
The Influence of Hyperthyroidism on the Coagulation and on the Risk of Thrombosis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Studied Population
2.2. Laboratory Analysis
- Activated partial thromboplastin time using IL cephaloplastin reagent, with reference values of 24–36 s. The test was performed on the ACL 6000 apparatus.
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Changes in FVIII Values in Hyperthyroid Patients
4.2. Changes in vWF Values in Hyperthyroid Patients
4.3. Changes in the Concentration of Fibrinogen
4.4. Hyperthyroidism and Dysfunction of the Fibrinolytic System
4.5. Anticardiolipin Antibodies and Thrombosis
4.6. Atrial Fibrillation in Patients with Hyperthyroidism
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.; Ding, C.; Guo, C.; Wang, J.; Liu, S. Association between thyroid dysfunction and venous thromboembolism: A systematic review and meta-analysis. Medicine 2023, 102, e33301. [Google Scholar] [CrossRef]
- Elbers, L.P.B.; Fliers, E.; Cannegieter, S.C. The influence of thyroid function on the coagulation system and its clinical consequences. J. Thromb. Haemost. 2018, 16, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Stuijver, D.J.; van Zaane, B.; Romualdi, E.; Brandjes, D.P.; Gerdes, V.E.; Squizzato, A. The effect of hyperthyroidism on procoagulant, anticoagulant and fibrinolytic factors: A systematic review and meta-analysis. Thromb. Haemost. 2012, 108, 1077–1088. [Google Scholar] [PubMed]
- Debeij, J.; van Zaane, B.; Dekkers, O.M.; Doggen, C.J.; Smit, J.W.; van Zanten, A.P.; Brandjes, D.P.; Büller, H.R.; Gerdes, V.E.; Rosendaal, F.R.; et al. High levels of procoagulant factors mediate the association between free thyroxine and the risk of venous thrombosis: The MEGA study. J. Thromb. Haemost. 2014, 12, 839–846. [Google Scholar] [CrossRef]
- Davis, P.J.; Mousa, S.A.; Schechter, G.P. New Interfaces of Thyroid Hormone Actions with Blood Coagulation and Thrombosis. Clin. Appl. Thromb. Hemost. 2018, 24, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Le Heuzey, J.Y.; Kay, G.N.; Lowe, J.E.; et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: Full Text: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 guidelines for the management of patients with atrial fibrillation) developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Europace 2006, 8, 651–745. [Google Scholar] [PubMed]
- Klein, I.; Danzi, S. Thyroid disease and the heart. Circulation 2007, 116, 725–735. [Google Scholar] [CrossRef]
- Traube, E.; Coplan, N.L. Embolic risk in atrial fibrillation that arises from hyperthyroidism: Review of the medical literature. Tex. Heart Inst. J. 2011, 38, 225–228. [Google Scholar] [PubMed]
- Petersen, P. Thromboembolic complications in atrial fibrillation. Stroke 1990, 21, 4–13. [Google Scholar] [CrossRef]
- Versini, M. Thyroid Autoimmunity and Antiphospholipid Syndrome: Not Such a Trivial Association. Front. Endocrinol. 2017, 8, 175. [Google Scholar] [CrossRef]
- Bithell, T.C. The diagnostic approach to the bleeding disorders. In Wintrobe’s Clinical Hematology; Lee R.G. Lea & Febiger: Philadelphia, PA, USA; London, UK, 1993; pp. 1301–1328. [Google Scholar]
- Bithell, T.C. Blood coagulation; fibrinolysis. In Wintrobe’s Clinical Hematology; Lee R.G. Lea & Febiger: Philadelphia, PA, USA; London, UK, 1993; pp. 592–615. [Google Scholar]
- Kellett, H.A.; Sawars, J.S.; Boulton, E.F.; Cholerton, S.; Park, B.K.; Toft, A.D. Problems of anticoagulation with warfarin in hyperthyroidism. Q. J. Med. 1986, 225, 43–51. [Google Scholar]
- Horne, K.M.; Singh, K.K.; Rosenfeld, G.K.; Wesley, R.; Skarulis, C.M.; Merryman, K.P.; Cullinane, A.; Costelo, R.; Patterson, A.; Eggerman, T.; et al. Is thyroid hormone suppression therapy prothrombotic? J. Clin. Endocrinol. Metab. 2004, 89, 4469–4473. [Google Scholar] [CrossRef]
- Tracy, P.R.; Arnold, M.A.; Ettiinger, W.; Fried, L.; Meilahn, E.; Savage, P. The relationship of fibrinogen and factor VII and VIII to incident cardiovascular disease and death in the elderly: Result from the cardiovascular health study. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 1776–1783. [Google Scholar] [CrossRef]
- Klein, I.; Levey, G.S. Unusual Manifestation of hypothyroidism. Arch. Intern. Med. 1984, 144, 123–128. [Google Scholar] [CrossRef]
- Li, Y.; Chen, H.; Tan, J.; Wang, X.; Liang, H.; Sun, H. Impaired release of tissue plasminogen activator from the endothelium in Graves’ disease-indicator of endothelial dysfunction and reduced fibrinolytic capacity. Eur. J. Clin. Investig. 1998, 28, 1050–1054. [Google Scholar] [CrossRef]
- Homoncik, M.; Alois, G.; Bernd, J.; Heinrich, V. Altered platelet plug formation in hyperthyroidism and hypothyroidism. J. Clin. Endocrinol. Metab. 2007, 92, 3006–3012. [Google Scholar] [CrossRef]
- Thögersen, M.A.; Jansson, J.H.; Boman, K.; Nilsson, K.T.; Weinehall, L.; Huhtasaari, F.; Hallmans, G. High plasminogen activator inhibitor and tissue plasminogen activator levels in plasma precede a first acute myocardial infarction in both men and women. Evidence for the fibrinolytic system as an independent primary risk factor. Circulation 1998, 98, 2241–2247. [Google Scholar] [CrossRef]
- Thompson, S.G.; Kienast, J.; Pyke, S.D.; Haverkate, F.; van den Loo, W.C. Hemostatic factors and the risk of myocardial infarction or sudden death in patients with angina pectoris. N. Engl. J. Med. 1995, 332, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Desforges, J.F. Hematologic manifestations of endocrine disorders. In Hematology; Basic Principles and Practice, 2nd ed.; Hoffman, A., Benz, E.J., Shattil, S.J., Furie, B., Cohen, J.H., Silberstein, L.E., Eds.; Churchill Livingstone: New York, NY, USA, 1995; pp. 2155–2156. [Google Scholar]
- Ma, J.; Hannekens, H.C.; Ridkrer, P.M.; Stamfer, J.M. A prospective study of fibrinogen and risk of myocardial infarction in the physicians Health study. J. Am. Coll. Cardiol. 1999, 33, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Dörr, M.; Wolf, B.; Robinson, M.D.; John, U.; Lüdeman, J.; Meg, W.; Felix, B.S.; Wölzke, H. The association of thyroid function with cardiac mass and left ventricular hypertrophy. J. Clin. Endocrinol. Metab. 2005, 90, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Triplett, D.A. Protein S deficiency. In Disorders of Haemostasis and Thrombosis; Goodnight, S.H., Hathaway, W.E., Eds.; The McGraw-Hill Companies: New York, NY, USA, 2001; pp. 374–380. [Google Scholar]
- Squizzato, A.; Romualdi, E.; Büller, H.R.; Gerdes, V.E. Clinical review: Thyroid dysfunction and effects on coagulation and fibrinolysis: A systematic review. J. Clin. Endocrinol. Metab. 2007, 92, 2415–2420. [Google Scholar] [CrossRef]
- Bovill, E.G. Fibrinolytic defects and thrombosis. In Disorders of Haemostasis and Thrombosis; Goodnight, S.H., Hathaway, W.E., Eds.; The McGraw-Hill Companies: New York, NY, USA, 2001; pp. 389–396. [Google Scholar]
- Kohler, P.H.; Grant, J.P. Plasminogen-activator inhibitor type 1 and coronary artery disease. N. Engl. J. Med. 2000, 342, 1792–1801. [Google Scholar] [CrossRef]
- Tofler, G.H.; D’Agostino, R.B.; Jacques, P.F.; Bostom, A.G.; Wilson, P.W.; Lipinska, I.; Mittleman, M.A.; Selhub, J. Association between increases homocysteine levels and impaired fibrinolytic potential: Potential mechanism for cardiovascular risk. Thromb. Haemost. 2002, 88, 799–804. [Google Scholar]
- Hamsten, A.; Walldius, G.; Szamosi, A.; Blombäck, M.; de Faire, U.; Dahlén, G.; Landou, C.; Wiman, B. Plasminogen activator inhibitors in plasma: Risk factor for recurrent myocardial infarction. Lancet 1987, 8549, 3–9. [Google Scholar] [CrossRef]
- Bauer, K.A. Hypercoagulable states. In Hematology: Basic Principles and Practice; Hoffman, R., Benz, E.J., Shattil, S.J., Furie, B., Cohen, H.J., Silberstein, L.E., McGlave, P., Eds.; Elsevier Churchill Livingstone: Philadelphia, PA, USA, 2005; pp. 2197–2224. [Google Scholar]
- Rand, J.H.; Senzel, L. Antiphospholipid antiboidies and the antiphospholipid syndrome. In Haemostasis and Thrombosis: Basic Principles and Clinical Practice; Colman, R.W., Clowes, A.W., Goldhaber, S.Z., Marder, V.J., George, J.N., Eds.; Lippincott Williams&Wilkins: Philadelphia, PA, USA, 2006; pp. 1621–1636. [Google Scholar]
- McCrae, K.R.; Feinstein, D.I.; Cines, D.B. Antiphospholipid antibodies and the antiphospholipid syndrome. In Haemostasis and Thrombosis: Basic Principles and Clinical Practice; Colman, R.W., Hirsh, J., Marder, V.J., Clowes, A.W., George, J.N., Eds.; Lippincott Williams&Wilkins: Philadelphia, PA, USA, 2001; pp. 1339–1356. [Google Scholar]
- Petersen, P.; Hansen, M.J. Stroke in thyrotoxicosis with atrial fibrilation. Stroke 1989, 19, 15–18. [Google Scholar] [CrossRef]
- Sheu, J.J.; Kang, J.H.; Lin, H.C.; Lin, H.C. Hyperthyroidism and risk of ischemic stroke in young adults: A 5-year follow-up study. Stroke 2010, 5, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Staffurth, J.S.; Gibberd, M.C.; Fui, S.N. Arterial embolism in thyrotoxicosis with atrial fibrillation. Br. Med. J. 1977, 2, 688–690. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.J.; Lawson, D.H. Death from thyrotoxicosis. Lancet 1973, 2, 894–895. [Google Scholar] [CrossRef]
- Parle, V.J.; Maisonneuve, P.; Sheppard, C.M.; Boyle, P.; Franklyn, A.J. Prediction of all-cause and cardiovascular mortality in elderly people from one low serum thyrothropin result: A 10-year cohort study. Lancet 2001, 358, 861–865. [Google Scholar] [CrossRef]
- Siu, C.W.; Pong, V.; Zhang, X.; Siu, C.W.; Pong, V.; Zhang, X.; Chan, Y.H.; Jim, M.H.; Liu, S.; Yiu, K.H.; et al. Risk of ischemic stroke after new-onset atrial fibrillation in patients with hyperthyroidism. Heart Rhythm 2009, 6, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Rietveld, I.M.; Lijfering, W.M.; le Cessie, S.; Bos, M.H.A.; Rosendaal, F.R.; Reitsma, P.H.; Cannegieter, S.C. High levels of coagulation factors and venous thrombosis risk: Strongest association for factor VIII and von Willebrand factor. J. Thromb. Haemost. 2019, 17, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Yang, Y.; Kan, H. Increased risk of pulmonary embolism among patients with hyperthyroidism: A 5-year follow-up study. J. Thromb. Haemost. 2010, 8, 2176–2181. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Hyperthyroidism n = 64 | Hypothyroidism n = 68 | Euthyreosis n = 68 | p |
|---|---|---|---|---|
| Age, years ± SD | 43.23 ± 13.77 | 48.09 ± 13.63 | 44.06 ± 14.86 | 0.129 |
| BMI, kg/m2 ± SD | 23.16 ± 3.74 | 27.21 ± 6.08 | 24.37 ± 3.84 | >0.05 |
| Female, % | 82.8 | 85.3 | 55.9 | 0.000 |
| Atrial fibrillation, % | 8.3 | 1.5 | 0.0 | 0.022 |
| Thrombotic events, % | 6.3 | 2.6 | 1.5 | 0.313 |
| aCLA IgG p.o., % | 5.9 | 10.6 | 0.0 | 0.113 |
| aCLA IgG p.s., % | 0.0 | 5.3 | 0.0 | 0.113 |
| aCLA IgG p.m., % | 5.9 | 5.3 | 0.0 | 0.113 |
| aLCA IgM p.o., % | 37.6 | 5.6 | 0.0 | 0.000 |
| aLCA IgM p.s., % | 18.8 | 5.6 | 0.0 | 0.000 |
| aCLA IgM p.m., % | 18.8 | 0.0 | 0.0 | 0.000 |
| Variable | Hyperthyroidism n = 64 | Hypothyroidism n = 68 | Euthyreosis n = 68 | p |
|---|---|---|---|---|
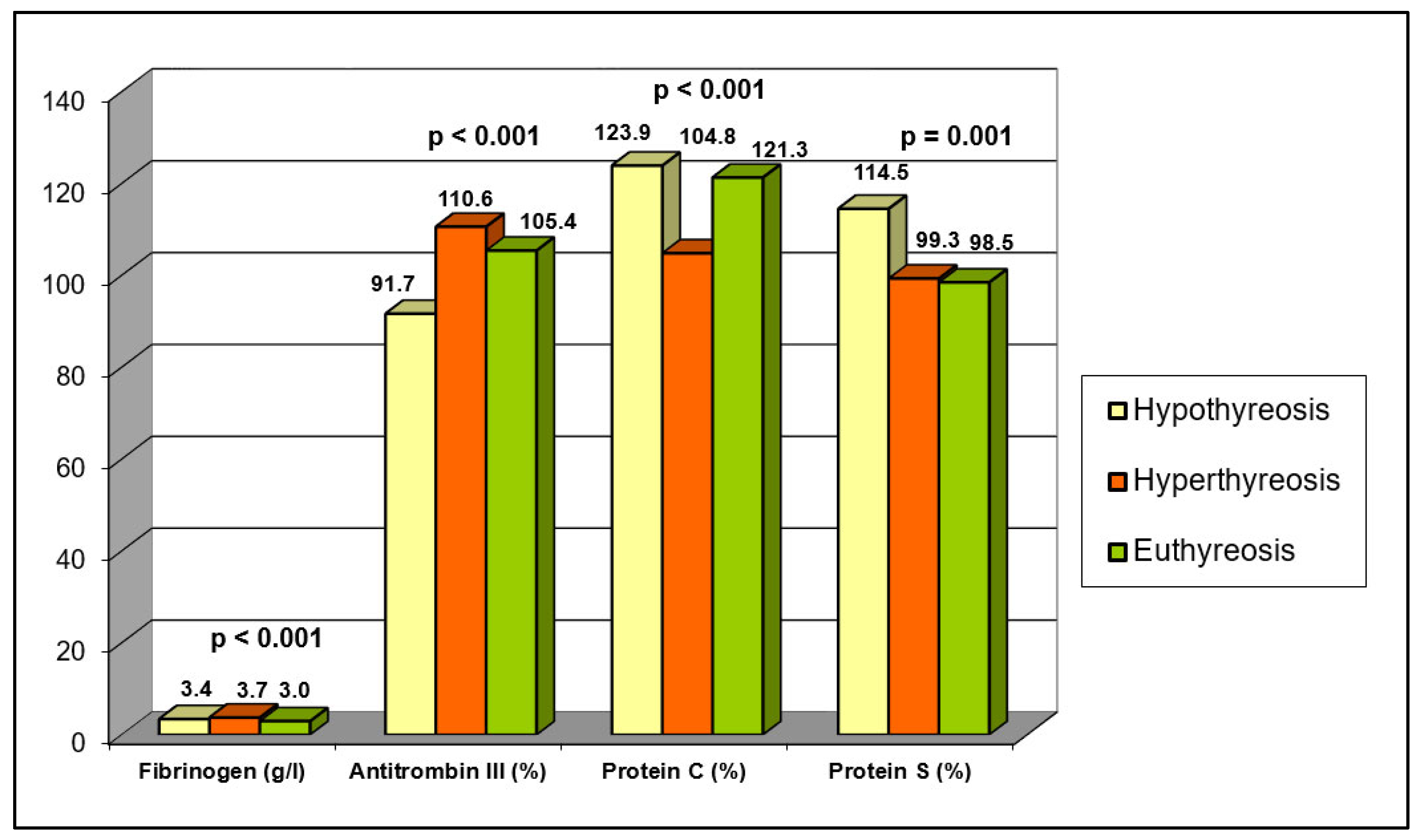
| Fibrinogen (g/L), mean ± SD | 3.74 ± 0.79 | 3.41 ± 1.06 | 2.96 ± 0.74 | 0.000 |
| Antithrombin III (%), mean ± SD | 110.60 ± 14.50 | 91.65 ± 16.68 | 105.41 ± 10.67 | 0.000 |
| FVIII (U/mL), mean ± SD | 1.67 ± 0.78 | 0.93 ± 0.40 | 0.95 ± 0.24 | 0.000 |
| FVIII (U/mL) ≥ 1.5 U/mL, % | 79.4 | 17.6 | 2.9 | 0.000 |
| vWF (%), mean ± SD | 115.8 ± 20.3 | 81.6 ± 19.6 | 91.0 ± 12.8 | 0.000 |
| Protein C (%), mean ± SD | 104.84 ± 24.10 | 123.91 ± 22.90 | 121.30 ± 21.45 | 0.000 |
| Protein S (%), mean ± SD | 99.33 ± 20.88 | 114.52 ± 21.65 | 98.48 ± 26.26 | 0.001 |
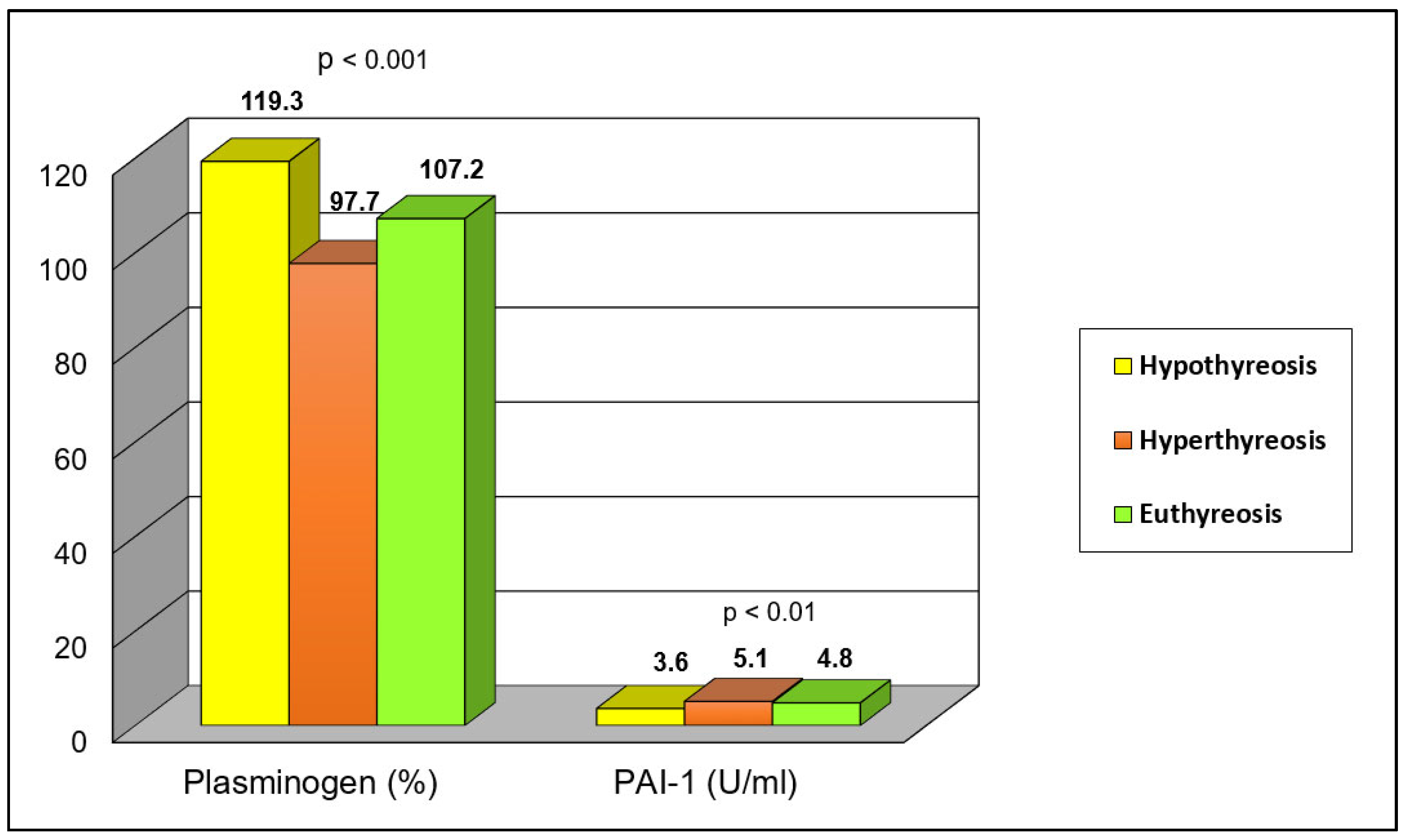
| Plasminogen (%), mean ± SD | 97.67 ± 20.39 | 119.28 ± 19.28 | 107.23 ± 18.51 | 0.000 |
| PAI-1 (U/mL), mean ± SD | 5.08 ± 1.94 | 3.62 ± 2.13 | 4.81 ± 1.56 | 0.001 |
| Fibrinogen > 4 g/L, % | 30.4 | 18.3 | 10.6 | 0.022 |
| Antithrombin > 75%, % | 98.1 | 86.5 | 100.0 | 0.001 |
| Protein C < 69%, % | 2.0 | 0.0 | 0.0 | 0.326 |
| Protein S < 65%, % | 4.8 | 2.3 | 9.7 | 0.266 |
| Plasminogen > 75%, % | 90.4 | 100.0 | 97.0 | 0.068 |
| PAI-1 > 3.5 U/mL, % | 73.0 | 53.6 | 73.8 | 0.133 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonijevic, N.; Matic, D.; Beleslin, B.; Mikovic, D.; Lekovic, Z.; Marjanovic, M.; Uscumlic, A.; Birovljev, L.; Jakovljevic, B. The Influence of Hyperthyroidism on the Coagulation and on the Risk of Thrombosis. J. Clin. Med. 2024, 13, 1756. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13061756
Antonijevic N, Matic D, Beleslin B, Mikovic D, Lekovic Z, Marjanovic M, Uscumlic A, Birovljev L, Jakovljevic B. The Influence of Hyperthyroidism on the Coagulation and on the Risk of Thrombosis. Journal of Clinical Medicine. 2024; 13(6):1756. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13061756
Chicago/Turabian StyleAntonijevic, Nebojsa, Dragan Matic, Biljana Beleslin, Danijela Mikovic, Zaklina Lekovic, Marija Marjanovic, Ana Uscumlic, Ljubica Birovljev, and Branko Jakovljevic. 2024. "The Influence of Hyperthyroidism on the Coagulation and on the Risk of Thrombosis" Journal of Clinical Medicine 13, no. 6: 1756. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13061756