
Long-Term Results of Endoscopic Metal Stenting for Biliary Anastomotic Stricture after Liver Transplantation
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Liver Transplantation
2.2. Endoscopic Management
2.3. Surgical Management
2.4. Data Collection
2.5. Outcomes
2.6. Statistics
3. Results
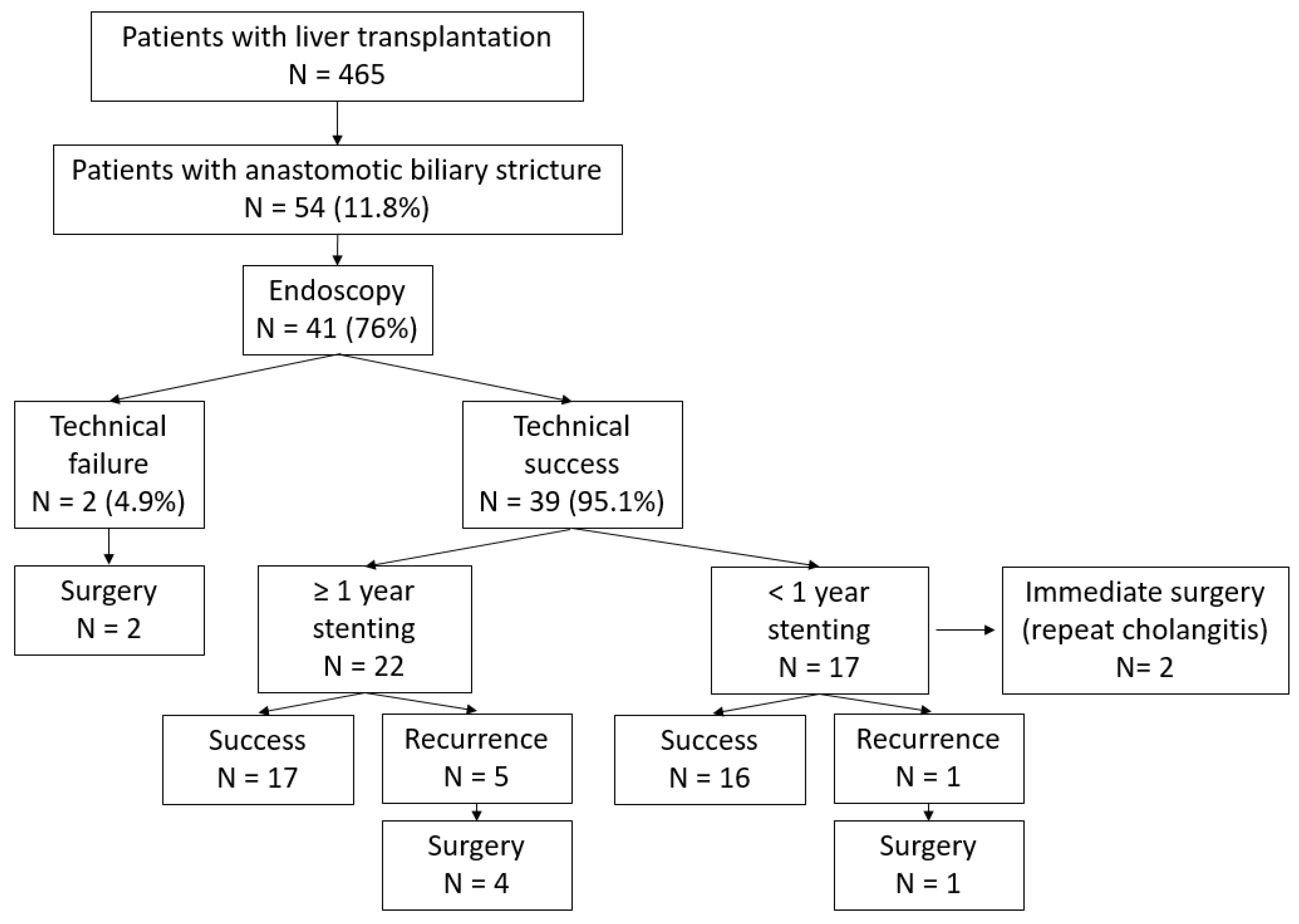
3.1. Patients and Management
3.2. Endoscopic Treatment Failure
3.3. Recurrence of ABS and Risk Factors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verdonk, R.C.; Buis, C.I.; Porte, R.J.; Haagsma, E.B. Biliary complications after liver transplantation: A review. Scand. J. Gastroenterol. 2006, 41, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Cantù, P.; Tenca, A.; Donato, M.; Rossi, G.; Forzenigo, L.; Piodi, L.; Rigamonti, C.; Agnelli, F.; Biondetti, P.; Conte, D.; et al. ERCP and short-term stent-trial in patients with anastomotic biliary stricture following liver transplantation. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2009, 41, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Gurakar, A.; Jabbour, N. Biliary strictures following liver transplantation: Past, present and preventive strategies. Liver Transpl. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transpl. Soc. 2008, 14, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Verdonk, R.C.; Buis, C.I.; Porte, R.J.; van der Jagt, E.J.; Limburg, A.J.; van den Berg, A.P.; Slooff, M.J.H.; Peeters, P.M.J.G.; de Jong, K.P.; Kleibeuker, J.H.; et al. Anastomotic biliary strictures after liver transplantation: Causes and consequences. Liver Transpl. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transpl. Soc. 2006, 12, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Linhares, M.; Gonzalez, A.; Goldman, S.; Coelho, R.; Sato, N.; Moura, R.; Silva, M.; Lanzoni, V.; Salzedas, A.; Serra, C.; et al. Magnetic resonance cholangiography in the diagnosis of biliary complications after orthotopic liver transplantation. Transplant. Proc. 2004, 36, 947–948. [Google Scholar] [CrossRef]
- Dumonceau, J.-M.; Tringali, A.; Papanikolaou, I.S.; Blero, D.; Mangiavillano, B.; Schmidt, A.; Vanbiervliet, G.; Costamagna, G.; Devière, J.; García-Cano, J.; et al. Endoscopic biliary stenting: Indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline—Updated October 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef]
- Holt, A.P.; Thorburn, D.; Mirza, D.; Gunson, B.; Wong, T.; Haydon, G. A Prospective Study of Standardized Nonsurgical Therapy in the Management of Biliary Anastomotic Strictures Complicating Liver Transplantation. Transplantation 2007, 84, 857–863. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485.
- Landi, F.; De’Angelis, N.; Sepulveda, A.; Martínez-Pérez, A.; Sobhani, I.; Laurent, A.; Soubrane, O. Endoscopic treatment of anastomotic biliary stricture after adult deceased donor liver transplantation with multiple plastic stents versus self-expandable metal stents: A systematic review and meta-analysis. Transpl. Int. Off. J. Eur. Soc. Organ. Transpl. 2018, 31, 131–151. [Google Scholar] [CrossRef]
- Lee, D.W.; Jo, H.H.; Abdullah, J.; Kahaleh, M. Endoscopic Management of Anastomotic Strictures after Liver Transplantation. Clin. Endosc. 2016, 49, 457–461. [Google Scholar] [CrossRef]
- Jarlot-Gas, C.; Muscari, F.; Mokrane, F.-Z.; Del Bello, A.; Culetto, A.; Buscail, E.; Péré, G.; Fares, N.; Péron, J.-M.; Cuellar, E.; et al. Management of anastomotic biliary stricture after liver transplantation and impact on survival. HPB 2021, 23, 1259–1268. [Google Scholar] [CrossRef]
- Aparício, D.P.d.S.; Otoch, J.P.; Montero, E.F.d.S.; Khan, M.A.; Artifon, E.L.d.A. Endoscopic approach for management of biliary strictures in liver transplant recipients: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2017, 5, 827–845. [Google Scholar] [CrossRef]
- Hamada, Y.; Ando, H.; Kamisawa, T.; Itoi, T.; Urushihara, N.; Koshinaga, T.; Saito, T.; Fujii, H.; Morotomi, Y. Diagnostic criteria for congenital biliary dilatation 2015. J. Hepato-Biliary-Pancreat. Sci. 2016, 23, 342–346. [Google Scholar] [CrossRef]
- Laurent, A.; Tayar, C.; Andréoletti, M.; Lauzet, J.-Y.; Merle, J.-C.; Cherqui, D. Laparoscopic liver resection facilitates salvage liver transplantation for hepatocellular carcinoma. J. Hepato-Biliary-Pancreat. Surg. 2009, 16, 310–314. [Google Scholar] [CrossRef]
- Tayar, C.; Kluger, M.D.; Laurent, A.; Cherqui, D. Optimizing outflow in piggyback liver transplantation without caval occlusion: The three-vein technique. Liver Transpl. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transpl. Soc. 2011, 17, 88–92. [Google Scholar] [CrossRef]
- Kato, H.; Kawamoto, H.; Tsutsumi, K.; Harada, R.; Fujii, M.; Hirao, K.; Kurihara, N.; Mizuno, O.; Ishida, E.; Ogawa, T.; et al. Long-term outcomes of endoscopic management for biliary strictures after living donor liver transplantation with duct-to-duct reconstruction. Transpl. Int. Off. J. Eur. Soc. Organ. Transpl. 2009, 22, 914–921. [Google Scholar] [CrossRef]
- Chang, J.H.; Lee, I.S.; Choi, J.Y.; Yoon, S.K.; Kim, D.G.; You, Y.K.; Chun, H.J.; Lee, D.K.; Choi, M.-G.; Chung, I.-S. Biliary Stricture after Adult Right-Lobe Living-Donor Liver Transplantation with Duct-to-Duct Anastomosis: Long-Term Outcome and Its Related Factors after Endoscopic Treatment. Gut Liver 2010, 4, 226–233. [Google Scholar] [CrossRef]
- Sato, T.; Kogure, H.; Nakai, Y.; Hamada, T.; Takahara, N.; Mizuno, S.; Kawaguchi, Y.; Akamatsu, N.; Kaneko, J.; Hasegawa, K.; et al. Long-term outcomes of endoscopic treatment for duct-to-duct anastomotic strictures after living donor liver transplantation. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39, 1954–1963. [Google Scholar] [CrossRef]
- Tringali, A.; Barbaro, F.; Pizzicannella, M.; Boškoski, I.; Familiari, P.; Perri, V.; Gigante, G.; Onder, G.; Hassan, C.; Lionetti, R.; et al. Endoscopic management with multiple plastic stents of anastomotic biliary stricture following liver transplantation: Long-term results. Endoscopy 2016, 48, 546–551. [Google Scholar] [CrossRef]
- Martins, F.P.; De Paulo, G.A.; Contini, M.L.; Ferrari, A.P. Metal versus plastic stents for anastomotic biliary strictures after liver transplantation: A randomized controlled trial. Gastrointest. Endosc. 2018, 87, 131.e1–131.e13. [Google Scholar] [CrossRef]
- Conigliaro, R.; Pigò, F.; Bertani, H.; Greco, S.; Burti, C.; Indriolo, A.; Di Sario, A.; Ortolani, A.; Maroni, L.; Tringali, A.; et al. Migration rate using fully covered metal stent in anastomotic strictures after liver transplantation: Results from the BASALT study group. Liver Int. Off. J. Int. Assoc. Study Liver 2022, 42, 1861–1871. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, L.W.; Martins, F.P.; De Paulo, G.A.; Contini, M.L.C.; Ferrari, A.P.; Della Libera, E. Endoscopic therapy using a self-expandable metallic stent with an anti-migration system for postorthotopic liver transplantation anastomotic biliary stricture. World J. Gastrointest. Endosc. 2022, 14, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, H.; Mikata, R.; Ishihara, T.; Sakai, Y.; Sugiyama, H.; Yasui, S.; Tsuyuguchi, T. Efficacy of multiple biliary stenting for refractory benign biliary strictures due to chronic calcifying pancreatitis. World J. Gastrointest. Endosc. 2017, 9, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Macías-Gómez, C.; Dumonceau, J.-M. Endoscopic management of biliary complications after liver transplantation: An evidence-based review. World J. Gastrointest. Endosc. 2015, 7, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Harshavardhan, R.B.; Hasim, A.; Suprabha, P.; Sudhindran, S.; Venu, R.P.; Rao, H.B.; Ahamed, H.; Panicker, S. Endoscopic therapy for biliary strictures complicating living donor liver transplantation: Factors predicting better outcome. World J. Gastrointest. Pathophysiol. 2017, 8, 77–86. [Google Scholar] [CrossRef]


{kind=link}
| Cohort | Failed Endoscopic Treatment | Successful Endoscopic Treatment | p-Value | |
|---|---|---|---|---|
| (N = 41) | (N = 9) | (N = 32) | ||
| Age at LT, years | 53.1 (10) (20.4; 69.9) | 50.5 (10.3) (31.4; 61.5) | 53.8 (9.9) (20.4; 69.9) | 0.415 |
| Gender | ||||
| Female | 6 (14.6%) | 2 (22.2%) | 4 (12.5%) | 0.597 |
| Male | 35 (85.4%) | 7 (77.8%) | 28 (87.5%) | |
| MELD score prior to LT | 20.3 (11.1) (6; 40) | 23.7 (7.3) (12.7; 33.2) | 19.4 (11.9) (6; 40) | 0.197 |
| Number of prior LTs | 1.1 (0.3) (1; 2) | 1 (0) (1; 1) | 1.1 (0.3) (1; 2) | 0.044 |
| LT indication | ||||
| Other | 30 (73.2%) | 5 (55.6%) | 25 (78.1%) | 0.217 |
| Cirrhosis | 11 (26.8%) | 4 (44.4%) | 7 (21.9%) | |
| Type of donor | ||||
| DDLT | 41 (100%) | 9 (100%) | 32 (100%) | --- |
| LDLT | 0 (0%) | 0 (0%) | 0 (0%) | |
| Domino | 0 (0%) | 0 (0%) | 0 (0%) | |
| Type of graft | ||||
| Full Graft | 36 (87.8%) | 9 (100%) | 27 (84.4%) | |
| Right liver | 5 (12.2%) | 0 (0%) | 5 (15.6%) | 0.568 |
| Left liver | 0 (0%) | 0 (0%) | 0 (0%) | --- |
| Donor age, years | 54.9 (19.7) (19; 89) | 64 (12.2) (50; 80) | 52.2 (20.8) (19; 89) | 0.043 |
| CMV mismatch (R−/D+) | ||||
| No | 26 (63.4%) | 5 (55.6%) | 21 (65.6%) | 0.701 |
| Yes | 15 (36.6%) | 4 (44.4%) | 11 (34.4%) | |
| Pre-LT cold ischemia duration | 7.6 (2) (4.1; 12.3) | 7.9 (2.1) (5.6; 11.9) | 7.5 (1.9) (4.1; 12.3) | 0.625 |
| Duration of LT | 7.9 (1.9) (4.5; 15) | 8.5 (3) (4.5; 15) | 7.7 (1.4) (4.7; 10.7) | 0.444 |
| Cohort | Failed Endoscopic Treatment | Successful Endoscopic Treatment | p-Value | |
|---|---|---|---|---|
| (N = 41) | (N = 9) | (N = 32) | ||
| LT to diagnosis delay (months) | 7.4 (10.6) (0; 54) | 7.2 (6.9) (0; 18) | 7.5 (11.6) (0; 54) | 0.937 |
| Associated bile leak | 10 (24.4%) | 2 (22.2%) | 8 (25%) | 0.99 |
| Baseline LFTs | ||||
| AP | 332.3 (206.7) (62; 1077) | 377.3 (211.2) (76; 713) | 318.7 (207) (62; 1077) | 0.476 |
| GGT | 598.9 (463) (44; 1639) | 551.8 (448.9) (101; 1267) | 613.1 (473.7) (44; 1639) | 0.728 |
| ALT | 133.6 (134.9) (10; 523) | 126.1 (158.3) (20; 523) | 135.9 (130.1) (10; 505) | 0.869 |
| AST | 85.1 (92.2) (14; 526) | 65.3 (59.2) (18; 214) | 91 (100.1) (14; 526) | 0.35 |
| Total bilirubin | 47.4 (82.5) (3; 362) | 49.4 (117.3) (5; 362) | 46.8 (71.6) (3; 304) | 0.95 |
| Conjugated bilirubin | 37.1 (67.8) (1; 322) | 42.1 (105.1) (1; 322) | 35.6 (54.4) (1; 220) | 0.863 |
| Baseline MRI findings | ||||
| Stenosis length (mm) | 10.5 (6.6) (2; 27) | 11 (5.7) (3; 18) | 10.4 (6.9) (2; 27) | 0.82 |
| Stenosis diameter (mm) | 0.6 (1) (0; 5) | 0.7 (0.8) (0; 2) | 0.6 (1.1) (0; 5) | 0.754 |
| Stenosis to hilum distance (mm) | 23.2 (6.9) (11; 37) | 25.3 (7.1) (18; 35) | 22.7 (6.9) (11; 37) | 0.405 |
| Associated stone | 4 (9.8) | 0 (0) | 4 (100) | 0.043 |
| Cohort | Failed Endoscopic Treatment | Successful Endoscopic Treatment | p-Value | |
|---|---|---|---|---|
| (N = 41) | (N = 9) | (N = 32) | ||
| First ERCP | ||||
| Stenosis length | 6.5 (4.5) (2; 20) | 9.2 (7.2) (2; 20) | 5.9 (3.6) (2; 15) | 0.327 |
| Stenosis diameter | 3.3 (1.4) (1; 7) | 2.8 (1) (2; 4) | 3.4 (1.5) (1; 7) | 0.234 |
| Stenosis-to-hilum distance | 24.6 (9.4) (10; 45) | 30 (12.2) (15; 45) | 23.8 (9) (10; 45) | 0.391 |
| IH bile ducts dilatation | 32 (78) | 5 (55.6) | 27 (84.4) | 0.07 |
| Proximal CBD dilatation | 33 (80.5) | 5 (55.6) | 28 (87.5) | 0.07 |
| Technical success (%) | 39 (95.1) | --- | --- | --- |
| Type and size of stent | ||||
| FC-SEMS | 35 (84.6) | 7 (100) | 28 (87.5) | 0.783 |
| 6 cm | 5 | 1 | 4 | |
| 8 cm | 30 | 6 | 24 | |
| Plastic followed by FC-SEMS | 4 (10.3) | 0 (0) | 4 (12.5) | |
| Follow-up during endoscopic treatment | ||||
| ERCPs due to stent migration | ||||
| 0 | 19 (46.3%) | 5 (55.6%) | 14 (43.8%) | 0.442 |
| 1 | 15 (36.6%) | 2 (22.2%) | 13 (40.6%) | |
| 2 | 5 (12.2%) | 1 (11.1%) | 4 (12.5%) | |
| 4 | 1 (2.4%) | 0 (0%) | 1 (3.1%) | |
| Number of stent exchange | 1.9 (1.8) (0; 7) | 1.6 (1.5) (0; 4) | 1.9 (1.9) (0; 7) | 0.537 |
| Total number of ERCPs | 3.8 (2) (1; 9) | 3.7 (1.8) (1; 6) | 3.8 (2) (2; 9) | 0.804 |
| Total treatment duration | 12.8 (9.1) (0; 36) | 8.7 (7.3) (0; 22) | 14 (9.3) (3; 36) | 0.633 |
| Anastomotic calibration duration | ||||
| <1 year | 19 (46.3%) | 5 (55.6%) | 14 (43.8%) | 0.709 |
| >1 year | 22 (53.7%) | 4 (44.4%) | 18 (56.2%) | |
| ERCP adverse events | ||||
| Post-sphincterotomy bleeding | 4 (9.8) | 1 | 3 | 0.99 |
| Acute pancreatitis | 6 (15) | 2 | 4 | 0.61 |
| Cholangitis | 2 (4.9) | 1 | 1 | 0.41 |
| Death | 0 (0.0) | 0 | 0 | 1 |
| Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Age at LT | 0.90 | 0.78, 1.05 | 0.2 |
| Gender | |||
| Female | _ | _ | _ |
| Male | 0.04 | 0.00, 3.10 | 0.14 |
| LT to diagnosis delay | 0.97 | 0.85, 1.11 | 0.6 |
| CMV mismatch (R−/D+) | |||
| No | |||
| Yes | 1.72 | 0.13, 23.5 | 0.7 |
| Type of graft | |||
| Full Graft | 13.756.90 | 0.00, inf | >0.9 |
| Right liver | _ | _ | _ |
| Left liver | _ | _ | _ |
| Donor age | 1.05 | 0.97, 1.14 | 0.2 |
| Pre-LT cold ischemia duration | 2.05 | 0.91, 4.60 | 0.079 |
| Baseline MRI findings | |||
| Stenosis length | 1.01 | 0.83, 1.23 | 0.9 |
| Stenosis to hilum short distance | 0.73 | 0.05, 10.7 | 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becq, A.; Laurent, A.; De Roux, Q.; Cremone, C.; Rotkopf, H.; Le Baleur, Y.; Mesli, F.; Duvoux, C.; Amiot, A.; Gagniere, C.; et al. Long-Term Results of Endoscopic Metal Stenting for Biliary Anastomotic Stricture after Liver Transplantation. J. Clin. Med. 2023, 12, 1453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041453
Becq A, Laurent A, De Roux Q, Cremone C, Rotkopf H, Le Baleur Y, Mesli F, Duvoux C, Amiot A, Gagniere C, et al. Long-Term Results of Endoscopic Metal Stenting for Biliary Anastomotic Stricture after Liver Transplantation. Journal of Clinical Medicine. 2023; 12(4):1453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041453
Chicago/Turabian StyleBecq, Aymeric, Alexis Laurent, Quentin De Roux, Cristiano Cremone, Hugo Rotkopf, Yann Le Baleur, Farida Mesli, Christophe Duvoux, Aurélien Amiot, Charlotte Gagniere, and et al. 2023. "Long-Term Results of Endoscopic Metal Stenting for Biliary Anastomotic Stricture after Liver Transplantation" Journal of Clinical Medicine 12, no. 4: 1453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12041453