
Pleiotropic Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Cardiovascular Disease and Chronic Kidney Disease

Abstract
:1. Introduction
2. Materials and Methods
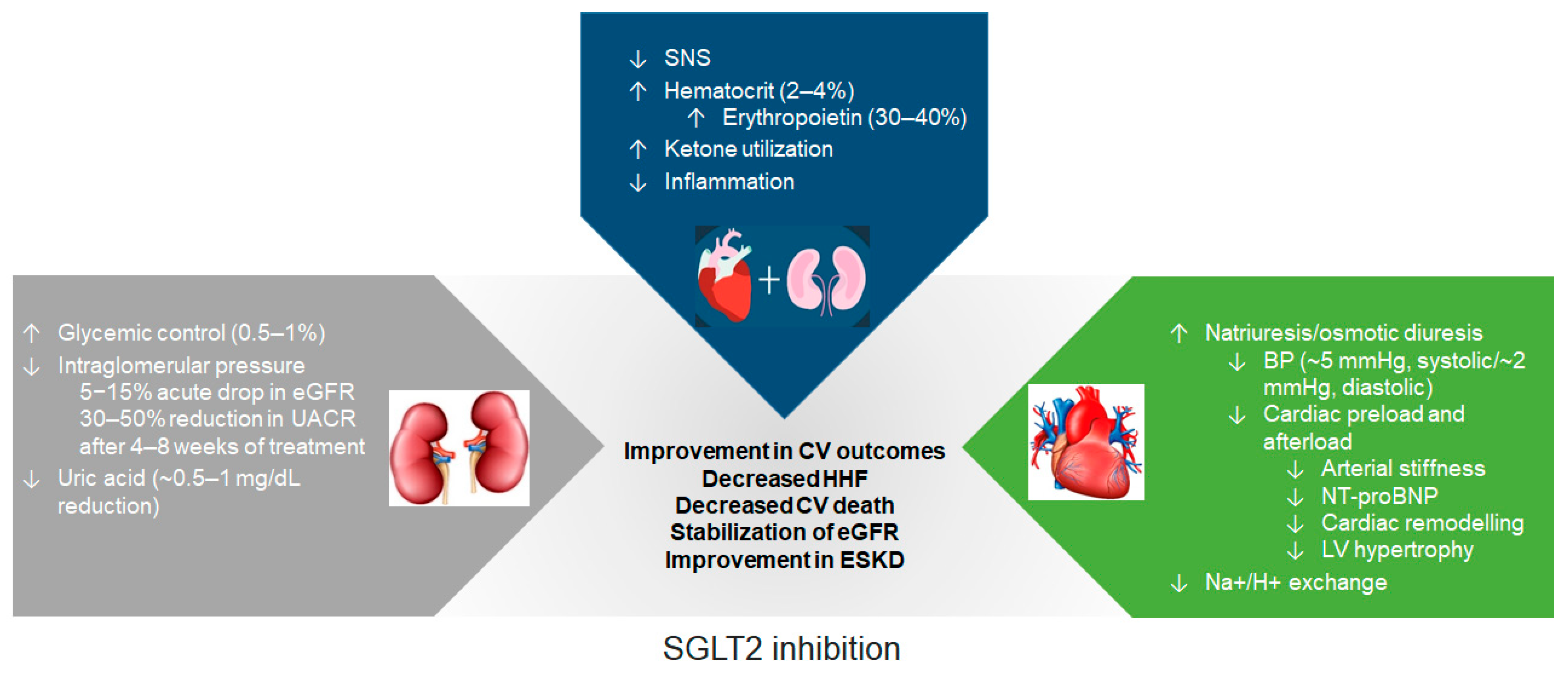
3. SGLT2i Mechanism of Action
3.1. Inhibition of SGLT2 and Glucose-Lowering Effects
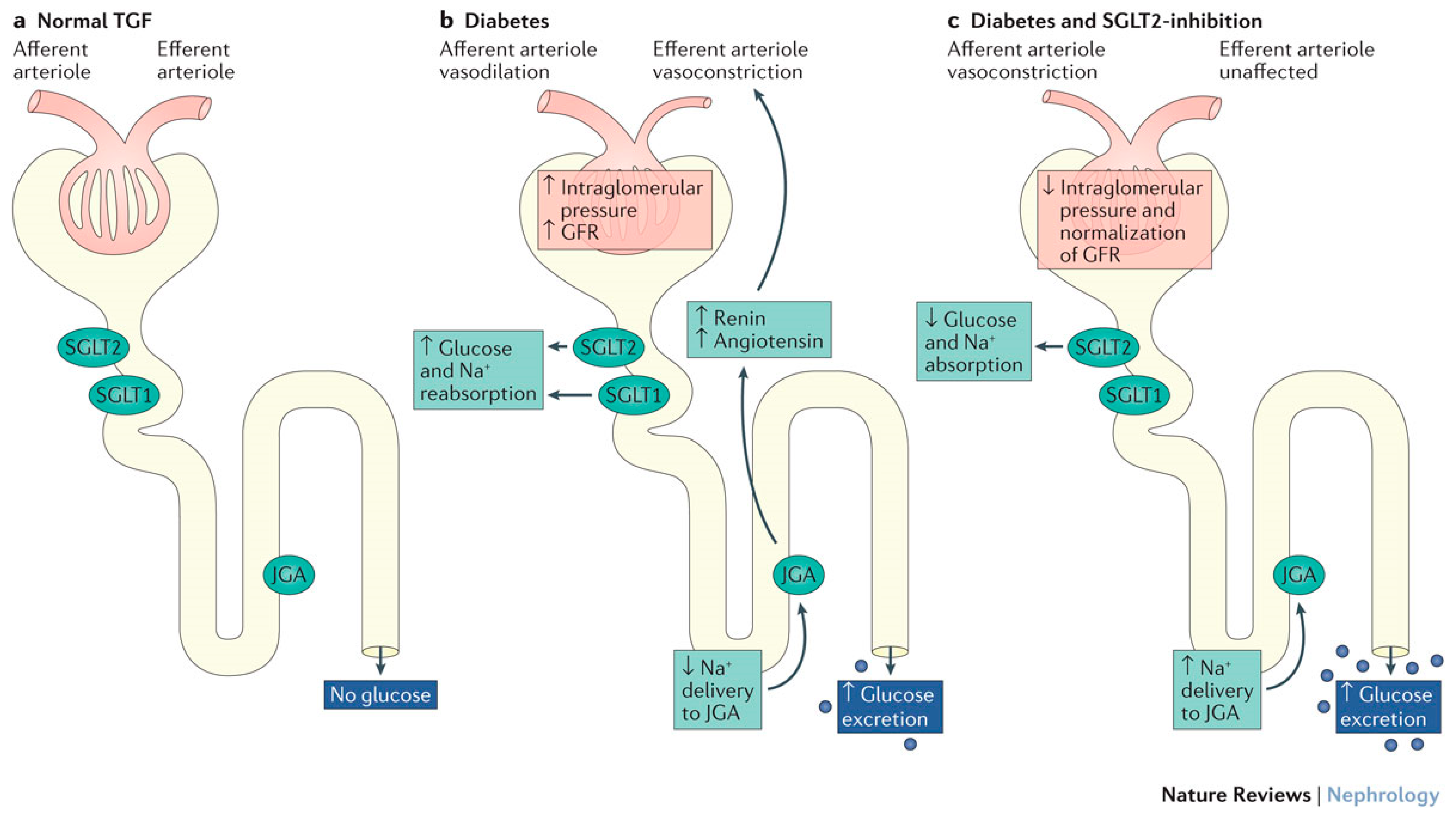
3.2. Reduction in Intraglomerular Pressure and Preservation of Renal Function
3.3. Reduction in Preload/Afterload and Effects on BP
3.4. Effects on Potassium Levels
3.5. Effects on LV Size and Function
3.6. Risk of Ventricular Arrhythmias
3.7. Reduction in SNS Activation
3.8. Effects on Hematologic Parameters
3.9. Reduction in Uric Acid Levels
3.10. Effects on Intracellular Sodium
3.11. Anti-Inflammatory, Antiplatelet, and Antioxidant Effects
3.12. Effects on Lipolysis and Ketone bodies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef]
- Fontes-Carvalho, R.; Santos-Ferreira, D.; Raz, I.; Marx, N.; Ruschitzka, F.; Cosentino, F. Protective Effects of SGLT-2 Inhibitors Across the Cardiorenal Continuum: Two Faces of the Same Coin. Eur. J. Prev. Cardiol. 2022, 29, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- The Emerging Risk Factors Collaboration. Diabetes Mellitus, Fasting Blood Glucose Concentration, and Risk of Vascular Disease: A Collaborative Meta-Analysis of 102 Prospective Studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [Green Version]
- Rydén, L.; Grant, P.J.; Anker, S.D.; Berne, C.; Cosentino, F.; Danchin, N.; Deaton, C.; Escaned, J.; Hammes, H.-P.; Huikuri, H.; et al. ESC Guidelines on Diabetes, pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD: The Task Force on Diabetes, pre-Diabetes, and Cardiovascular Diseases of the European Society of Cardiology (ESC) and Developed in Collaboration with the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2013, 34, 3035–3087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seufert, J. SGLT2 Inhibitors—An Insulin-Independent Therapeutic Approach for Treatment of Type 2 Diabetes: Focus on Canagliflozin. Diabetes Metab. Syndr. Obes. 2015, 8, 543–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; Deswal, A.; Dickson, V.V.; Kosiborod, M.N.; Lekavich, C.L.; et al. Type 2 Diabetes Mellitus and Heart Failure: A Scientific Statement from the American Heart Association and the Heart Failure Society of America: This statement does not represent an update of the 2017 ACC/AHA/HFSA heart failure guideline update. Circulation 2019, 140, e294–e324. [Google Scholar] [CrossRef]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.W. Chronic Kidney Disease: Global Dimension and Perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of Estimated Glomerular Filtration Rate and Albuminuria with All-Cause and Cardiovascular Mortality in General Population Cohorts: A Collaborative Meta-Analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef] [Green Version]
- Scirica, B.M.; Mosenzon, O.; Bhatt, D.L.; Udell, J.A.; Steg, P.G.; McGuire, D.K.; Im, K.; Kanevsky, E.; Stahre, C.; Sjöstrand, M.; et al. Cardiovascular Outcomes According to Urinary Albumin and Kidney Disease in Patients with Type 2 Diabetes at High Cardiovascular Risk: Observations from the SAVOR-TIMI 53 Trial. JAMA Cardiol. 2018, 3, 155–163. [Google Scholar] [CrossRef] [Green Version]
- AstraZeneca. Farxiga® (Dapagliflozin) Tablets, for Oral Use [Prescribing Information]. Available online: https://den8dhaj6zs0e.cloudfront.net/50fd68b9-106b-4550-b5d0-12b045f8b184/0be9cb1b-3b33-41c7-bfc2-04c9f718e442/0be9cb1b-3b33-41c7-bfc2-04c9f718e442_viewable_rendition__v.pdf (accessed on 28 February 2023).
- Boehringer Ingelheim. Jardiance® (Empagliflozin) Tablets, for Oral Use [Prescribing Information]. Available online: https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Jardiance/jardiance.pdf (accessed on 28 March 2022).
- Janssen Pharmaceuticals. Invokana (Canagliflozin) Tablets, for Oral Use [Prescribing Information]. Available online: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVOKANA-pi.pdf (accessed on 29 March 2022).
- Merck & Co. Steglatro™ (Ertugliflozin) Tablets, for Oral Use [Prescribing Information]. Available online: https://www.merck.com/product/usa/pi_circulars/s/steglatro/steglatro_pi.pdf (accessed on 28 March 2022).
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [Green Version]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Cefalu, W.T.; Kaul, S.; Gerstein, H.C.; Holman, R.R.; Zinman, B.; Skyler, J.S.; Green, J.B.; Buse, J.B.; Inzucchi, S.E.; Leiter, L.A.; et al. Cardiovascular Outcomes Trials in Type 2 Diabetes: Where Do We Go from Here? Reflections from a Diabetes Care Editors’ Expert Forum. Diabetes Care 2018, 41, 14–31. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Szarek, M.; Pitt, B.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Inzucchi, S.E.; Kosiborod, M.N.; et al. Sotagliflozin in Patients with Diabetes and Chronic Kidney Disease. N. Engl. J. Med. 2021, 384, 129–139. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Jhund, P.S.; Kondo, T.; Butt, J.H.; Docherty, K.F.; Claggett, B.L.; Desai, A.S.; Vaduganathan, M.; Gasparyan, S.B.; Bengtsson, O.; Lindholm, D.; et al. Dapagliflozin Across the Range of Ejection Fraction in Patients with Heart Failure: A Patient-Level, Pooled Meta-Analysis of DAPA-HF and DELIVER. Nat. Med. 2022, 28, 1956–1964. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- The EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Mc Causland, F.R.; Claggett, B.L.; Vaduganathan, M.; Desai, A.S.; Jhund, P.; de Boer, R.A.; Docherty, K.; Fang, J.; Hernandez, A.F.; Inzucchi, S.E.; et al. Dapagliflozin and Kidney Outcomes in Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction: A Prespecified Analysis of the DELIVER Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 56–65. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- UK Kidney Association. UK Kidney Association Clinical Practice Guideline: Sodium-Glucose Co-Transporter-2 (SGLT-2) Inhibition in Adults with Kidney Disease. Available online: https://ukkidney.org/sites/renal.org/files/UKKA%20guideline_SGLT2i%20in%20adults%20with%20kidney%20disease%20v1%2020.10.21.pdf (accessed on 26 March 2022).
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Wanner, C. EMPA-REG OUTCOME: The Nephrologist’s Point of View. Am. J. Cardiol. 2017, 120, S59–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kshirsagar, R.P.; Kulkarni, A.A.; Chouthe, R.S.; Pathan, S.K.; Une, H.D.; Reddy, G.B.; Diwan, P.V.; Ansari, S.A.; Sangshetti, J.N. SGLT Inhibitors as Antidiabetic Agents: A Comprehensive Review. RSC Adv. 2020, 10, 1733–1756. [Google Scholar] [CrossRef] [Green Version]
- Zelniker, T.A.; Braunwald, E. Mechanisms of Cardiorenal Effects of Sodium-Glucose Cotransporter 2 Inhibitors: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Shepard, B.D.; Pluznick, J.L. Saving the Sweetness: Renal Glucose Handling in Health and Disease. Am. J. Physiol. Renal. Physiol. 2017, 313, F55–F61. [Google Scholar] [CrossRef] [Green Version]
- Lytvyn, Y.; Bjornstad, P.; Udell, J.A.; Lovshin, J.A.; Cherney, D.Z.I. Sodium Glucose Cotransporter-2 Inhibition in Heart Failure: Potential Mechanisms, Clinical Applications, and Summary of Clinical Trials. Circulation 2017, 136, 1643–1658. [Google Scholar] [CrossRef]
- Wilcox, T.; De Block, C.; Schwartzbard, A.Z.; Newman, J.D. Diabetic Agents, from Metformin to SGLT2 Inhibitors and GLP1 Receptor Agonists: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 1956–1974. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-N.; Zhou, Y.; Chen, X.; Che, W.-S.; Leung, S.-W. The Efficacy of Dapagliflozin Combined with Hypoglycaemic Drugs in Treating Type 2 Diabetes Mellitus: Meta-Analysis of Randomised Controlled Trials. BMJ Open 2014, 4, e004619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Sun, J.; Han, R.; Fan, D.; Dong, X.; Luan, Z.; Xiang, R.; Zhao, M.; Yang, J. Efficacy and Safety of Sodium-Glucose Cotransporter-2 Inhibitors Versus Dipeptidyl Peptidase-4 Inhibitors as Monotherapy or Add-on to Metformin in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Obes. Metab. 2018, 20, 113–120. [Google Scholar] [CrossRef]
- Tadic, M.; Sala, C.; Saeed, S.; Grassi, G.; Mancia, G.; Rottbauer, W.; Cuspidi, C. New Antidiabetic Therapy and HFpEF: Light at the End of Tunnel? Heart Fail. Rev. 2022, 27, 1137–1146. [Google Scholar] [CrossRef]
- Caruso, I.; Giorgino, F. SGLT-2 Inhibitors as Cardio-Renal Protective Agents. Metabolism 2022, 127, 154937. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Veltkamp, S.A.; Smulders, R.A.; Kadokura, T. Renal Glucose Handling: Impact of Chronic Kidney Disease and Sodium-Glucose Cotransporter 2 Inhibition in Patients with Type 2 Diabetes. Diabetes Care 2013, 36, 1260–1265. [Google Scholar] [CrossRef] [Green Version]
- Fioretto, P.; Zambon, A.; Rossato, M.; Busetto, L.; Vettor, R. SGLT2 Inhibitors and the Diabetic Kidney. Diabetes Care 2016, 39, S165–S171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherney, D.Z.I.; Cooper, M.E.; Tikkanen, I.; Pfarr, E.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Lund, S.S. Pooled analysis of Phase III trials indicate contrasting influences of renal function on blood pressure, body weight, and HbA1c reductions with empagliflozin. Kidney Int. 2018, 93, 231–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.L.; Perazella, M.A. SGLT2 Inhibitor Therapy in Patients with Type-2 Diabetes Mellitus: Is Acute Kidney Injury a Concern? J. Nephrol. 2020, 33, 985–994. [Google Scholar] [CrossRef]
- List, J.F.; Woo, V.; Morales, E.; Tang, W.; Fiedorek, F.T. Sodium-Glucose Cotransport Inhibition with Dapagliflozin in Type 2 Diabetes. Diabetes Care 2009, 32, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clar, C.; Gill, J.A.; Court, R.; Waugh, N. Systematic Review of SGLT2 Receptor Inhibitors in Dual or Triple Therapy in Type 2 Diabetes. BMJ Open 2012, 2, e001007. [Google Scholar] [CrossRef] [PubMed]
- Tamargo, J. Sodium-glucose Cotransporter 2 Inhibitors in Heart Failure: Potential Mechanisms of Action, Adverse Effects and Future Developments. Eur. Cardiol. 2019, 14, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Rahmoune, H.; Thompson, P.W.; Ward, J.M.; Smith, C.D.; Hong, G.; Brown, J. Glucose Transporters in Human Renal Proximal Tubular Cells Isolated from the Urine of Patients with Non–Insulin-Dependent Diabetes. Diabetes 2005, 54, 3427–3434. [Google Scholar] [CrossRef] [Green Version]
- Anders, H.-J.; Davis, J.M.; Thurau, K. Nephron Protection in Diabetic Kidney Disease. N. Engl. J. Med. 2016, 375, 2096–2098. [Google Scholar] [CrossRef]
- Anders, H.-J.; Huber, T.B.; Isermann, B.; Schiffer, M. CKD in Diabetes: Diabetic Kidney Disease Versus Nondiabetic Kidney Disease. Nat. Rev. Nephrol. 2018, 14, 361–377. [Google Scholar] [CrossRef]
- Sen, T.; Heerspink, H.J.L. A Kidney Perspective on the Mechanism of Action of Sodium Glucose Co-Transporter 2 Inhibitors. Cell Metab. 2021, 33, 732–739. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Norton, L.; Abdul-Ghani, M. Renal, metabolic and cardiovascular considerations of SGLT2 inhibition. Nat. Rev. Nephrol. 2017, 13, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Zelniker, T.A.; Braunwald, E. Cardiac and Renal Effects of Sodium-Glucose Co-Transporter 2 Inhibitors in Diabetes: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Heerspink, H.J.L.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; Hantel, S.; Woerle, H.-J.; Broedl, U.C.; von Eynatten, M.; et al. Empagliflozin and Kidney Function Decline in Patients with Type 2 Diabetes: A Slope Analysis from the EMPA-REG OUTCOME Trial. J. Am. Soc. Nephrol. 2018, 29, 2755–2769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Bommel, E.J.M.; Muskiet, M.H.A.; van Baar, M.J.B.; Tonneijck, L.; Smits, M.M.; Emanuel, A.L.; Bozovic, A.; Danser, A.H.J.; Geurts, F.; Hoorn, E.J.; et al. The Renal Hemodynamic Effects of the SGLT2 Inhibitor Dapagliflozin Are Caused by Post-Glomerular Vasodilatation Rather than pre-Glomerular Vasoconstriction in Metformin-Treated Patients with Type 2 Diabetes in the Randomized, Double-Blind RED Trial. Kidney Int. 2020, 97, 202–212. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Cosentino, F.; Dagogo-Jack, S.; McGuire, D.K.; Pratley, R.; Frederich, R.; Maldonado, M.; Liu, C.-C.; Liu, J.; Pong, A.; et al. Ertugliflozin and Slope of Chronic eGFR. Clin. J. Am. Soc. Nephrol. 2021, 16, 1345–1354. [Google Scholar] [CrossRef]
- Kraus, B.J.; Weir, M.R.; Bakris, G.L.; Mattheus, M.; Cherney, D.Z.I.; Sattar, N.; Heerspink, H.J.L.; Ritter, I.; von Eynatten, M.; Zinman, B.; et al. Characterization and Implications of the Initial Estimated Glomerular Filtration Rate ‘Dip’ upon Sodium-Glucose Cotransporter-2 Inhibition with Empagliflozin in the EMPA-REG OUTCOME Trial. Kidney Int. 2021, 99, 750–762. [Google Scholar] [CrossRef]
- Oshima, M.; Jardine, M.J.; Agarwal, R.; Bakris, G.; Cannon, C.P.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; Levin, A.; et al. Insights From CREDENCE Trial Indicate an Acute Drop in Estimated Glomerular Filtration Rate during Treatment with Canagliflozin with Implications for Clinical Practice. Kidney Int. 2021, 99, 999–1009. [Google Scholar] [CrossRef]
- Adamson, C.; Docherty, K.F.; Heerspink, H.J.L.; de Boer, R.A.; Damman, K.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Petrie, M.C.; et al. Initial Decline (Dip) in Estimated Glomerular Filtration Rate after Initiation of Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction: Insights from DAPA-HF. Circulation 2022, 146, 438–449. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Cosentino, F.; Dagogo-Jack, S.; McGuire, D.K.; Pratley, R.E.; Frederich, R.; Maldonado, M.; Liu, C.C.; Pong, A.; Cannon, C.P.; et al. Initial eGFR Changes with Ertugliflozin and Associations with Clinical Parameters: Analyses from the VERTIS CV Trial. Am. J. Nephrol. 2022, 53, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Jongs, N.; Chertow, G.M.; Greene, T.; McMurray, J.J.V.; Langkilde, A.M.; Correa-Rotter, R.; Kashihara, N.; Rossing, P.; Sjostrom, C.D.; Stefansson, B.V.; et al. Correlates and Consequences of an Acute Change in eGFR in Response to the SGLT2 Inhibitor Dapagliflozin in Patients with CKD. J. Am. Soc. Nephrol. 2022, 33, 2094–2107. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Vart, P.; Jongs, N.; Toto, R.D.; Gorriz, J.L.; Hou, F.F.; McMurray, J.J.V.; Correa-Rotter, R.; Rossing, P.; Sjöström, C.D.; et al. Effects of Dapagliflozin in Stage 4 Chronic Kidney Disease. J. Am. Soc. Nephrol. 2021, 32, 2352–2361. [Google Scholar] [CrossRef] [PubMed]
- Mosenzon, O.; Wiviott, S.D.; Cahn, A.; Rozenberg, A.; Yanuv, I.; Goodrich, E.L.; Murphy, S.A.; Heerspink, H.J.L.; Zelniker, T.A.; Dwyer, J.P.; et al. Effects of Dapagliflozin on Development and Progression of Kidney Disease in Patients with Type 2 Diabetes: An Analysis from the DECLARE-TIMI 58 Randomised Trial. Lancet Diabetes Endocrinol. 2019, 7, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Cherney, D.Z.I. Clinical Implications of an Acute Dip in eGFR after SGLT2 Inhibitor Initiation. Clin. J. Am. Soc. Nephrol. 2021, 16, 1278–1280. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Johnsson, E.; Gause-Nilsson, I.; Cain, V.A.; Sjöström, C.D. Dapagliflozin Reduces Albuminuria in Patients with Diabetes and Hypertension Receiving Renin-Angiotensin Blockers. Diabetes Obes. Metab. 2016, 18, 590–597. [Google Scholar] [CrossRef] [Green Version]
- Cherney, D.Z.I.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; von Eynatten, M.; Wanner, C. Effects of Empagliflozin on the Urinary Albumin-to-Creatinine Ratio in Patients with Type 2 Diabetes and Established Cardiovascular Disease: An Exploratory Analysis from the EMPA-REG OUTCOME Randomised, Placebo-Controlled Trial. Lancet Diabetes Endocrinol. 2017, 5, 610–621. [Google Scholar] [CrossRef]
- Petrykiv, S.I.; Laverman, G.D.; de Zeeuw, D.; Heerspink, H.J.L. The Albuminuria-Lowering Response to Dapagliflozin Is Variable and Reproducible among Individual Patients. Diabetes Obes. Metab. 2017, 19, 1363–1370. [Google Scholar] [CrossRef]
- Jongs, N.; Greene, T.; Chertow, G.M.; McMurray, J.J.V.; Langkilde, A.M.; Correa-Rotter, R.; Rossing, P.; Sjöström, C.D.; Stefansson, B.V.; Toto, R.D.; et al. Effect of Dapagliflozin on Urinary Albumin Excretion in Patients with Chronic Kidney Disease with and without Type 2 Diabetes: A Prespecified Analysis from the DAPA-CKD Trial. Lancet Diabetes Endocrinol. 2021, 9, 755–766. [Google Scholar] [CrossRef]
- Mosenzon, O.; Wiviott, S.D.; Heerspink, H.J.L.; Dwyer, J.P.; Cahn, A.; Goodrich, E.L.; Rozenberg, A.; Schechter, M.; Yanuv, I.; Murphy, S.A.; et al. The Effect of Dapagliflozin on Albuminuria in DECLARE-TIMI 58. Diabetes Care 2021, 44, 1805–1815. [Google Scholar] [CrossRef]
- Neuen, B.L.; Ohkuma, T.; Neal, B.; Matthews, D.R.; de Zeeuw, D.; Mahaffey, K.W.; Fulcher, G.; Li, Q.; Jardine, M.; Oh, R.; et al. Effect of Canagliflozin on Renal and Cardiovascular Outcomes across Different Levels of Albuminuria: Data from the CANVAS Program. J. Am. Soc. Nephrol. 2019, 30, 2229–2242. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.E.; Thorpe, K.E. Acute Kidney Injury with Sodium-Glucose Co-Transporter-2 Inhibitors: A Meta-Analysis of Cardiovascular Outcome Trials. Diabetes Obes. Metab. 2019, 21, 1996–2000. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Cherney, D.; Postmus, D.; Stefánsson, B.V.; Chertow, G.M.; Dwyer, J.P.; Greene, T.; Kosiborod, M.; Langkilde, A.M.; McMurray, J.J.V.; et al. A Pre-Specified Analysis of the Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) Randomized Controlled Trial on the Incidence of Abrupt Declines in Kidney Function. Kidney Int. 2022, 101, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Jhund, P.S.; Solomon, S.D.; Docherty, K.F.; Heerspink, H.J.L.; Anand, I.S.; Böhm, M.; Chopra, V.; de Boer, R.A.; Desai, A.S.; Ge, J.; et al. Efficacy of Dapagliflozin on Renal Function and Outcomes in Patients with Heart Failure with Reduced Ejection Fraction: Results of DAPA-HF. Circulation 2021, 143, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Lambers Heerspink, H.J.; de Zeeuw, D.; Wie, L.; Leslie, B.; List, J. Dapagliflozin a Glucose-Regulating Drug with Diuretic Properties in Subjects with Type 2 Diabetes. Diabetes Obes. Metab. 2013, 15, 853–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sha, S.; Polidori, D.; Heise, T.; Natarajan, J.; Farrell, K.; Wang, S.-S.; Sica, D.; Rothenberg, P.; Plum-Mörschel, L. Effect of the Sodium Glucose Co-Transporter 2 Inhibitor Canagliflozin on Plasma Volume in Patients with Type 2 Diabetes Mellitus. Diabetes Obes. Metab. 2014, 16, 1087–1095. [Google Scholar] [CrossRef]
- Karg, M.V.; Bosch, A.; Kannenkeril, D.; Striepe, K.; Ott, C.; Schneider, M.P.; Boemke-Zelch, F.; Linz, P.; Nagel, A.M.; Titze, J.; et al. SGLT-2-Inhibition with Dapagliflozin Reduces Tissue Sodium Content: A Randomised Controlled Trial. Cardiovasc. Diabetol. 2018, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Baker, W.L.; Smyth, L.R.; Riche, D.M.; Bourret, E.M.; Chamberlin, K.W.; White, W.B. Effects of Sodium-Glucose Co-Transporter 2 Inhibitors on Blood Pressure: A Systematic Review and Meta-Analysis. J. Am. Soc. Hypertens. 2014, 8, 262–275. [Google Scholar] [CrossRef]
- Liu, X.-Y.; Zhang, N.; Chen, R.; Zhao, J.-G.; Yu, P. Efficacy and Safety of Sodium-Glucose Cotransporter 2 Inhibitors in Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials for 1 to 2years. J. Diabetes Complicat. 2015, 29, 1295–1303. [Google Scholar] [CrossRef]
- Staels, B. Cardiovascular Protection by Sodium Glucose Cotransporter 2 Inhibitors: Potential Mechanisms. Am. J. Med. 2017, 130, S30–S39. [Google Scholar] [CrossRef] [Green Version]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholtes, R.A.; Muskiet, M.H.A.; van Baar, M.J.B.; Hesp, A.C.; Greasley, P.J.; Karlsson, C.; Hammarstedt, A.; Arya, N.; van Raalte, D.H.; Heerspink, H.J.L. Natriuretic Effect of Two Weeks of Dapagliflozin Treatment in Patients with Type 2 Diabetes and Preserved Kidney Function during Standardized Sodium Intake: Results of the DAPASALT Trial. Diabetes Care 2021, 44, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Böhm, M.; Fitchett, D.; Ofstad, A.P.; Brueckmann, M.; Kaspers, S.; George, J.T.; Zwiener, I.; Zinman, B.; Wanner, C.; Marx, N.; et al. Heart Failure and Renal Outcomes According to Baseline and Achieved Blood Pressure in Patients with Type 2 Diabetes: Results from EMPA-REG OUTCOME. J. Hypertens. 2020, 38, 1829–1840. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Rao, V.S.; Ivey-Miranda, J.; Fleming, J.; Mahoney, D.; Maulion, C.; Suda, N.; Siwakoti, K.; Ahmad, T.; Jacoby, D.; et al. Empagliflozin in Heart Failure: Diuretic and Cardiorenal Effects. Circulation 2020, 142, 1028–1039. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.; Dewan, P.; Anand, I.; Belohlavek, J.; Bengtsson, O.; de Boer, R.; Böhm, M.; Boulton, D.; Chopra, V.; Demets, D.; et al. Dapagliflozin and Diuretic Use in Patients with Heart Failure and Reduced Ejection Fraction in DAPA-HF. Circulation 2020, 142, 1040–1054. [Google Scholar] [CrossRef]
- Chilton, R.; Tikkanen, I.; Cannon, C.P.; Crowe, S.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. Effects of Empagliflozin on Blood Pressure and Markers of Arterial Stiffness and Vascular Resistance in Patients with Type 2 Diabetes. Diabetes Obes. Metab. 2015, 17, 1180–1193. [Google Scholar] [CrossRef] [Green Version]
- Solini, A.; Giannini, L.; Seghieri, M.; Vitolo, E.; Taddei, S.; Ghiadoni, L.; Bruno, R.M. Dapagliflozin Acutely Improves Endothelial Dysfunction, Reduces Aortic Stiffness and Renal Resistive Index in Type 2 Diabetic Patients: A Pilot Study. Cardiovasc. Diabetol. 2017, 16, 138. [Google Scholar] [CrossRef] [Green Version]
- Striepe, K.; Jumar, A.; Ott, C.; Karg, M.V.; Schneider, M.P.; Kannenkeril, D.; Schmieder, R.E. Effects of the Selective Sodium-Glucose Cotransporter 2 Inhibitor Empagliflozin on Vascular Function and Central Hemodynamics in Patients with Type 2 Diabetes Mellitus. Circulation 2017, 136, 1167–1169. [Google Scholar] [CrossRef]
- Li, H.; Shin, S.E.; Seo, M.S.; An, J.R.; Choi, I.-W.; Jung, W.K.; Firth, A.L.; Lee, D.S.; Yim, M.J.; Choi, G.; et al. The anti-Diabetic Drug Dapagliflozin Induces Vasodilation via Activation of PKG and Kv Channels. Life Sci. 2018, 197, 46–55. [Google Scholar] [CrossRef]
- Chilton, R.J.; Gullestad, L.; Fitchett, D.; Inzucchi, S.E.; Mattheus, M.; Woerle, H.J.; Johansen, O.E. Empagliflozin Reduces Markers of Arterial Stiffness, Vascular Resistance and Cardiac Workload in EMPA-REG OUTCOME. Circulation 2016, 134, 13520. [Google Scholar]
- Michel, A.; Martín-Pérez, M.; Ruigómez, A.; García Rodríguez, L.A. Risk Factors for Hyperkalaemia in a Cohort of Patients with Newly Diagnosed Heart Failure: A Nested Case-Control Study in UK General Practice. Eur. J. Heart Fail. 2015, 17, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Toledo, C.C.; Vellosa Schwartzmann, P.; Miguel Silva, L.; da Silva Ferreira, G.; Bianchini Cardoso, F.; Citelli Ribeiro, V.; Paim, L.R.; Antunes-Correa, L.M.; Carvalho Sposito, A.; Matos Souza, J.R.; et al. Serum Potassium Levels Provide Prognostic Information in Symptomatic Heart Failure Beyond Traditional Clinical Variables. ESC Heart Fail. 2021, 8, 2133–2143. [Google Scholar] [CrossRef] [PubMed]
- Neuen, B.L.; Oshima, M.; Agarwal, R.; Arnott, C.; Cherney, D.Z.; Edwards, R.; Langkilde, A.M.; Mahaffey, K.W.; McGuire, D.K.; Neal, B.; et al. Sodium-Glucose Cotransporter 2 Inhibitors and Risk of Hyperkalemia in People with Type 2 Diabetes: A Meta-Analysis of Individual Participant Data from Randomized, Controlled Trials. Circulation 2022, 145, 1460–1470. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.P.; Zannad, F.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Jamal, W.; Steubl, D.; Schueler, E.; et al. Interplay of Mineralocorticoid Receptor Antagonists and Empagliflozin in Heart Failure: EMPEROR-Reduced. J. Am. Coll. Cardiol. 2021, 77, 1397–1407. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Butler, J.; Zannad, F.; Filippatos, G.; Schueler, E.; Steubl, D.; Zeller, C.; Januzzi, J.L.; Pocock, S.; Packer, M.; et al. Mineralocorticoid Receptor Antagonists and Empagliflozin in Patients with Heart Failure and Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2022, 79, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Kristensen, S.L.; Bengtsson, O.; Böhm, M.; de Boer, R.A.; Docherty, K.F.; Inzucchi, S.E.; Katova, T.; Køber, L.; Kosiborod, M.N.; et al. Dapagliflozin in HFrEF Patients Treated with Mineralocorticoid Receptor Antagonists: An Analysis of DAPA-HF. JACC Heart Fail. 2021, 9, 254–264. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Zannad, F.; Butler, J.; Filipattos, G.; Ritter, I.; Schüler, E.; Kraus, B.J.; Pocock, S.J.; Anker, S.D.; Packer, M. Empagliflozin and Serum Potassium in Heart Failure: An Analysis from EMPEROR-Pooled. Eur. Heart J. 2022, 43, 2984–2993. [Google Scholar] [CrossRef]
- Brown, A.J.M.; Gandy, S.; McCrimmon, R.; Houston, J.G.; Struthers, A.D.; Lang, C.C. A Randomized Controlled Trial of Dapagliflozin on Left Ventricular Hypertrophy in People with Type Two Diabetes: The DAPA-LVH Trial. Eur. Heart J. 2020, 41, 3421–3432. [Google Scholar] [CrossRef]
- Lee, M.M.Y.; Brooksbank, K.J.M.; Wetherall, K.; Mangion, K.; Roditi, G.; Campbell, R.T.; Berry, C.; Chong, V.; Coyle, L.; Docherty, K.F.; et al. Effect of Empagliflozin on Left Ventricular Volumes in Patients with Type 2 Diabetes, or Prediabetes, and Heart Failure with Reduced Ejection Fraction (SUGAR-DM-HF). Circulation 2021, 143, 516–525. [Google Scholar] [CrossRef]
- Omar, M.; Jensen, J.; Ali, M.; Frederiksen, P.H.; Kistorp, C.; Videbæk, L.; Poulsen, M.K.; Tuxen, C.D.; Möller, S.; Gustafsson, F.; et al. Associations of Empagliflozin with Left Ventricular Volumes, Mass, and Function in Patients with Heart Failure and Reduced Ejection Fraction: A Substudy of the Empire HF Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 836–840. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Vargas-Delgado, A.P.; Requena-Ibanez, J.A.; Garcia-Ropero, A.; Mancini, D.; Pinney, S.; Macaluso, F.; Sartori, S.; Roque, M.; Sabatel-Perez, F.; et al. Randomized Trial of Empagliflozin in Nondiabetic Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Soga, F.; Tatsumi, K.; Mochizuki, Y.; Sano, H.; Toki, H.; Matsumoto, K.; Shite, J.; Takaoka, H.; Doi, T.; et al. Positive Effect of Dapagliflozin on Left Ventricular Longitudinal Function for Type 2 Diabetic Mellitus Patients with Chronic Heart Failure. Cardiovasc. Diabetol. 2020, 19, 6. [Google Scholar]
- Sezai, A.; Sekino, H.; Unosawa, S.; Taoka, M.; Osaka, S.; Tanaka, M. Canagliflozin for Japanese Patients with Chronic Heart Failure and Type II Diabetes. Cardiovasc. Diabetol. 2019, 18, 76. [Google Scholar] [CrossRef] [Green Version]
- Curtain, J.P.; Docherty, K.F.; Jhund, P.S.; Petrie, M.C.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Effect of Dapagliflozin on Ventricular Arrhythmias, Resuscitated Cardiac Arrest, or Sudden Death in DAPA-HF. Eur. Heart J. 2021, 42, 3727–3738. [Google Scholar] [CrossRef] [PubMed]
- Sano, M. A New Class of Drugs for Heart Failure: SGLT2 Inhibitors Reduce Sympathetic Overactivity. J. Cardiol. 2018, 71, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoccali, C.; Mallamaci, F.; Parlongo, S.; Cutrupi, S.; Benedetto, F.A.; Tripepi, G.; Bonanno, G.; Rapisarda, F.; Fatuzzo, P.; Seminara, G.; et al. Plasma Norepinephrine Predicts Survival and Incident Cardiovascular Events in Patients with End-Stage Renal Disease. Circulation 2002, 105, 1354–1359. [Google Scholar] [CrossRef] [Green Version]
- Barretto, A.C.P.; Santos, A.C.; Munhoz, R.; Rondon, M.U.P.B.; Franco, F.G.; Trombetta, I.C.; Roveda, F.; de Matos, L.N.J.; Braga, A.M.W.; Middlekauff, H.R.; et al. Increased Muscle Sympathetic Nerve Activity Predicts Mortality in Heart Failure Patients. Int. J. Cardiol. 2009, 135, 302–307. [Google Scholar] [CrossRef]
- Amami, K.; Yamada, S.; Yoshihisa, A.; Kaneshiro, T.; Hijioka, N.; Nodera, M.; Nehashi, T.; Takeishi, Y. Predictive Impacts of Chronic Kidney Disease and Cardiac Sympathetic Nervous Activity on Lethal Arrhythmic Events in Chronic Heart Failure. Ann. Noninvasive Electrocardiol. 2022, 27, e12900. [Google Scholar] [CrossRef]
- Hillis, G.S.; Hata, J.; Woodward, M.; Perkovic, V.; Arima, H.; Chow, C.K.; Zoungas, S.; Patel, A.; Poulter, N.R.; Mancia, G.; et al. Resting Heart Rate and the Risk of Microvascular Complications in Patients with Type 2 Diabetes Mellitus. J. Am. Heart Assoc. 2012, 1, e002832. [Google Scholar] [CrossRef] [Green Version]
- Vazir, A.; Claggett, B.; Pitt, B.; Anand, I.; Sweitzer, N.; Fang, J.; Fleg, J.; Rouleau, J.; Shah, S.; Pfeffer, M.A.; et al. Prognostic Importance of Temporal Changes in Resting Heart Rate in Heart Failure and Preserved Ejection Fraction: From the TOPCAT Study. JACC Heart Fail. 2017, 5, 782–791. [Google Scholar] [CrossRef]
- Herat, L.Y.; Magno, A.L.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.C.; Arcambal, A.; Kiuchi, M.G.; Head, G.A.; Schlaich, M.P.; et al. SGLT2 Inhibitor–Induced Sympathoinhibition: A Novel Mechanism for Cardiorenal Protection. JACC Basic Transl. Sci. 2020, 5, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Gueguen, C.; Burke, S.L.; Barzel, B.; Eikelis, N.; Watson, A.M.D.; Jha, J.C.; Jackson, K.L.; Sata, Y.; Lim, K.; Lambert, G.W.; et al. Empagliflozin modulates renal sympathetic and heart rate baroreflexes in a rabbit model of diabetes. Diabetologia 2020, 63, 1424–1434. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Chen, S.; Imazeki, H.; Ochiai, H.; Seino, Y. Changes in Heart Rate in Patients with Type 2 Diabetes Mellitus after Treatment with Luseogliflozin: Subanalysis of Placebo-Controlled, Double-Blind Clinical Trials. J. Diabetes Investig. 2018, 9, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, W.; Kubota, Y.; Hoshika, Y.; Mozawa, K.; Tara, S.; Tokita, Y.; Yodogawa, K.; Iwasaki, Y.-K.; Yamamoto, T.; Takano, H.; et al. Effects of Empagliflozin Versus Placebo on cardiac Sympathetic Activity in Acute Myocardial Infarction Patients with Type 2 Diabetes Mellitus: The EMBODY Trial. Cardiovasc. Diabetol. 2020, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Hamaoka, T.; Murai, H.; Hirai, T.; Sugimoto, H.; Mukai, Y.; Inoue, O.; Takashima, S.; Kato, T.; Takata, S.; Usui, S.; et al. Different Responses of Muscle Sympathetic Nerve Activity to Dapagliflozin between Patients with Type 2 Diabetes with and without Heart Failure. J. Am. Heart Assoc. 2021, 10, e022637. [Google Scholar] [CrossRef]
- Oshima, M.; Neuen, B.L.; Jardine, M.J.; Bakris, G.; Edwards, R.; Levin, A.; Mahaffey, K.W.; Neal, B.; Pollock, C.; Rosenthal, N.; et al. Effects of Canagliflozin on Anaemia in Patients with Type 2 Diabetes and Chronic Kidney Disease: A Post-Hoc Analysis From the CREDENCE Trial. Lancet Diabetes Endocrinol. 2020, 8, 903–914. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Zinman, B.; Fitchett, D.; Wanner, C.; Ferrannini, E.; Schumacher, M.; Schmoor, C.; Ohneberg, K.; Johansen, O.E.; George, J.T.; et al. How Does Empagliflozin Reduce Cardiovascular Mortality? Insights from a Mediation Analysis of the EMPA-REG OUTCOME Trial. Diabetes Care 2018, 41, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Cherney, D.Z.I.; Cosentino, F.; Pratley, R.E.; Dagogo-Jack, S.; Frederich, R.; Maldonado, M.; Liu, J.; Pong, A.; Liu, C.C.; Cannon, C.P.; et al. The Differential Effects of Ertugliflozin on Glucosuria and Natriuresis Biomarkers: Prespecified Analyses from VERTIS CV. Diabetes Obes. Metab. 2022, 24, 1114–1122. [Google Scholar] [CrossRef]
- Segar, M.W.; Kolkailah, A.A.; Frederich, R.; Pong, A.; Cannon, C.P.; Cosentino, F.; Dagogo-Jack, S.; McGuire, D.K.; Pratley, R.E.; Liu, C.C.; et al. Mediators of Ertugliflozin Effects on Heart Failure and Kidney Outcomes among Patients with Type 2 Diabetes Mellitus. Diabetes Obes. Metab. 2022, 24, 1829–1839. [Google Scholar] [CrossRef]
- Kolkailah, A.A.; Wiviott, S.D.; Raz, I.; Murphy, S.A.; Mosenzon, O.; Bhatt, D.L.; Leiter, L.A.; Wilding, J.P.H.; Gause-Nilsson, I.; Sabatine, M.S.; et al. Effect of Dapagliflozin on Hematocrit in Patients with Type 2 Diabetes at High Cardiovascular Risk: Observations from DECLARE-TIMI 58. Diabetes Care 2022, 45, e27–e29. [Google Scholar] [CrossRef]
- Petrie, M.C.; Verma, S.; Docherty, K.F.; Inzucchi, S.E.; Anand, I.; Belohlávek, J.; Böhm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; et al. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients with Heart Failure with and without Diabetes. JAMA 2020, 323, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Goto, S. Possible Mechanism of Hematocrit Elevation by Sodium Glucose Cotransporter 2 Inhibitors and Associated Beneficial Renal and Cardiovascular Effects. Circulation 2019, 139, 1985–1987. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, H.; Abuaysheh, S.; Hejna, J.; Green, K.; Batra, M.; Makdissi, A.; Chaudhuri, A.; Dandona, P. Dapagliflozin Suppresses Hepcidin and Increases Erythropoiesis. J. Clin. Endocrinol. Metab. 2020, 105, e1056–e1063. [Google Scholar] [CrossRef] [PubMed]
- Mazer, C.D.; Hare, G.M.T.; Connelly, P.W.; Gilbert, R.E.; Shehata, N.; Quan, A.; Teoh, H.; Leiter, L.A.; Zinman, B.; Jüni, P.; et al. Effect of Empagliflozin on Erythropoietin Levels, Iron Stores, and Red Blood Cell Morphology in Patients with Type 2 Diabetes Mellitus and Coronary Artery Disease. Circulation 2020, 141, 704–707. [Google Scholar] [CrossRef]
- Li, J.; Woodward, M.; Perkovic, V.; Figtree, G.A.; Heerspink, H.J.L.; Mahaffey, K.W.; de Zeeuw, D.; Vercruysse, F.; Shaw, W.; Matthews, D.R.; et al. Mediators of the Effects of Canagliflozin on Heart Failure in Patients with Type 2 Diabetes. JACC Heart Fail. 2020, 8, 57–66. [Google Scholar] [CrossRef]
- Sano, M.; Takei, M.; Shiraishi, Y.; Suzuki, Y. Increased Hematocrit during Sodium-Glucose Cotransporter 2 Inhibitor Therapy Indicates Recovery of Tubulointerstitial Function in Diabetic Kidneys. J. Clin. Med. Res. 2016, 8, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Liu, H.; Dong, P. Empagliflozin Reduces Blood Pressure and Uric Acid in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. J. Hum. Hypertens. 2019, 33, 327–339. [Google Scholar] [CrossRef]
- Zhao, Y.; Xu, L.; Tian, D.; Xia, P.; Zheng, H.; Wang, L.; Chen, L. Effects of Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitors on Serum Uric Acid Level: A Meta-Analysis of Randomized Controlled Trials. Diabetes Obes. Metab. 2018, 20, 458–462. [Google Scholar] [CrossRef]
- Akbari, A.; Rafiee, M.; Sathyapalan, T.; Sahebkar, A. Impacts of Sodium/Glucose Cotransporter-2 Inhibitors on Circulating Uric Acid Concentrations: A Systematic Review and Meta-Analysis. J. Diabetes Res. 2022, 2022, 7520632. [Google Scholar] [CrossRef]
- McDowell, K.; Welsh, P.; Docherty, K.F.; Morrow, D.A.; Jhund, P.S.; De Boer, R.A.; O’Meara, E.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; et al. Dapagliflozin Reduces Uric Acid Concentration, an Independent Predictor of Adverse Outcomes in DAPA-HF. Eur. J. Heart Fail. 2022, 24, 1066–1076. [Google Scholar] [CrossRef]
- Chino, Y.; Samukawa, Y.; Sakai, S.; Nakai, Y.; Yamaguchi, J.; Nakanishi, T.; Tamai, I. SGLT2 Inhibitor Lowers Serum Uric Acid through Alteration of Uric Acid Transport Activity in Renal Tubule by Increased Glycosuria. Biopharm. Drug Dispos. 2014, 35, 391–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doehner, W.; Anker, S.D.; Butler, J.; Zannad, F.; Filippatos, G.; Ferreira, J.P.; Salsali, A.; Kaempfer, C.; Brueckmann, M.; Pocock, S.J.; et al. Uric Acid and Sodium-Glucose Cotransporter-2 Inhibition with Empagliflozin in Heart Failure with Reduced Ejection Fraction: The EMPEROR-Reduced Trial. Eur. Heart J. 2022, 43, 3435–3446. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Zannad, F. Effects of Sodium-Glucose Cotransporter 2 Inhibitors for the Treatment of Patients with Heart Failure: Proposal of a Novel Mechanism of Action. JAMA Cardiol. 2017, 2, 1025–1029. [Google Scholar] [CrossRef]
- Packer, M. Activation and Inhibition of Sodium-Hydrogen Exchanger Is a Mechanism that Links the Pathophysiology and Treatment of Diabetes Mellitus with that of Heart Failure. Circulation 2017, 136, 1548–1559. [Google Scholar] [CrossRef] [PubMed]
- Baartscheer, A.; Schumacher, C.A.; Wüst, R.C.I.; Fiolet, J.W.T.; Stienen, G.J.M.; Coronel, R.; Zuurbier, C.J. Empagliflozin Decreases Myocardial Cytoplasmic Na(+) through Inhibition of the Cardiac Na(+)/H(+) Exchanger in Rats and Rabbits. Diabetologia 2017, 60, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Uthman, L.; Baartscheer, A.; Bleijlevens, B.; Schumacher, C.A.; Fiolet, J.W.T.; Koeman, A.; Jancev, M.; Hollmann, M.W.; Weber, N.C.; Coronel, R.; et al. Class Effects of SGLT2 Inhibitors in Mouse Cardiomyocytes and Hearts: Inhibition of Na(+)/H(+) Exchanger, Lowering of Cytosolic Na(+) and Vasodilation. Diabetologia 2018, 61, 722–726. [Google Scholar] [CrossRef] [Green Version]
- Uthman, L.; Li, X.; Baartscheer, A.; Schumacher, C.A.; Baumgart, P.; Hermanides, J.; Preckel, B.; Hollmann, M.W.; Coronel, R.; Zuurbier, C.J.; et al. Empagliflozin Reduces Oxidative Stress through Inhibition of the Novel Inflammation/NHE/[Na(+)](c)/ROS-Pathway in Human Endothelial Cells. Biomed. Pharmacother. 2022, 146, 112515. [Google Scholar] [CrossRef]
- Chung, Y.J.; Park, K.C.; Tokar, S.; Eykyn, T.R.; Fuller, W.; Pavlovic, D.; Swietach, P.; Shattock, M.J. Off-Target Effects of Sodium-Glucose Co-Transporter 2 Blockers: Empagliflozin Does Not Inhibit Na+/H+ Exchanger-1 or Lower [Na+]i in the Heart. Cardiovasc. Res. 2021, 117, 2794–2806. [Google Scholar] [CrossRef]
- Sharma, A.; Tate, M.; Mathew, G.; Vince, J.E.; Ritchie, R.H.; de Haan, J.B. Oxidative Stress and NLRP3-Inflammasome Activity as Significant Drivers of Diabetic Cardiovascular Complications: Therapeutic Implications. Front. Physiol. 2018, 9, 114. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, F.; Scheen, A.J. Effects of SGLT2 Inhibitors on Systemic and Tissue Low-Grade Inflammation: The Potential Contribution to Diabetes Complications and Cardiovascular Disease. Diabetes Metab. 2018, 44, 457–464. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Perco, P.; Mulder, S.; Leierer, J.; Hansen, M.K.; Heinzel, A.; Mayer, G. Canagliflozin Reduces Inflammation and Fibrosis Biomarkers: A Potential Mechanism of Action for Beneficial Effects of SGLT2 Inhibitors in Diabetic Kidney Disease. Diabetologia 2019, 62, 1154–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aragón-Herrera, A.; Feijóo-Bandín, S.; Otero Santiago, M.; Barral, L.; Campos-Toimil, M.; Gil-Longo, J.; Costa Pereira, T.M.; García-Caballero, T.; Rodriguez-Segade, S.; Rodriguez, J.; et al. Empagliflozin Reduces the Levels of CD36 and Cardiotoxic Lipids while Improving Autophagy in the Hearts of Zucker Diabetic Fatty Rats. Biochem. Pharmacol. 2019, 170, 113677. [Google Scholar] [CrossRef]
- Lee, N.; Heo, Y.J.; Choi, S.E.; Jeon, J.Y.; Han, S.J.; Kim, D.J.; Kang, Y.; Lee, K.W.; Kim, H.J. Anti-inflammatory Effects of Empagliflozin and Gemigliptin on LPS-Stimulated Macrophage via the IKK/NF-kappaB, MKK7/JNK, and JAK2/STAT1 Signalling Pathways. J. Immunol. Res. 2021, 2021, 9944880. [Google Scholar] [CrossRef] [PubMed]
- Steven, S.; Oelze, M.; Hanf, A.; Kröller-Schön, S.; Kashani, F.; Roohani, S.; Welschof, P.; Kopp, M.; Godtel-Armbrust, U.; Xia, N.; et al. The SGLT2 Inhibitor Empagliflozin Improves the Primary Diabetic Complications in ZDF Rats. Redox Biol. 2017, 13, 370–385. [Google Scholar] [CrossRef] [PubMed]
- Gohari, S.; Reshadmanesh, T.; Khodabandehloo, H.; Karbalaee-Hasani, A.; Ahangar, H.; Arsang-Jang, S.; Ismail-Beigi, F.; Dadashi, M.; Ghanbari, S.; Taheri, H.; et al. The Effect of EMPAgliflozin on Markers of Inflammation in Patients with Concomitant Type 2 Diabetes Mellitus and Coronary ARtery Disease: The EMPA-CARD Randomized Controlled Trial. Diabetol. Metab. Syndr. 2022, 14, 170. [Google Scholar] [CrossRef]
- Seecheran, N.; Ramdeen, A.; Debideen, N.; Ali, K.; Grimaldos, K.; Grimaldos, G.; Karan, A.; Seecheran, R.; Seecheran, V.; Persad, S.; et al. The Effect of Empagliflozin on Platelet Function Profiles in Patients with Stable Coronary Artery Disease in Trinidad: The EFFECT Pilot Study. Cardiol. Ther. 2021, 10, 189–199. [Google Scholar] [CrossRef]
- Seecheran, N.; Grimaldos, K.; Ali, K.; Grimaldos, G.; Richard, S.; Ishmael, A.; Gomes, C.; Karan, A.; Seecheran, R.; Seecheran, V.; et al. The Effect of Dapagliflozin on Platelet Function Testing Profiles in Diabetic Patients: The EDGE Pilot Study. Cardiol. Ther. 2021, 10, 561–568. [Google Scholar] [CrossRef]
- Gao, Y.M.; Feng, S.T.; Wen, Y.; Tang, T.T.; Wang, B.; Liu, B.C. Cardiorenal Protection of SGLT2 inhibitors-Perspectives from Metabolic Reprogramming. EBioMedicine 2022, 83, 104215. [Google Scholar] [CrossRef]
- Hiruma, S.; Shigiyama, F.; Hisatake, S.; Mizumura, S.; Shiraga, N.; Hori, M.; Ikeda, T.; Hirose, T.; Kumashiro, N. A Prospective Randomized Study Comparing Effects of Empagliflozin to Sitagliptin on Cardiac Fat Accumulation, Cardiac Function, and Cardiac Metabolism in Patients with Early-Stage Type 2 Diabetes: The ASSET Study. Cardiovasc. Diabetol. 2021, 20, 32. [Google Scholar] [CrossRef]
- Kappel, B.A.; Lehrke, M.; Schütt, K.; Artati, A.; Adamski, J.; Lebherz, C.; Marx, N. Effect of Empagliflozin on the Metabolic Signature of Patients with Type 2 Diabetes Mellitus and Cardiovascular Disease. Circulation 2017, 136, 969–972. [Google Scholar] [CrossRef]
- Nishimura, R.; Tanaka, Y.; Koiwai, K.; Ishida, K.; Salsali, A.; Kaspers, S.; Kohler, S.; Lund, S.S. Effect of Empagliflozin on Free Fatty Acids and Ketone Bodies in Japanese Patients with Type 2 Diabetes Mellitus: A Randomized Controlled Trial. Adv. Ther. 2019, 36, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Bitar, Z.I.; Maadarani, O.S.; Alabdali, F.; Teama, A.; Elsawah, W.; Mohsen, M.J.; Elzoueiry, M.M. Sodium-Glucose Cotransporter-2 Inhibitors Induced Euglycemic Diabetic Ketoacidosis: Two Case Reports and a Review of the Literature. Clin. Case Rep. 2022, 10, e05440. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Name | Drug | Population | CV Outcomes, HR (95% CI) | Renal Outcomes, HR (95% CI) |
|---|---|---|---|---|
| CVOTs in patients with T2D | ||||
| CANVAS [15] | Canagliflozin | Age ≥30 y with T2D and established CVD OR Age ≥50 y with T2D and ≥2 CVD risk factors (N = 10,142) | MACE a,b: 0.86 (0.75–0.97) p < 0.001 for noninferiority, p = 0.02 for superiority; CV death or HHF: 0.78 (0.67–0.91); HHF: 0.67 (0.52–0.87); CV death: 0.87 (0.72–1.06) | Progression of albuminuria: 0.73 (0.67–0.79); 40% reduction in eGFR, RRT initiation, or death from renal causes: 0.60 (0.47–0.77) |
| DECLARE–TIMI 58 [18] | Dapagliflozin | Age ≥40 y with T2D and established CVD OR Age ≥55 y (men) or ≥60 y (women) with T2D and ≥1 CVD risk factor (N = 17,160) | MACE a,b: 0.93 (0.84–1.03) p < 0.001 for noninferiority, p = 0.17 for superiority; CV death or HHF a: 0.83 (0.73–0.95) p = 0.005 for superiority; HHF: 0.73 (0.61–0.88); CV death: 0.98 (0.82–1.17) | ≥40% reduction in eGFR to <60 mL/min/1.73 m2, ESKD, or death from CV or renal causes: 0.76 (0.67–0.87) ≥40% reduction in eGFR to <60 mL/min/1.73 m2, ESKD, or death from renal causes: 0.53 (0.43–0.66) |
| EMPA-REG OUTCOME [14,17] | Empagliflozin | Age ≥18 y with T2D and established CVD (N = 7020) | MACE a,b: 0.86 (0.74–0.99) p < 0.001 for noninferiority, p = 0.04 for superiority; MACE b or hospitalization for UA: 0.89 (0.78–1.01) p < 0.001 for noninferiority, p = 0.08 for superiority; CV death or HHF: 0.66 (0.55–0.79) p < 0.001 HHF: 0.65 (0.50–0.85) p = 0.002; CV death: 0.62 (0.49–0.77) p < 0.001 | Incident or worsening nephropathyc or CV death: 0.61 (0.55–0.69) p < 0.001; Incident or worsening nephropathyc: 0.61 (0.53–0.70) p < 0.001; Doubling of sCr with eGFR ≤45 mL/min/1.73 m2, RRT initiation, or death from renal causes: 0.54 (0.40–0.75) p < 0.001 |
| VERTIS CV [19] | Ertugliflozin | Age ≥40 y with T2D and established CVD (N = 8246) | MACE a,b: 0.97 (0.85–1.11) p < 0.001 for noninferiority, CV death or HHF: 0.88 (0.75–1.03) p = 0.11; HHF: 0.70 (0.54–0.90); CV death: 0.92 (0.77–1.11) | Doubling of sCr, RRT initiation, or death from renal causes: 0.81 (0.63–1.04) |
| Renal outcomes trials | ||||
| CREDENCE [28] | Canagliflozin | Age ≥30 y with T2D and CKDd (N = 4401) | MACE b: 0.80 (0.67–0.95) p = 0.01; CV death or HHF: 0.69 (0.57–0.83) p < 0.001; HHF: 0.61 (0.47–0.80) p < 0.001; CV death: 0.78 (0.61–1.00) p = 0.05 | ESKD, doubling of sCr, or death from renal or CV causes a: 0.66 (0.53–0.81) p < 0.001; Doubling of sCr: 0.60 (0.48–0.76) p < 0.001; ESKD: 0.68 (0.54–0.86) p = 0.002 |
| DAPA-CKD [27] | Dapagliflozin | Age ≥18 y with CKDe with or without T2D (N = 4094) Patients without T2D: 32.5% of total population | CV death or HHF: 0.71 (0.55–0.92) p = 0.009; CV death: 0.81 (0.58–1.12); All-cause mortality: 0.69 (0.53–0.88) p = 0.004 | Sustained ≥50% reduction in eGFR, ESKD, or death from renal or CV causes a: 0.61 (0.51–0.72) p < 0.001; Sustained ≥50% reduction in eGFR, ESKD, or death from renal causes: 0.56 (0.45–0.68) p < 0.001; ≥50% reduction in eGFR: 0.53 (0.42–0.67); ESKD: 0.64 (0.50–0.82) |
| EMPA-KIDNEY [29] | Empagliflozin | Adults with CKDf with or without T2D (N = 6609) Patients without T2D: 54% of total population | HHF or death from CV causes: 0.84 (0.67–1.07) p = 0.15; All-cause mortality: 0.87 (0.70–1.08) p = 0.21; All-cause hospitalization 0.86 (0.78–0.95) p = 0.003; Death from CV causes: 0.84 (0.60–1.19) | Kidney disease progression or death from CV causes: 0.72 (0.64–0.82) p < 0.001; Kidney disease progression: 0.71 (0.62–0.81); ESKD or death from CV causes: 0.73 (0.59–0.89) |
| SCORED [20] | Sotagliflozin | Age ≥18 y with T2D, CKDg, and additional CV risk factorsh (N = 10,584) | CV death, HHF, or urgent HF visit a: 0.74 (0.63–0.88) p < 0.001 HHF or urgent HF visit: 0.67 (0.55–0.82) p < 0.001; CV death: 0.90 (0.73–1.12) p = 0.35; MACE: 0.77 (0.65–0.91) | Sustained ≥50% reduction in eGFR for ≥30 d, long-term dialysis, renal transplantation, or sustained eGFR of <15 mL/min/1.73 m2 for ≥30 d: 0.71 (0.46–1.08) |
| HF outcome trials | ||||
| DAPA-HF [23] | Dapagliflozin | Age ≥18 y with NYHA class II–IV HFrEF (EF ≤40%) (N = 4744) Patients without T2D (including previously undiagnosed): n = 2605 (54.9% of total population) | Worsening HFh or CV deatha: 0.74 (0.65–0.85) p < 0.001; CV death or HHF: 0.75 (0.65–0.85) p < 0.001; Worsening HFi: 0.70 (0.59–0.83); HHF: 0.70 (0.59–0.83); Urgent HF visit: 0.43 (0.20–0.90); CV death: 0.82 (0.69–0.98); ΔKCCQ: 1.18 (1.11–1.26) p < 0.001; All-cause mortality: 0.83 (0.71–0.97) | Worsening renal function j: 0.71 (0.44–1.16) |
| DELIVER [25,30] | Dapagliflozin | Age ≥40 y with NYHA class II–IV HFpEF (EF > 40%) with or without T2D (N = 6263) Patients without T2D: n = 3457 (55.2% of total population) | CV death, HHF or urgent HF visita: 0.82 (0.73–0.92) p < 0.001; HF events (HHF/urgent HF visit): 0.79 (0.69–0.91); CV death: 0.88 (0.74–1.05); ΔKCCQ: 1.11 (1.03–1.21) p = 0.009 | Mean difference (95% CI) in eGFR slope change per year vs. placebo (from baseline to end of trial): 0.5 mL/min/1.73 m2 (0.1–0.9) p = 0.01; Mean difference (95% CI) in eGFR slope change per year vs. placebo (from month 1 to end of trial): 1.4 mL/min/1.73 m2 (1.0–1.8) p = 0.001; Composite renal outcome k: 1.08 (0.79–1.49) |
| EMPEROR-Reduced [24] | Empagliflozin | Age ≥18 y with NYHA class II–IV HFrEF (EF ≤ 40%) (N = 3730) Patients without T2D: n = 1874 (50.2% of total population) | CV death or HHF a: 0.75 (0.65–0.86) p < 0.001; HHF: 0.69 (0.59–0.81); CV death: 0.92 (0.75–1.12) | Composite renal outcomel: 0.50 (0.32–0.77) |
| EMPEROR-Preserved [22] | Empagliflozin | Age ≥18 y with NYHA class II–IV HFpEF (EF > 40%) (N = 5988) Patients without T2D: n = 3050 (50.9% of total population) | CV death or HHF a: 0.79 (0.69–0.90) p < 0.001; HHF: 0.71 (0.60–0.83); CV death: 0.91 (0.76–1.09) | Mean difference (95% CI) in eGFR slope change per year vs. placebo: 1.36 mL/min/1.73 m2 (1.06–1.66) p < 0.001; Composite renal outcomej: 0.95 (0.73–1.24) |
| SOLOIST-WHF [21] | Sotagliflozin | Age 18–85 y with T2D and hospitalized for signs and symptoms of HF, treated with intravenous diuretics (N = 1222) | CV death, HHF, or urgent HF visita: 0.67 (0.52–0.85) p < 0.001; HHF or urgent HF visit: 0.64 (0.49–0.83) p < 0.001; CV death: 0.84 (0.58–1.22) p = 0.36 | Difference (95% CI) in LS mean change in eGFR: –0.16 (–1.30, +0.98) mL/min/1.73 m2 |
| Inflammatory Marker | Canagliflozin | Dapagliflozin | Empagliflozin |
|---|---|---|---|
| Adiponectin a | ↑ * | ↑ * | |
| Leptin | ↓ | ↓ | |
| hsCRP | ↓ | ↓ * | ↓ |
| TNF-α | ↓ | ↓ * | ↓ * |
| TNFR1 | ↓ * | ||
| IL-6 | ↓ * | ↓ * | |
| IFN-γ | ↓ * | ||
| MMP7 | ↓ * | ||
| FN1 | ↓ * | ||
| CCL5 | No change | ||
| HGF | ↓ | ||
| VEGFA | ↓300 mg (but not 100 mg) | ||
| FABP1 | ↓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rastogi, A.; Januzzi, J.L., Jr. Pleiotropic Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Cardiovascular Disease and Chronic Kidney Disease. J. Clin. Med. 2023, 12, 2824. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12082824
Rastogi A, Januzzi JL Jr. Pleiotropic Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Cardiovascular Disease and Chronic Kidney Disease. Journal of Clinical Medicine. 2023; 12(8):2824. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12082824
Chicago/Turabian StyleRastogi, Anjay, and James L. Januzzi, Jr. 2023. "Pleiotropic Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Cardiovascular Disease and Chronic Kidney Disease" Journal of Clinical Medicine 12, no. 8: 2824. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12082824