, n (%) | 106 (31.4) | 82 (32.0) | 24 (29.3) | n.s. |
| CRVD, n (%) | 34 (10.1) | 25 (9.8) | 9 (11.0) | n.s. |
| PAD, n (%) | 28 (8.3) | 20 (7.8) | 8 (9.8) | n.s. |
| Study Population (n = 338) | Low-TPP (n = 256) | High-TPP (n = 82) | p-Value | |
|---|---|---|---|---|
| TPV, mm3 | 296.5 (462.25) | 248 (446.5) | 457.0 (443.5) | <0.001 |
| Carotid plaque volume, mm3 | 86.0 (230.25) | 72.0 (199.75) | 125 (235) | 0.006 |
| Femoral plaque volume, mm3 | 174.0 (282.0) | 135.5 (262) | 218.5 (278) | <0.001 |
| Carotid IMT, mm | 0.72 (0.19) | 0.72 (0.19) | 0.76 (0.23) | 0.003 |
| ABI | 0.91 (0.15) | 0.91 (0.16) | 0.91 (0.15) | n.s. |
| PWV, m/s | 5.9 (2.4) | 5.72 (2.18) | 6.4 (2.5) | 0.004 |
| Plaque Progression in mm3 (95% CI) | p | |
|---|---|---|
| sP-selectin | 46.09 (24.75–67.43) | <0.001 |
| +personal data | 38.64 (19.12–58.17) | <0.001 |
| +CVRF | 30.19 (12.27–48.11) | <0.001 |
| +laboratory parameters | 24.15 (7.64–44.48) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sommer, P.; Schreinlechner, M.; Noflatscher, M.; Lener, D.; Mair, F.; Theurl, M.; Kirchmair, R.; Marschang, P. Increasing Soluble P-Selectin Levels Predict Higher Peripheral Atherosclerotic Plaque Progression. J. Clin. Med. 2023, 12, 6430. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12206430
Sommer P, Schreinlechner M, Noflatscher M, Lener D, Mair F, Theurl M, Kirchmair R, Marschang P. Increasing Soluble P-Selectin Levels Predict Higher Peripheral Atherosclerotic Plaque Progression. Journal of Clinical Medicine. 2023; 12(20):6430. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12206430
Chicago/Turabian StyleSommer, Philip, Michael Schreinlechner, Maria Noflatscher, Daniela Lener, Fabian Mair, Markus Theurl, Rudolf Kirchmair, and Peter Marschang. 2023. "Increasing Soluble P-Selectin Levels Predict Higher Peripheral Atherosclerotic Plaque Progression" Journal of Clinical Medicine 12, no. 20: 6430. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12206430