3. Results
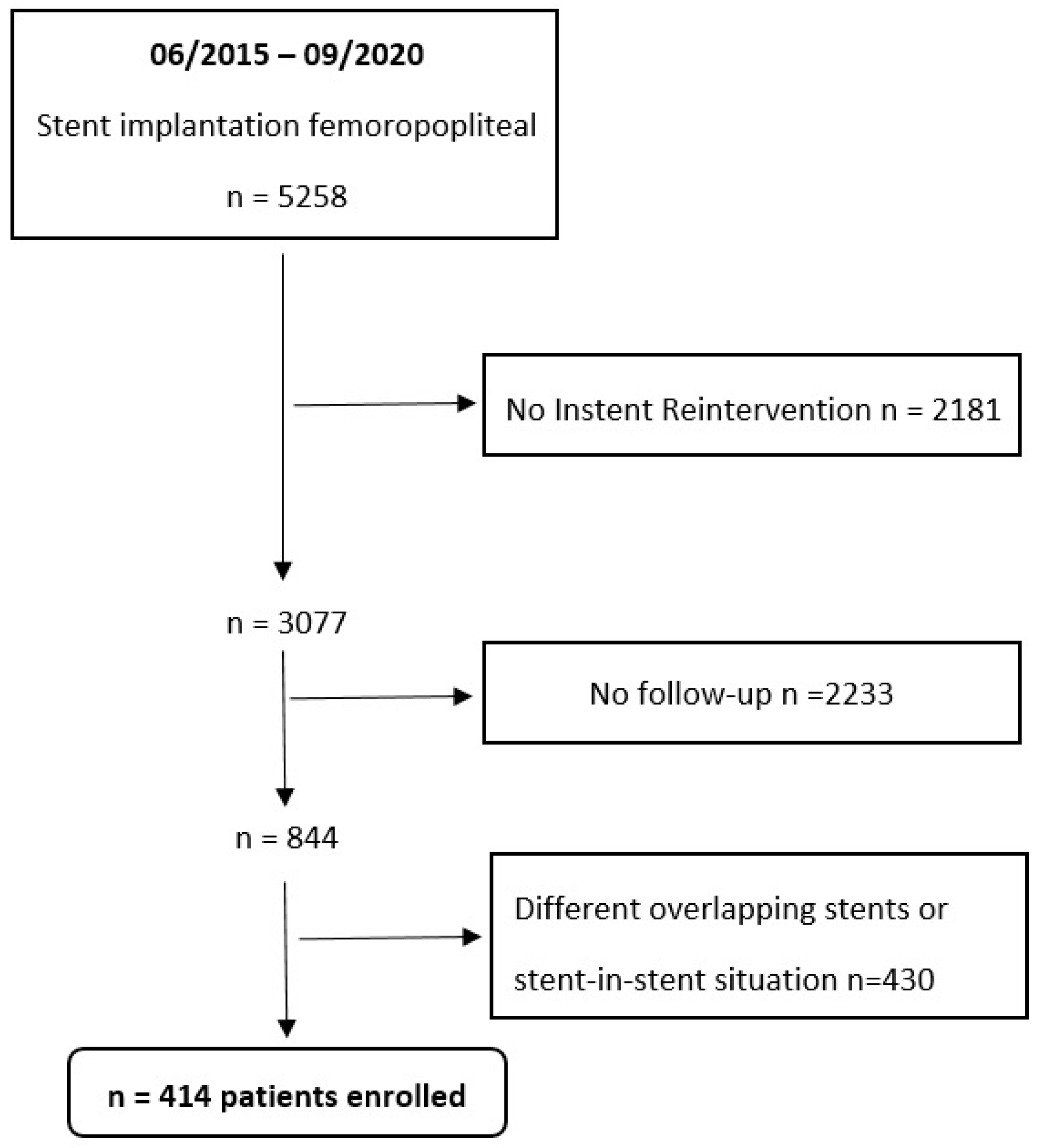
The cohort studied included 414 patients with 236 Supera stents, 67 BioMimics 3D stents, 48 Zilver® PTX® stents, 38 SMART Control stents, and 25 VIABAHN® endoprosthesis lesions.
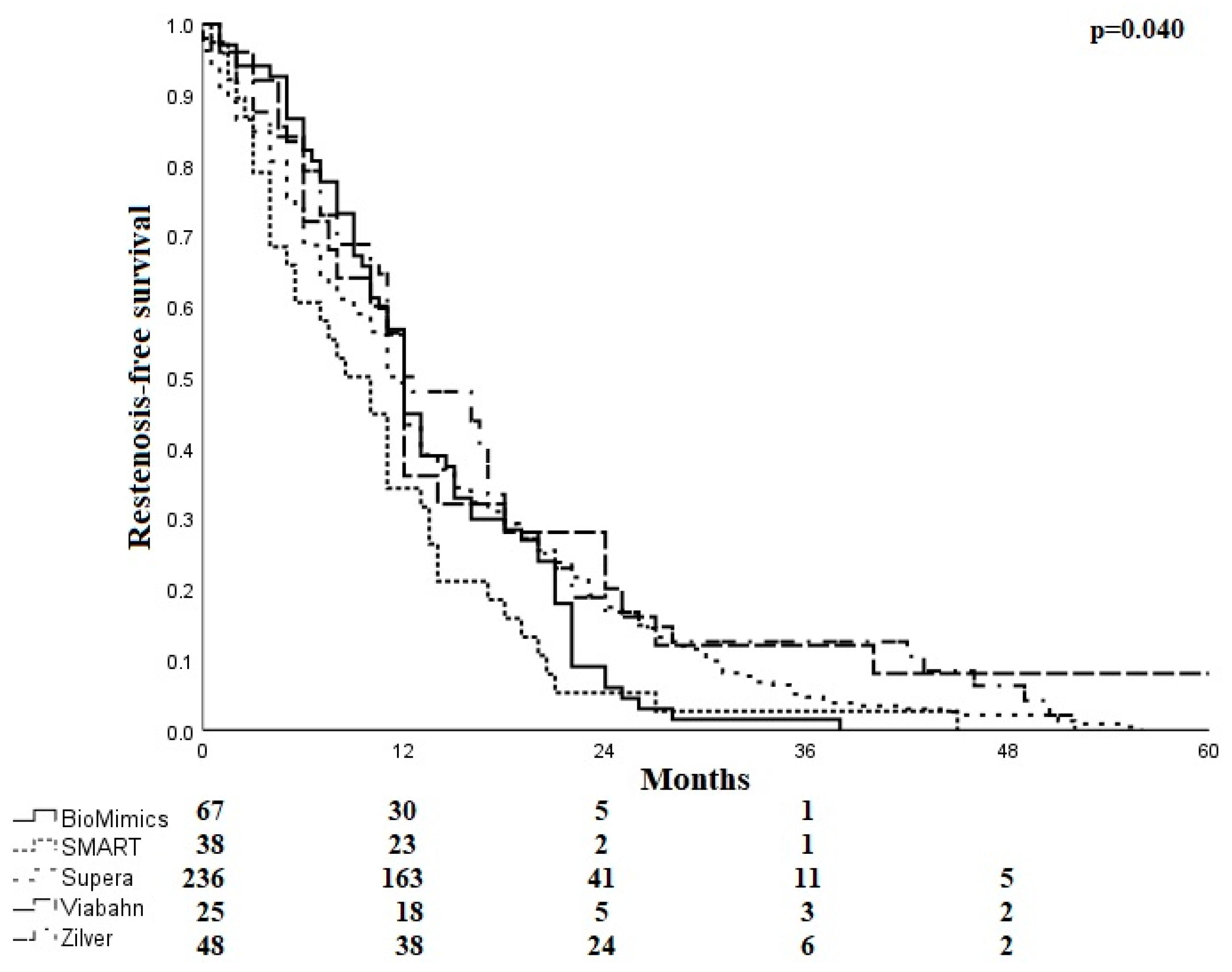
After stent implantation, the mean time to restenosis ranged from 10.5 ± 8.7 months for SMART stents to 18.9 ± 22.4 months for Viabahn endoprostheses. The mean time to restenosis was 13.3 ± 7.6 months for the BioMimics 3D stent, 14.1 ± 11.6 months for the Supera stent, and 16.6 ± 13.5 months for the Zilver PTX stent. Freedom from restenosis is shown in
Figure 3.
The number of ISR occlusions was higher if the index lesion was a CTO, as compared to stenosis (79.4% vs. 43.1%, p < 0.001).
Most ISR lesions presented as occlusions (n = 279, 67.4%) rather than focal (n = 55, 13.3%) or diffuse restenoses (n = 80, 19.3%). The proportion of occlusions ranged from 56.3% in Zilver to 76.0% in Viabahn (p = 0.354). For focal stenoses, the range extended from 9.7% in Supera to 24.0% in Viabahn (p = 0.137). Diffuse stenoses occurred from 10.5% in SMART to 27.1% in the Zilver groups (p = 0.036). Viabahn endoprostheses had either focal stenosis or occlusion but no diffuse stenoses. Edge stenosis was present in approximately 20.0%, ranging from 14.6% in Zilver PTX to 24.0% in the Viabahn groups (p = 0.553).
Regarding lesion extension (
Table 3), the BioMimics 3D performed slightly differently compared with the other stent systems, with fewer patients affected by a lesion in all thirds (76.1% versus 82.1%,
p = 0.163).
In addition, the proportion of patients in which only the proximal third of the stent was affected was 9.0% in the BioMimics stent cohort compared to 5.8% in the other devices (p = 0.230). In one case in the BioMimics 3D stent cohort, the stenosis was localized in the middle (1.5%), and in another case, it was localized in the distal segment (1.5%, 0.683). In comparison, in the other stents, the stenosis was in the middle segment in six cases (1.7%) and in the distal segment in seven cases (2.0%, p = 0.619).
Stents involving the popliteal segment were more frequently affected by occlusions (73.2%) than in patients without knee involvements (60.8%,
p = 0.005) (
Table 4).
The proportion of occlusions was 67.4% across all stent diameters. The percentage of occlusions was the lowest in the 6 to 6.5 mm stent diameter range (62.1%,
p < 0.001) (
Table 4).
Except for Supera, the longer the total stent length, the more frequently occlusions occurred in all systems, and the shorter the stent length, the more frequently stenoses were seen (
Table 4).
Outflow conditions had no significant impact on the proportion of stent occlusions in the entire study cohort; the percentage of occlusions in the overall cohort was 71.5%, with one patent with a below-the-knee vessel, 64.3% with two, and 69.2% with three. However, in the BioMimics 3D and Viabahn cohorts, the proportion of occlusions decreased with the increasing number of open vessels (
Table 4).
The mean Rutherford class at baseline in the cohort with an occlusion was 3.4 ± 0.99 and 3.3 ± 0.89 in the cohort with stenosis. Before reintervention, the mean Rutherford class in the cohort with a stent occlusion was 3.57 ± 0.95, and in the cohort with stenosis, it was 3.23 ± 1.2. Rutherford Becker classes at the time of primary stent implantation and at the time of reintervention are shown in
Table 5.
Multivariate logistic regression analysis identified active smoking, pre-interventional occlusion, and popliteal intervention as risk factors for restenosis or reocclusion (
Table 6).
4. Discussion
In the present study, we compared five self-expanding nitinol stent geometries and designs regarding their restenosis or reocclusion characteristics. In summary, potentially due to the small numbers, no significant differences in the percentage of stent occlusions or ISR lesion location within the stent were found.
Special attention was given to the BioMimics 3D helical centerline system, which is designed to potentially suppress the development of neo-intima-related restenosis by creating increased swirling flow-induced wall shear stress [
5]. Of note, swirling flow inside the BioMimics 3D stent is created 2 to 3 cm distal to the proximal stent edge; the first 2 centimeters of the stent are straight. Therefore, one focus of the analysis was restenosis location within the course of the stent. We expected to find more restenoses in the proximal compared to the mid and distal thirds of the BioMimics 3D stent and a more uniform lesion distribution in the straight stent designs.
The comparison of the restenosis patterns is limited by an uneven distribution of stent location and stent length between the study cohorts. The BioMimics 3D and Supera stents were primarily used in the distal segment of the SFA and the popliteal artery. Compared to more proximal SFA segments, these vessel segments are characterized by more pronounced leg motion, inducing vessel and stent deformation [
10]. The helical design of the BioMimics 3D stent can intercept shortening of the femoropopliteal artery during knee flexion. With straight stents, the compression stress is more localized, increasing the risk of stent fracture [
11].
The interwoven Supera stent is also designed helically and is particularly resistant to compression forces. It is, therefore, also well suited for use in distal femoral or popliteal segments and in calcified lesions [
12].
Regarding the localization of restenosis within the stent, the proportion of stents with all three thirds of the stent affected was highest across all systems. If occlusions were present, all thirds of the stent were almost invariably affected. Across all stents, there were also significantly more occlusions than stenoses. By trend, Zilver PTX (56.3%) and BioMimics 3D (64.2%) presented the lowest occlusion rates compared to Supera (69.1%), SMART (71.1%), Viabahn (76.0%), and the overall cohort (67.4%) (p = 0.354), respectively. A design-specific finding of the Viabahn endoprosthesis was lesion presentation, either as total occlusion or focal edge stenosis, as neo-intima hyperproliferation within the endoprosthesis is only reported anecdotical, explaining the high proportion of extensive lesions with this particular device.
The reduction in neo-intimal hyperplasia by high wall shear stress induced by swirling flow in helical stents might explain why lesions were more focal in the BioMimics 3D stent cohort compared with the other systems. As expected by the design of this particular stent, lesions exclusively located in the proximal third were seen as more frequent by trend as compared to the other stent designs.
In ten healthy pigs, Caro et al. investigated the effect of helical stent geometry compared with straight stent geometry on self-expanding nitinol stents. Digital subtraction angiography demonstrated the presence of swirling flow in the helical stent. A histological examination showed an average 45% reduction in intimal thickness, i.e., significantly reduced neo-intimal hyperplasia in vessels treated with a helical stent compared with those treated with a straight stent. In addition, significantly reduced intimal hyperplasia was observed in the helical stent design due to the altered wall shear stress, especially in the distal region, whereas it was more pronounced proximally and medially. In straight stents, the intimal thickness is distributed inversely [
13]. Shinke et al. also noted swirling flow with decreased intimal hyperplasia, attributing this to increased wall shear stress [
14].
A small randomized controlled trial found a significantly better patency rate of the BioMimics 3D stent compared with the straight control stent after two years, indicating the positive influence of swirling flow and the associated increased wall shear stress in helical stents [
15].
In the present study, the mean time to restenosis was the longest for the Viabahn endoprosthesis, followed by the Zilver PTX stent. Both devices are drug-coated or covered: the Viabahn with PTFE and the Zilver PTX stent with paclitaxel. For the BioMimics, the time to restenosis was shorter but comparable to the Supera stent and longer than after implantation of the SMART stent.
Stent occlusion occurred more frequently if the index lesion prior to stent implantation was an occlusion, as compared to stenosis (79.4% vs. 43.1%, p < 0.001). BioMimics had the lowest occlusion rate if the index lesion was stenosis (17.6%). In multivariate analysis, pre-interventional occlusion was a risk factor for restenosis or reocclusion.
Several studies confirm the link between index lesion occlusion and stent occlusion [
8,
16,
17].
The type of stent patency failure, stenosis vs. occlusion, has significant implications for the treatment success of ISR. Armstrong et al. stratified treatment outcomes after endovascular treatment of femoropopliteal ISR according to Tosaka’s ISR classification. ISR with total occlusion posed a significantly increased risk of recurrence of ISR or occlusion compared with stenotic ISR lesions [
16]. In a small retrospective study, Ihnat et al. showed a similar trend comparing the treatment of nitinol stent ISR with PTA regarding restenosis rate, stratified to ISR occlusion vs. stenosis: 67% of stent occlusions required reintervention during follow-up, whereas none of the nine ISR stenoses experienced recurrent ISR or reocclusion over a 17.8-month period [
17].
The total occlusion rate in the present study (entire cohort—67.4%, BioMimics cohort—64.2%) is twice as high as reported in previous studies dealing with ISR treatment [
8,
16]. The majority of the stents in this study were implanted in the distal femoral and extended into the popliteal segment. Popliteal intervention was a predictor of restenosis and reocclusion in multivariate analyses.
Shibuya et al. investigated the relationship between stent location and occlusion. Particular attention was paid to 15 patients who had occlusions in either the common femoral or popliteal artery belonging to study Group A. Group B included patients with occlusions mostly in the SFA. Group A occlusions were more likely to have more severe symptoms than group B. A bypass was also needed more often. The authors hypothesize that the adverse outcomes were caused by the localization of the stent in flexed areas or vessel segments with collaterals [
18]. Further studies suggest that stents in the popliteal region have an increased risk of developing stent occlusion due to physiologic vessel motion and associated stent deformities, resulting in intermittent low or no flow and an increased risk of stent thrombosis and stent fractures [
19,
20,
21].
The present study showed a clear link between stent length and stent occlusion, with increasing stent length or a chain of stents leading to more occlusions.
In lesions exceeding 200 mm in length, a chain of overlapping stents was implanted, except in some Viabahn cases, which generally worsens the outcome, presumably because decreasing vessel mobility in overlap zones increases the risk of stent fractures [
22]. However, this does not explain the higher occlusion rate of the BioMimics stent in longer lesions compared to the other systems. It is conceivable that the protective effect of swirling flow against neo-intima hyperproliferation decreases over longer distances or is disturbed by the overlap zones of multiple stents. In the BioMimics 3D study, with a mean stented lesion length of 130.8 mm ± 79.2 mm, lesions longer than 150 mm were associated with a significantly lower primary patency rate than shorter lesions [
23]. Hong et al. also found significantly higher primary patency in short stents compared with long stents, with long stents extending into the distal popliteal artery or chains of stents being an independent predictor of restenosis [
24]. In the multivariate analysis, however, stent length was not a risk factor for restenosis or reocclusion.
The impact of the number of outflow vessels on stent occlusion did vary between the groups. In the multivariate analysis, the number of patent leg vessels was not a risk factor for restenosis or reocclusion. In contrast to the remaining devices, in the BioMimics 3D stent cohort, we saw a relationship between the number of patent outflow vessels and stent occlusions: three patent below-the-knee vessels were associated with a proportion of occlusions of 50.0% vs. 65.5% and 75% in the presence of one or two patent outflow vessels, respectively. The potential protective effect of swirling flow preventing ISR development may be reduced by increased peripheral vascular resistance due to impaired outflow conditions. Some former studies confirm the negative impact of outflow vessel obstruction on stent patency.
London et al. and Hong et al. showed that stent patency is influenced by the number of patent outflow vessels [
24,
25]. Davies et al. also found that patients who had poor outflow vessel conditions were more often symptomatic, in addition to presenting a higher rate of restenosis [
26]. However, Sullivan et al. did not confirm our finding; in their study, the number of patent outflow vessels had no statistically significant effect on the primary patency of the BioMimics 3D stent at 24 months [
27,
28].
An interesting, not yet widely discussed, question is whether ISR results in different symptoms as compared to the clinical stage before the intervention, in particular if a Viabahn is implanted, potentially covering collateral vessels. In more than half of the patients in our entire cohort, there was no difference in the Rutherford class before the index stent procedure or prior to the reintervention, with the BioMimics group showing the lowest rate of change in the Rutherford class. Worsening of symptoms occurred in 25.9% of the entire cohort, while it was 20.9% for the BioMimics 3D stent cohort. In the Viabahn group, there was a worsening of the symptoms in 32%. However, critical limb ischemia was no more frequent before reintervention (n = 3) than before Viabahn implantation (n = 4). Unfortunately, these data are not comparable to previous studies, as these studies report clinical symptoms at predefined study intervals and included patients who already underwent a TLR during follow-up. Therefore, clinical outcomes such as ankle–brachial index and Rutherford category do not differ significantly in RCTs, as shown in the BioMimics RCT, where improvement of at least one Rutherford category at 12 and 24 months was seen in 86% and 88% of patients with a BioMimics stent, as compared to 82% and 86% with the control stent, respectively [
15].

 ,
, 



{kind=link}
{kind=link}
{kind=link}