Differentiating SIADH from Cerebral/Renal Salt Wasting: Failure of the Volume Approach and Need for a New Approach to Hyponatremia

Abstract
:1. Introduction
2. Pathophysiology of RSW and SIADH and Evolution of Controversy on Rarity of Cerebral Salt Wasting
3. Differentiating SIADH from RSW

{kind=link}
{kind=link}
{kind=link}
| Clinical Findings Common to both SIADH and RSW |
| Association with intracranial disease |
| Hyponatremia |
| Concentrated urine |
| Urine sodium [Na] usually >20 mEq/L |
| Non-edematous |
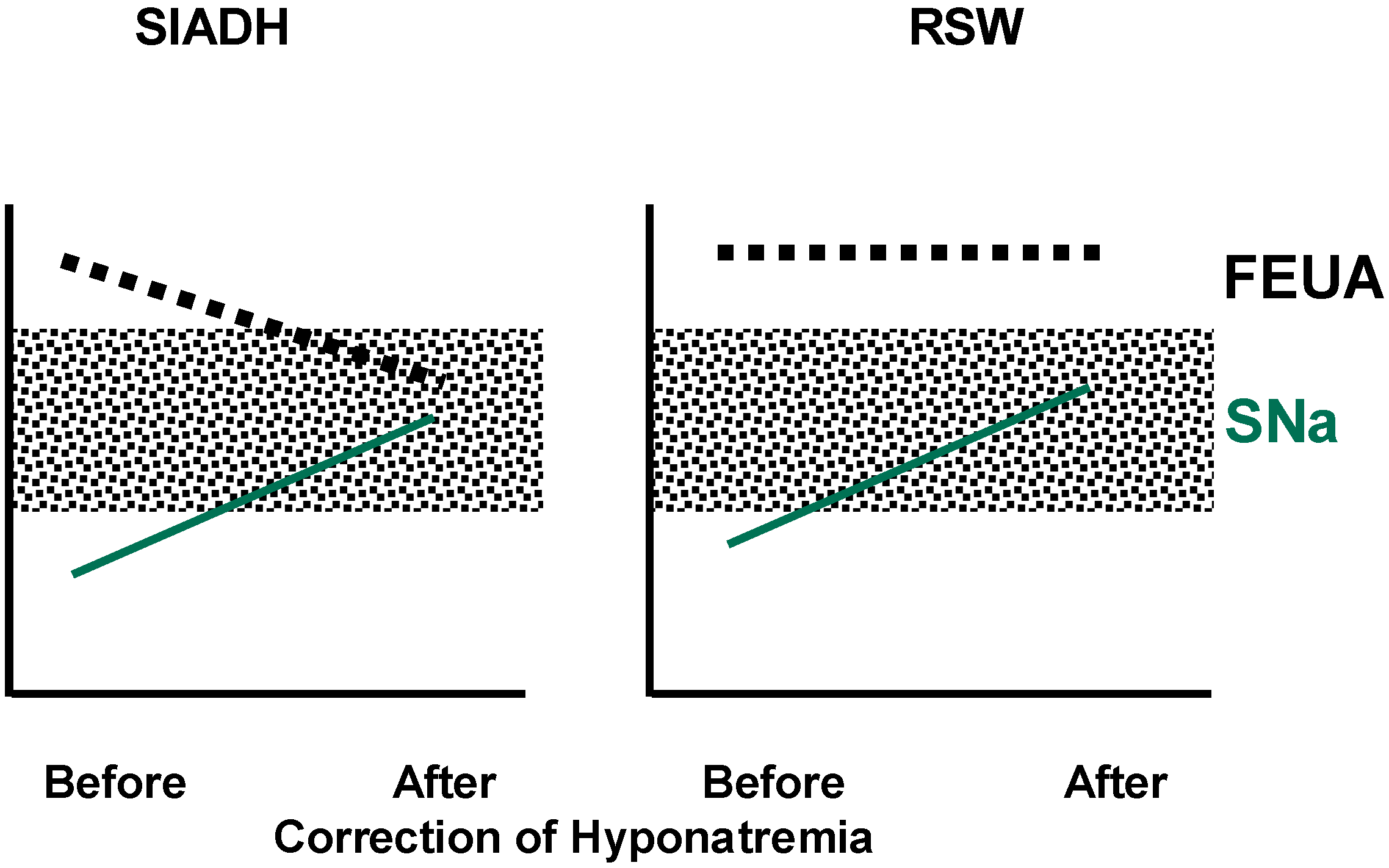
| Hypouricemia, with increased fractional excretion urate (FEurate) |
| Only Difference between SIADH and RSW |
| Volume state: normal/high in SIADH |
| low in RSW |
| Author [ref.] | No. of Patients | Low Blood Volume RSW | Increased Blood Volume SIADH | Urine Na mEq/L |
|---|---|---|---|---|
| Nelson [20] | 12 | 10 (83%) | 2 | 41–203 |
| Wijdicks [21] | 9 | 8 (89%) | 1 | -- |
| Sivakumar [23] | 18 | 17 (94%) | 43–210 |
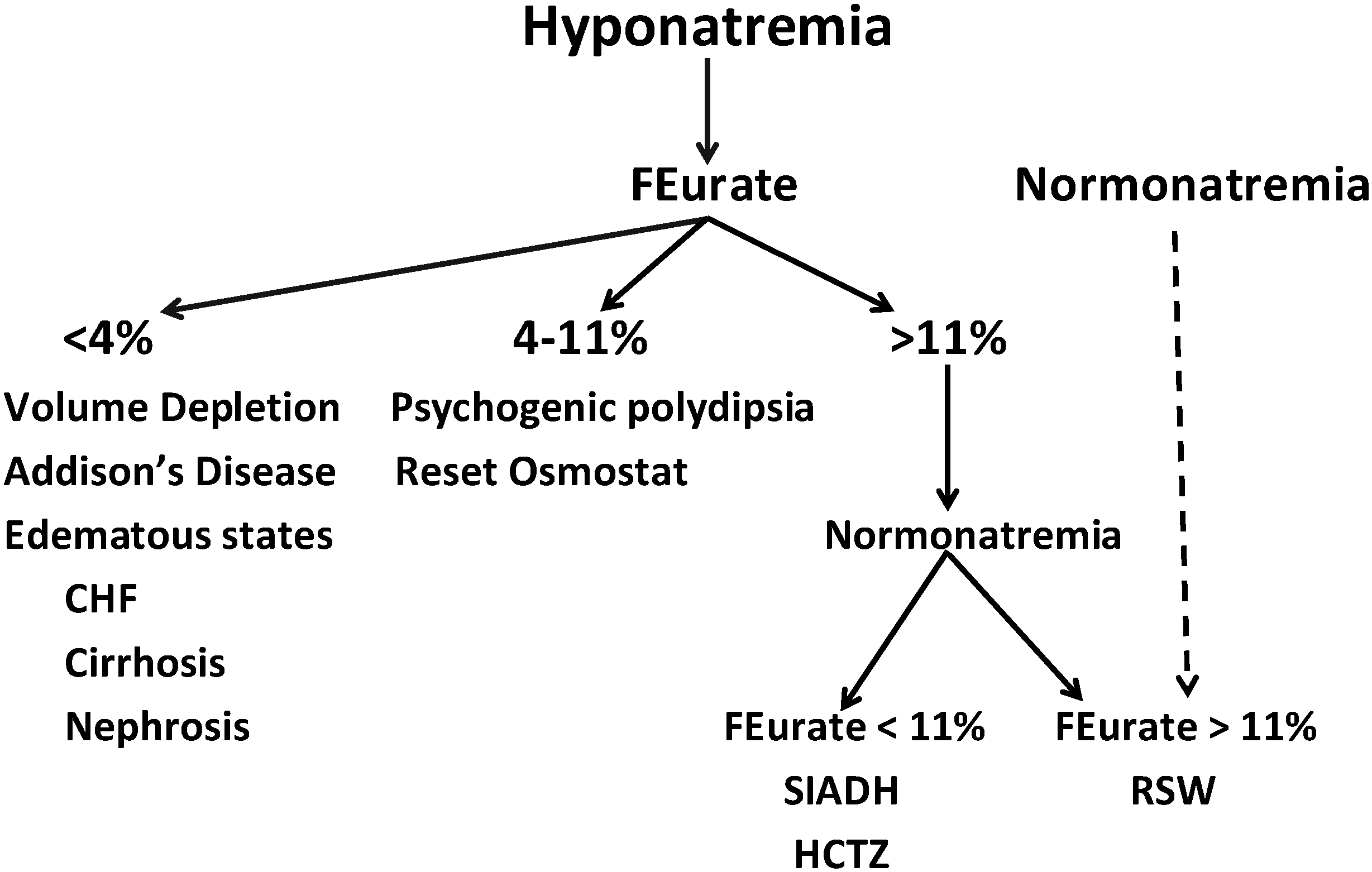
4. Value of Determining FEurate in Differentiating SIADH from RSW and Changing CSW to RSW


| FE Na (%) | FE Urate (%) | Reference | |||
|---|---|---|---|---|---|
| Control | Exp. | Control | Exp. | ||
| Isotonic | 1.04 | 4.43 | 7.98 | 9.76 | [37] |
| 1.6 | 8.2 | 5.0 | 5.8 | [36] | |
| Hypertonic | 2.9 | 18.6 | 5.4 | 12.1 | [36] |
| 1.4 | 14.5 | 12.5 | 18.7 | [35] | |
| Hypotonic | 1.1 | 6.1 | 4.0 | 7.3 | [36] |
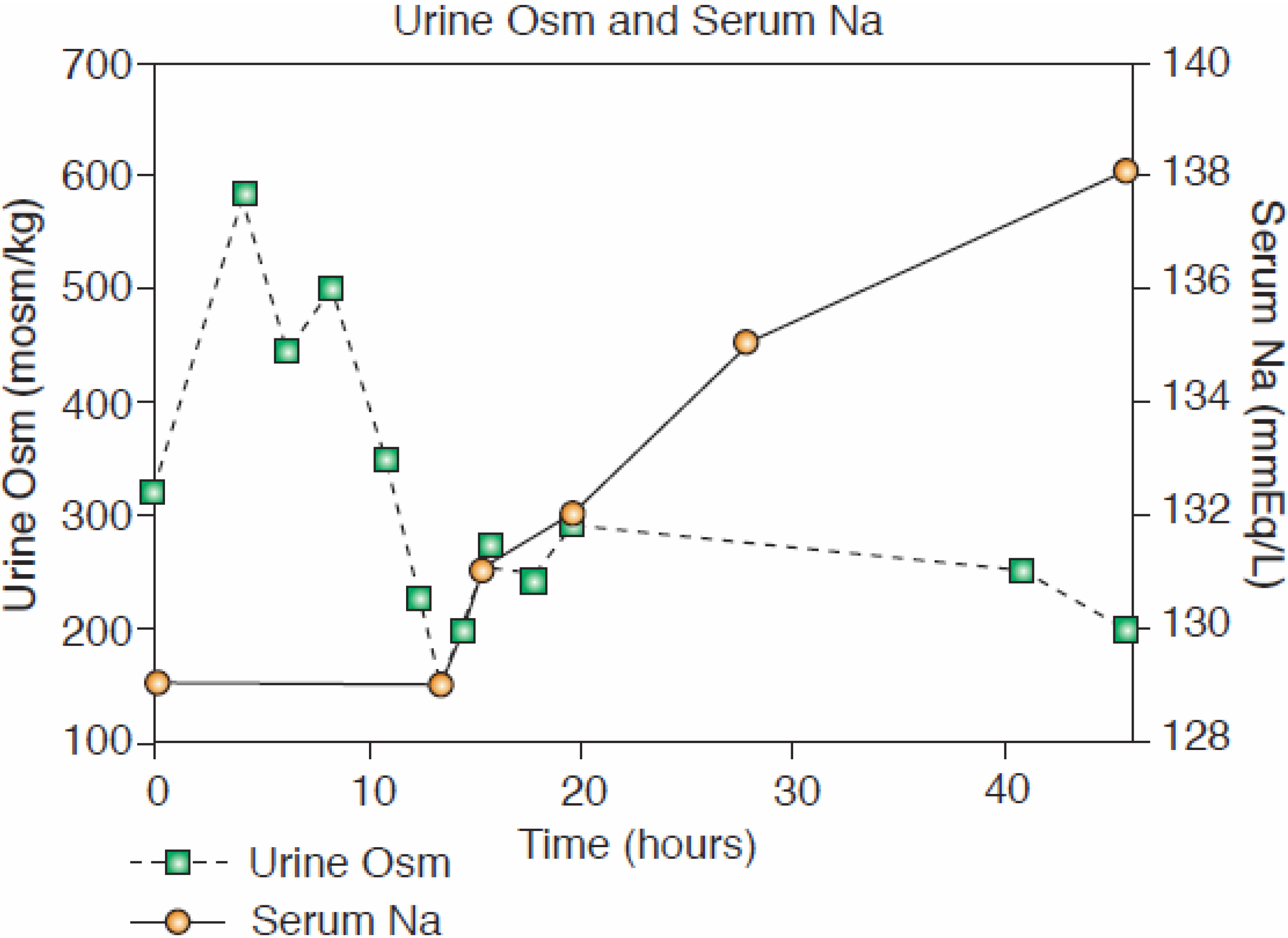
5. Normal FEurate Identifies Patients with Reset Osmostat
6. Proposal of New Algorithm

7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ellison, D.H.; Berl, T. The syndrome of inappropriate antidiuresis. N. Engl. J. Med. 2007, 356, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Giuliani, C.; Parenti, G.; Norello, D.; Verbalis, J.G.; Forti, G.; Maggi, M.; Peri, A. Moderate hyponatremia is associated with increased risk of mortality: Evidence from a meta-analysis. PLoS One 2013, 8, e80451. [Google Scholar] [CrossRef] [PubMed]
- Berl, T.; Quittnat-Pelletier, F.; Verbalis, J.G.; Schrier, R.W.; Bichet, D.G.; Ouyang, J.; Czerwiec, F.S.; S ALTWATER Investigators. Oral tolvaptan is safe and effective in chronic hyponatremia. J. Am. Soc. Nephrol. 2010, 21, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Decaux, G. Is asymptomatic hyponatremia really asymptomatic? Am. J. Med. 2006, 119 (Suppl. 1), S79–S82. [Google Scholar] [CrossRef]
- Gankam Kengne, F.; Andres, C.; Sattar, L.; Melot, C.; Decaux, G. Mild hyponatremia and risk of fracture in the ambulatory elderly. QJM 2008, 101, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Hoorn, E.J.; van der Lubbe, N.; Zietse, R. SIADH and hyponatremia: Why does it matter? NDT Plus 2009, 2 (Suppl. 3), 5–11. [Google Scholar]
- Renneboog, B.; Musch, W.; Vandemergel, X.; Mantu, M.U.; Cedaux, G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am. J. Med. 2006, 119, 711–718. [Google Scholar] [CrossRef]
- Schrier, R. Does “asymptomatic hyponatremia” exist? Nat. Rev. Nephrol. 2010, 6. [Google Scholar] [CrossRef]
- Arieff, A.I.; Llach, F.; Massry, S.G. Neurological manifestations and morbidity of hyponatremia: Correlation with brain water and electrolytes. Medicine (Baltimore) 1976, 55, 121–129. [Google Scholar] [CrossRef]
- Robertson, G.L.; Ganguly, A. Osmo-regulation and baro-regulation of plasma vasopressin in essential hypertension. Cardiovasc. Pharmacol. 1986, 8 (Suppl. 7), S87–S91. [Google Scholar]
- Bitew, S.; Imbriano, L.; Miyawaki, N.; Fishbane, S.; Maesaka, J.K. More on renal salt wasting without cerebral disease, response to saline infusion. Clin. J. Am. Soc. Nephol. 2009, 4, 309–315. [Google Scholar] [CrossRef]
- Maesaka, J.K.; Miyawaki, N.; Palaia, T.; Fishbane, S.; Durham, J. Renal salt wasting without cerebral disease: Value of determining urate in hyponatremia. Kidney Int. 2007, 71, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.P.; Welt, L.G.; Sims, E.A.H.; Orloff, J.; Needham, J. A salt-wasting syndrome associated with cerebral disease. Trans. Assoc. Am. Physicians 1950, 63, 57–64. [Google Scholar] [PubMed]
- Maesaka, J.K.; Imbriano, L.; Shirazian, S.; Miyawaki, N. Complexity of differentiating cerebral-renal salt wasting from SIADH, emerging importance of determining fractional urate excretion. In Novel Insights on Chronic Kidney Disease, Acute Kidney Injury and Polycystic Kidney Disease; Vijayakumar, S., Ed.; InTech: Rijeka, Croatia, 2012; pp. 41–66. [Google Scholar]
- Strauss, M.B.; Lamdin, E.; Smith, P.; Bleifer, D.J. Surfeit and deficit of sodium. Arch. Int. Med. 1958, 102, 527–536. [Google Scholar] [CrossRef]
- McCance, R.A. Experimental sodium chloride deficiency in man. Proc. R. Soc. Lond. 1936, 119, 245–268. [Google Scholar] [CrossRef]
- Hollenberg, N.K. Set point for sodium homeostasis: Surfeit, deficit, and their implication. Kidney Int. 1980, 17, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Leaf, A.; Bartter, F.C.; Santos, R.F.; Wrong, O. Evidence in man that urinary electrolyte loss induced by pitressin is a function of water retention. J. Clin. Investig. 1953, 32, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, W.B.; Bennett, W.; Curelop, S. A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am. J. Med. 1957, 23, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.B.; Seif, S.M.; Maroon, J.C.; Robinson, A.G. Hyponatremia in intracranial disease: Perhaps not the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). J. Neurosurg. 1981, 55, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Vermeulen, M.; Haaf, J.A.; Hijdra, A.; Bakker, W.H.; van Gijn, J. Volume depletion and natriuresis in patients with a ruptured intracranial aneurysm. Ann. Neurol. 1985, 18, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Verbalis, J.G.; Barsony, J.; Sugimura, Y.; Tian, Y.; Adams, D.J.; Carter, E.A.; Resnick, H.E. Hyponatremia-induced osteoporosis. J. Bone Miner. Metab. 2010, 25, 554–563. [Google Scholar] [CrossRef]
- Sivakumar, V.; Rajshekhar, V.; Chandy, M.J. Management of neurosurgical patient with hyponatremia and natriuresis. Neurosurgery 1994, 43, 269–274. [Google Scholar] [CrossRef]
- Gutierrez, O.M.; Lin, H.Y. Refractory hyponatremia. Kidney Int. 2007, 71, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Vermeulen, M.; Hijdra, A.; van Gijn, J. Hyponatremia and cerebral Infarction in patients with ruptured intracranial aneurysm: Is fluid restriction harmful? Ann. Neurol. 1985, 17, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Assadi, F.K.; John, E.G. Hypouricemia in neonates with syndrome of inappropriate secretion of antidiuretic hormone. Pediatr. Res. 1985, 19, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.H. Hypouricemia in the syndrome of inappropriate secretion of antidiuretic hormone. N. Engl. J. Med. 1979, 301, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Dorhout Mees, E.J.; Blom van Assendelft, P.; Nieuwenhuis, M.G. Elevation of urate clearance caused by inappropriate antidiuretic hormone secretion. Acta Med. 1971, 189, 69–72. [Google Scholar] [CrossRef]
- Sonnenblick, M.; Rosin, A. Increased uric acid clearance in the syndrome of inappropriate secretion of antidiuretic hormone. Isr. J. Med. Sci. 1988, 24, 20–23. [Google Scholar] [PubMed]
- Maesaka, J.K.; Batuman, V.; Yudd, M.; Sale, M.; Sved, A.F.; Venkatesan, J. Hyponatremia and hypouricemia: Differentiation from the syndrome of inappropriate secretion of antidiuretic hormone. Clin. Nephrol. 1990, 33, 174–178. [Google Scholar] [PubMed]
- Maesaka, J.K.; Venkatesan, J.; Piccione, J.M.; Decker, R.; Dreisbach, A.W.; Wetherington, J.D. Abnormal renal urate transport in patients with intracranial disease. Am. J. Kidney Dis. 1992, 19, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Drakakis, J.; Imbriano, L.; Miyawaki, N.; Shirazian, S.; Maesaka, J.K. Normalization of fractional excretion of urate (FEurate) after correction of hyponatremia differentiates SIADH from cerebral/renal salt wasting (RSW). In Proceedings of the Abstracts Annual Meeting American Society of Nephrology, Philadelphia, PA, USA, 8–13 November 2011.
- Maesaka, J.K.; Wolf-Klein, G.; Piccione, J.M.; Ma, C.M. Hyporuicemia, abnormal renal tubular urate transport and plasma natriuretic factor(s) in patients with Alzheimer’s disease. J. Am. Geriatr. Soc. 1993, 41, 501–506. [Google Scholar] [PubMed]
- Maesaka, J.K.; Imbriano, L.; Ali, N.; Ilamathi, E. Mini review. Is it cerebral or renal salt wasting? Kidney Int. 2009, 76, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Cannon, P.J.; Svahn, D.S.; Demartini, F.E. The influence of hypertonic saline infusions upon the fractional reabsorption of urate and other ions in normal and hypertensive man. Circulation 1970, 41, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Diamond, H.; Meisel, A. Influence of volume expansion, serum sodium, and fractional excretion of sodium on urate excretion. Pflugers. Arch. 1975, 356, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Steele, T. Evidence for altered renal urate reabsorption during changes in volume of the extracellular fluid. J. Lab. Clin. Med. 1969, 74, 288–299. [Google Scholar] [PubMed]
- Maesaka, J.K.; Fishbane, S. Regulation of renal urate excretion: A critical review. Am. J. Kidney Dis. 1998, 32, 917–933. [Google Scholar] [CrossRef] [PubMed]
- Decaux, G.; Namias, B.; Gulbis, B.; Soupart, A. Evidence in hyponatremia related to inappropriate secretion of ADH that V1 receptor stimulation contributes to the increase in renal uric acid clearance. J. Am. Soc. Nephrol. 1996, 7, 805–810. [Google Scholar] [PubMed]
- Decaux, G.; Prospert, F.; Soupart, A.; Musch, W. Evidence that chronicity of hyponatremia contributes to the high urate clearance observed in the syndrome of inappropriate secretion of antidiuretic hormone. Am. J. Kidney Dis. 2000, 36, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Maesaka, J.K.; Venkatesan, J.; Piccione, J.M.; Decker, R.; Dreisbach, A.W.; Wetherington, J. Plasma natriuretic factor(s) in patients with intracranial disease, renal salt wasting and hyperuricosuria. Life Sci. 1993, 52, 1875–1882. [Google Scholar] [CrossRef] [PubMed]
- Imbriano, L.J.; Ilamathi, E.; Ali, N.M.; Miyawaki, N.; Maesaka, J.K. Normal fractional urate excretion identifies hyponatremic patients with reset osmostat. J. Nephrol. 2012, 5, 833–838. [Google Scholar] [CrossRef]
- Zerbe, R.; Stropes, L.; Robertson, G. Vasopressin function in the syndrome of inappropriate antidiuresis. Annu. Rev. Med. 1980, 31, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Milionis, H.J.; Kakafika, A.L.; Tsouli, S.G.; Athyros, V.G.; Bairaktari, E.T.; Seferiadis, K.I.; Elisaf, M.S. Effects of statin treatment on uric acid homeostasis in patient with primary hyperlipidemia. Am. Heart J. 2004, 148, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Moriwaki, Y.; Takahashi, S.; Tsutsumi, Z.; Hada, T. Effect of losartan potassium, an angiotensin II receptor antagonist, on renal excretion of oxypurinol and purine bases. J. Rheumatol. 2000, 27, 2232–2236. [Google Scholar] [PubMed]
- Ali, N.; Imbriano, L.; Miyawaki, N.; Maesaka, J.K. 66-Year-old male with Hyponatremia. Kidney Int. 2009, 76, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Berl, T. Impact of solute intake on urine flow and water excretion. J. Am. Soc. Nephrol. 2008, 19, 1076–1078. [Google Scholar] [CrossRef] [PubMed]
- Abuelo, J.G. Normotensive ischemic acute renal failure. N. Eng. J. Med. 2007, 357, 797–798. [Google Scholar] [CrossRef]
- Maesaka, J.; Gallagher, D.; Mattana, J.; Imbriano, L. Unexpectedly high Frequency of reset osmostat and cerebral-renal salt wasting in non-edematous hyponatremia: Value of determining total, extracellular and intracellular water volumes and fractional excretion of urate. In Proceedings of the Abstracts Annual Meeting American Society of Nephrology, Philadelphia, PA, USA, 9–11 September 2013.
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maesaka, J.K.; Imbriano, L.; Mattana, J.; Gallagher, D.; Bade, N.; Sharif, S. Differentiating SIADH from Cerebral/Renal Salt Wasting: Failure of the Volume Approach and Need for a New Approach to Hyponatremia. J. Clin. Med. 2014, 3, 1373-1385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm3041373
Maesaka JK, Imbriano L, Mattana J, Gallagher D, Bade N, Sharif S. Differentiating SIADH from Cerebral/Renal Salt Wasting: Failure of the Volume Approach and Need for a New Approach to Hyponatremia. Journal of Clinical Medicine. 2014; 3(4):1373-1385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm3041373
Chicago/Turabian StyleMaesaka, John K., Louis Imbriano, Joseph Mattana, Dympna Gallagher, Naveen Bade, and Sairah Sharif. 2014. "Differentiating SIADH from Cerebral/Renal Salt Wasting: Failure of the Volume Approach and Need for a New Approach to Hyponatremia" Journal of Clinical Medicine 3, no. 4: 1373-1385. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm3041373