

Introducing Machine Perfusion into Routine Clinical Practice for Liver Transplantation in the United States: The Moment Has Finally Come

{kind=link}
Abstract
:1. Potential Benefits of Machine Perfusion Technologies
2. Why Machine Perfusion Has Been Slower to Be Adopted in USA Than Europe?
3. Current Pressures on Organ Donation and Why They Have Increased the Push for Machine Perfusion in the USA
4. Machine Perfusion Platforms Available Commercially or as Part of a Clinical Trial in the USA
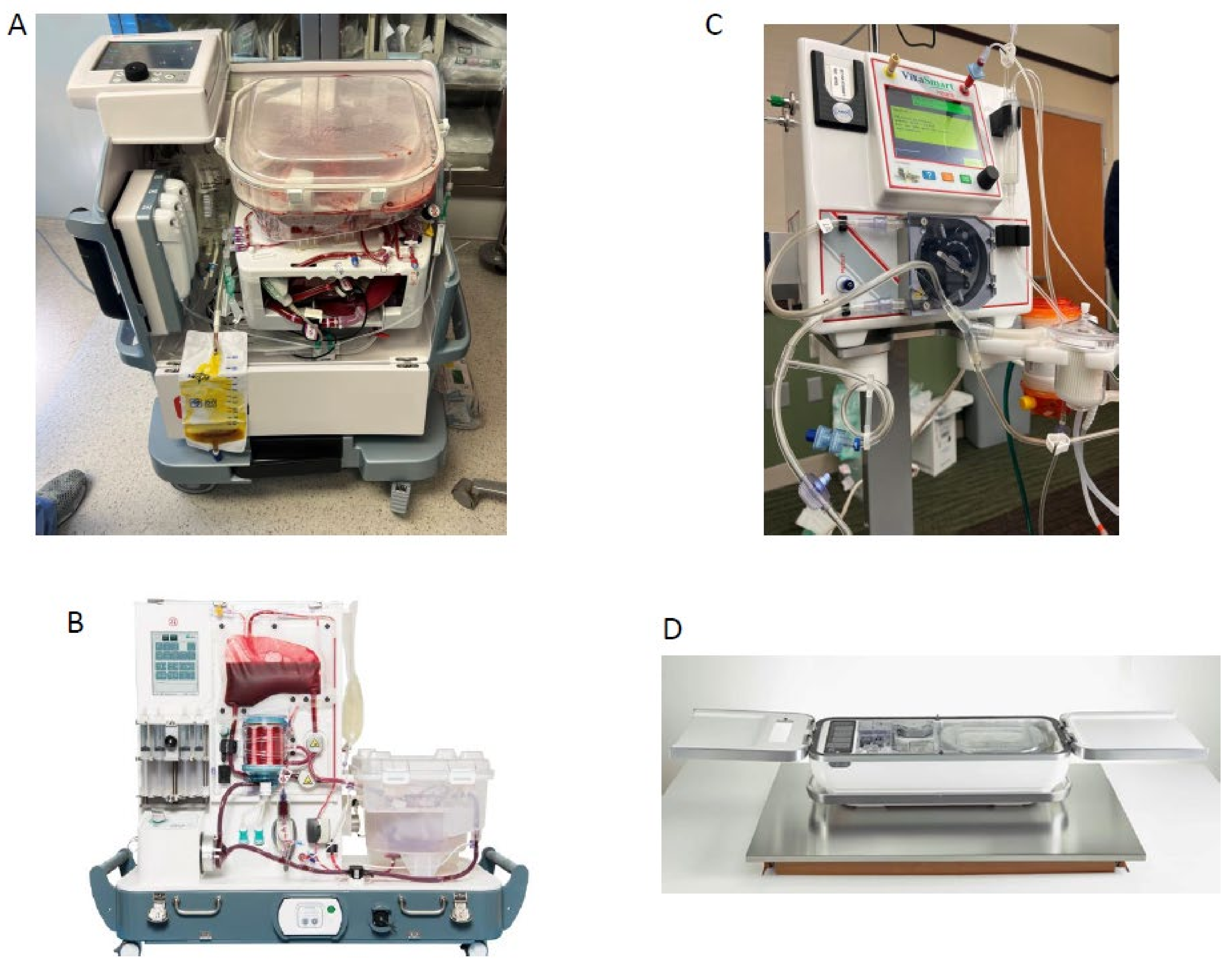
- OCS liver system (TransMedics): NMP, FDA approved.
- OrganOx metra® System: NMP, FDA approved.
- LifePort Liver Transporter (LLT) system: HMP, DHOPE, clinical trial complete with FDA approval pending.
- VitaSmart Liver Machine Perfusion System (Bridge to Life): HMP, HOPE via portal vein alone, clinical trial currently recruiting.

5. Ex situ Normothermic Machine Perfusion in the USA
6. Ex situ Hypothermic Machine Perfusion in the USA
7. Normothermic Regional Perfusion in the USA
- Perfusion of the organs in the body: This is not autoresuscitation or resuscitation of the donor. The donor is dead before the initiation of NRP. NRP is mechanically assisted regional perfusion and oxygenation of organs for transplantation.
- Clamping the brachiocephalic vessels before the initiation of TA-NRP ensures that the brain is not reperfused. Circulatory death has already been determined under the UDDA and in accordance with accepted medical standards when the brachiocephalic vessels are clamped.
- Reperfusing the heart in the body on NRP is no different that restarting the heart outside of the body with machine perfusion. While this is optically different, in both cases, the heart is restarted with artificial machine assistance for the purpose of organ donation in a person who died intending to donate their organs. The heart would not continue to function within the donor without ventilatory support, so it is functioning only with mechanical assistance for the purposes of organ donation.
8. The Future of Machine Perfusion in the USA
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| CIT | Cold ischemia time |
| CT | Computed tomography |
| DCD | Donation after Circulatory Death |
| DBD | Donation after Brain Death |
| D-HOPE | Dual dual portal vein and hepatic artery hypothermic oxygenated perfusion |
| DRI | Donor risk index |
| HCC | Hepatocellular carcinoma |
| HMP | Hypothermic Machine Perfusion |
| KDPI | Kidney donor profile index |
| LT | Liver transplant |
| MELD | Model for end stage liver disease |
| NMP | Normothermic Machine Perfusion |
| NRP | Normothermic Regional Perfusion |
| OCS | Organ Care System |
| OPO | Organ procurement Organization |
| OPTN | Organ Procurement Transplant Network |
| RCT | Randomized Control Trial |
| SD | Standard deviation |
| STAR | Standard Analysis and Research |
| TA-NRP | Thoraco-abdominal Machine Perfusion |
| UNOS | United Network for Organ Sharing |
References
- Kwong, A.J.; Ebel, N.H.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Foutz, J.; Gauntt, K.; Cafarella, M.; et al. OPTN/SRTR 2020 Annual Data Report: Liver. Am. J. Transplant. 2022, 22 (Suppl. S2), 204–309. [Google Scholar] [CrossRef] [PubMed]
- MacConmara, M.; Hanish, S.I.; Hwang, C.S.; De Gregorio, L.; Desai, D.M.; Feizpour, C.A.; Tanriover, B.; Markmann, J.F.; Zeh H 3rd Vagefi, P.A. Making Every Liver Count: Increased Transplant Yield of Donor Livers through Normothermic Machine Perfusion. Ann. Surg. 2020, 272, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Markmann, J.F.; Vagefi, P.A.; MacConmara, M.P. Normothermic Machine Perfusion Increases Donor Liver Use. JAMA Surg. 2022, 157, 742–743. [Google Scholar] [CrossRef] [PubMed]
- Oniscu, G.C.; Mehew, J.; Butler, A.J.; Sutherland, A.; Gaurav, R.; Hogg, R.; Currie, I.; Jones, M.; Watson, C.J.E. Improved Organ Utilization and Better Transplant Outcomes with In Situ Normothermic Regional Perfusion in Controlled Donation After Circulatory Death. Transplantation 2022. Epub ahead of printing. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.; Brockmann, J.G.; Coussios, C.; Friend, P.J. The role of normothermic extracorporeal perfusion in minimizing ischemia reperfusion injury. Transplant. Rev. 2012, 26, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Ravikumar, R.; Jassem, W.; Mergental, H.; Heaton, N.; Mira, D.; Perera, M.T.P.R.; Quaglia, A.; Holroyd, D.; Vogel, T.; Coussios, C.C.; et al. Liver transplantation after ex vivo normothermic machine preservation: A phase 1 (first-in-man) clinical trial. Am. J. Transplant. 2016, 16, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; García-Valdecasas, J.C.; Heaton, N.; et al. A randomized trial of normothermic preservation in liver transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef]
- Schlegel, A.; Muller, X.; Kalisvaart, M.; Muellhaupt, B.; Perera, M.T.P.; Isaac, J.R.; Clavien, P.-A.; Muiesan, P.; Dutkowski, P. Outcomes of liver transplantations from donation after circulatory death (DCD) treated by hypothermic oxygenated perfusion (HOPE) before implantation. J. Hepatol. 2019, 2, 50–57. [Google Scholar] [CrossRef]
- Van Rijn, R.; Schurink, I.J.; de Vries, Y.; van den Berg, A.P.; Cortes Cerisuelo, M.; Darwish Murad, S.; Erdmann, J.I.; Gilbo, N.; de Haas, R.J.; Heaton, N.; et al. DHOPE-DCD Trial Investigators. Hypothermic Machine Perfusion in Liver Transplantation—A Randomized Trial. N. Engl. J. Med. 2021, 384, 1391–1401. [Google Scholar] [CrossRef]
- Hessheimer, A.J.; de la Rosa, G.; Gastaca, M.; Ruíz, P.; Otero, A.; Gómez, M.; Alconchel, F.; Ramírez, P.; Bosca, A.; López-Andújar, R.; et al. Abdominal normothermic regional perfusion in controlled donation after circulatory determination of death liver transplantation: Outcomes and risk factors for graft loss. Am. J. Transplant. 2022, 22, 1169–1181. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Available online: https://www.fda.gov/medical-devices/recently-approved-devices/organ-care-system-ocs-liver-p200031 (accessed on 23 October 2022).
- Hwang, T.J.; Sokolov, E.; Franklin, J.M.; Kesselheim, A.S. Comparison of rates of safety issues and reporting of trial outcomes for medical devices approved in the European Union and United States: Cohort study. BMJ 2016, 353, i3323. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, J.R.; Highet, A.; Hobeika, M.J.; Englesbe, M.J.; McElroy, L.M. Going the distance for procurement of donation after circulatory death livers for transplantation-Does reimbursement reflect reality? Clin. Transplant. 2020, 34, e13780. [Google Scholar] [CrossRef]
- Cardini, B.; Oberhuber, R.; Fodor, M.; Hautz, T.; Margreiter, C.; Resch, T.; Scheidl, S.; Maglione, M.; Bösmüller, C.; Mair, H.; et al. Clinical Implementation of Prolonged Liver Preservation and Monitoring through Normothermic Machine Perfusion in Liver Transplantation. Transplantation 2020, 104, 1917–1928. [Google Scholar] [CrossRef]
- Brüggenwirth, I.M.; Mueller, M.; Lantinga, V.A.; Camagni, S.; De Carlis, R.; De Carlis, L.; Colledan, M.; Dondossola, D.; Drefs, M.; Eden, J.; et al. Prolonged preservation by hypothermic machine perfusion facilitates logistics in liver transplantation: A European observational cohort study. Am. J. Transplant. 2022, 22, 1842–1851. [Google Scholar] [CrossRef]
- Pavicevic, S.; Uluk, D.; Reichelt, S.; Fikatas, P.; Globke, B.; Raschzok, N.; Schmelzle, M.; Öllinger, R.; Schöning, W.; Eurich, D.; et al. Hypothermic oxygenated machine perfusion for extended criteria donor allografts: Preliminary experience with extended organ preservation times in the setting of organ reallocation. Artif. Organs. 2022, 46, 306–311. [Google Scholar] [CrossRef]
- Boteon, A.P.C.S.; Schlegel, A.; Carvalho, M.F.; Boteon, Y.L. Hypothermic oxygenated machine perfusion as a tool to facilitate liver transplantation in the acute-on-chronic liver failure scenario. Liver Transpl. 2022, 28, 1678–1680. [Google Scholar] [CrossRef] [PubMed]
- Executive Order 13879—Advancing American Kidney Health. Available online: https://www.govinfo.gov/content/pkg/DCPD-201900464/pdf/DCPD-201900464.pdf (accessed on 23 October 2022).
- Medicare and Medicaid Programs. Organ Procurement Organizations Conditions for Coverage: Revisions to the Outcome Measure Requirements for Organ Procurement Organizations. Available online: https://www.federalregister.gov/documents/2020/12/02/2020-26329/medicare-and-medicaid-programs-organ-procurement-organizations-conditions-for-coverage-revisions-to (accessed on 23 October 2022).
- New National Liver and Intestinal Organ Transplant System in Effect 4 February 2020. Available online: https://unos.org/policy/liver-distribution/ (accessed on 23 October 2022).
- Wey, A.; Noreen, S.; Gentry, S.; Cafarella, M.; Trotter, J.; Salkowski, N.; Segev, D.; Israni, A.; Kasiske, B.; Hirose, R.; et al. The Effect of Acuity Circles on Deceased Donor Transplant and Offer Rates Across Model for End-Stage Liver Disease Scores and Exception Statuses. Liver Transpl. 2022, 28, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.H.; Chyou, D.; Goldberg, D.S. Impact of major hepatocellular carcinoma policy changes on liver transplantation for hepatocellular carcinoma in the United States. Liver Transpl. 2022. Epub ahead of printing. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Muller, X.; Dutkowski, P. Hypothermic Machine Preservation of the Liver: State of the Art. Curr. Transpl. Rep. 2018, 5, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical Trials.gov. OCS Liver PROTECT Trial: Preserving and Assessing Donor Livers for Transplantation (PROTECT). Available online: https://clinicaltrials.gov/ct2/show/NCT02522871?term=NCT02522871&draw=2&rank=1 (accessed on 23 October 2022).
- Markmann, J.F.; Abouljoud, M.S.; Ghobrial, R.M.; Bhati, C.S.; Pelletier, S.J.; Lu, A.D.; Ottmann, S.; Klair, T.; Eymard, C.; Roll, G.R.; et al. Impact of Portable Normothermic Blood-Based Machine Perfusion on Outcomes of Liver Transplant: The OCS Liver PROTECT Randomized Clinical Trial. JAMA Surg. 2022, 157, 189–198. [Google Scholar] [CrossRef]
- Clinical Trials.gov. A Multicenter Randomized Controlled Trial to Compare the Efficacy of Ex-Vivo Normothermic Machine Profusion with Static Cold Storage in Human Liver Transplantation. Available online: https://clinicaltrials.gov/ct2/show/NCT02775162 (accessed on 23 October 2022).
- OrganOx FDA Approval. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf20/P200035B.pdf (accessed on 2 December 2022).
- Clinical Trials.gov. Pilot Study to Assess Safety and Feasibility of Normothermic Machine Preservation in Human Liver Transplantation. Available online: https://clinicaltrials.gov/ct2/show/NCT02515708?term=nct02515708&draw=2&rank=1 (accessed on 23 October 2022).
- Quintini, C.; Del Prete, L.; Simioni, A.; Del Angel, L.; Diago Uso, T.; D’Amico, G.; Hashimoto, K.; Aucejo, F.; Fujiki, M.; Eghtesad, B.; et al. Transplantation of declined livers after normothermic perfusion. Surgery 2022, 171, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Croome, K.P.; Mao, S.; Taner, C.B. The Current Landscape of Liver Transplantation After Ex Situ Machine Perfusion and Normothermic Regional Perfusion in the United States. Liver Transpl. 2022, 28, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Guarrera, J.V.; Henry, S.D.; Samstein, B.; Odeh-Ramadan, R.; Kinkhabwala, M.; Goldstein, M.J.; Ratner, L.E.; Renz, J.F.; Lee, H.T.; Brown, R.S., Jr.; et al. Hypothermic machine preservation in human liver transplantation: The first clinical series. Am. J. Transplant. 2010, 10, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials.gov. Hypothermic Machine Preservation-Phase 2 (HMP2). Available online: https://clinicaltrials.gov/ct2/show/NCT01274520 (accessed on 23 October 2022).
- Guarrera, J.V.; Henry, S.D.; Samstein, B.; Reznik, E.; Musat, C.; Lukose, T.I.; Ratner, L.E.; Brown, R.S., Jr.; Kato, T.; Emond, J.C. Hypothermic machine preservation facilitates successful transplantation of “orphan” extended criteria donor livers. Am. J. Transplant. 2015, 15, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials.gov. Study to Evaluate Performance of the Organ Recovery Systems LifePort® Liver Transporter System, a Machine Perfusion System, for Liver Transplant (PILOT™). Available online: https://clinicaltrials.gov/ct2/show/NCT03484455 (accessed on 23 October 2022).
- Clinical Trials.gov. Bridge to HOPE: Hypothermic Oxygenated Perfusion versus Cold Storage Prior to Liver Transplantation. Available online: https://clinicaltrials.gov/ct2/show/NCT05045794 (accessed on 23 October 2022).
- Rojas-Peña, A.; Sall, L.E.; Gravel, M.T.; Cooley, E.G.; Pelletier, S.J.; Bartlett, R.H.; Punch, J.D. Donation after circulatory determination of death: The university of michigan experience with extracorporeal support. Transplantation 2014, 98, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.R.H.; McMaster, W.G.; Rali, A.S.; Rahaman, Z.; Balsara, K.; Absi, T.; Levack, M.; Brinkley, M.; Menachem, J.; Punnoose, L.; et al. Early US experience with cardiac donation after circulatory death (DCD) using normothermic regional perfusion. J. Heart Lung. Transplant. 2021, 10, 1408–1418. [Google Scholar] [CrossRef] [PubMed]
- Sellers, M.T.; Nassar, A.; Alebrahim, M.; Sasaki, K.; Lee, D.D.; Bohorquez, H.; Cannon, R.M.; Selvaggi, G.; Neidlinger, N.; McMaster, W.G.; et al. Early United States experience with liver donation after circulatory determination of death using thoraco-abdominal normothermic regional perfusion: A multi-institutional observational study. Clin. Transplant. 2022, 36, e14659. [Google Scholar] [CrossRef]
- Chadha, R.M.; Croome, K.P.; Aniskevich, S.; Pai, S.L.; Nguyen, J.; Burns, J.; Perry, D.; Taner, C.B. Intraoperative Events in Liver Transplantation Using Donation After Circulatory Death Donors. Liver Transpl. 2019, 25, 1833–1840. [Google Scholar] [CrossRef]
- American College of Physicians. Ethics, Determination of Death, and Organ Transplantation in Normothermic Regional Perfusion (NRP) with Controlled Donation after Circulatory Death (cDCD): American College of Physicians Statement of Concern. Available online: https://www.acponline.org/acp_policy/policies/ethics_determination_of_death_and_organ_transplantation_in_nrp_2021.pdf (accessed on 16 May 2022).
- Parent, B.; Caplan, A.; Moazami, N.; Montgomery, R.A. Response to American College of Physician’s statement on the ethics of transplant after normothermic regional perfusion. Am. J. Transplant. 2022, 22, 1307–1310. [Google Scholar] [CrossRef]
- Wall, A.E.; Fiedler, A.; Karp, S.; Shah, A.; Testa, G. Applying the ethical framework for donation after circulatory death to thoracic normothermic regional perfusion procedures. Am. J. Transplant. 2022, 22, 1311–1315. [Google Scholar] [CrossRef]
- American Society of Transplant Surgeons Statement Supporting TA-NRP. Available online: https://asts.org/about-asts/position-statements#.YyINW6TMJaQ (accessed on 23 October 2022).
- Croome, K.P.; Barbas, A.S.; Whitson, B.; Zarrinpar, A.; Taner, T.; Lo, D.; Morganti, R. American Society of Transplant Surgeons (ASTS) Recommendations on Best Practices in Donation after Circulatory Death Organ Procurement. Am. J. Transplant. 2022, in press. [Google Scholar]
- Croome, K.P.; Taner, C.B. The Changing Landscapes in DCD Liver Transplantation. Curr. Transplant. Rep. 2020, 7, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Melandro, F.; Basta, G.; Torri, F.; Biancofiore, G.; Del Turco, S.; Orlando, F.; Guarracino, F.; Maremmani, P.; Lazzeri, C.; Peris, A.; et al. Normothermic regional perfusion in liver transplantation from donation after cardiocirculatory death: Technical, biochemical, and regulatory aspects and review of literature. Artif. Organs. 2022, 46, 1727–1740. [Google Scholar] [CrossRef] [PubMed]
- Del Turco, S.; Cappello, V.; Tapeinos, C.; Moscardini, A.; Sabatino, L.; Battaglini, M.; Melandro, F.; Torri, F.; Martinelli, C.; Babboni, S.; et al. Cerium oxide nanoparticles administration during machine perfusion of discarded human livers: A pilot study. Liver Transpl. 2022, 28, 1173–1185. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Croome, K.P. Introducing Machine Perfusion into Routine Clinical Practice for Liver Transplantation in the United States: The Moment Has Finally Come. J. Clin. Med. 2023, 12, 909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12030909
Croome KP. Introducing Machine Perfusion into Routine Clinical Practice for Liver Transplantation in the United States: The Moment Has Finally Come. Journal of Clinical Medicine. 2023; 12(3):909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12030909
Chicago/Turabian StyleCroome, Kristopher P. 2023. "Introducing Machine Perfusion into Routine Clinical Practice for Liver Transplantation in the United States: The Moment Has Finally Come" Journal of Clinical Medicine 12, no. 3: 909. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12030909