
Are Artificial Intelligence-Assisted Three-Dimensional Histological Reconstructions Reliable for the Assessment of Trabecular Microarchitecture?
 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Procedures
2.2. MicroCT Imaging
2.3. Histological Processing and Scanning
2.4. Three-Dimensional Histological Reconstruction
2.5. Tissue Segmentation
2.6. Measurement Pre-Processing
2.7. Micromorphometric Analysis of the MicroCT and Three-Dimensional Histological Reconstructions
2.8. Statistical Analysis
2.8.1. Spearman’s Rank Correlation Coefficient
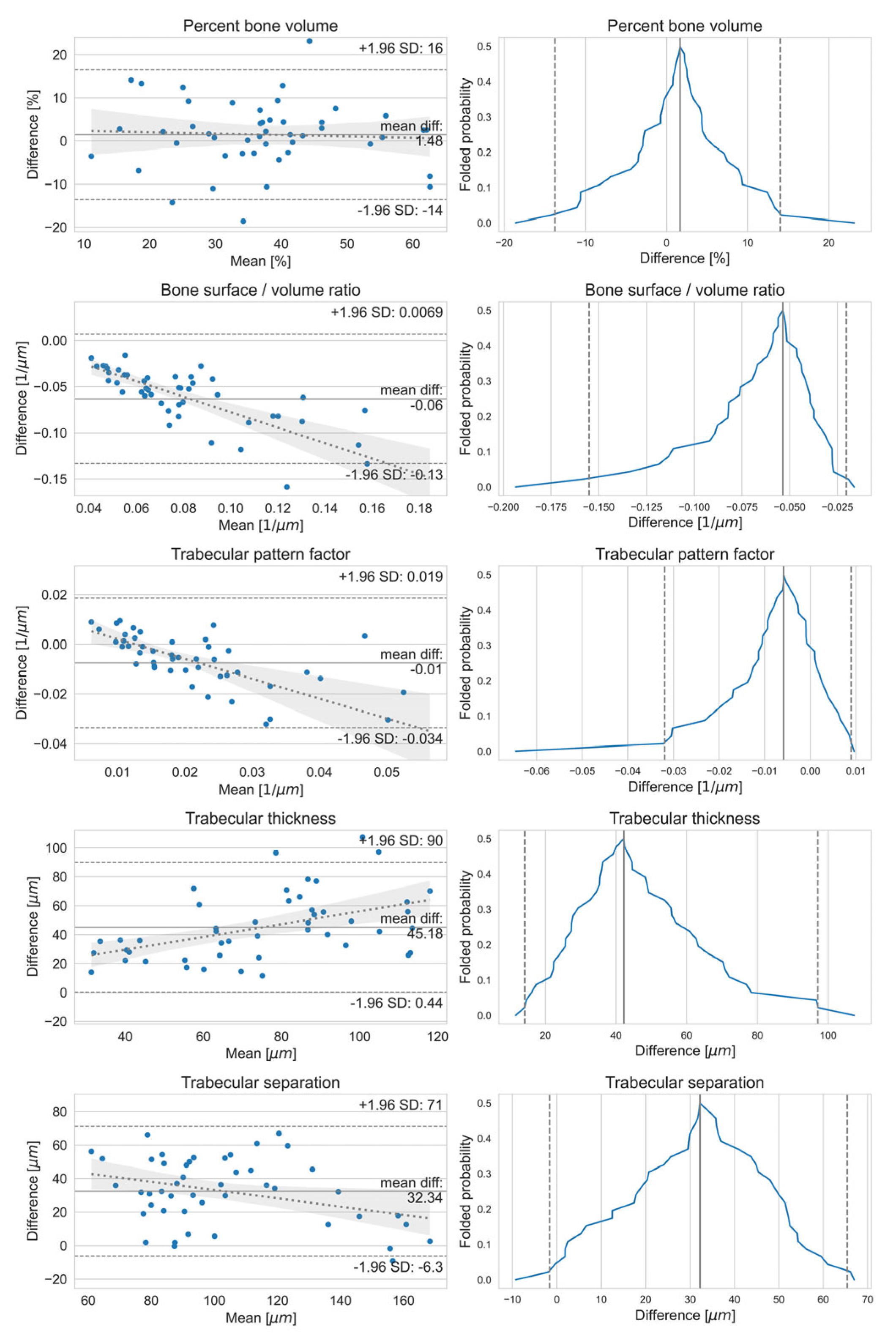
2.8.2. Bland–Altman and Mountain Plots
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (II). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Norton, M.R.; Gamble, C. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implant. Res. 2001, 12, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Nicolielo, L.F.P.; Van Dessel, J.; Jacobs, R.; Quirino Silveira Soares, M.; Collaert, B. Relationship between trabecular bone architecture and early dental implant failure in the posterior region of the mandible. Clin. Oral Implant. Res. 2020, 31, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Bone quality and quantity and dental implant failure: A systematic review and meta-analysis. Int. J. Prosthodont. 2017, 30, 219–237. [Google Scholar] [CrossRef] [PubMed]
- Friberg, B.; Jemt, T.; Lekholm, U. Early failures in 4,641 consecutively placed brånemark dental implants: A study from stage 1 surgery to the connection of completed prostheses. Int. J. Oral. Maxillofac. Implant. 1991, 6, 142–146. [Google Scholar]
- de Oliveira, R.C.; Leles, C.R.; Lindh, C.; Ribeiro-Rotta, R.F. Bone tissue microarchitectural characteristics at dental implant sites. Part 1: Identification of clinical-related parameters. Clin. Oral Implant. Res. 2012, 23, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Friberg, B.; Sennerby, L.; Meredith, N.; Lekholm, U. A comparison between cutting torque and resonance frequency measurements of maxillary implants. A 20-month clinical study. Int. J. Clin. Oral Maxillofac. Surg. 1999, 28, 297–303. [Google Scholar] [CrossRef]
- Murakami, K.; Yamamoto, K.; Ishida, J.; Tsutsumi, S.; Kirita, T. Analysis of implant stability changes in immediate loading using a laser displacement sensor in vivo and comparison of its sensitivity with that of resonance frequency analysis. Clin. Oral Implant. Res. 2021, 32, 1341–1356. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Wang, H.L.; Misch, C.M.; Sharawy, M.; Lemons, J.; Judy, K.W. Rationale for the application of immediate load in implant dentistry: Part I. Implant Dent. 2004, 13, 207–217. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef]
- Kivovics, M.; Szabó, B.T.; Németh, O.; Iványi, D.; Trimmel, B.; Szmirnova, I.; Orhan, K.; Mijiritsky, E.; Szabó, G.; Dobó-Nagy, C. Comparison between micro-computed tomography and cone-beam computed tomography in the assessment of bone quality and a long-term volumetric study of the augmented sinus grafted with an albumin impregnated allograft. J. Clin. Med. 2020, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, E. Methods for assessing bone quality: A review. Clin. Orthop. Relat. Res. 2011, 469, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.C.; Huang, H.L.; Shen, Y.W.; Cai, J.Y.; Fuh, L.J.; Hsu, J.T. Variations in crestal cortical bone thickness at dental implant sites in different regions of the jawbone. Clin. Implant Dent. Relat. Res. 2017, 19, 440–446. [Google Scholar] [CrossRef]
- Fu, M.W.; Shen, E.C.; Fu, E.; Lin, F.G.; Wang, T.Y.; Chiu, H.C. Assessing bone type of implant recipient sites by stereomicroscopic observation of bone core specimens: A comparison with the assessment using dental radiography. J. Periodontol. 2017, 88, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, H.; Moreira-Gonçalves, D.; Coriolano, H.J.; Duarte, J.A. Bone quality: The determinants of bone strength and fragility. Sports Med. 2014, 44, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Rotta, R.F.; de Oliveira, R.C.; Dias, D.R.; Lindh, C.; Leles, C.R. Bone tissue microarchitectural characteristics at dental implant sites part 2: Correlation with bone classification and primary stability. Clin. Oral Implant. Res. 2014, 25, e47–e53. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Sennerby, L.; McGlumphy, E.A.; Tözüm, T.F. Biomechanical aspects of primary implant stability: A human cadaver study. Clin. Implant Dent. Relat. Res. 2009, 11, 113–119. [Google Scholar] [CrossRef]
- Körmöczi, K.; Komlós, G.; Papócsi, P.; Horváth, F.; Joób-Fancsaly, Á. The early loading of different surface-modified implants: A randomized clinical trial. BMC Oral Health 2021, 21, 207. [Google Scholar] [CrossRef]
- Joób-Fancsaly, Á.; Karacs, A.; Pető, G.; Körmöczi, K.; Bogdán, S.; Huszár, T. Effects of a nano-structured surface layer on titanium implants for osteoblast proliferation activity. Acta Polytech. Hung. 2016, 13, 7–25. [Google Scholar]
- Schulze, R.; Heil, U.; Gross, D.; Bruellmann, D.D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A review. Dentomaxillofac. Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are hounsfield units applicable? Dentomaxillofac Radiol. 2015, 44, 20140238. [Google Scholar] [CrossRef]
- Dias, D.R.; Leles, C.R.; Batista, A.C.; Lindh, C.; Ribeiro-Rotta, R.F. Agreement between histomorphometry and microcomputed tomography to assess bone microarchitecture of dental implant sites. Clin. Implant Dent. Relat. Res. 2015, 17, 732–741. [Google Scholar] [CrossRef]
- Kopp, S.; Warkentin, M.; Öri, F.; Ottl, P.; Kundt, G.; Frerich, B. Section plane selection influences the results of histomorphometric studies: The example of dental implants. Biomed. Tech. 2012, 57, 365–370. [Google Scholar] [CrossRef]
- Sarve, H.; Lindblad, J.; Borgefors, G.; Johansson, C.B. Extracting 3d information on bone remodeling in the proximity of titanium implants in srμct image volumes. Comput. Methods Programs Biomed. 2011, 102, 25–34. [Google Scholar] [CrossRef]
- Van Oossterwyck, H.; Duyck, J.; Vander Sloten, J.; Van der Perre, G.; Jansen, J.; Wevers, M.; Naert, I. Use of microfocus computerized tomography as a new technique for characterizing bone tissue around oral implants. J. Oral Implantol. 2000, 26, 5–12. [Google Scholar] [CrossRef]
- Vandeweghe, S.; Coelho, P.G.; Vanhove, C.; Wennerberg, A.; Jimbo, R. Utilizing micro-computed tomography to evaluate bone structure surrounding dental implants: A comparison with histomorphometry. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 1259–1266. [Google Scholar] [CrossRef]
- Müller, R.; Van Campenhout, H.; Van Damme, B.; Van Der Perre, G.; Dequeker, J.; Hildebrand, T.; Rüegsegger, P. Morphometric analysis of human bone biopsies: A quantitative structural comparison of histological sections and micro-computed tomography. Bone 1998, 23, 59–66. [Google Scholar] [CrossRef]
- Chappard, D.; Baslé, M.F.; Legrand, E.; Audran, M. Trabecular bone microarchitecture: A review. Morphologie 2008, 92, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.S. Section plane effects on morphometric values of microcomputed tomography. Biomed. Res. Int. 2019, 2019, 7905404. [Google Scholar] [CrossRef] [PubMed]
- Dalle Carbonare, L.; Valenti, M.T.; Bertoldo, F.; Zanatta, M.; Zenari, S.; Realdi, G.; Lo Cascio, V.; Giannini, S. Bone microarchitecture evaluated by histomorphometry. Micron 2005, 36, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Chappard, D.; Retailleau-Gaborit, N.; Legrand, E.; Baslé, M.F.; Audran, M. Comparison insight bone measurements by histomorphometry and microct. J. Bone Miner. Res. 2005, 20, 1177–1184. [Google Scholar] [CrossRef]
- Schambach, S.J.; Bag, S.; Schilling, L.; Groden, C.; Brockmann, M.A. Application of micro-ct in small animal imaging. Methods 2010, 50, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K. Overview of deep learning in medical imaging. Radiol. Phys. Technol. 2017, 10, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Zadrożny, Ł.; Regulski, P.; Brus-Sawczuk, K.; Czajkowska, M.; Parkanyi, L.; Ganz, S.; Mijiritsky, E. Artificial intelligence application in assessment of panoramic radiographs. Diagnostics 2022, 12, 224. [Google Scholar] [CrossRef] [PubMed]
- Mureșanu, S.; Almășan, O.; Hedeșiu, M.; Dioșan, L.; Dinu, C.; Jacobs, R. Artificial intelligence models for clinical usage in dentistry with a focus on dentomaxillofacial cbct: A systematic review. Oral. Radiol. 2023, 39, 18–40. [Google Scholar] [CrossRef] [PubMed]
- Mohammad-Rahimi, H.; Motamedian, S.R.; Rohban, M.H.; Krois, J.; Uribe, S.E.; Mahmoudinia, E.; Rokhshad, R.; Nadimi, M.; Schwendicke, F. Deep learning for caries detection: A systematic review. J. Dent. 2022, 122, 104115. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, B.A.; Galluci, G.O.; Att, W.; Krishnamurthy, V.R. Artificial intelligence applications in implant dentistry: A systematic review. J. Prosthet. Dent. 2023, 129, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Siddiquee, M.M.R.; Tajbakhsh, N.; Liang, J. Unet++: A nested u-net architecture for medical image segmentation. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support, Proceedings of the 4th International Workshop, DLMIA 2018, and 8th International Workshop, ML-CDS 2018, Held in Conjunction with MICCAI 2018, Granada, Spain, 20 September 2018; Springer International Publishing: Cham, Switzerland, 2018; Volume 11045, pp. 3–11. [Google Scholar]
- Zhang, J.; Liu, Y.; Wu, Q.; Wang, Y.; Liu, Y.; Xu, X.; Song, B. Swtru: Star-shaped window transformer reinforced u-net for medical image segmentation. Comput. Biol. Med. 2022, 150, 105954. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Golla, T.; Dreher, M.; Krois, J. Convolutional neural networks for dental image diagnostics: A scoping review. J. Dent. 2019, 91, 103226. [Google Scholar] [CrossRef]
- Niazi, M.K.K.; Parwani, A.V.; Gurcan, M.N. Digital pathology and artificial intelligence. Lancet Oncol. 2019, 20, e253–e261. [Google Scholar] [CrossRef]
- Kvasnicka, H.M.; Thiele, J.; Amend, T.; Fischer, R. Three-dimensional reconstruction of histologic structures in human bone marrow from serial sections of trephine biopsies. Spatial appearance of sinusoidal vessels in primary (idiopathic) osteomyelofibrosis. Anal. Quant. Cytol. Histol. 1994, 16, 159–166. [Google Scholar]
- Pichat, J.; Iglesias, J.E.; Yousry, T.; Ourselin, S.; Modat, M. A survey of methods for 3d histology reconstruction. Med. Image Anal. 2018, 46, 73–105. [Google Scholar] [CrossRef]
- Kim, J.N.; Lee, J.Y.; Shin, K.J.; Gil, Y.C.; Koh, K.S.; Song, W.C. Haversian system of compact bone and comparison between endosteal and periosteal sides using three-dimensional reconstruction in rat. Anat. Cell Biol. 2015, 48, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Westhauser, F.; Reible, B.; Höllig, M.; Heller, R.; Schmidmaier, G.; Moghaddam, A. Combining advantages: Direct correlation of two-dimensional microcomputed tomography datasets onto histomorphometric slides to quantify three-dimensional bone volume in scaffolds. J. Biomed. Mater. Res. Part A 2018, 106, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.; Gilbert, B.; Harkes, J.; Jukic, D.; Satyanarayanan, M. Openslide: A vendor-neutral software foundation for digital pathology. J. Pathol. Inform. 2013, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Bradski, G. The opencv library. Dr. Dobb’s J. Softw. Tools Prof. Program. 2000, 25, 120–123. [Google Scholar]
- Nagara, K.; Roth, H.R.; Nakamura, S.; Oda, H.; Moriya, T.; Oda, M.; Mori, K. Micro-CT guided 3d reconstruction of histological images. In Patch-Based Techniques in Medical Imaging, Proceedings of the Third International Workshop, Patch-MI 2017, Held in Conjunction with MICCAI 2017, Quebec City, QC, Canada, 14 September 2017, Proceedings 3; Wu, G., Munsell, B.C., Zhan, Y., Bai, W., Sanroma, G., Coupé, P., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 93–101. [Google Scholar]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. ; et al. Qupath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J. Scipy 1.0: Fundamental algorithms for scientific computing in python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Measurement in medicine: The analysis of method comparison studies. J. R. Stat. Soc. Ser. A Stat. Soc. 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Krouwer, J.S.; Monti, K.L. A simple, graphical method to evaluate laboratory assays. J. Clin. Chem. Clin. Biochem. 1995, 33, 525–528. [Google Scholar]
- Barrett, J.F.; Keat, N. Artifacts in ct: Recognition and avoidance. Radiographics 2004, 24, 1679–1691. [Google Scholar] [CrossRef]
- Huang, J.; Hu, J.; Luo, R.; Xie, S.; Wang, Z.; Ye, Y. Linear measurements of sinus floor elevation based on voxel-based superimposition of cone beam computed tomography images. Clin. Implant Dent. Relat. Res. 2019, 21, 1048–1053. [Google Scholar] [CrossRef]
- Hua, Y.; Nackaerts, O.; Duyck, J.; Maes, F.; Jacobs, R. Bone quality assessment based on cone beam computed tomography imaging. Clin. Oral Implant. Res. 2009, 20, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.; Parsa, A.; Hassan, B.; van der Stelt, P.; Aartman, I.H.; Wismeijer, D. Accuracy of trabecular bone microstructural measurement at planned dental implant sites using cone-beam ct datasets. Clin. Oral Implant. Res. 2014, 25, 941–945. [Google Scholar] [CrossRef] [PubMed]
- González-García, R.; Monje, F. The reliability of cone-beam computed tomography to assess bone density at dental implant recipient sites: A histomorphometric analysis by micro-ct. Clin. Oral Implant. Res. 2013, 24, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Yi, W.J.; Heo, M.S.; Lee, S.S.; Choi, S.C.; Huh, K.H. Three-dimensional evaluation of human jaw bone microarchitecture: Correlation between the microarchitectural parameters of cone beam computed tomography and micro-computer tomography. Oral Surg. Oral Med. Oral Radiol. 2015, 120, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Sessirisombat, S.; Panmekiate, S. Mandibular bone structure analysis using cone beam computed tomography vs primary implant stability: An ex vivo study. Int. J. Oral Maxillofac. Implants. 2017, 32, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Van Dessel, J.; Huang, Y.; Depypere, M.; Rubira-Bullen, I.; Maes, F.; Jacobs, R. A comparative evaluation of cone beam ct and micro-ct on trabecular bone structures in the human mandible. Dentomaxillofac. Radiol. 2013, 42, 20130145. [Google Scholar] [CrossRef]
- Van Dessel, J.; Nicolielo, L.F.; Huang, Y.; Coudyzer, W.; Salmon, B.; Lambrichts, I.; Jacobs, R. Accuracy and reliability of different cone beam computed tomography (cbct) devices for structural analysis of alveolar bone in comparison with multislice ct and micro-ct. Eur. J. Oral Implantol. 2017, 10, 95–105. [Google Scholar] [PubMed]
- Oliveira, M.R.; Gonçalves, A.; Gabrielli, M.A.C.; de Andrade, C.R.; Vieira, E.H.; Pereira-Filho, V.A. Evaluation of alveolar bone quality: Correlation between histomorphometric analysis and lekholm and zarb classification. J. Craniofac. Surg. 2021, 32, 2114–2118. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normality Test | One Sample t-Test | Linear Regression | Spearman Correlation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Statistic | p | Statistic | p | Slope | Intercept | p | Correlation Coefficient | p | |
| BV/TV | 2.160 | 0.340 | 1.313 | 0.196 | −0.033 ± 0.091 | 2.691 ± 3.556 | 0.721 | 0.777 | 1.389 × 10−10 |
| BS/TV | 22.399 | 1.000 | −11.977 | 9.971 × 10−16 | −0.839 ± 0.095 | −0.006 ± 0.009 | 2.291 × 10−11 | 0.717 | 1.441 × 10−8 |
| Tb.Pf | 31.800 | 1.000 | −3.824 | 3.933 × 10−4 | −0.800 ± 0.116 | 0.010 ± 0.003 | 1.436 × 10−8 | 0.705 | 3.187 × 10−8 |
| Tb.Th | 5.364 | 0.068 | 13.423 | 1.608 × 10−17 | 0.441 ± 0.122 | 11.889 ± 9.635 | 7.118 × 10−4 | 0.666 | 3.272 × 10−7 |
| Tb.Sp | 3.483 | 0.175 | 11.118 | 1.257 × 10−14 | −0.247 ± 0.102 | 57.799 ± 10.844 | 0.019 | 0.687 | 9.561 × 10−8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Báskay, J.; Pénzes, D.; Kontsek, E.; Pesti, A.; Kiss, A.; Guimarães Carvalho, B.K.; Szócska, M.; Szabó, B.T.; Dobó-Nagy, C.; Csete, D.; et al. Are Artificial Intelligence-Assisted Three-Dimensional Histological Reconstructions Reliable for the Assessment of Trabecular Microarchitecture? J. Clin. Med. 2024, 13, 1106. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13041106
Báskay J, Pénzes D, Kontsek E, Pesti A, Kiss A, Guimarães Carvalho BK, Szócska M, Szabó BT, Dobó-Nagy C, Csete D, et al. Are Artificial Intelligence-Assisted Three-Dimensional Histological Reconstructions Reliable for the Assessment of Trabecular Microarchitecture? Journal of Clinical Medicine. 2024; 13(4):1106. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13041106
Chicago/Turabian StyleBáskay, János, Dorottya Pénzes, Endre Kontsek, Adrián Pesti, András Kiss, Bruna Katherine Guimarães Carvalho, Miklós Szócska, Bence Tamás Szabó, Csaba Dobó-Nagy, Dániel Csete, and et al. 2024. "Are Artificial Intelligence-Assisted Three-Dimensional Histological Reconstructions Reliable for the Assessment of Trabecular Microarchitecture?" Journal of Clinical Medicine 13, no. 4: 1106. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13041106