
Effects of Melatonin Administration on Post-Stroke Delirium in Patients with Intracerebral Hemorrhage
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Regulations
2.2. Study Population
2.3. Participants’ Exclusion Criteria
2.4. Melatonin Administration
2.5. Data Collection
2.6. Study Endpoints
2.7. Statistical Analysis
3. Results
3.1. Participants’ Characteristics and Post-ICH PSD Prevalence
3.2. Effect of Melatonin Administration on PSD Prevention
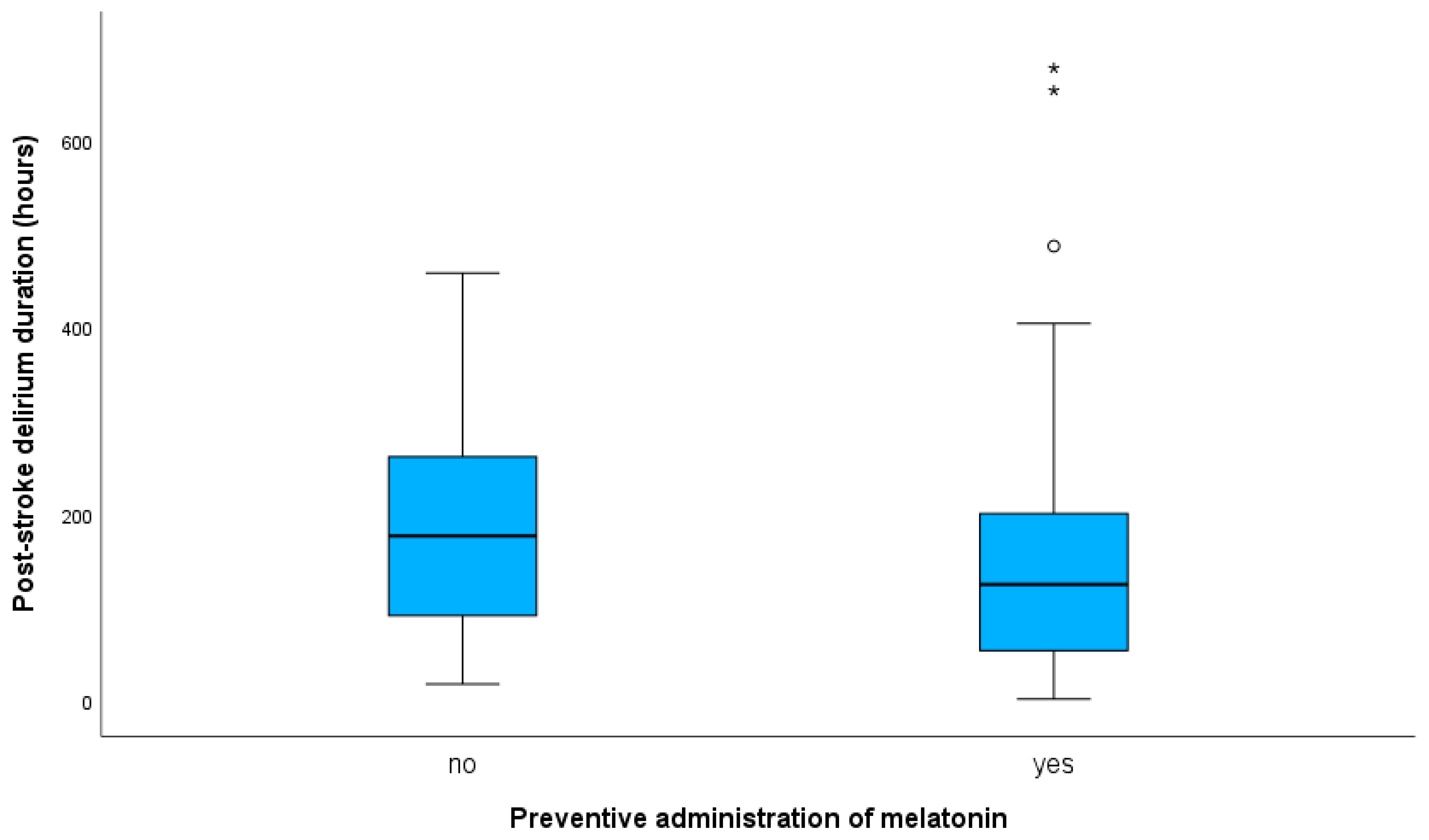
3.2.1. Effect of Melatonin Administration on PSD Duration
3.2.2. Effect of Melatonin Administration on SU-Stay Duration
Post-ICH PSD Patients
Post-ICH without PSD Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bosselmann, C.; Zurloh, J.; Stefanou, M.I.; Stadler, V.; Weber, Y.; Lerche, H.; Poli, S.; Ziemann, U.; Mengel, A. Delirium Screening in Aphasic Patients with the Intensive Care Delirium Screening Checklist (ICDSC): A Prospective Cohort Study. Front. Neurol. 2019, 10, 1198. [Google Scholar] [CrossRef] [PubMed]
- Naidech, A.M.; Beaumont, J.L.; Rosenberg, N.F.; Maas, M.B.; Kosteva, A.R.; Ault, M.L.; Cella, D.; Ely, E.W. Intracerebral hemorrhage and delirium symptoms. Length of stay, function, and quality of life in a 114-patient cohort. Am. J. Respir. Crit. Care Med. 2013, 188, 1331–1337. [Google Scholar] [CrossRef] [Green Version]
- Siokas, V.; Fleischmann, R.; Feil, K.; Liampas, I.; Kowarik, M.C.; Bai, Y.; Stefanou, M.I.; Poli, S.; Ziemann, U.; Dardiotis, E.; et al. The Role of Vascular Risk Factors in Post-Stroke Delirium: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5835. [Google Scholar] [CrossRef]
- Alvarez-Perez, F.J.; Paiva, F. Prevalence and Risk Factors for Delirium in Acute Stroke Patients. A Retrospective 5-Years Clinical Series. J. Stroke Cereb. Dis. 2017, 26, 567–573. [Google Scholar] [CrossRef]
- Pasinska, P.; Kowalska, K.; Klimiec, E.; Szyper-Maciejowska, A.; Wilk, A.; Klimkowicz-Mrowiec, A. Frequency and predictors of post-stroke delirium in PRospective Observational POLIsh Study (PROPOLIS). J. Neurol. 2018, 265, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Marrama, F.; Kyheng, M.; Pasi, M.; Pierre Rutgers, M.; Moulin, S.; Diomedi, M.; Leys, D.; Cordonnier, C.; Hénon, H.; Casolla, B. Early-onset delirium after spontaneous intracerebral hemorrhage. Int. J. Stroke 2021, 98, 17474930211059636. [Google Scholar] [CrossRef]
- Reznik, M.E.; Margolis, S.A.; Mahta, A.; Wendell, L.C.; Thompson, B.B.; Stretz, C.; Rudolph, J.L.; Boukrina, O.; Barrett, A.M.; Daiello, L.A.; et al. Impact of Delirium on Outcomes after Intracerebral Hemorrhage. Stroke 2022, 53, 505–513. [Google Scholar] [CrossRef]
- Sauvigny, T.; Mohme, M.; Grensemann, J.; Dührsen, L.; Regelsberger, J.; Kluge, S.; Schmidt, N.O.; Westphal, M.; Czorlich, P. Rate and risk factors for a hyperactivity delirium in patients with aneurysmal subarachnoid haemorrhage. Neurosurg. Rev. 2019, 42, 481–488. [Google Scholar] [CrossRef]
- Reimann, F.; Rinner, T.; Lindner, A.; Kofler, M.; Ianosi, B.A.; Schiefecker, A.J.; Beer, R.; Schmutzhard, E.; Pfausler, B.; Helbok, R.; et al. Hyperactive delirium in patients after non-traumatic subarachnoid hemorrhage. J. Crit. Care 2021, 64, 45–52. [Google Scholar] [CrossRef]
- Fleischmann, R.; Warwas, S.; Andrasch, T.; Kunz, R.; Witt, C.; Mengel, A.; von Sarnowski, B. Course and Recognition of Poststroke Delirium: A Prospective Noninferiority Trial of Delirium Screening Tools. Stroke 2021, 52, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Dostović, Z.; Smajlović, D.; Sinanović, O.; Vidović, M. Duration of delirium in the acute stage of stroke. Acta Clin. Croat. 2009, 48, 13–17. [Google Scholar] [PubMed]
- van Gool, W.A.; van de Beek, D.; Eikelenboom, P. Systemic infection and delirium: When cytokines and acetylcholine collide. Lancet 2010, 375, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Maclullich, A.M.; Ferguson, K.J.; Miller, T.; de Rooij, S.E.; Cunningham, C. Unravelling the pathophysiology of delirium: A focus on the role of aberrant stress responses. J. Psychosom. Res. 2008, 65, 229–238. [Google Scholar] [CrossRef] [Green Version]
- van Munster, B.C.; de Rooij, S.E.; Korevaar, J.C. The role of genetics in delirium in the elderly patient. Dement. Geriatr. Cogn. Disord. 2009, 28, 187–195. [Google Scholar] [CrossRef]
- Mansutti, I.; Saiani, L.; Palese, A. Delirium in patients with ischaemic and haemorrhagic stroke: Findings from a scoping review. Eur. J. Cardiovasc. Nurs. 2019, 18, 435–448. [Google Scholar] [CrossRef]
- Pohanka, M. New Uses of Melatonin as a Drug; A Review. Curr. Med. Chem. 2022, 29, 3622–3637. [Google Scholar] [CrossRef] [PubMed]
- Zisapel, N. New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation. Br. J. Pharm. 2018, 175, 3190–3199. [Google Scholar] [CrossRef] [Green Version]
- Daou, M.; Telias, I.; Younes, M.; Brochard, L.; Wilcox, M.E. Abnormal Sleep, Circadian Rhythm Disruption, and Delirium in the ICU: Are They Related? Front. Neurol. 2020, 11, 549908. [Google Scholar] [CrossRef]
- Sheng, A.Z.; Shen, Q.; Cordato, D.; Zhang, Y.Y.; Yin Chan, D.K. Delirium within three days of stroke in a cohort of elderly patients. J. Am. Geriatr. Soc. 2006, 54, 1192–1198. [Google Scholar] [CrossRef]
- Shigeta, H.; Yasui, A.; Nimura, Y.; Machida, N.; Kageyama, M.; Miura, M.; Menjo, M.; Ikeda, K. Postoperative delirium and melatonin levels in elderly patients. Am. J. Surg. 2001, 182, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Balan, S.; Leibovitz, A.; Zila, S.O.; Ruth, M.; Chana, W.; Yassica, B.; Rahel, B.; Richard, G.; Neumann, E.; Blagman, B.; et al. The relation between the clinical subtypes of delirium and the urinary level of 6-SMT. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 363–366. [Google Scholar] [CrossRef]
- Walker, C.K.; Gales, M.A. Melatonin Receptor Agonists for Delirium Prevention. Ann. Pharm. 2017, 51, 72–78. [Google Scholar] [CrossRef]
- Ford, A.H.; Flicker, L.; Kelly, R.; Patel, H.; Passage, J.; Wibrow, B.; Anstey, M.; Edwards, M.; Almeida, O.P. The Healthy Heart-Mind Trial: Randomized Controlled Trial of Melatonin for Prevention of Delirium. J. Am. Geriatr. Soc. 2020, 68, 112–119. [Google Scholar] [CrossRef]
- Mengel, A.; Zurloh, J.; Boßelmann, C.; Brendel, B.; Stadler, V.; Sartor-Pfeiffer, J.; Meisel, A.; Fleischmann, R.; Ziemann, U.; Poli, S.; et al. Delirium REduction after administration of melatonin in acute ischemic stroke (DREAMS): A propensity score-matched analysis. Eur. J. Neurol. 2021, 28, 1958–1966. [Google Scholar] [CrossRef]
- Dianatkhah, M.; Najafi, A.; Sharifzadeh, M.; Ahmadi, A.; Sharifnia, H.; Mojtahedzadeh, M.; Najmeddin, F.; Moghaddas, A. Melatonin Supplementation May Improve the Outcome of Patients with Hemorrhagic Stroke in the Intensive Care Unit. J. Res. Pharm. Pract. 2017, 6, 173–177. [Google Scholar] [CrossRef]
- Ohta, T.; Murao, K.; Miyake, K.; Takemoto, K. Melatonin receptor agonists for treating delirium in elderly patients with acute stroke. J. Stroke Cereb. Dis. 2013, 22, 1107–1110. [Google Scholar] [CrossRef]
- Hatta, K.; Kishi, Y.; Wada, K.; Takeuchi, T.; Odawara, T.; Usui, C.; Nakamura, H. Preventive effects of ramelteon on delirium: A randomized placebo-controlled trial. JAMA Psychiatry 2014, 71, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Pierce, M.; Linnebur, S.A.; Pearson, S.M.; Fixen, D.R. Optimal Melatonin Dose in Older Adults: A Clinical Review of the Literature. Sr. Care Pharm. 2019, 34, 419–431. [Google Scholar] [CrossRef]
- Bergeron, N.; Dubois, M.J.; Dumont, M.; Dial, S.; Skrobik, Y. Intensive Care Delirium Screening Checklist: Evaluation of a new screening tool. Intensive Care Med. 2001, 27, 859–864. [Google Scholar] [CrossRef]
- Smyrnis, N.; Theleritis, C.; Evdokimidis, I.; Muri, R.M.; Karandreas, N. Single-pulse transcranial magnetic stimulation of parietal and prefrontal areas in a memory delay arm pointing task. J. Neurophysiol. 2003, 89, 3344–3350. [Google Scholar] [CrossRef]
- Stuart, E.A.; Lee, B.K.; Leacy, F.P. Prognostic score-based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J. Clin. Epidemiol. 2013, 66, S84–S90.e81. [Google Scholar] [CrossRef]
- Rubin, D.B. Using Propensity Scores to Help Design Observational Studies: Application to the Tobacco Litigation. Health Serv. Outcomes Res. Methodol. 2001, 2, 169–188. [Google Scholar] [CrossRef]
- Makango, B.; Alemu, Z.A.; Solomon, T.; Lemma, N.; Girma, T.; Mohammednur, T.; Alayu, M.; Fufa, Y. Prevalence and factors associated with post-traumatic stress disorder among internally displaced people in camps at Debre Berhan, Amhara Region, Ethiopia: A cross-sectional study. BMC Psychiatry 2023, 23, 81. [Google Scholar] [CrossRef]
- Soltani, F.; Salari, A.; Javaherforooshzadeh, F.; Nassajjian, N.; Kalantari, F. The effect of melatonin on reduction in the need for sedative agents and duration of mechanical ventilation in traumatic intracranial hemorrhage patients: A randomized controlled trial. Eur. J. Trauma Emerg. Surg. 2022, 48, 545–551. [Google Scholar] [CrossRef]
- Rhee, J.Y.; Colman, M.A.; Mendu, M.; Shah, S.J.; Fox, M.D.; Rost, N.S.; Kimchi, E.Y. Associations between Stroke Localization and Delirium: A Systematic Review and Meta-Analysis. J. Stroke Cereb. Dis. 2022, 31, 106270. [Google Scholar] [CrossRef]
- Ostrowski, R.P.; Stępień, K.; Pucko, E.; Matyja, E. The efficacy of hyperbaric oxygen in hemorrhagic stroke: Experimental and clinical implications. Arch. Med. Sci. 2017, 13, 1217–1223. [Google Scholar] [CrossRef]
- Evensen, S.; Bourke, A.K.; Lydersen, S.; Sletvold, O.; Saltvedt, I.; Wyller, T.B.; Taraldsen, K. Motor activity across delirium motor subtypes in geriatric patients assessed using body-worn sensors: A Norwegian cross-sectional study. BMJ Open 2019, 9, e026401. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Patients’ Characteristics | All ICH Patients n = 339 | ICH Patients with PSD n = 127 | ICH Patients without PSD n = 212 | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age, y median, (IQR) | 74.00 (20.00) | 78.00 (16.00) | 71.50 (22.00) | 0.001 ^ |
| Sex, n (%) | 0.454 * | |||
| Male | 186 (54.9) | 73 (57.5) | 113 (53.3) | |
| Female | 153 (45.1) | 54 (42.5) | 99 (46.7) | |
| Risk Factors, n (%) | ||||
| HP | 268 (79.1) | 104 (81.9) | 164 (77.4) | 0.321 * |
| DM | 64 (18.9) | 27 (21.3) | 37 (17.5) | 0.386 * |
| HCL | 67 (19.8) | 28 (22.0) | 39 (18.4) | 0.414 * |
| AF | 94 (27.7) | 46 (36.2) | 48 (22.6) | 0.007 * |
| CAD | 60 (17.8) | 26 (20.5) | 34 (16.1) | 0.310 * |
| Obesity (BMI > 30) | 61 (18.0) | 22 (17.3) | 39 (18.4) | 0.803 * |
| Chronic renal failure | 38 (11.2) | 15 (11.8) | 23 (10.8) | 0.786 * |
| Chronic hepatic failure | 8 (2.4) | 2 (1.6) | 6 (2.8) | 0.461 * |
| Smoking | 46 (13.6) | 15 (11.8) | 31 (14.6) | 0.464 * |
| Alcohol | 27 (8.0) | 10 (7.9) | 17 (8.0) | 0.962 * |
| Malignancy | 36 (10.2) | 12 (9.4) | 24 (11.3) | 0.588 * |
| Depression | 21 (6.2) | 7 (5.5) | 14 (6.6) | 0.686 * |
| Cognition | 0.153 *# | |||
| Health | 301 (89.6) | 109 (86.5) | 192 (91.4) | |
| MCI | 31 (9.2) | 13 (10.3) | 18 (8.6) | |
| Dementia | 4 (1.2) | 4 (3.2) | 0 (0.0) | |
| Any kind of infection | 176 (51.9) | 85 (66.9) | 91 (42.9) | <0.001 * |
| Baseline clinical variables/scales | ||||
| NIHSS oa, median (IQR) | 7.00 (10.0) | 8.00 (9.00) | 6.00 (11.00) | 0.005 ^ |
| Aphasia oa, n (%) | 125 (37.4) | 53 (41.7) | 72 (34.8) | 0.203 * |
| ICH-score oa, median (IQR) | 1.00 (1.00) | 2.00 (1.00) | 1.00 (2.00) | <0.001 ^ |
| mRS before the ICH, median (IQR) | 0.00 (2.00) | 1.00 (2.00) | 0.00 (1.00) | 0.131 ^ |
| Etiology, n (%) | ||||
| Hypertension | 191 (56.3) | 82 (64.6) | 109 (51.4) | 0.018 * |
| CAA | 27 (8.0) | 12 (9.4) | 15 (7.1) | 0.435 * |
| Mass | 26 (7.7) | 8 (6.3) | 18 (8.5) | 0.463 |
| OAC | 92 (27.2) | 44 (34.6) | 48 (22.6) | 0.016 * |
| Vessel pathology | 20 (5.9) | 2 (1.6) | 18 (8.5) | 0.009 * |
| Other/unknown | 67 (19.8) | 21 (16.5) | 46 (21.7) | 0.248 * |
| Location at baseline, n (%) | ||||
| DWM | 157 (46.6) | 65 (51.2) | 92 (43.4) | 0.189 * |
| Lobar | 139 (41.0) | 46 (36.2) | 93 (43.9) | 0.166 * |
| Brainstem | 18 (5.3) | 4 (3.2) | 14 (6.6) | 0.172 * |
| Cerebellum | 41 (12.2) | 15 (11.8) | 26 (12.4) | 0.877 * |
| Left hemisphere | 182 (53.7) | 65 (51.2) | 117 (55.2) | 0.474 * |
| Right hemisphere | 174 (51.3) | 64 (50.4) | 110 (51.9) | 0.790 * |
| IVH oa | 5 (1.5) | 2 (1.6) | 3 (1.4) | 0.906 * |
| IVH extension | 139 (41.2) | 66 (52.4) | 73 (34.6) | 0.001 * |
| ICH Volume (cm3), median (IQR) | 11.00 (22.00) | 11.50 (23.00) | 10.50 (22.00) | 0.478 ^ |
| Invasive procedures n (%) | ||||
| Surgical evacuation | 49 (14.5) | 13 (10.2) | 36 (17.0) | 0.087 * |
| EVD | 49 (14.5) | 24 (18.9) | 25 (11.8) | 0.078 * |
| Patients’ Characteristics | Melatonin Treated n = 119 | Control Cohort n = 220 | p-Value 1 | PSM Control Cohort n = 118 | p-Value 2 | SMD 2 |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Age, y median, (IQR) | 76.00 (18.00) | 74.00 (21.00) | 0.059 | 74.50 (22.00) | 0.136 ^ | 0.014 |
| Sex, n (%) | 0.536 * | 0.597 * | 0.053 | |||
| Male | 68 (57.1) | 118 (53.6) | 71 (60.2) | |||
| Female | 51 (42.9) | 102 (46.4) | 47 (39.8) | |||
| Risk Factors, n (%) | ||||||
| HP | 101 (84.9) | 167 (75.9) | 0.053 * | 93 (78.8) | 0.238 * | 0.159 |
| DM | 19 (16.0) | 45 (20.5) | 0.314 * | 27 (22.9) | 0.189 * | 0.175 |
| HCL | 34 (28.1) | 33 (15.0) | 0.003 * | 24 (20.3) | 0.131 * | 0.116 |
| AF | 32 (26.9) | 62 (28.2) | 0.800 * | 38 (32.2) | 0.393 * | 0.183 |
| CAD | 26 (21.8) | 34 (15.5) | 0.146 * | 22 (18.8) | 0.539 * | 0.075 |
| Obesity (BMI > 30) | 20 (16.8) | 41 (18.6) | 0.676 * | 24 (20.3) | 0.504 * | 0.090 |
| Chronic renal failure | 15 (12.6) | 23 (10.5) | 0.549 * | 14 (11.9) | 0.843 * | 0.021 |
| Chronic hepatic failure | 2 (1.7) | 6 (2.7) | 0.545 * | 3 (2.5) | 0.651 * | 0.056 |
| Smoking | 14 (11.8) | 32 (14.5) | 0.475 * | 23 (19.5) | 0.107 * | 0.213 |
| Alcohol | 10 (8.4) | 17 (7.5) | 0.826 * | 10 (8.5) | 1.000 * | 0.004 |
| Malignancy | 13 (10.9) | 23 (10.5) | 0.893 * | 15 (12.7) | 0.687 * | 0.056 |
| Depression | 6 (5.0) | 15 (6.8) | 0.517 * | 7 (5.9) | 0.775 * | 0.040 |
| Cognition | 0.822 *# | 0.393 *# | 0.107 | |||
| Health | 106 (89.1) | 195 (89.9) | 107 (92.2) | |||
| MCI | 11 (9.2) | 20 (9.2) | 9 (7.8) | |||
| Dementia | 2 (1.7) | 2 (0.9) | 0 (0.0) | |||
| Any kind of infection | 55 (46.2) | 121 (55.0) | 0.122 * | 61 (51.7) | 0.436 * | 0.110 |
| Baseline clinical variables/scales | ||||||
| NIHSS oa, median (IQR) | 5.00 (8.0) | 9.00 (11.00) | <0.001 ^ | 6.00 (9.00) | 0.076 ^ | 0.029 |
| Aphasia oa, n (%) | 38 (31.9) | 87 (40.5) | 0.123 * | 42 (35.6) | 0.582 * | 0.078 |
| ICH-score oa, median (IQR) | 1.00 (2.00) | 2.00 (1.00) | 0.003 ^ | 1.00 (1.00) | 0.097 ^ | 0.213 |
| mRS before the ICH, median (IQR) | 0.00 (1.00) | 1.00 (2.00) | 0.128 ^ | 0.00 (2.00) | 0.524 ^ | 0.000 |
| Etiology | ||||||
| Hypertension | 69 (58.0) | 122 (55.5) | 0.645 * | 66 (55.9) | 0.693 * | 0.042 |
| CAA | 12 (10.1) | 15 (6.8) | 0.289 * | 7 (5.9) | 0.232 * | 0.155 |
| Mass | 9 (7.6) | 17 (7.9) | 0.957 * | 9 (7.6) | 1.000 * | 0.000 |
| OAC | 42 (35.3) | 50 (22.7) | 0.013 * | 32 (27.1) | 0.161 * | 0.178 |
| Vessel pathology | 4 (3.4) | 16 (7.3) | 0.145 * | 10 (8.5) | 0.098 * | 0.217 |
| Other/unknown | 25 (21.0) | 42 (19.1) | 0.672 * | 17 (14.4) | 0.229 * | 0.174 |
| Location at baseline | ||||||
| DWM | 53 (45.3) | 104 (47.3) | 0.730 * | 57 (48.3) | 0.689 * | 0.060 |
| Lobar | 47 (39.5) | 92 (41.8) | 0.678 * | 43 (36.4) | 0.687 * | 0.064 |
| Brainstem | 3 (2.5) | 15 (6.8) | 0.093 * | 10 (8.5) | 0.046 * | 0.265 |
| Cerebellum | 15 (12.6) | 26 (11.9) | 0.856 * | 16 (13.7) | 0.827 * | 0.033 |
| Left hemisphere | 68 (57.1) | 114 (51.8) | 0.348 * | 70 (59.3) | 0.792 * | 0.045 |
| Right hemisphere | 56 (47.1) | 118 (53.6) | 0.247 * | 56 (47.5) | 0.896 * | 0.008 |
| IVH oa | 1 (0.8) | 4 (1.8) | 0.476 * | 3 (2.5) | 0.313 * | 0.134 |
| IVH extension | 40 (33.6) | 99 (45.4) | 0.035 * | 48 (40.7) | 0.282 * | 0.147 |
| ICH Volume (cm3) | 8.00 (12.00) | 13 (27.00) | 0.004 ^ | 7.00 (22.00) | 0.997 ^ | 0.009 |
| Invasive procedures, n (%) | ||||||
| Surgical evacuation | 8 (6.7) | 41 (18.6) | 0.003 * | 13 (11.0) | 0.161 * | 0.152 |
| EVD | 9 (7.6) | 40 (18.3) | 0.007 * | 14 (11.9) | 0.272 * | 0.145 |
| Patients’ Characteristics | PSD Melatonin Treated n = 57 | PSD Control Cohort n = 31 | p-Value |
|---|---|---|---|
| Demographics | |||
| Age, y median, (IQR) | 80.00 (16.00) | 79.00 (16.00) | 0.624 ^ |
| Sex, n (%) | 0.640 * | ||
| Male | 32 (56.1) | 19 (61.3) | |
| Female | 25 (43.9) | 12 (38.7) | |
| Risk Factors, n (%) | |||
| HP | 51 (89.5) | 25 (80.6) | 0.249 * |
| DM | 12 (21.1) | 8 (25.8) | 0.611 * |
| HCL | 19 (33.3) | 6 (19.4) | 0.165 * |
| AF | 19 (33.3) | 14 (45.2) | 0.274 * |
| CAD | 15 (26.3) | 9 (29.0) | 0.785 * |
| Obesity (BMI > 30) | 10 (17.5) | 6 (19.4) | 0.833 * |
| Chronic renal failure | 8 (14.0) | 4 (12.9) | 0.883 * |
| Chronic hepatic failure | 1 (1.8) | 0 (0.0) | 0.458 * |
| Smoking | 6 (10.5) | 5 (16.1) | 0.448 * |
| Alcohol | 7 (12.3) | 1 (3.2) | 0.158 * |
| Malignancy | 4 (7.0) | 4 (12.9) | 0.359 * |
| Depression | 2 (3.5) | 3 (9.7) | 0.232 * |
| Cognition | 0.570 *# | ||
| Health | 47 (82.5) | 27 (87.1) | |
| MCI | 8 (14.0) | 4 (12.9) | |
| Dementia | 2 (3.5) | 0 (0.0) | |
| Any kind of infection | 33 (57.9) | 0.067 * | |
| Baseline clinical variables/scales | |||
| NIHSS oa, median (IQR) | 6.00 (8.00) | 10.00 (8.00) | 0.018 ^ |
| Aphasia oa, n (%) | 20 (35.1) | 16 (51.6) | 0.132 * |
| ICH-score oa, median (IQR) | 2.00 (1.00) | 2.00 (1.00) | 0.305 ^ |
| mRS before the ICH, median (IQR) | 0.50 (3.00) | 0.00 (1.00) | 0.190 ^ |
| Etiology | |||
| Hypertension | 39 (68.4) | 18 (58.1) | 0.331 * |
| CAA | 7 (12.3) | 3 (9.7) | 0.713 * |
| Mass | 2 (3.5) | 4 (12.9) | 0.095 * |
| OAC | 24 (42.1) | 10 (32.3) | 0.365 * |
| Vessel pathology | 0 (0.40) | 0 (0.0) | NA * |
| Other/unknown | 9 (15.8) | 4 (12.9) | 0.715 * |
| Location at baseline | |||
| DWM | 31 (54.4) | 14 (45.2) | 0.408 * |
| Lobar | 20 (35.1) | 13 (41.9) | 0.526 * |
| Brainstem | 0 (0.0) | 2 (6.5) | 0.054 * |
| Cerebellum | 6 (10.5) | 4 (12.9) | 0.737 * |
| Left hemisphere | 32 (56.1) | 18 (58.1) | 0.862 * |
| Right hemisphere | 27 (47.4) | 13 (41.9) | 0.625 * |
| IVH oa | 1 (1.8) | 0 (0.0) | 0.458 * |
| IVH extension | 28 (49.1) | 16 (51.6) | 0.823 * |
| ICH Volume (cm3) | 9.00 (17.00) | 10.00 (23.00) | 0.958 ^ |
| Invasive procedures, n (%) | |||
| Surgical evacuation | 1 (1.8) | 2 (6.5) | 0.246 * |
| EVD | 5 (8.8) | 5 (16.1) | 0.299 * |
| PSD Cohort | ||
|---|---|---|
| PSD Duration | B (95CI) | p-Value |
| Unadjusted | −0.189 (−0.407–0.029) | 0.088 |
| Adjusted ^ | −0.071 (−0.273–0.131) | 0.486 |
| PSD Cohort | Non-PSD Cohort | |||
|---|---|---|---|---|
| SU-Stay Duration | B (95CI) | p-Value | B (95CI) | p-Value |
| Unadjusted | −0.147 (−0.278–−0.016) | 0.028 | −0.004 (−0.114–0.123) | 0.941 |
| Adjusted * | −0.094 (−0.207–0.020) | 0.104 | 0.036 (−0.60–0.131) | 0.460 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siokas, V.; Roesch, S.; Stefanou, M.-I.; Buesink, R.; Wilke, V.; Sartor-Pfeiffer, J.; Adeyemi, K.; Poli, S.; Dardiotis, E.; Ziemann, U.; et al. Effects of Melatonin Administration on Post-Stroke Delirium in Patients with Intracerebral Hemorrhage. J. Clin. Med. 2023, 12, 1937. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051937
Siokas V, Roesch S, Stefanou M-I, Buesink R, Wilke V, Sartor-Pfeiffer J, Adeyemi K, Poli S, Dardiotis E, Ziemann U, et al. Effects of Melatonin Administration on Post-Stroke Delirium in Patients with Intracerebral Hemorrhage. Journal of Clinical Medicine. 2023; 12(5):1937. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051937
Chicago/Turabian StyleSiokas, Vasileios, Sara Roesch, Maria-Ioanna Stefanou, Rebecca Buesink, Vera Wilke, Jennifer Sartor-Pfeiffer, Kamaldeen Adeyemi, Sven Poli, Efthimios Dardiotis, Ulf Ziemann, and et al. 2023. "Effects of Melatonin Administration on Post-Stroke Delirium in Patients with Intracerebral Hemorrhage" Journal of Clinical Medicine 12, no. 5: 1937. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12051937