

Characterizing and Predicting Post-Acute Sequelae of SARS CoV-2 Infection (PASC) in a Large Academic Medical Center in the US

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Definition of Demographics, Socioeconomic Status, and Other Covariates
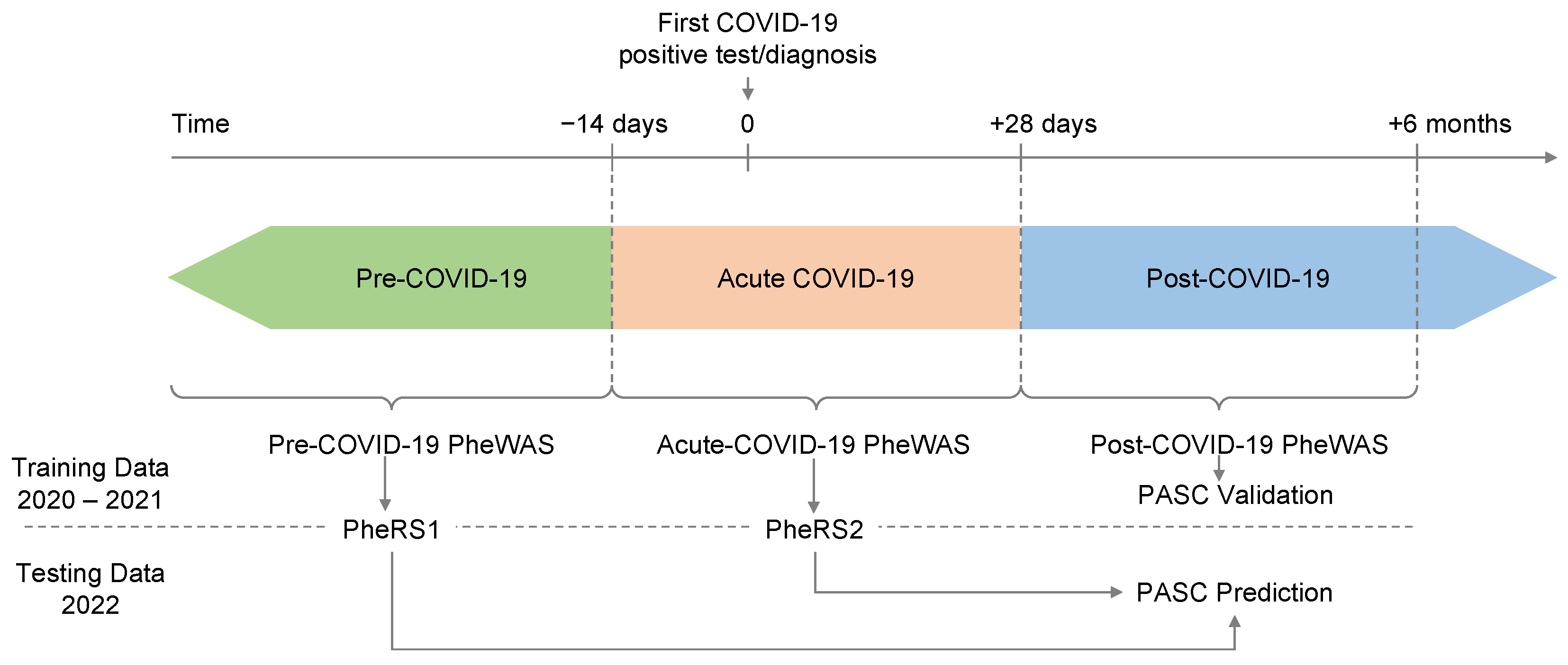
2.3. Time-Restricted Phenomes
2.4. Matching
2.5. Statistical Analysis
2.5.1. PASC-Associated PheCodes in Post COVID-19 Period
2.5.2. Pre-Disposing PheCodes
2.5.3. Phenotype Risk Scores (PheRS)
PheRS Generation
PheRS Evaluation
3. Results
3.1. Patient Characteristics
3.2. PASC Symptoms/Post-COVID-19 PheWAS
3.3. Pre-COVID-19 PheWAS
3.4. Acute-COVID-19 PheWAS
3.5. Comparison of “Pre-PASC” Associated PheCode across Three PheWAS
3.6. Developing Phenotype Risk Scores for Predicting PASC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Neighborhood Disadvantage Index (NDI)
Appendix A.2. Pre- and Post-COVID-19 Years in EHR
Appendix A.3. Vaccination Status
Appendix A.4. COVID-19 Severity
Appendix A.5. Elixhauser comorbidity score
Appendix A.6. Healthcare Worker (HCW) Status
References
- Microsoft Corporation. Bing COVID-19 Tracker. Available online: https://www.bing.com/covid/local/unitedstates (accessed on 13 October 2022).
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Ayuzo Del Valle, N.C.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. Long-COVID in children and adolescents: A systematic review and meta-analyses. Sci. Rep. 2022, 12, 9950. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Post-COVID Conditions: Information for Healthcare Providers. Avaliable online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-index.html (accessed on 15 June 2022).
- Centers for Disease Control and Prevention. Public Health Recommendations. Avaliable online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-public-health-recs.html (accessed on 15 June 2022).
- Centers for Disease Control and Prevention. Long COVID or Post-COVID Conditions. Avaliable online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 15 June 2022).
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Baig, A.M. Chronic COVID syndrome: Need for an appropriate medical terminology for long-COVID and COVID long-haulers. J. Med. Virol. 2021, 93, 2555–2556. [Google Scholar] [CrossRef] [PubMed]
- Nath, A. Long-Haul COVID. Neurology 2020, 95, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Chippa, V.; Aleem, A.; Anjum, F. Post Acute Coronavirus (COVID-19) Syndrome. In StatPearls; StatPearls Publishing; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef]
- Stefanou, M.I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological manifestations of long-COVID syndrome: A narrative review. Ther. Adv. Chronic Dis. 2022, 13, 20406223221076890. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Taquet, M.; Sillett, R.; Zhu, L.; Mendel, J.; Camplisson, I.; Dercon, Q.; Harrison, P.J. Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: An analysis of 2-year retrospective cohort studies including 1,284,437 patients. Lancet Psychiatry 2022, 9, 815–827. [Google Scholar] [CrossRef] [PubMed]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Wang, W.; Wang, C.Y.; Wang, S.I.; Wei, J.C. Long-term cardiovascular outcomes in COVID-19 survivors among non-vaccinated population: A retrospective cohort study from the TriNetX US collaborative networks. EClinicalMedicine 2022, 53, 101619. [Google Scholar] [CrossRef]
- Xu, E.; Xie, Y.; Al-Aly, Z. Long-term neurologic outcomes of COVID-19. Nat. Med. 2022, 28, 2406–2415. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of long covid symptoms after covid-19 vaccination: Community based cohort study. Bmj 2022, 377, e069676. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.M.; Liu, T.C.; Motwani, Y.; Sim, M.S.; Viswanathan, N.; Samras, N.; Hsu, F.; Wenger, N.S. Factors Associated with Post-Acute Sequelae of SARS-CoV-2 (PASC) After Diagnosis of Symptomatic COVID-19 in the Inpatient and Outpatient Setting in a Diverse Cohort. J. Gen. Intern. Med. 2022, 37, 1988–1995. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Cervia, C.; Zurbuchen, Y.; Taeschler, P.; Ballouz, T.; Menges, D.; Hasler, S.; Adamo, S.; Raeber, M.E.; Bächli, E.; Rudiger, A.; et al. Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome. Nat. Commun. 2022, 13, 446. [Google Scholar] [CrossRef]
- Pfaff, E.R.; Girvin, A.T.; Bennett, T.D.; Bhatia, A.; Brooks, I.M.; Deer, R.R.; Dekermanjian, J.P.; Jolley, S.E.; Kahn, M.G.; Kostka, K.; et al. Identifying who has long COVID in the USA: A machine learning approach using N3C data. Lancet Digit Health 2022, 4, e532–e541. [Google Scholar] [CrossRef]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895. [Google Scholar] [CrossRef]
- Salvatore, M.; Beesley, L.J.; Fritsche, L.G.; Hanauer, D.; Shi, X.; Mondul, A.M.; Pearce, C.L.; Mukherjee, B. Phenotype risk scores (PheRS) for pancreatic cancer using time-stamped electronic health record data: Discovery and validation in two large biobanks. J. Biomed. Inform. 2021, 113, 103652. [Google Scholar] [CrossRef]
- Salvatore, M.; Gu, T.; Mack, J.A.; Prabhu Sankar, S.; Patil, S.; Valley, T.S.; Singh, K.; Nallamothu, B.K.; Kheterpal, S.; Lisabeth, L.; et al. A Phenome-Wide Association Study (PheWAS) of COVID-19 Outcomes by Race Using the Electronic Health Records Data in Michigan Medicine. J. Clin. Med. 2021, 10, 1351. [Google Scholar] [CrossRef]
- Estiri, H.; Strasser, Z.H.; Brat, G.A.; Semenov, Y.R.; Patel, C.J.; Murphy, S.N. Evolving phenotypes of non-hospitalized patients that indicate long COVID. BMC Med. 2021, 19, 249. [Google Scholar] [CrossRef]
- National Center for Immunization and Respiratory Diseases (NCIRD); Division of Viral Diseases. Evaluating and Caring for Patients with Post-COVID Conditions: Interim Guidance. Available online: https://stacks.cdc.gov/view/cdc/107148 (accessed on 6 February 2023).
- Clarke, P.; Melendez, R. National Neighborhood Data Archive (NaNDA): Neighborhood Socioeconomic and Demographic Characteristics by Tract, United States, 2000-2010; ICPSR: Ann Arbor, MI, USA, 2019; V1. [Google Scholar] [CrossRef]
- Melendez, R.; Clarke, P.; Khan, A.; Gomez-Lopez, I.; Li, M.; Chenoweth, M. National Neighborhood Data Archive (NaNDA): Socioeconomic Status and Demographic Characteristics of ZIP Code Tabulation Areas, United States, 2008–2017; ICPSR: Ann Arbor, MI, USA, 2020. [Google Scholar]
- Gasparini, A. comorbidity: An R package for computing comorbidity scores. J. Open Source Softw. 2018, 3, 648. [Google Scholar] [CrossRef] [Green Version]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef]
- Wu, P.; Gifford, A.; Meng, X.; Li, X.; Campbell, H.; Varley, T.; Zhao, J.; Carroll, R.; Bastarache, L.; Denny, J.C.; et al. Mapping ICD-10 and ICD-10-CM Codes to Phecodes: Workflow Development and Initial Evaluation. JMIR Med. Inform. 2019, 7, e14325. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.J.; Bastarache, L.; Denny, J.C. R PheWAS: Data analysis and plotting tools for phenome-wide association studies in the R environment. Bioinformatics 2014, 30, 2375–2376. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef]
- Friedman, J.H.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Hoerl, A.E.; Kennard, R.W. Ridge Regression: Biased Estimation for Nonorthogonal Problems. Technometrics 1970, 12, 55–67. [Google Scholar] [CrossRef]
- Jain, R.K. Ridge regression and its application to medical data. Comput. Biomed. Res. 1985, 18, 363–368. [Google Scholar] [CrossRef]
- Mangiafico, S. Rcompanion: Functions to Support Extension Education Program Evaluation. 2021. Available online: https://cran.r-project.org/package=rcompanion (accessed on 15 June 2022).
- Signorell, A. {DescTools}: Tools for Descriptive Statistics. Available online: https://cran.r-project.org/package=DescTools (accessed on 15 June 2022).
- Rodríguez-Álvarez, M.X.; Iácio, V. {ROCnReg}: An {R} Package for Receiver Operating Characteristic Curve Inference with and Without Covariates. BCAM Inst. Rep. Data 2021, 13, 525–555. [Google Scholar] [CrossRef]
- Kosmidis, I. {brglm2}: Bias Reduction in Generalized Linear Models. Available online: https://cran.r-project.org/package=brglm2 (accessed on 15 June 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk factors for post-COVID-19 condition in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur. Respir. J. 2022, 59, 1–11. [Google Scholar] [CrossRef]
- Vodnar, D.C.; Mitrea, L.; Teleky, B.E.; Szabo, K.; Calinoiu, L.F.; Nemes, S.A.; Martau, G.A. Coronavirus Disease (COVID-19) Caused by (SARS-CoV-2) Infections: A Real Challenge for Human Gut Microbiota. Front. Cell Infect. Microbiol. 2020, 10, 575559. [Google Scholar] [CrossRef]
- Chen, J.; Hall, S.; Vitetta, L. Altered gut microbial metabolites could mediate the effects of risk factors in Covid-19. Rev. Med. Virol. 2021, 31, 1–13. [Google Scholar] [CrossRef]
- Chen, J.; Vitetta, L. Gut-brain axis in the neurological comorbidity of COVID-19. Brain Commun. 2021, 3, fcab118. [Google Scholar] [CrossRef]
- Apple, A.C.; Oddi, A.; Peluso, M.J.; Asken, B.M.; Henrich, T.J.; Kelly, J.D.; Pleasure, S.J.; Deeks, S.G.; Allen, I.E.; Martin, J.N.; et al. Risk factors and abnormal cerebrospinal fluid associate with cognitive symptoms after mild COVID-19. Ann. Clin. Transl. Neurol. 2022, 9, 221–226. [Google Scholar] [CrossRef]
- Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuño, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5913. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.R.; Oh, J.Y.; Lee, J.H.; Small, P.M.; Chung, K.F.; Song, W.J. Long-COVID severe refractory cough: Discussion of a case with 6-week longitudinal cough characterization. Asia Pac. Allergy 2022, 12, e19. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Palacios-Ceña, D.; Florencio, L.L.; Guijarro, C.; Martín-Guerrero, J.D. Symptoms Experienced at the Acute Phase of SARS-CoV-2 Infection as Risk Factor of Long-term Post-COVID Symptoms: The LONG-COVID-EXP-CM Multicenter Study. Int. J. Infect. Dis. 2022, 116, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Cabrera Martimbianco, A.L.; Pacheco, R.L.; Bagattini, Â.M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14357. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; á Steig, B.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin. Infect. Dis. 2021, 73, e4058–e4063. [Google Scholar] [CrossRef]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Thabane, L.; Mbuagbaw, L.; Zhang, S.; Samaan, Z.; Marcucci, M.; Ye, C.; Thabane, M.; Giangregorio, L.; Dennis, B.; Kosa, D.; et al. A tutorial on sensitivity analyses in clinical trials: The what, why, when and how. BMC Med. Res. Methodol. 2013, 13, 92. [Google Scholar] [CrossRef]
- Borgonovo, E.; Plischke, E. Sensitivity analysis: A review of recent advances. Eur. J. Oper. Res. 2016, 248, 869–887. [Google Scholar] [CrossRef]
- Bell, M.L.; Catalfamo, C.J.; Farland, L.V.; Ernst, K.C.; Jacobs, E.T.; Klimentidis, Y.C.; Jehn, M.; Pogreba-Brown, K. Post-acute sequelae of COVID-19 in a non-hospitalized cohort: Results from the Arizona CoVHORT. PLoS ONE 2021, 16, e0254347. [Google Scholar] [CrossRef]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 2022, 13, 3528. [Google Scholar] [CrossRef]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef]
- Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: A prospective observational study. Lancet Respir. Med. 2022, 10, 761–775. [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. Bmj 2020, 370, m3026. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. New ICD-10-CM code for Post-COVID Conditions, following the 2019 Novel Coronavirus (COVID-19). Available online: https://www.cdc.gov/nchs/data/icd/announcement-new-icd-code-for-post-covid-condition-april-2022-final.pdf (accessed on 17 January 2023).
- American Academy of Physical Medicine and Rehabilitation. CDC Announces Approval of ICD-10 Code for Post-Acute Sequelae of COVID-19. Available online: https://www.aapmr.org/members-publications/member-news/member-news-details/2021/07/20/cdc-announces-approval-of-icd-10-code-for-post-acute-sequelae-of-covid-19 (accessed on 17 January 2023).
- Brackel, C.L.H.; Lap, C.R.; Buddingh, E.P.; van Houten, M.A.; van der Sande, L.; Langereis, E.J.; Bannier, M.; Pijnenburg, M.W.H.; Hashimoto, S.; Terheggen-Lagro, S.W.J. Pediatric long-COVID: An overlooked phenomenon? Pediatr. Pulmonol. 2021, 56, 2495–2502. [Google Scholar] [CrossRef]
- Parkin, A.; Davison, J.; Tarrant, R.; Ross, D.; Halpin, S.; Simms, A.; Salman, R.; Sivan, M. A Multidisciplinary NHS COVID-19 Service to Manage Post-COVID-19 Syndrome in the Community. J. Prim. Care Community Health 2021, 12, 21501327211010994. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Long COVID Household Pulse Survey. Avaliable online: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm (accessed on 15 July 2019).
- Wang, L.; Foer, D.; MacPhaul, E.; Lo, Y.C.; Bates, D.W.; Zhou, L. PASCLex: A comprehensive post-acute sequelae of COVID-19 (PASC) symptom lexicon derived from electronic health record clinical notes. J. Biomed. Inform. 2022, 125, 103951. [Google Scholar] [CrossRef]
- Tripepi, G.; Jager, K.J.; Dekker, F.W.; Zoccali, C. Selection Bias and Information Bias in Clinical Research. Nephron Clin. Pract. 2010, 115, c94–c99. [Google Scholar] [CrossRef]
- Ma, Q.; Liu, J.; Liu, Q.; Kang, L.; Liu, R.; Jing, W.; Wu, Y.; Liu, M. Global Percentage of Asymptomatic SARS-CoV-2 Infections Among the Tested Population and Individuals With Confirmed COVID-19 Diagnosis: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2137257. [Google Scholar] [CrossRef]
- He, J.; Guo, Y.; Mao, R.; Zhang, J. Proportion of asymptomatic coronavirus disease 2019: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 820–830. [Google Scholar] [CrossRef]
- Xie, Y.; Bowe, B.; Al-Aly, Z. Burdens of post-acute sequelae of COVID-19 by severity of acute infection, demographics and health status. Nat. Commun. 2021, 12, 6571. [Google Scholar] [CrossRef]
- Gluckman, T.J.; Bhave, N.M.; Allen, L.A.; Chung, E.H.; Spatz, E.S.; Ammirati, E.; Baggish, A.L.; Bozkurt, B.; Cornwell, W.K., 3rd; Harmon, K.G.; et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 79, 1717–1756. [Google Scholar] [CrossRef]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A central role for amyloid fibrin microclots in long COVID/PASC: Origins and therapeutic implications. Biochem. J. 2022, 479, 537–559. [Google Scholar] [CrossRef]
- Parker, A.M.; Brigham, E.; Connolly, B.; McPeake, J.; Agranovich, A.V.; Kenes, M.T.; Casey, K.; Reynolds, C.; Schmidt, K.F.R.; Kim, S.Y.; et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: A multidisciplinary model of care. Lancet Respir. Med. 2021, 9, 1328–1341. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Caring for People with Post-COVID Conditions. Avaliable online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/care-post-covid.html (accessed on 15 July 2019).
- Peluso, M.J.; Thomas, I.J.; Munter, S.E.; Deeks, S.G.; Henrich, T.J. Lack of Antinuclear Antibodies in Convalescent Coronavirus Disease 2019 Patients With Persistent Symptoms. Clin. Infect. Dis. 2022, 74, 2083–2084. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Use of COVID-19 Vaccines in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html#primary-series (accessed on 19 March 2022).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 Patients with PASC Diagnosis | COVID-19 Patients without PASC Diagnosis | ||||
|---|---|---|---|---|---|
| Unmatched | p Value * | Matched | p Value * | ||
| n | 1724 | 61951 | 17205 | ||
| Age at index date; mean (SD) | 47.88 (18.85) | 41.67 (22.14) | <0.001 | 47.12 (18.94) | 0.110 |
| Pre-test years in EHR; mean (SD) | 11.70 (7.47) | 10.41 (7.49) | <0.001 | 11.67 (7.37) | 0.870 |
| Post-test years in EHR; mean (SD) | 1.07 (0.56) | 0.93 (0.55) | <0.001 | 1.05 (0.55) | 0.445 |
| Female; n (%) | 1112 (64.5) | 35713 (57.6) | <0.001 | 11089 (64.5) | 0.989 |
| Primary care at MM; n (%) | 1047 (60.7) | 28773 (46.4) | <0.001 | 10435 (60.7) | 0.969 |
| Race/ethnicity; n (%) | 0.151 | 0.990 | |||
| Caucasian/Non-Hispanic | 1273 (73.8) | 44822 (72.4) | 12730 (74.0) | ||
| African American/Non-Hispanic | 199 (11.5) | 7020 (11.3) | 1990 (11.6) | ||
| Other/Non-Hispanic or Hispanic | 175 (10.2) | 6593 (10.6) | 1746 (10.1) | ||
| Other/unknown ethnicity | 77 (4.5) | 3516 (5.7) | 739 (4.3) | ||
| Quarter of year at index date; n (%) | <0.001 | 1.000 | |||
| 2020/1 | 27 (1.6) | 588 (0.9) | 263 (1.5) | ||
| 2020/2 | 57 (3.3) | 1697 (2.7) | 555 (3.2) | ||
| 2020/3 | 64 (3.7) | 2617 (4.2) | 640 (3.7) | ||
| 2020/4 | 273 (15.8) | 13317 (21.5) | 2730 (15.9) | ||
| 2021/1 | 236 (13.7) | 7063 (11.4) | 2360 (13.7) | ||
| 2021/2 | 241 (14.0) | 5475 (8.8) | 2410 (14.0) | ||
| 2021/3 | 168 (9.7) | 4088 (6.6) | 1680 (9.8) | ||
| 2021/4 | 282 (16.4) | 10853 (17.5) | 2820 (16.4) | ||
| 2022/1 | 268 (15.5) | 10887 (17.6) | 2680 (15.6) | ||
| 2022/2 | 100 (5.8) | 5008 (8.1) | 1000 (5.8) | ||
| 2022/3 | 8 (0.5) | 358 (0.6) | 67 (0.4) | ||
| Neighborhood Deprivation Index (%) | 0.003 | 0.350 | |||
| Quartile 1 | 631 (36.6) | 22679 (36.6) | 6629 (38.5) | ||
| Quartile 2 | 401 (23.3) | 13028 (21.0) | 3708 (21.6) | ||
| Quartile 3 | 325 (18.9) | 11330 (18.3) | 3203 (18.6) | ||
| Quartile 4 | 253 (14.7) | 9235 (14.9) | 2444 (14.2) | ||
| Missing | 114 (6.6) | 5679 (9.2) | 1221 (7.1) | ||
| Population density (%) | 0.002 | 0.128 | |||
| Quartile 1 | 413 (24.0) | 15218 (24.6) | 4417 (25.7) | ||
| Quartile 2 | 491 (28.5) | 17796 (28.7) | 5013 (29.1) | ||
| Quartile 3 | 551 (32.0) | 18123 (29.3) | 5229 (30.4) | ||
| Quartile 4 | 155 (9.0) | 5135 (8.3) | 1325 (7.7) | ||
| Missing | 114 (6.6) | 5679 (9.2) | 1221 (7.1) | ||
| Elixhauser Score AHRQ; mean (SD) | 4.52 (12.97) | 3.75 (10.72) | 0.003 | 4.01 (11.36) | 0.077 |
| Predictor | Testing Data | AAUC a (95% CI) | Pseudo-R2 b | Brier Score | |
|---|---|---|---|---|---|
| n Cases | n Controls | ||||
| PheRS1 | 349 | 3248 | 0.548 (0.516, 0.580) | n/a c | n/a c |
| PheRS1 | 123 | 1154 | 0.555 (0.496, 0.612) | 0.0116 | 0.0857 |
| PheRS2 | 0.605 (0.549, 0.663) | 0.0547 | 0.0823 | ||
| PheRS1 and PheRS2 | 0.615 (0.561, 0.670) | 0.0553 | 0.0824 | ||
| PheRS | Upper Risk Bin | %Cases in Risk Bin | %Cases in Lower 50% | OR (95% CI) a | p |
|---|---|---|---|---|---|
| PheRS1 | 25–50% | 10.0 | 7.8 | 1.48 (0.91, 2.42) | 0.12 |
| 10–25% | 12.1 | 1.86 (1.06, 3.25) | 0.029 | ||
| ≥10% | 13.6 | 2.48 (1.24, 4.97) | 0.011 | ||
| ≥25% | 12.7 | 2.10 (1.29, 3.43) | 0.0029 | ||
| PheRS2 | 25–50% | 8.1 | 6.6 | 1.26 (0.76, 2.08) | 0.38 |
| 10–25% | 12.6 | 2.13 (1.25, 3.62) | 0.0053 | ||
| ≥10% | 21.6 | 4.10 (2.28, 7.40) | 2.7 × 10−6 | ||
| ≥25% | 16.5 | 2.92 (1.85, 4.59) | 3.9 × 10−6 | ||
| PheRS1 and PheRS2 | 25–50% | 8.3 | 6.2 | 1.36 (0.82, 2.28) | 0.23 |
| 10–25% | 15.2 | 2.91 (1.73, 4.90) | 5.8 × 10−5 | ||
| ≥10% | 19.4 | 3.94 (2.10, 7.42) | 2.1 × 10−5 | ||
| ≥25% | 17.0 | 3.48 (2.19, 5.55) | 1.5 × 10−7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fritsche, L.G.; Jin, W.; Admon, A.J.; Mukherjee, B. Characterizing and Predicting Post-Acute Sequelae of SARS CoV-2 Infection (PASC) in a Large Academic Medical Center in the US. J. Clin. Med. 2023, 12, 1328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041328
Fritsche LG, Jin W, Admon AJ, Mukherjee B. Characterizing and Predicting Post-Acute Sequelae of SARS CoV-2 Infection (PASC) in a Large Academic Medical Center in the US. Journal of Clinical Medicine. 2023; 12(4):1328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041328
Chicago/Turabian StyleFritsche, Lars G., Weijia Jin, Andrew J. Admon, and Bhramar Mukherjee. 2023. "Characterizing and Predicting Post-Acute Sequelae of SARS CoV-2 Infection (PASC) in a Large Academic Medical Center in the US" Journal of Clinical Medicine 12, no. 4: 1328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041328