
TIcagrelor in Rotational Atherectomy to Reduce TROPonin Enhancement: The TIRATROP Study, A Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Antithrombotic Therapy Management and Procedural Technique
2.3. High Sensitivity Troponin
2.4. End Points
2.5. Statistical Analysis
3. Results
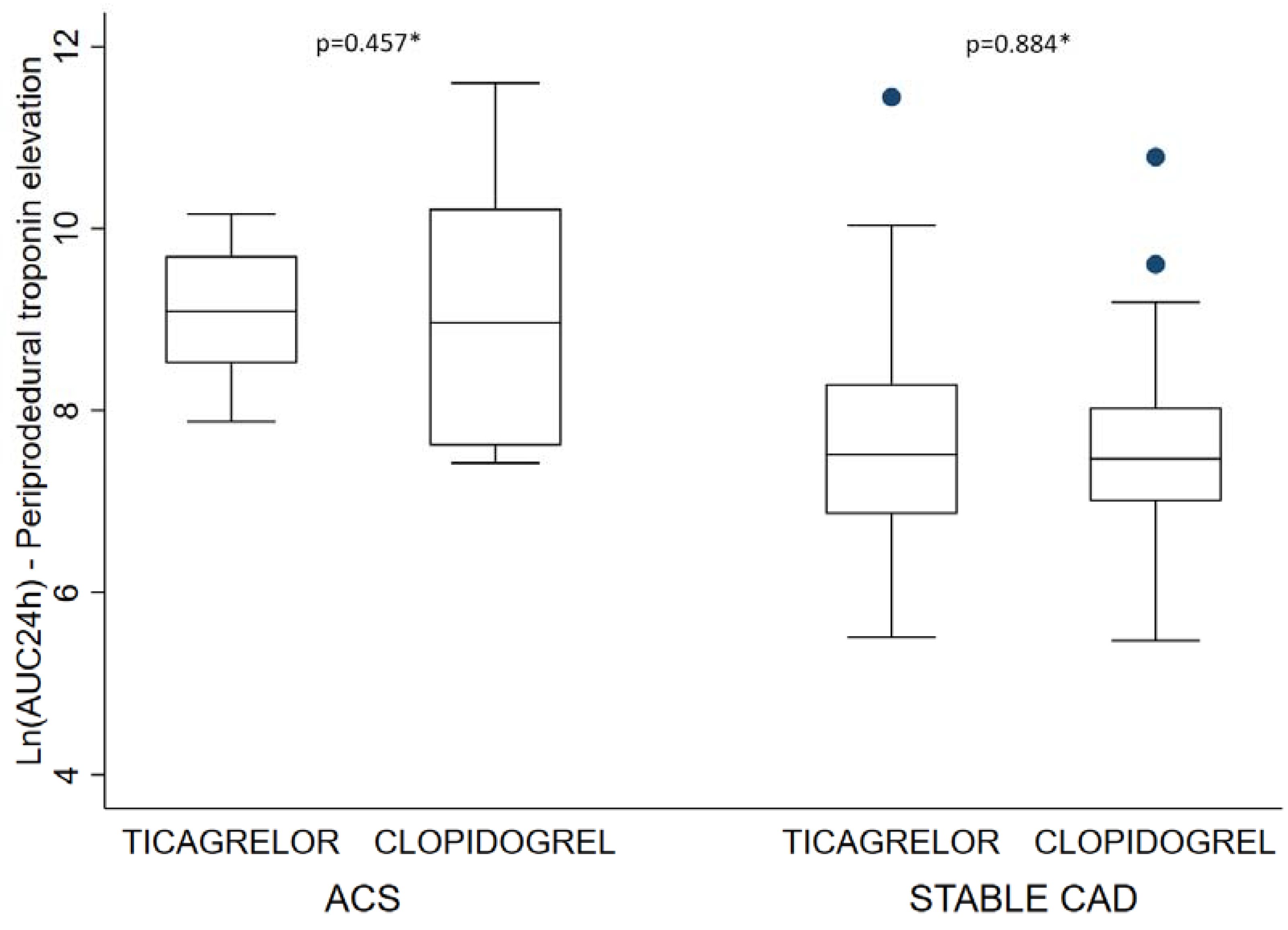
3.1. Periprocedural Troponin Release
3.2. Periprocedural and In-Hospital Complications
4. Discussion
5. Conclusions
6. Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Storey, R.F.; Angiolillo, D.J.; Patil, S.B.; Desai, B.; Ecob, R.; Husted, S.; Emanuelsson, H.; Cannon, C.P.; Becker, R.C.; Wallentin, L. Inhibitory effects of ticagrelor compared with clopidogrel on platelet function in patients with acute coronary syndromes: The PLATO (PLATelet inhibition and patient Outcomes) PLATELET substudy. J. Am. Coll. Cardiol. 2010, 56, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, D.; Galati, A.; Xanthopoulou, I.; Mavronasiou, E.; Kassimis, G.; Theodoropoulos, K.C.; Makris, G.; Damelou, A.; Tsigkas, G.; Hahalis, G.; et al. Ticagrelor versus Prasugrel in Acute Coronary Syndrome Patients with High On-Clopidogrel Platelet Reactivity Following Percutaneous Coronary Intervention: A Pharmacodynamic Study. J. Am. Coll. Cardiol. 2012, 60, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 130, 2354–2394. [Google Scholar] [CrossRef]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevationTask Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Sun, Y.; Zhang, Y.; Liu, B.; Fang, L.; Shen, C.; Li, Y.; Meng, S. Effect of a 180 mg ticagrelor loading dose on myocardial necrosis in patients undergoing elective percutaneous coronary intervention: A preliminary study. Cardiol. J. 2017, 24, 15–24. [Google Scholar] [CrossRef]
- Bonello, L.; Laine, M.; Thuny, F.; Paganelli, F.; Lemesle, G.; Roch, A.; Kerbaul, F.; Dignat-George, F.; Berbis, J.; Frere, C. Platelet reactivity in patients receiving a maintenance dose of P2Y12-ADP receptor antagonists undergoing elective percutaneous coronary intervention. Int. J. Cardiol. 2016, 216, 190–193. [Google Scholar] [CrossRef]
- Orme, R.C.; Parker, W.A.E.; Thomas, M.R.; Judge, H.M.; Baster, K.; Sumaya, W.; Morgan, K.P.; McMellon, H.C.; Richardson, J.D.; Grech, E.D.; et al. Study of Two Dose Regimens of Ticagrelor Compared with Clopidogrel in Patients Undergoing Percutaneous Coronary Intervention for Stable Coronary Artery Disease (STEEL-PCI). Circulation 2018, 138, 1290–1300. [Google Scholar] [CrossRef]
- Kini, A.; Kini, S.; Marmur, J.D.; Bertea, T.; Dangas, G.; Cocke, T.P.; Sharma, S.K. Incidence and mechanism of creatine kinase-MB enzyme elevation after coronary intervention with different devices. Catheter. Cardiovasc. Interv. 1999, 48, 123–129. [Google Scholar] [CrossRef]
- Sharma, S.K.; Dangas, G.; Mehran, R.; Duvvuri, S.; Kini, A.; Cocke, T.P.; Kakarala, V.; Cohen, A.M.; Marmur, J.D.; Ambrose, J.A. Risk Factors for the Development of Slow Flow during Rotational Coronary Atherectomy. Am. J. Cardiol. 1997, 80, 219–222. [Google Scholar] [CrossRef]
- Kini, A.; Marmur, J.D.; Duvvuri, S.; Dangas, G.; Choudhary, S.; Sharma, S.K. Rotational atherectomy: Improved procedural outcome with evolution of technique and equipment. Single-center results of first 1,000 patients. Catheter. Cardiovasc. Interv. 1999, 46, 305–311. [Google Scholar] [CrossRef]
- Dehmer, G.J.; Nichols, T.C.; Bode, A.P.; Liles, D.; Sigman, J.; Li, S.; Koch, G.; Tate, D.A.; Griggs, T.R. Assessment of platelet activation by coronary sinus blood sampling during balloon angioplasty and directional coronary atherectomy. Am. J. Cardiol. 1997, 80, 871–877. [Google Scholar] [CrossRef]
- Bau, J.; Gutensohn, K.; Kuck, K.H.; Beythien, C.; Stein, J.; Kühnl, P. [Flow-cytometric analysis of platelet activation during rotablation]. Z. Kardiol. 2000, 89, 15–20. [Google Scholar] [CrossRef]
- Giannitsis, E.; Kurz, K.; Hallermayer, K.; Jarausch, J.; Jaffe, A.S.; Katus, H.A. Analytical validation of a high-sensitivity cardiac troponin T assay. Clin. Chem. 2010, 56, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Basit, M.; Bakshi, N.; Hashem, M.; Allebban, Z.; Lawson, N.; Rosman, H.S.; Maciejko, J.J. The effect of freezing and long-term storage on the stability of cardiac troponin T. Am. J. Clin. Pathol. 2007, 128, 164–167. [Google Scholar] [CrossRef]
- Huber, M.S.; Mooney, J.F.; Madison, J.; Mooney, M.R. Use of a morphologic classification to predict clinical outcome after dissection from coronary angioplasty. Am. J. Cardiol. 1991, 68, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef]
- Ellis, S.G.; Popma, J.J.; Buchbinder, M.; Franco, I.; Leon, M.B.; Kent, K.M.; Pichard, A.D.; Satler, L.F.; Topol, E.J.; Whitlow, P.L. Relation of clinical presentation, stenosis morphology, and operator technique to the procedural results of rotational atherectomy and rotational atherectomy-facilitated angioplasty. Circulation 1994, 89, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Reisman, M.; Shuman, B.J.; Harms, V. Analysis of heat generation during rotational atherectomy using different operational techniques. Catheter. Cardiovasc. Diagn. 1998, 44, 453–455. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Lincoff, A.M.; Califf, R.M.; Simoons, M.L.; Tcheng, J.E.; Brener, S.J.; Wolski, K.E.; Topol, E.J. The benefit of abciximab in percutaneous coronary revascularization is not device-specific. Am. J. Cardiol. 2000, 85, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Koch, K.C.; vom Dahl, J.; Kleinhans, E.; Klues, H.G.; Radke, P.W.; Ninnemann, S.; Schulz, G.; Buell, U.; Hanrath, P. Influence of a platelet GPIIb/IIIa receptor antagonist on myocardial hypoperfusion during rotational atherectomy as assessed by myocardial Tc-99m sestamibi scintigraphy. J. Am. Coll. Cardiol. 1999, 33, 998–1004. [Google Scholar] [CrossRef]
- Kini, A.; Reich, D.; Marmur, J.D.; Mitre, C.A.; Sharma, S.K. Reduction in periprocedural enzyme elevation by abciximab after rotational atherectomy of type B2 lesions: Results of the Rota ReoPro randomized trial. Am. Heart J. 2001, 142, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Reisman, M.; Shuman, B.J.; Dillard, D.; Fei, R.; Misser, K.H.; Gordon, L.S.; Harms, V. Analysis of low-speed rotational atherectomy for the reduction of platelet aggregation. Cathet. Cardiovasc. Diagn. 1998, 45, 208–214. [Google Scholar] [CrossRef]
- Whitlow, P.L.; Bass, T.A.; Kipperman, R.M.; Sharaf, B.L.; Ho, K.K.; Cutlip, D.E.; Zhang, Y.; Kuntz, R.E.; Williams, D.O.; Lasorda, D.M.; et al. Results of the study to determine rotablator and transluminal angioplasty strategy (STRATAS). Am. J. Cardiol. 2001, 87, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Tricoci, P. Consensus or Controversy? Evolution of Criteria for Myocardial Infarction after Percutaneous Coronary Intervention. Clin. Chem. 2017, 63, 82–90. [Google Scholar] [CrossRef]
- Nienhuis, M.B.; Ottervanger, J.P.; Bilo, H.J.G.; Dikkeschei, B.D.; Zijlstra, F. Prognostic value of troponin after elective percutaneous coronary intervention: A meta-analysis. Catheter. Cardiovasc. Interv. 2008, 71, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G.; Colleran, R.; Braun, S.; Cassese, S.; Hieber, J.; Fusaro, M.; Kufner, S.; Ott, I.; Byrne, R.A.; Husser, O.; et al. High-Sensitivity Troponin T and Mortality after Elective Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2016, 68, 2259–2268. [Google Scholar] [CrossRef]
- Tricoci, P.; Leonardi, S.; White, J.; White, H.D.; Armstrong, P.W.; Montalescot, G.; Giugliano, R.P.; Gibson, C.M.; Van de Werf, F.; Califf, R.M.; et al. Cardiac troponin after percutaneous coronary intervention and 1-year mortality in non-ST-segment elevation acute coronary syndrome using systematic evaluation of biomarker trends. J. Am. Coll. Cardiol. 2013, 62, 242–251. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Clopidogrel (n = 84) | Ticagrelor (n = 89) | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Diagnosis at admission | 0.885 | ||||
| Stable CAD | 73 | 86.9 | 78 | 87.6 | |
| ACS | 11 | 13.1 | 11 | 12.4 | |
| Male gender | 61/84 | 72.6 | 71/89 | 79.8 | 0.269 |
| Age (years) | 76.7 | ±10.3 * | 74.8 | ±9.9 | 0.213 |
| Smoking | 0.465 | ||||
| No | 47 | 56.0 | 41 | 46.6 | |
| Former smoker | 27 | 32.1 | 35 | 39.8 | |
| Current smoker | 10 | 11.9 | 12 | 13.6 | |
| Treated arterial hypertension | 64/84 | 76.2 | 61/89 | 68.5 | 0.261 |
| Treated dyslipidaemia | 45/84 | 53.6 | 44/88 | 50.0 | 0.639 |
| Type 2 Diabetes mellitus | 0.546 | ||||
| No | 56 | 66.7 | 56 | 62.9 | |
| Yes (regimen) | 4 | 4.8 | 8 | 9.0 | |
| Yes (treated) | 24 | 28.6 | 25 | 28.1 | |
| Body mass index (kg/m2) | 26.2 | ± 4.2 | 26.7 | ±4.4 | 0.414 |
| Cardiac frequency (bpm) | 72.4 | ±12.2 | 73.4 | ±16.6 | 0.649 |
| GFR < 60 mL/min/1.73 m2 † | 32/84 | 38.1 | 29/88 | 33.0 | 0.481 |
| C reactive protein (mg/L) | 2.9 | (1.3–6.6) ‡ | 3.0 | (1.2–8.0) | 0.985 |
| Systolic blood pressure (mmHg) | 139 | ±22 | 140 | ±19 | 0.682 |
| Diastolic blood pressure (mmHg) | 73 | ±15 | 75 | ± 12 | 0.376 |
| Left ventricular ejection fraction (%) | 50.2 | ±12.5 | 52.6 | ±11.6 | 0.265 |
| Clopidogrel (n = 84) | Ticagrelor (n = 89) | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Procedural characteristics | |||||
| Left main stenosis | 0.108 | ||||
| None | 56 | 67.5 | 53 | 59.6 | |
| <50% | 6 | 7.2 | 16 | 18.0 | |
| >50% | 21 | 25.3 | 20 | 22.5 | |
| LAD stenosis | 0.986 | ||||
| None | 7 | 8.3 | 7 | 7.9 | |
| <50% | 7 | 8.3 | 7 | 7.9 | |
| >50% | 70 | 83.3 | 75 | 84.3 | |
| CX stenosis | 0.925 | ||||
| None | 27 | 32.1 | 30 | 33.7 | |
| <50% | 11 | 13.1 | 10 | 11.2 | |
| >50% | 46 | 54.8 | 49 | 55.1 | |
| RCA stenosis | 0.224 | ||||
| None | 20 | 23.8 | 13 | 14.6 | |
| <50% | 5 | 6.0 | 9 | 10.1 | |
| >50% | 59 | 70.2 | 67 | 75.3 | |
| Number of lesions treated with RA | 0.497 | ||||
| 1 | 64 | 76.2 | 59 | 67.8 | |
| 2 | 17 | 20.2 | 23 | 26.4 | |
| 3 | 3 | 3.6 | 5 | 5.7 | |
| RA procedure for left main | 16/84 | 19.0 | 15/87 | 17.2 | 0.759 |
| RA procedure for LAD | 40/84 | 47.6 | 48/87 | 55.2 | 0.323 |
| RA procedure for CX | 11/84 | 13.1 | 14/87 | 16.1 | 0.579 |
| RA procedure for RCA | 30/84 | 35.7 | 32/87 | 36.8 | 0.885 |
| Radial vascular access | 58/71 | 81.7 | 66/76 | 86.8 | 0.390 |
| Sheath caliber | 0.053 | ||||
| 6 Fr | 62 | 87.3 | 73 | 96.1 | |
| 7 Fr | 9 | 12.7 | 3 | 4.0 | |
| Predilatation | 81/84 | 96.4 | 77/85 | 90.6 | 0.124 |
| Stent implantation in RA-treated lesion (s) | 84/84 | 100.0 | 86/87 | 98.9 | 1 |
| PCI for another lesion (same procedure) | 30/84 | 35.7 | 21/87 | 24.1 | |
| Number of burrs used | 0.659 | ||||
| 1 | 60 | 72.3 | 59 | 67.8 | |
| 2 | 19 | 22.9 | 21 | 24.1 | |
| 3 or 4 | 4 | 4.8 | 7 | 8.0 | |
| Burr diameter * | 0.927 | ||||
| 1.25 | 10 | 11.8 | 10 | 11.5 | |
| 1.5 | 57 | 67.1 | 60 | 69.0 | |
| >1.5 | 18 | 21.2 | 17 | 19.5 | |
| Reference Vessel Diameter (mm) † | 3.35 | ±0.52 ‡ | 3.34 | ±0.50 | 0.908 |
| Total number of burr runs | 3.6 | ±2.0 | 4.0 | ±2.3 | 0.259 |
| Minimal speed used (rev/min) | 169,398 | ±14,140 | 168,494 | ±14,158 | 0.678 |
| Maximal speed used (rev/min) | 178,602 | ±11,210 | 178,529 | ±14,268 | 0.970 |
| Burr runs total length (seconds) | 34 | (24–56) § | 39 | (25–62) | 0.316 |
| Procedural success | 82/84 | 97.6 | 87/89 | 97.8 | 0.953 |
| Clopidogrel (n = 84) | Ticagrelor (n = 89) | p | |||
|---|---|---|---|---|---|
| Mean (SD) | Median (Q1–Q3) | Mean (SD) | Median (Q1–Q3) | ||
| Troponin (ng/L) H00 | 154 (588) | 24 (12–44) | 113 (345) | 21 (13–42) | 0.694 |
| Troponin (ng/L) H06 | 200 (633) | 48 (28–88) | 162 (350) | 52 (30–130) | 0.446 |
| Troponin (ng/L) H12 | 249 (616) | 81 (48–178) | 226 (395) | 95 (48–225) | 0.347 |
| Troponin (ng/L) H18 | 277 (593) | 106 (59–205) | 290 (651) | 130 (57–286) | 0.479 |
| Troponin (ng/L) H24 | 297 (559) | 107 (62–286) | 283 (584) | 141 (57–298) | 0.805 |
| AUC Troponin H00–H24 | 5746 (14,412) | 1847 (1155–4094) | 5316 (10,900) | 2264 (1108–5275) | |
| AUC Troponin H00–H24 (ln) | 7.74 (1.13) | 7.52 (7.05–8.32) | 7.83 (1.13) | 7.72 (7.01–8.57) | |
| Adj. Mean * | SD | Adj. Mean * | SD | ||
| AUC Troponin H00–H24 (ln) | 8.77 | 0.34 | 8.85 | 0.33 | 0.606 |
| b | p | |
|---|---|---|
| ACS | 1.30 | <0.001 |
| GFR > 60 mL/min/1.73 m2) | 0.52 | 0.001 |
| C-Reactive protein (mg/L) * | 0.13 | 0.016 |
| >1 lesion treated with RA | 0.39 | 0.021 |
| R2 = 0.327 | ||
| n = 149 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lhermusier, T.; Motreff, P.; Bataille, V.; Cayla, G.; Farah, B.; Roncalli, J.; Elbaz, M.; Boudou, N.; Campello-Parada, F.; Bouisset, F.; et al. TIcagrelor in Rotational Atherectomy to Reduce TROPonin Enhancement: The TIRATROP Study, A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 1445. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041445
Lhermusier T, Motreff P, Bataille V, Cayla G, Farah B, Roncalli J, Elbaz M, Boudou N, Campello-Parada F, Bouisset F, et al. TIcagrelor in Rotational Atherectomy to Reduce TROPonin Enhancement: The TIRATROP Study, A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(4):1445. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041445
Chicago/Turabian StyleLhermusier, Thibault, Pascal Motreff, Vincent Bataille, Guillaume Cayla, Bruno Farah, Jerome Roncalli, Meyer Elbaz, Nicolas Boudou, Fransisco Campello-Parada, Frederic Bouisset, and et al. 2023. "TIcagrelor in Rotational Atherectomy to Reduce TROPonin Enhancement: The TIRATROP Study, A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 4: 1445. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041445