
Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search Method
2.4. Data Extraction Process
2.5. Statistical Analysis
3. Results
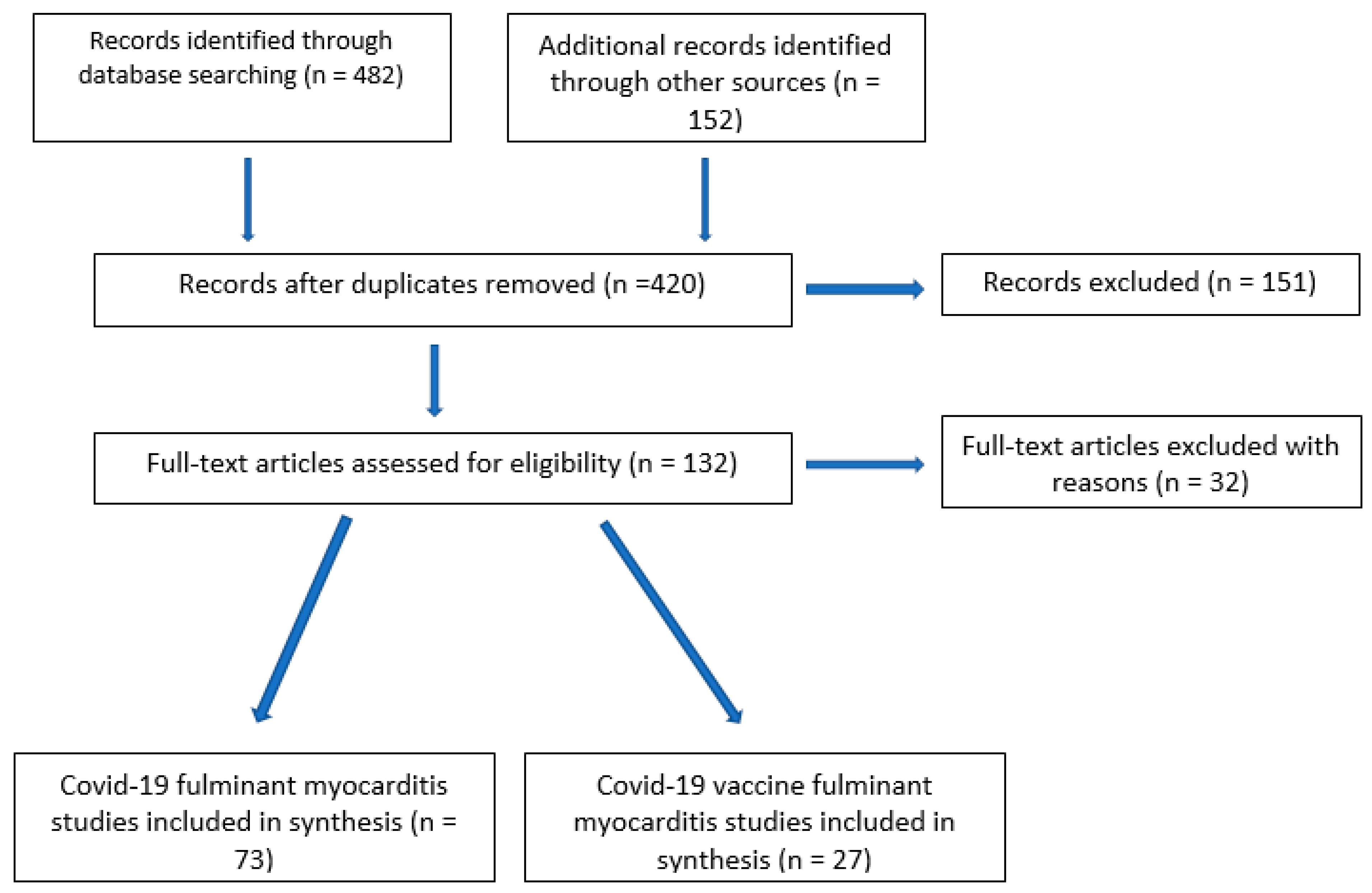
3.1. Literature Search
3.2. Patient Characteristics
3.2.1. Fulminant Myocarditis in COVID-19 Positive Patients
3.2.2. Fulminant Myocarditis after COVID-19 Vaccination
3.2.3. Comparison of COVID-19 FM with COVID-vaccine FM
4. Discussion
- Patients with COVID-19 FM, in comparison with COVID-19 vaccine FM, had higher a heart rate, lower diastolic and mean blood pressures, and a higher prevalence of pulmonary infiltrates on chest X-ray, and they presented more commonly with fever and shortness of breath and less commonly with generalized symptoms.
- Despite differences in presentation, mortality in COVID-19 FM myocarditis and COVID-19 vaccine FM was similar (27.7% and 27.8%, respectively).
- There was no difference in pathology between COVID-19 FM myocarditis and COVID-19 vaccine FM, with most biopsies/autopsies demonstrating lymphocytic infiltrates and some eosinophilic or mixed infiltrates.
- There was no predominance of young males in COVID-19 vaccine FM cases. Females represented 59.3% of this cohort.
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 FM | COVID-19 fulminant myocarditis |
| COVID-19 vaccine FM | COVID-19 vaccine associated fulminant myocarditis |
| CS | Cardiogenic Shock |
| MCS | Mechanical Circulatory Support |
| VA-ECMO | Venoarterial Extracorporeal Membrane Oxygenation |
| IABP | Intraortic Balloon Pump |
| LVEF | Left Ventricular Ejection Fraction |
| ACE2 | Angiotensin-Converting Enzyme-2 |
References
- Guglin, M.; Ballut, K.; Ilonze, O.; Jones, M.; Rao, R. Clinical variants of myocardial involvement in COVID-19-positive patients: A cumulative experience of 2020. Hearth Fail. Rev. 2021, 27, 1341–1353. [Google Scholar] [CrossRef] [PubMed]
- Ilonze, O.J.; Guglin, M.E. Myocarditis following COVID-19 vaccination in adolescents and adults: A cumulative experience of 2021. Hearth Fail. Rev. 2022, 27, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, C.L.; Carmona-Rubio, A.E.; Weiss, A.J.; Procop, G.G.; Starling, R.C.; Rodriguez, E.R. The Enemy within: Sudden-Onset Reversible Cardiogenic Shock with Biopsy-Proven Cardiac Myocyte Infection by Severe Acute Respiratory Syndrome Coronavirus 2. Circulation 2020, 142, 1865–1870. [Google Scholar] [CrossRef]
- Altman, N.L.; Berning, A.A.; Saxon, C.E.; Adamek, K.E.; Wagner, J.A.; Slavov, D.; Quaife, R.A.; Gill, E.A.; Minobe, W.A.; Jonas, E.R.; et al. Myocardial Injury and Altered Gene Expression Associated with SARS-CoV-2 Infection or mRNA Vaccination. JACC Basic Transl. Sci. 2022, in press. [Google Scholar] [CrossRef]
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Afriyie, F.; Fohle, E.; Dekowski, S.S.; Kumar, S. A Case of Isolated SARS-CoV-2 Fulminant Myopericarditis without Respiratory Failure. Cureus 2021, 13, e14003. [Google Scholar] [CrossRef]
- Aldeghaither, S.M.; Qutob, R.M.; Assanangkornchai, N.M.; Issa-Chergui, B.; Tam, M.C.; Larotondo, R.R.; Samoukovic, G.M. Clinical and Histopathologic Features of Myocarditis in Multisystem Inflammatory Syndrome (Adult)—Associated COVID-19. Crit. Care Explor. 2022, 10, e0630. [Google Scholar] [CrossRef]
- Almanza-Hurtado, A.; Martínez-Ávila, M.C.; Rodríguez-Yánez, T.; Paternina-Mendoza, M.C.; Gutiérrez-Ariza, J.C.; Gómez-Arroyo, G. Viral Cardiomyopathies Associated with SARS-CoV-2 Infection. Clin. Med. Insights Case Rep. 2022, 15, 11795476221088140. [Google Scholar] [CrossRef]
- Anupama, B.K.; Thapa, S.S.; Amzuta, I. Transient Cardiomyopathy in a Patient with Coronavirus Disease-2019. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620947577. [Google Scholar] [CrossRef]
- Bergman, Z.R.; Prathibha, S.; Bauman, B.D.; Yannopoulos, D.; Brunsvold, M.E. Venoarteriovenous ECMO in Concomitant Acute Respiratory Distress Syndrome and Cardiomyopathy Associated with COVID-19 Infection. Case Rep. Crit. Care 2021, 2021, 8848013. [Google Scholar] [CrossRef]
- Bernal-Torres, W.; Herrera-Escandón, Á.; Hurtado-Rivera, M.; Plata-Mosquera, C.A. COVID-19 fulminant myocarditis: A case report. Eur. Hearth J. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Kirincich, J.; Rampersad, P.; Soltesz, E.; Krishnan, S. Fulminant myocarditis in COVID-19 and favorable outcomes with VA-ECMO. Resuscitation 2022, 175, 75–76. [Google Scholar] [CrossRef]
- Bulbul, R.F.; Suwaidi, J.A.; Al-Hijji, M.; Tamimi, H.A.; Fawzi, I. COVID-19 Complicated By Acute Respiratory Distress Syndrome, Myocarditis, and Pulmonary Embolism. A Case Report. J. Crit. Care Med. 2021, 7, 123–129. [Google Scholar] [CrossRef]
- Chitturi, K.R.; Thacker, S.; Al-Saadi, M.A.; Kassi, M. Successful treatment of acute heart failure in COVID-19-induced cytokine storm with tocilizumab: A case report. Eur. Hearth J. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Coll, M.D.; Yanamandala, M.; Ferro, E.G.; Nutt, C.T.; Wei, E.Q.; Wang, C.J.; Mehra, M.R. Early Immunosuppression and Rapid Recovery of Cardiogenic Shock in Multisystem Inflammatory Syndrome from Convalescent COVID-19. JACC: Case Rep. 2021, 3, 1403–1408. [Google Scholar] [CrossRef]
- Coyle, J.; Igbinomwanhia, E.; Sanchez-Nadales, A.; Danciu, S.; Chu, C.; Shah, N. A Recovered Case of COVID-19 Myocarditis and ARDS Treated with Corticosteroids, Tocilizumab, and Experimental AT-001. JACC Case Rep. 2020, 2, 1331–1336. [Google Scholar] [CrossRef]
- Craver, R.; Huber, S.; Sandomirsky, M.; McKenna, D.; Schieffelin, J.; Finger, L. Fatal Eosinophilic Myocarditis in a Healthy 17-Year-Old Male with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2c). Fetal Pediatr. Pathol. 2020, 39, 263–268. [Google Scholar] [CrossRef]
- Fiore, G.; Sanvito, F.; Fragasso, G.; Spoladore, R. Case report of cardiogenic shock in COVID-19 myocarditis: Peculiarities on diagnosis, histology, and treatment. Eur. Hearth J. 2021, 5, ytab357. [Google Scholar] [CrossRef]
- Fried, J.A.; Ramasubbu, K.; Bhatt, R.; Topkara, V.K.; Clerkin, K.J.; Horn, E.; Rabbani, L.; Brodie, D.; Jain, S.S.; Kirtane, A.J.; et al. The Variety of Cardiovascular Presentations of COVID-19. Circulation 2020, 141, 1930–1936. [Google Scholar] [CrossRef] [Green Version]
- Garau, G.; Joachim, S.; Duliere, G.; Melissopoulou, M.; Boccar, S.; Fraipont, V.; Dugauquier, C.; Troisfontaines, P.; Hougrand, O.; Delvenne, P.; et al. Sudden cardiogenic shock mimicking fulminant myocarditis in a surviving teenager affected by severe acute respiratory syndrome coronavirus 2 infection. ESC Hearth Fail. 2020, 8, 766–773. [Google Scholar] [CrossRef]
- Garot, J.; Amour, J.; Pezel, T.; Dermoch, F.; Messadaa, K.; Felten, M.L.; Raymond, V.; Baubillier, E.; Sanguineti, F.; Garot, P. SARS-CoV-2 Fulminant Myocarditis. JACC Case Rep. 2020, 2, 1342–1346. [Google Scholar] [CrossRef]
- Gauchotte, G.; Venard, V.; Segondy, M.; Cadoz, C.; Esposito-Fava, A.; Barraud, D.; Louis, G. SARS-Cov-2 fulminant myocarditis: An autopsy and histopathological case study. Int. J. Leg. Med. 2021, 135, 577–581. [Google Scholar] [CrossRef]
- Gaudriot, B.; Mansour, A.; Thibault, V.; Lederlin, M.; Cauchois, A.; Lelong, B.; Ross, J.T.; Leurent, G.; Tadié, J.M.; Revest, M.; et al. Successful heart transplantation for COVID-19-associated post-infectious fulminant myocarditis. ESC Heart Fail. 2021, 8, 2625–2630. [Google Scholar] [CrossRef] [PubMed]
- Gay, H.C.; Sinha, A.; Michel, E.; Mozer, A.B.; Budd, A.; Feinstein, M.J.; Benzuly, K.H.; Al-Qamari, A.; Pawale, A.A.; Vorovich, E.E. Fulminant myocarditis in a patient with coronavirus disease 2019 and rapid myocardial recovery following treatment. ESC Hearth Fail. 2020, 7, 4367–4370. [Google Scholar] [CrossRef] [PubMed]
- Ghafoor, K.; Ahmed, A.; Abbas, M. Fulminant Myocarditis with ST Elevation and Cardiogenic Shock in a SARS-CoV-2 Patient. Cureus 2021, 13, e16149. [Google Scholar] [CrossRef] [PubMed]
- Gill, G.S.; Vlacancich, R.; Mehta, N.; Chaturvedi, M.; Papolos, A. Spectrum of Cardiac Involvement in COVID-19. Cureus 2020, 12, e8638. [Google Scholar] [CrossRef] [PubMed]
- Gómez, H.L.; Bielsa, A.P.; Banzo, M.J.A. Fulminant myocarditis and cardiogenic shock during SARS-CoV-2 infection. Med. Clin. 2020, 155, 463–464. [Google Scholar] [CrossRef]
- Hamdan, R.; E Nassef, M.; Khan, J.; Cheriyan, A.; Yaseen, N.; Singer, N.A.H.M.; Kadri, Z.; Al Nooryani, A. Reverse TakoTsubo or Fulminant myocarditis? Life saving VA ECMO in a COVID 19 patient. Ann. Cardiol. D′angéiologie 2022, 71, 228–231. [Google Scholar] [CrossRef]
- Hu, H.; Ma, F.; Wei, X.; Fang, Y. Coronavirus fulminant myocarditis saved with glucocorticoid and human immunoglobulin. Eur. Heart J. 2021, 42, 206. [Google Scholar] [CrossRef] [Green Version]
- Hussain, H.; Fadel, A.; Alwaeli, H.; Guardiola, V. Coronavirus (COVID-19) Fulminant Myopericarditis and Acute Respiratory Distress Syndrome (ARDS) in a Middle-Aged Male Patient. Cureus 2020, 12, e8808. [Google Scholar] [CrossRef]
- Irabien-Ortiz, Á.; Carreras-Mora, J.; Sionis, A.; Pàmies, J.; Montiel, J.; Tauron, M. Fulminant myocarditis due to COVID-19. Rev. Esp. Cardiol. 2020, 73, 503–504. [Google Scholar] [CrossRef]
- Ishikura, H.; Maruyama, J.; Hoshino, K.; Matsuoka, Y.; Yano, M.; Arimura, T.; Katano, H.; Kato, S.; Kitamura, T.; Nakamura, Y. Coronavirus disease (COVID-19) associated delayed-onset fulminant myocarditis in patient with a history of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. J. Infect. Chemother. 2021, 27, 1760–1764. [Google Scholar] [CrossRef]
- Jacobs, W.; Lammens, M.; Kerckhofs, A.; Voets, E.; Van San, E.; Van Coillie, S.; Peleman, C.; Mergeay, M.; Sirimsi, S.; Matheeussen, V.; et al. Fatal lymphocytic cardiac damage in coronavirus disease 2019 (COVID-19): Autopsy reveals a ferroptosis signature. ESC Hearth Fail. 2020, 7, 3772–3781. [Google Scholar] [CrossRef]
- Kallel, O.; Bourouis, I.; Bougrine, R.; Housni, B.; El Ouafi, N.; Ismaili, N. Acute myocarditis related to Covid-19 infection: 2 cases report. Ann. Med. Surg. 2021, 66, 102431. [Google Scholar] [CrossRef]
- Khatri, A.; Wallach, F. Coronavirus disease 2019 (Covid-19) presenting as purulent fulminant myopericarditis and cardiac tamponade: A case report and literature review. Hearth Lung 2020, 49, 858–863. [Google Scholar] [CrossRef]
- Li, A.; Garcia-Bengochea, Y.; Stechel, R.; Azari, B.M. Management of COVID-19 myopericarditis with reversal of cardiac dysfunction after blunting of cytokine storm: A case report. Eur. Hearth J. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Mansour, J.; Short, R.G.; Bhalla, S.; Woodard, P.K.; Verma, A.; Robinson, X.; Raptis, D.A. Acute myocarditis after a second dose of the mRNA COVID-19 vaccine: A report of two cases. Clin. Imaging 2021, 78, 247–249. [Google Scholar] [CrossRef]
- Menter, T.; Cueni, N.; Gebhard, E.C.; Tzankov, A. Case Report: Co-occurrence of Myocarditis and Thrombotic Microangiopathy Limited to the Heart in a COVID-19 Patient. Front. Cardiovasc. Med. 2021, 8, 695010. [Google Scholar] [CrossRef]
- Milla-Godoy, G.C.; Park, R.; Jiang, W.; Hartkopf, M.W.; Treadwell, T. Fulminant COVID-19-Associated Myocarditis in an Otherwise Healthy Female. Cureus 2021, 13, 12736. [Google Scholar] [CrossRef]
- Nakatani, S.; Ohta-Ogo, K.; Nishio, M.; Amemiya, K.; Sato, S.; Sawano, H.; Hatakeyama, K.; Katano, H.; Suzuki, T.; Hirooka, K. Microthrombosis as a cause of fulminant myocarditis-like presentation with COVID-19 proven by endomyocardial biopsy. Cardiovasc. Pathol. 2022, 60, 107435. [Google Scholar] [CrossRef] [PubMed]
- Naneishvili, T.; Khalil, A.; O’Leary, R.; Prasad, N. Fulminant myocarditis as an early presentation of SARS-CoV-2. BMJ Case Rep. 2020, 13, e237553. [Google Scholar] [CrossRef] [PubMed]
- Nwaejike, N.; Strang, T.; Garcia, M.; Charlesworth, M.; Shaw, S.M.; Barnard, J.B. Emergency biventricular assist device implantation in a patient with suspected COVID-19 disease. Anaesth. Rep. 2020, 8, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Okor, I.; Sleem, A.; Zhang, A.; Kadakia, R.; Bob-Manuel, T.; Krim, S.R. Suspected COVID-19–Induced Myopericarditis. Ochsner J. 2021, 21, 181–186. [Google Scholar] [CrossRef]
- Othenin-Girard, A.; Regamey, J.; Lamoth, F.; Horisberger, A.; Glampedakis, E.; Epiney, J.B.; Kuntzer, T.; de Leval, L.; Carballares, M.; Hurni, C.A.; et al. Multisystem inflammatory syndrome with refractory cardiogenic shock due to acute myocarditis and mononeuritis multiplex after SARS-CoV-2 infection in an adult. Swiss Med. Wkly. 2020, 150, w20387. [Google Scholar] [CrossRef]
- Papageorgiou, J.-M.; Almroth, H.; Törnudd, M.; van der Wal, H.; Varelogianni, G.; Lawesson, S.S. Fulminant myocarditis in a COVID-19 positive patient treated with mechanical circulatory support—A case report. Eur. Hearth J. 2020, 5, ytaa523. [Google Scholar] [CrossRef]
- Purdy, A.; Ido, F.; Sterner, S.; Tesoriero, E.; Matthews, T.; Singh, A. Myocarditis in COVID-19 presenting with cardiogenic shock: A case series. Eur. Hearth J. 2021, 5, ytab028. [Google Scholar] [CrossRef]
- Rajpal, S.; Kahwash, R.; Tong, M.S.; Paschke, K.; Satoskar, A.A.; Foreman, B.; Fuster, V. Fulminant Myocarditis Following SARS-CoV-2 Infection: JACC Patient Care Pathways. JACC Case Rep. 2022, 4, 567–575. [Google Scholar] [CrossRef]
- Richard, I.; Robinson, B.; Dawson, A.; Aya, A.; Ali, R. An Atypical Presentation of Fulminant Myocarditis Secondary to COVID-19 Infection. Cureus 2020, 12, e9179. [Google Scholar] [CrossRef]
- Ruiz, J.G.; Kandah, F.; Dhruva, P.; Ganji, M.; Goswami, R. Case of Coronavirus Disease 2019 Myocarditis Managed with Biventricular Impella Support. Cureus 2021, 13, 13197. [Google Scholar] [CrossRef]
- Salamanca, J.; Díez-Villanueva, P.; Martínez, P.; Cecconi, A.; de Marcos, B.G.; Reyes, G.; Salas, C.; Segovia, J.; Jiménez-Borreguero, L.J.; Alfonso, F. COVID-19 “Fulminant Myocarditis” Successfully Treated with Temporary Mechanical Circulatory Support. JACC: Cardiovasc. Imaging 2020, 13, 2457–2459. [Google Scholar] [CrossRef]
- Sampaio, P.P.N.; Ferreira, R.M.; de Albuquerque, F.N.; Colafranceschi, A.S.; Almeida, A.C.; Nunes, M.A.V.; Filho, J.M.; Lima, R.A.C. Rescue Venoarterial Extracorporeal Membrane Oxygenation After Cardiac Arrest in COVID-19 Myopericarditis: A Case Report. Cardiovasc. Revascul. Med. 2020, 28, 57–60. [Google Scholar] [CrossRef]
- Sánchez-Recalde, Á.; Solano-López, J.; Miguelena-Hycka, J.; Martín-Pinacho, J.J.; Sanmartín, M.; Zamorano, J.L. COVID-19 and cardiogenic shock. Different cardiovascular presentations with high mortality. Rev. Esp. Cardiol. 2020, 73, 669–672. [Google Scholar] [CrossRef]
- Shah, J.Z.; Kumar, S.A.; Patel, A.A. Myocarditis and Pericarditis in Patients with COVID-19. Heart Views 2020, 21, 209–214. [Google Scholar]
- Shahrami, B.; Davoudi-Monfared, E.; Rezaei, Z.; Gheibi, S.; Ardabili, A.V.; Arabzadeh, A.A.; Talebi, A.; Mojtahedzadeh, M. Management of a critically ill patient with COVID-19-related fulminant myocarditis: A case report. Respir. Med. Case Rep. 2022, 36, 101611. [Google Scholar] [CrossRef]
- Shen, M.; Milner, A.; Foppiano Palacios, C.; Ahmad, T. Multisystem inflammatory syndrome in adults (MIS-A) associated with SARS-CoV-2 infection with delayed-onset myocarditis: Case report. Eur. Heart J. Case Rep. 2021, 5, ytab470. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Thaker, R.; Shah, A.; Kim, J.; Kassi, M. Acute Circulatory Collapse and Advanced Therapies in Patients with COVID-19 Infection. Methodist DeBakey Cardiovasc. J. 2021, 17, 43–52. [Google Scholar] [CrossRef]
- Thomson, A.; Totaro, R.; Cooper, W.; Dennis, M. Fulminant Delta COVID-19 myocarditis: A case report of fatal primary cardiac dysfunction. Eur. Hearth J. 2022, 6, ytac142. [Google Scholar] [CrossRef]
- Trpkov, C.; MacMullan, P.; Feuchter, P.; Kachra, R.; Heydari, B.; Merchant, N.; Bristow, M.S.; White, J.A. Rapid Response to Cytokine Storm Inhibition Using Anakinra in a Patient with COVID-19 Myocarditis. CJC Open 2020, 3, 210–213. [Google Scholar] [CrossRef]
- Verma, A.K.; Olagoke, O.; Moreno, J.D.; Rezaee, N.; Ma, P.; Liu, J.; Javaheri, A.; Lavine, K.; Lin, C.-Y. SARS-CoV-2-Associated Myocarditis: A Case of Direct Myocardial Injury. Circ. Heart Fail. 2022, 15, e008273. [Google Scholar] [CrossRef] [PubMed]
- Veronese, G.; Cipriani, M.; Bottiroli, M.; Garascia, A.; Mondino, M.; Pedrotti, P.; Pini, D.; Cozzi, O.; Messina, A.; Droandi, G.; et al. Fulminant myocarditis triggered by OC43 subtype coronavirus: A disease deserving evidence-based care bundles. J. Cardiovasc. Med. 2020, 21, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Yalcinkaya, D.; Yarlioglues, M.; Yigit, H.; Caydere, M.; Murat, S.N. Cardiac mobile thrombi formation in an unvaccinated young man with SARS-CoV-2 associated fulminant eosinophilic myocarditis. Eur. Heart J. Case Rep. 2022, 6, ytac036. [Google Scholar] [CrossRef] [PubMed]
- Yeleti, R.; Guglin, M.; Saleem, K.; Adigopula, S.V.; Sinha, A.; Upadhyay, S.; Everett, J.E.; Ballut, K.; Uppuluri, S.; Rao, R.A. Fulminant myocarditis: COVID or not COVID? Reinfection or co-infection? Future Cardiol. 2021, 17, 1307–1311. [Google Scholar] [CrossRef]
- Zeng, J.-H.; Liu, Y.-X.; Yuan, J.; Wang, F.-X.; Wu, W.-B.; Li, J.-X.; Wang, L.-F.; Gao, H.; Wang, Y.; Dong, C.-F.; et al. First case of COVID-19 complicated with fulminant myocarditis: A case report and insights. Infection 2020, 48, 773–777. [Google Scholar] [CrossRef] [Green Version]
- Abbate, A.; Gavin, J.; Madanchi, N.; Kim, C.; Shah, P.R.; Klein, K.; Boatman, J.; Roberts, C.; Patel, S.; Danielides, S. Fulminant myocarditis and systemic hyperinflammation temporally associated with BNT162b2 mRNA COVID-19 vaccination in two patients. Int. J. Cardiol. 2021, 340, 119–121. [Google Scholar] [CrossRef]
- Agdamag, A.C.C.; Gonzalez, D.; Carlson, K.; Konety, S.; McDonald, W.C.; Martin, C.M.; Maharaj, V.; Alexy, T. Fulminant myocarditis following coronavirus disease 2019 vaccination: A case report. Eur. Hearth J. 2022, 6, ytac007. [Google Scholar] [CrossRef]
- Ameratunga, R.; Woon, S.T.; Sheppard, M.N.; Garland, J.; Ondruschka, B.; Wong, C.X.; Stewart, R.A.; Tatley, M.; Stables, S.R.; Tse, R.D. First Identified Case of Fatal Fulminant Necrotizing Eosinophilic Myocarditis Following the Initial Dose of the Pfizer-BioNTech mRNA COVID-19 Vaccine (BNT162b2, Comirnaty): An Extremely Rare Idiosyncratic Hypersensitivity Reaction. J. Clin. Immunol. 2022, 42, 441–447. [Google Scholar] [CrossRef]
- Araki, T.; Morimoto, R.; Ito, R.; Mizutani, T.; Kimura, Y.; Kazama, S.; Oishi, H.; Kuwayama, T.; Hiraiwa, H.; Kondo, T.; et al. A Case of Systemic Capillary Leak Syndrome with Severe Cardiac Dysfunction After mRNA Vaccination for COVID-19. CJC Open 2022, 4, 656–659. [Google Scholar] [CrossRef]
- Brage, E.T.; Ruíz, J.R.; Martín, J.G.; Rodríguez, J.D.O.; Tocino, R.V.; Diego, S.R.; Hernández, P.L.S.; Hernández, L.B.; Sánchez, E.F. Fulminant myocarditis in a patient with a lung adenocarcinoma after the third dose of modern COVID-19 vaccine. A case report and literature review. Curr. Probl. Cancer 2022, 6, 100153. [Google Scholar] [CrossRef]
- Choi, S.; Lee, S.; Seo, J.-W.; Kim, M.-J.; Jeon, Y.H.; Park, J.H.; Lee, J.K.; Yeo, N.S. Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med. Sci. 2021, 36, e286. [Google Scholar] [CrossRef]
- Cui, G.; Li, R.; Zhao, C.; Wang, D.W. Case Report: COVID-19 Vaccination Associated Fulminant Myocarditis. Front. Cardiovasc. Med. 2022, 8, 769616. [Google Scholar] [CrossRef]
- Hoshino, N.; Yanase, M.; Ichiyasu, T.; Kuwahara, K.; Kawai, H.; Muramatsu, T.; Ishii, H.; Tsukamoto, T.; Morimoto, S.-I.; Izawa, H. An autopsy case report of fulminant myocarditis: Following mRNA COVID-19 vaccination. J. Cardiol. Cases 2022, 26, 391–394. [Google Scholar] [CrossRef]
- Kadwalwala, M.; Chadha, B.; Ortoleva, J.; Joyce, M. Multimodality imaging and histopathology in a young man presenting with fulminant lymphocytic myocarditis and cardiogenic shock after mRNA-1273 vaccination. BMJ Case Rep. 2021, 14, e246059. [Google Scholar] [CrossRef]
- Kawano, H.; Motokawa, T.; Kurohama, H.; Okano, S.; Akashi, R.; Yonekura, T.; Ikeda, S.; Izumikawa, K.; Maemura, K. Fulminant Myocarditis 24 Days after Coronavirus Disease Messenger Ribonucleic Acid Vaccination: A Case Report. Intern. Med. 2022, 61, 2319–2325. [Google Scholar] [CrossRef]
- Kazama, S.; Okumura, T.; Kimura, Y.; Ito, R.; Araki, T.; Mizutani, T.; Oishi, H.; Kuwayama, T.; Hiraiwa, H.; Kondo, T.; et al. Biopsy-Proven Fulminant Myocarditis Requiring Mechanical Circulatory Support Following COVID-19 mRNA Vaccination. CJC Open 2022, 4, 501–505. [Google Scholar] [CrossRef]
- Kim, D.; Choi, J.H.; Jang, J.Y.; So, O.; Cho, E.; Choi, H.; Hong, K.S.; Park, K.T. A Case Report for Myopericarditis after BNT162b2 COVID-19 mRNA Vaccination in a Korean Young Male. J. Korean Med. Sci. 2021, 36, e277. [Google Scholar] [CrossRef]
- Kimura, M.; Hashimoto, T.; Noda, E.; Ishikawa, Y.; Ishikita, A.; Fujino, T.; Matsushima, S.; Ide, T.; Kinugawa, S.; Nagaoka, K.; et al. Fulminant necrotizing eosinophilic myocarditis after COVID-19 vaccination survived with mechanical circulatory support. ESC Hearth Fail. 2022, 9, 2732–2737. [Google Scholar] [CrossRef]
- Koiwaya, H.; Nishihira, K.; Tomozoe, K.; Shibata, Y. Serial histopathologic assessment of fulminant myocarditis after the first mRNA COVID-19 vaccine dose. Eur. Hearth J. 2022, 43, 1995. [Google Scholar] [CrossRef]
- Lim, Y.; Kim, M.C.; Kim, K.H.; Jeong, I.-S.; Cho, Y.S.; Choi, Y.D.; Lee, J.E. Case Report: Acute Fulminant Myocarditis and Cardiogenic Shock After Messenger RNA Coronavirus Disease 2019 Vaccination Requiring Extracorporeal Cardiopulmonary Resuscitation. Front. Cardiovasc. Med. 2021, 8, 758996. [Google Scholar] [CrossRef]
- Nassar, M.; Nso, N.; Gonzalez, C.; Lakhdar, S.; Alshamam, M.; Elshafey, M.; Abdalazeem, Y.; Nyein, A.; Punzalan, B.; Durrance, R.J.; et al. COVID-19 vaccine-induced myocarditis case report with literature review. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102205. [Google Scholar] [CrossRef] [PubMed]
- Oka, A.; Sudo, Y.; Miyoshi, T.; Ozaki, M.; Kimura, Y.; Takagi, W.; Ugawa, S.; Okada, T.; Nosaka, K.; Doi, M. Fulminant myocarditis after the second dose of COVID-19 mRNA vaccination. Clin. Case Rep. 2022, 10, e05378. [Google Scholar] [CrossRef] [PubMed]
- Olmos, C.V.; Trahan, S.; Rochon, A.; Ducharme, A. Severe myocarditis after SARS-CoV-2 vaccination in a 49-year-old woman. CMAJ 2022, 194, E581–E584. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.G.; Sobieszczyk, P.S.; Bhatt, D.L. Acute Myocardial Infarction within 24 Hours After COVID-19 Vaccination. Am. J. Cardiol. 2021, 156, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Ujueta, F.; Azimi, R.; Lozier, M.R.; Poppiti, R.; Ciment, A. Lymphohistocytic myocarditis after Ad26.COV2.S viral vector COVID-19 vaccination. IJC Hearth Vasc. 2021, 36, 100869. [Google Scholar] [CrossRef]
- Verma, A.K.; Lavine, K.J.; Lin, C.-Y. Myocarditis after Covid-19 mRNA Vaccination. N. Engl. J. Med. 2021, 385, 1332–1334. [Google Scholar] [CrossRef]
- Wu, L.; Baylan, U.; van der Leeden, B.; Schurink, B.; Roos, E.; Schalkwijk, C.G.; Bugiani, M.; van der Valk, P.; van Rossum, A.C.; Zeerleder, S.S.; et al. Cardiac inflammation and microvascular procoagulant changes are decreased in second wave compared to first wave deceased COVID-19 patients. Int. J. Cardiol. 2021, 349, 157–165. [Google Scholar] [CrossRef]
- Yamamoto, M.; Tajiri, K.; Ayuzawa, S.; Ieda, M. Pathological findings of clinically suspected myocarditis temporally associated with COVID -19 vaccination. Eur. J. Hearth Fail. 2022, 24, 1132–1138. [Google Scholar] [CrossRef]
- Naveed, Z.; Li, J.; Spencer, M.; Wilton, J.; Naus, M.; García, H.A.V.; Otterstatter, M.; Janjua, N.Z. Observed versus expected rates of myocarditis after SARS-CoV-2 vaccination: A population-based cohort study. CMAJ 2022, 194, E1529–E1536. [Google Scholar] [CrossRef]
- Roh, D.-E.; Na, H.; Kwon, J.-E.; Choi, I.; Kim, Y.-H.; Cho, H.-J. Chest Pain and Suspected Myocarditis Related to COVID-19 Vaccination in Adolescents—A Case Series. Children 2022, 9, 693. [Google Scholar] [CrossRef]
- Park, H.; Yun, K.W.; Kim, K.-R.; Song, S.H.; Ahn, B.; Kim, D.R.; Kim, G.B.; Huh, J.; Choi, E.H.; Kim, Y.-J. Epidemiology and Clinical Features of Myocarditis/Pericarditis before the Introduction of mRNA COVID-19 Vaccine in Korean Children: A Multicenter Study. J. Korean Med Sci. 2021, 36, e232. [Google Scholar] [CrossRef]
- Lane, S.; Yeomans, A.; Shakir, S. Reports of myocarditis and pericarditis following mRNA COVID-19 vaccination: A systematic review of spontaneously reported data from the UK, Europe and the USA and of the scientific literature. BMJ Open 2022, 12, e059223. [Google Scholar] [CrossRef]
- Tuvali, O.; Tshori, S.; Derazne, E.; Hannuna, R.R.; Afek, A.; Haberman, D.; Sella, G.; George, J. The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. J. Clin. Med. 2022, 11, 2219. [Google Scholar] [CrossRef]
- Turner, A.J.; Hiscox, J.A.; Hooper, N.M. ACE2, from vasopeptidase to SARS virus receptor. Trends Pharmacol. Sci. 2004, 25, 291–294. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Dolhnikoff, M.; Ferreira Ferranti, J.; de Almeida Monteiro, R.A.; Duarte-Neto, A.N.; Soares Gomes-Gouvêa, M.; Viu Degaspare, N. SARS-CoV-2 in cardiac tissue of a child with COVID-19-related multisystem inflammatory syndrome. Lancet Child Adolesc. Health 2020, 4, 790–794. [Google Scholar] [CrossRef]
- Kim, D.; Quinn, J.; Pinsky, B.; Shah, N.H.; Brown, I. Rates of Co-infection Between SARS-CoV-2 and Other Respiratory Pathogens. JAMA 2020, 323, 2085–2086. [Google Scholar] [CrossRef] [Green Version]
- Jone, P.N.; John, A.; Oster, M.E.; Allen, K.; Tremoulet, A.H.; Saarel, E.V.; Lambert, L.M.; Miyamoto, S.D.; De Ferranti, S.D. American Heart Association Leadership Committee and Congenital Cardiac Defects Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young. SARS-CoV-2 Infection and Associated Cardiovascular Manifestations and Complications in Children and Young Adults: A Scientific Statement from the American Heart Association. Circulation 2022, 145, e1037–e1052. [Google Scholar]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: Clinical observations and potential mechanisms. Nat. Rev. Cardiol. 2021, 19, 75–77. [Google Scholar] [CrossRef]
- Bansal, S.; Perincheri, S.; Fleming, T.; Poulson, C.; Tiffany, B.; Bremner, R.M.; Mohanakumar, T. Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines. J. Immunol. 2021, 207, 2405–2410. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Country | Age, Years | Sex (M = 1; F = 2) | Vasoactive Agents (Yes = 1; No or not Reported = 2) | Intra-Aortic Balloon Pump (Yes = 1; No = 2) | Impella (Yes = 1; No = 2) | ECMO (Yes = 1; No = 2) | Survival to Discharge (Yes = 1; No = 2) | Treatment | Biopsy/Infiltrate |
|---|---|---|---|---|---|---|---|---|---|---|
| Afriyie [7] | USA | 27 | 1 | 1 | 2 | Remdesivir, Steroids | ||||
| Albert [4] | USA | 49 | 1 | 2 | 1 | 1 | Tocilizumab, Steroids, IVIG | Lymphocytes | ||
| Aldeghaither [8] | Canada | 39 | 2 | 1 | 1 | 1 | Steroids | Eosinophils | ||
| Aldeghaither [8] | Canada | 25 | 1 | 1 | 2 | 1 | Steroids, IVIG, Anakinra (IL-antagonist) | Eosinophils | ||
| Aldeghaither [8] | Canada | 21 | 1 | 1 | 1 | 1 | Steroids, Anakinra, IVIG | Lymphocytes | ||
| Almanza [9] | Colombia | 75 | 2 | 1 | 2 | Tocilizumab | Lymphocytes | |||
| Anupama [10] | USA | 66 | 1 | 1 | 1 | Hydroxy-chloroquine, IV diuretics, IVIG, convalescent plasma | ||||
| Bergman [11] | USA | 53 | 1 | 1 | 1 | 1 | Hydroxy-chloroquine, Sarilumab (IL-6 inhibitor) | |||
| Bernal-Torres [12] | Colombia | 38 | 2 | 1 | 1 | Steroids, IVIG, Hydroxy-chloroquine, Lopinavir/Ritonavir | ||||
| Bhardwaj [13] | USA | 22 | 1 | 2 | 1 | 1 | Steroids, Remdesivir | |||
| Bhardwaj [13] | USA | 53 | 2 | 2 | 1 | 1 | Steroids, Remdesivir, Convalescent Plasma | |||
| Bhardwaj [13] | USA | 28 | 2 | 2 | 1 | 2 | Steroids, Remdesivir, Tocilizumab, IVIG | |||
| Bhardwaj [13] | USA | 27 | 2 | 2 | 1 | 1 | Steroids, Remdesivir, IVIG | |||
| Bhardwaj [13] | USA | 46 | 1 | 2 | 1 | 1 | Steroids, Remdesivir, IVIG | |||
| Bhardwaj [13] | USA | 68 | 1 | 2 | 1 | 2 | Steroids | |||
| Bhardwaj [13] | USA | 26 | 2 | 2 | 1 | 1 | Steroids | |||
| Bhardwaj [13] | USA | 66 | 1 | 2 | 1 | 1 | Steroids | |||
| Bhardwaj [13] | USA | 24 | 1 | 2 | 1 | 1 | Steroids | |||
| Bulbul [14] | Qatar | 49 | 2 | 1 | 1 | 1 | Hydroxy-chloroquine, Oseltamivir, Teicoplanin, Steroids, Tocilizumab, Lopinavir, Ritonavir | |||
| Chitturi [15] | USA | 65 | 2 | 1 | 2 | 1 | Remdesivir, Steroids, Tocilizumab | |||
| Coll [16] | USA | 39 | 1 | 1 | 2 | 2 | 2 | 1 | Steroids, IVIG | |
| Coyle [17] | USA | 57 | 1 | 1 | 1 | Hydroxy-chloroquine, Steroids, Colchicine, Tocilizumab | ||||
| Craver [18] | USA | 18 | 1 | 2 | 2 | Eosinophils | ||||
| Fiore [19] | Italy | 45 | 1 | 1 | 1 | 2 | 2 | 1 | Hydroxy-chloroquine, Anakinra, | Lymphocytes |
| Fried [20] | USA | 38 | 1 | 1 | 1 | Hydroxy-chloroquine | ||||
| Fried [20] | USA | 64 | 2 | 1 | 2 | |||||
| Garau [21] | Belgium | 18 | 2 | 1 | 1 | 1 | 1 | Steroids, Hydroxy-chloroquine, IVIG | Lymphocytes | |
| Garot [22] | France | 18 | 1 | 1 | 1 | Hydroxy-chloroquine | ||||
| Gauchotte [23] | France | 69 | 1 | 1 | 1 | 2 | Lymphocytes | |||
| Gaudriot [24] | France | 38 | 1 | 1 | 1 | 2 | 1 | 1 | Steroids, Mycophenolate Mofetil, Cyclosporine | Lymphocytes |
| Gay [25] | USA | 56 | 1 | 1 | 2 | 1 | 1 | Steroids, Tocilizumab | ||
| Ghafoor [26] | USA | 54 | 2 | 1 | 2 | 2 | 1 | 2 | ||
| Gill [27] | USA | 65 | 2 | 1 | 1 | 2 | 2 | |||
| Gill [27] | USA | 34 | 2 | 2 | 1 | 1 | Colchicine, Steroids | |||
| Gomez [28] | Spain | 53 | 1 | 1 | 2 | |||||
| Hamdan [29] | UAE | 45 | 2 | 1 | 1 | 1 | Steroids | |||
| Hu [30] | China | 37 | 1 | 1 | 1 | Steroids, IVIG. | ||||
| Hussain [31] | USA | 51 | 1 | 1 | Hydroxy-chloroquine, Azithromycin, Colchicine, Steroids, Remdesivir | |||||
| Irabien-Ortiz [32] | Spain | 59 | 2 | 1 | 1 | 1 | Lopinavir/Ritonavir, IVIG, Steroids | |||
| Ishikura [33] | Japan | 35 | 1 | 1 | 1 | 1 | 1 | IVIG, Steroids | Lymphocytes | |
| Jacobs [34] | Belgium | 48 | 1 | 1 | 1 | 2 | Hydroxy-chloroquine | Lymphocytes | ||
| Kallel [35] | Morocco | 26 | 1 | 1 | 2 | 2 | 2 | 1 | ||
| Khatri [36] | USA | 50 | 1 | 1 | 2 | 2 | Hydroxy-chloroquine, IVIG, Steroids | |||
| Li [37] | USA | 60 | 1 | 1 | 1 | Hydroxy-chloroquine, Steroids, IVIG | ||||
| Mansoor [38] | USA | 72 | 2 | 1 | 2 | Chloroquine, IVIG, Steroids | ||||
| Menter [39] | Switzer-land | 47 | 2 | 1 | 2 | 2 | 2 | 2 | Lymphocytes, Neutrophils | |
| Milla-Godoy [40] | USA | 45 | 2 | 1 | 2 | Hydroxy-chloroquine | ||||
| Nakatani [41] | Japan | 49 | 1 | 1 | 2 | IVIG, Steroids | Lymphocytes | |||
| Naneishvili [42] | UK | 44 | 2 | 1 | 1 | Steroids | ||||
| Nwaejike [43] | UK | 39 | 1 | 1 | 1 | 1 | ||||
| Okor [44] | USA | 72 | 2 | 1 | 2 | 2 | 2 | 2 | Steroids | |
| Othenin-Girard [45] | Switzer-land | 22 | 1 | 2 | 1 | 1 | Steroids, Tocilizumab, IVIG, Cyclo-phosphamide, Rituximab | Lymphocytes | ||
| Papageorgiou [46] | Sweden | 43 | 1 | 1 | 1 | 1 | Steroids, Colchicine | None | ||
| Purdy [47] | USA | 53 | 1 | 1 | 1 | Steroids, Hydroxy-chloroquine | ||||
| Rajpal [48] | USA | 60 | 2 | 1 | 1 | 1 | Steroids | Lymphocytes | ||
| Richard [49] | USA | 28 | 2 | 1 | 1 | 1 | Steroids | |||
| Ruiz [50] | USA | 35 | 2 | 2 | 1 | 1 | IVIG, Remdesivir, Steroids | |||
| Salamanca [51] | Spain | 44 | 1 | 1 | 1 | 1 | Steroids, Tocilizumab, Hydroxy-chloroquine, Lopinavir/Ritonavir | Lymphocytes | ||
| Sampaio [52] | Brazil | 45 | 2 | 1 | 1 | 1 | Tocilizumab, IVIG, Convalescent Plasma, Steroids | |||
| Sanchez [53] | Spain | 42 | 2 | 2 | 1 | 1 | 2 | |||
| Shah [54] | Qatar | 19 | 1 | 1 | Steroids, Hydroxy-chloroquine, Tocilizumab, IVIG | |||||
| Shahrami [55] | Iran | 78 | 1 | 1 | 2 | Steroids, IVIG, Hydroxy-chloroquine | ||||
| Shen [56] | USA | 43 | 1 | 1 | 1 | 2 | 2 | 1 | IVIG | |
| Tavazzi [57] | Italy | 69 | 1 | 1 | 1 | 1 | 2 | Lopinavir/Ritonavir, Hydroxy-chloroquine, Steroids | Lymphocytes | |
| Thaker [58] | USA | 42 | 2 | 2 | 1 | 2 | 2 | 1 | Tocilizumab | |
| Thaker [58] | USA | 42 | 2 | 2 | 1 | Steroids, Tocilizumab, IVIG | ||||
| Thomson [59] | Australia | 39 | 2 | 1 | 1 | 2 | Steroids, IVIG | Macrophages | ||
| Trpkov [60] | Canada | 62 | 2 | 2 | 1 | Steroids, Anakinra | ||||
| Verma [61] | USA | 48 | 2 | 2 | 1 | 1 | 1 | Steroids, IVIG, Remdesivir, Tocilizumab | Macrophages | |
| Veronese [62] | Italy | 51 | 2 | 2 | 1 | 1 | 1 | Steroids | Lymphocytes | |
| Yalcinkaya [63] | Turkey | 29 | 1 | 1 | Eosinophils | |||||
| Yeleti [64] | USA | 25 | 2 | 2 | 2 | 1 | 1 | Steroids Remdesivir, Convalescent Plasma | Lymphocytes | |
| Zeng [65] | China | 63 | 1 | 2 | 2 | Antiviral |
| Authors | Country | Age, Years | Sex (M = 1; F = 2) | Type of Vaccine (Pfizer =1; Moderna = 2; Vero Cell =3; AstraZeneca = 4; Janssen = 5) | Dose to Symptoms (Days) | Number of Doses | Vasoactive Agents (Yes = 1; No or not Reported = 2) | Intra-Aortic Balloon Pump (Yes = 1; No = 2) | Impella (Yes = 1; No = 2) | ECMO (Yes = 1; No = 2) | Survival to Discharge (Yes = 1; No = 2) | Treatment | Biopsy/ Infiltrate |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abbate [66] | USA | 27 | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | Steroids | |
| Abbate [66] | USA | 34 | 2 | 1 | 9 | 1 | 1 | 2 | 2 | 1 | 1 | Steroids | Lymphocytes |
| Agdamag [67] | USA | 80 | 2 | 1 | 7 | 1 | 1 | 2 | 1 | 2 | 1 | Steroids | Eosinophils |
| Ameratunga [68] | New Zealand | 57 | 2 | 1 | 1 | 1 | 2 | 2 | Eosinophils | ||||
| Araki [69] | Japan | 53 | 2 | 1 | 4 | 2 | 1 | 1 | 1 | 1 | 1 | Steroids | None |
| Brage [70] | Spain | 62 | 2 | 2 | 1 | 3 | 1 | 2 | 1 | 2 | 1 | Steroids | |
| Choi [71] | Korea | 22 | 1 | 1 | 5 | 1 | 2 | 2 | 2 | 2 | 2 | Neutrophils, Histiocytes | |
| Cui [72] | China | 57 | 2 | 3 | 4 | 1 | 1 | 2 | 2 | 1 | Steroids | Lymphocytes | |
| Cui [72] | China | 63 | 1 | 3 | 4 | 1 | 2 | 1 | 2 | 2 | 1 | Steroids | Lymphocytes |
| Hoshino [73] | Japan | 27 | 1 | 2 | 8 | 1 | 1 | 1 | 1 | 2 | Steroids, IVIG | Lymphocytes | |
| Kadwalwala [74] | USA | 38 | 1 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | Steroids | Lymphocytes |
| Kawano [75] | Japan | 60 | 2 | 1 | 24 | 2 | 1 | 2 | 1 | 1 | 1 | Steroids | Lymphocytes |
| Kazama [76] | Japan | 48 | 2 | 2 | 7 | 2 | 1 | 1 | 1 | 1 | 1 | Lymphocytes | |
| Kim [77] | Korea | 63 | 2 | 4 | 1 | 1 | 2 | 2 | 2 | 1 | 2 | Lymphocytes | |
| Kimura [78] | Japan | 69 | 1 | 1 | 7 | 1 | 1 | 1 | 1 | 1 | 1 | Steroids | Lymphocytes, Eosinophils |
| Koiwaya [79] | Japan | 77 | 1 | 1 | 8 | 1 | 2 | 1 | 2 | 1 | 1 | Lymphocytes | |
| Lim [80] | South Korea | 38 | 2 | 1 | 7 | 2 | 2 | 1 | 1 | Lymphocytes | |||
| Nassar [81] | USA | 70 | 2 | 5 | 2 | 1 | 2 | 2 | 2 | 2 | |||
| Oka [82] | Japan | 50 | 1 | 1 | 10 | 2 | 1 | 2 | 2 | 2 | 1 | Steroids | Lymphocytes |
| Olmos [83] | Canada | 49 | 2 | 1 | 6 | 2 | 1 | 1 | 1 | Steroids | Lymphocytes, Eosinophils | ||
| Sung [84] | USA | 63 | 1 | 1 | 7 | 2 | 1 | 1 | 1 | Steroids | Giant cells | ||
| Ujieta [85] | USA | 62 | 2 | 5 | 4 | 1 | 2 | Steroids | Lymphocytes | ||||
| Verma [86] | USA | 45 | 2 | 1 | 10 | 1 | 1 | 2 | 2 | 2 | 1 | Lymphocytes, Eosinophils | |
| Verma [86] | USA | 42 | 1 | 2 | 14 | 2 | 2 | 2 | Lymphocytes, Eosinophils | ||||
| Wu [87] | Taiwan | 44 | 2 | 4 | 2 | 1 | 2 | 2 | 2 | 1 | |||
| Yamamoto [88] | Japan | 41 | 1 | 2 | 19 | 2 | 2 | 1 | 1 | 1 | Steroids | Lymphocytes | |
| Yamamoto [88] | Japan | 18 | 2 | 1 | 9 | 1 | 2 | 1 | 2 | 2 | 1 | Steroids | Lymphocytes |
| COVID-19 Fulminant Myocarditis | COVID-19 Vaccine Fulminant Myocarditis | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Continuous Variables | |||||||
| n | Mean | SD | n | Mean | SD | p-Value | |
| Heart rate, beats per minute | 29 | 125.1 | 21.9 | 18 | 106.8 | 30.7 | 0.0211 |
| Diastolic blood pressure, mmHg | 28 | 54.6 | 14.8 | 17 | 62.9 | 12.7 | 0.0312 |
| Mean arterial pressure, mmHg | 33 | 62.1 | 17.0 | 18 | 69.7 | 17.6 | 0.0497 |
| BNP, pg/dL | 16 | 11,468.3 | 18,237.7 | 9 | 947.0 | 614.8 | 0.0558 |
| Age | 73 | 45.1 | 15.8 | 27 | 50.3 | 16.4 | 0.1490 |
| Systolic blood pressure, mmHg | 30 | 86.7 | 18.8 | 18 | 90.2 | 17.0 | 0.5287 |
| White blood cells, peak | 33 | 19.2 | 9.8 | 12 | 14.3 | 10.2 | 0.1457 |
| Lactate | 33 | 7.3 | 4.2 | 8 | 9.6 | 8.4 | 0.7174 |
| C-reactive protein | 55 | 94.2 | 350.8 | 14 | 33.6 | 68.1 | 0.0552 |
| Peak troponin I | 20 | 5.7 × 108 | 2.5 × 109 | 13 | 6.4 × 108 | 2.3 × 109 | 0.5311 |
| LVEF at admission | 63 | 19.3 | 8.9 | 24 | 20.8 | 9.7 | 0.5513 |
| Length of stay total | 41 | 26.9 | 20.0 | 15 | 27.1 | 25.4 | 0.5661 |
| Categorical variables | |||||||
| n | Yes | No | n | Yes | No | ||
| Fever | 48 | 38 | 10 | 26 | 14 | 12 | 0.0229 |
| Shortness of breath | 42 | 35 | 7 | 24 | 10 | 14 | 0.0005 |
| Pulmonary infiltrates on chest X-ray | 73 | 34 | 39 | 27 | 5 | 22 | 0.0117 |
| General symptoms | 73 | 10 | 63 | 27 | 13 | 14 | 0.0008 |
| Cardiac arrest | 22 | 18 | 4 | 23 | 7 | 16 | 0.0008 |
| VA-ECMO | 49 | 38 | 11 | 23 | 12 | 11 | 0.0293 |
| Gender | 73 | 40 (M) | 33 (F) | 27 | 11 (M) | 16 (F) | 0.2120 |
| Intubation | 73 | 30 | 43 | 27 | 9 | 18 | 0.4798 |
| Right ventricular dysfunction | 73 | 26 | 47 | 27 | 3 | 24 | 0.0165 |
| Chest pain | 73 | 10 | 63 | 27 | 11 | 16 | 0.0032 |
| Pericardial effusion | 73 | 15 | 58 | 27 | 12 | 15 | 0.0169 |
| Intra-aortic balloon pump | 73 | 12 | 61 | 27 | 8 | 19 | 0.1432 |
| Survival | 73 | 44 | 29 | 27 | 19 | 8 | 0.3532 |
| Gastrointestinal symptoms | 73 | 16 | 57 | 27 | 4 | 23 | 0.4305 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guglin, M.E.; Etuk, A.; Shah, C.; Ilonze, O.J. Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review. J. Clin. Med. 2023, 12, 1849. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051849
Guglin ME, Etuk A, Shah C, Ilonze OJ. Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review. Journal of Clinical Medicine. 2023; 12(5):1849. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051849
Chicago/Turabian StyleGuglin, Maya E., Aniekeme Etuk, Chirag Shah, and Onyedika J. Ilonze. 2023. "Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review" Journal of Clinical Medicine 12, no. 5: 1849. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051849