Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention


Abstract
:1. Introduction
2. Materials and Methods
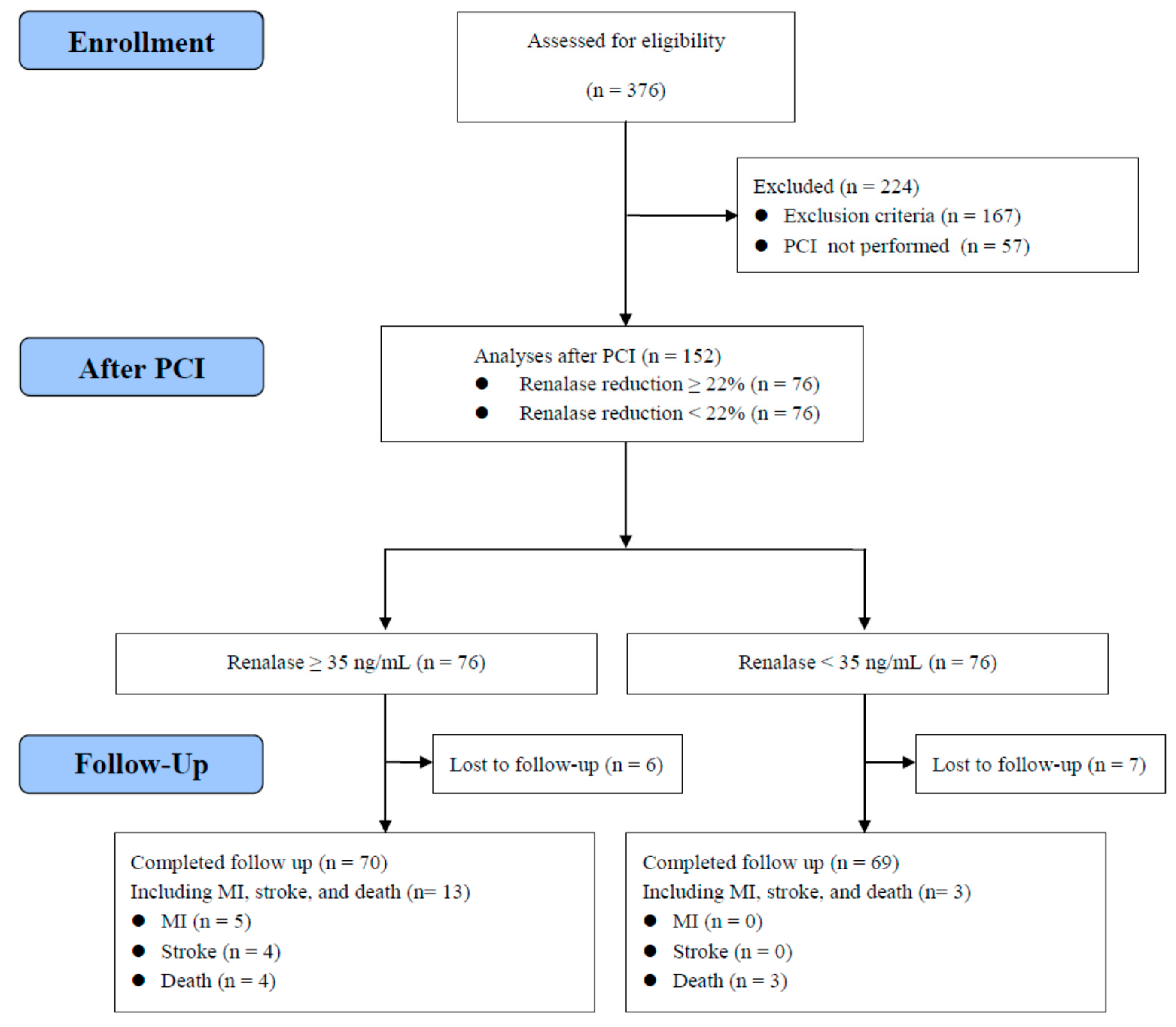
2.1. Subjects
2.2. Methods
2.3. Statistical Analysis
3. Results
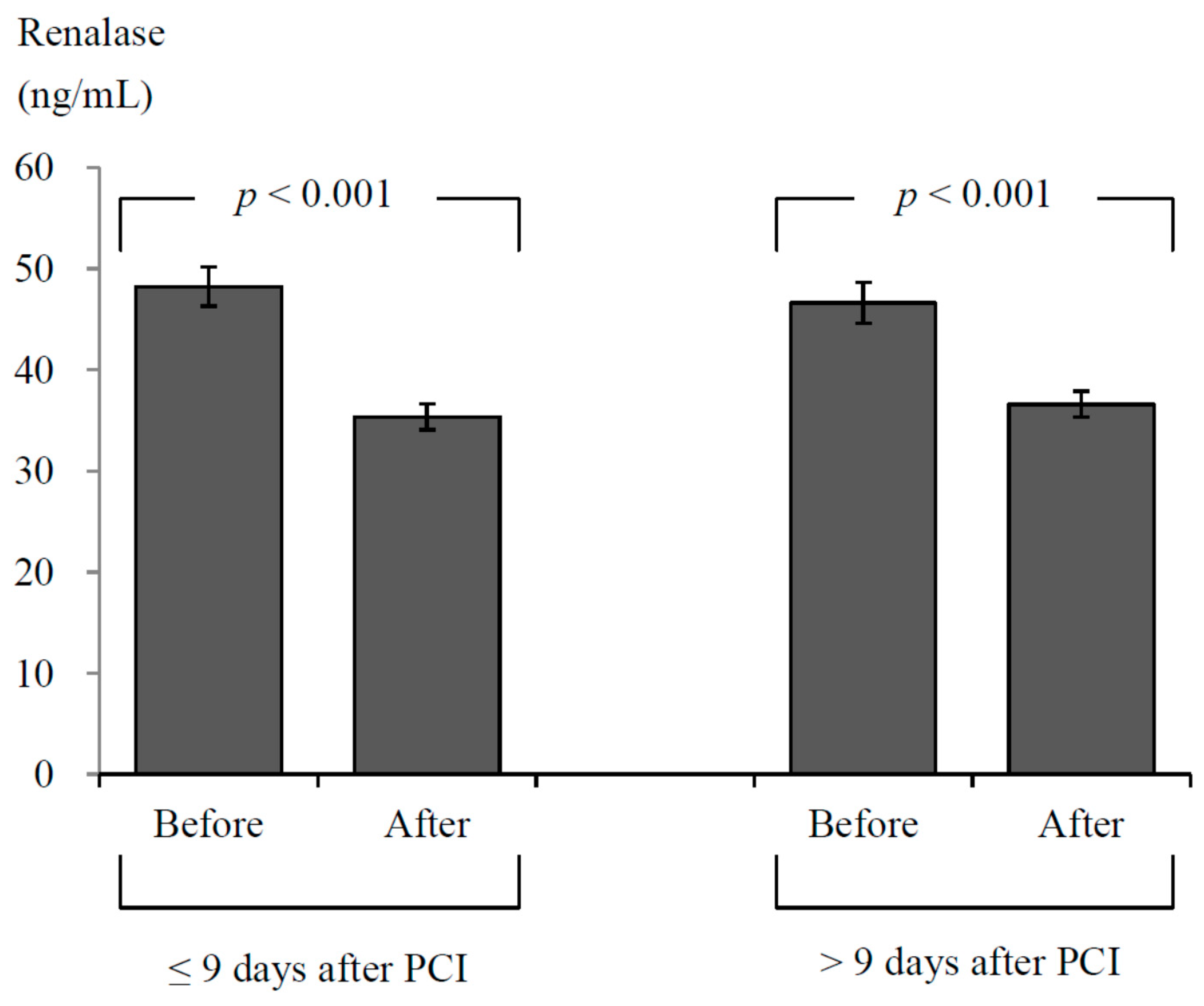
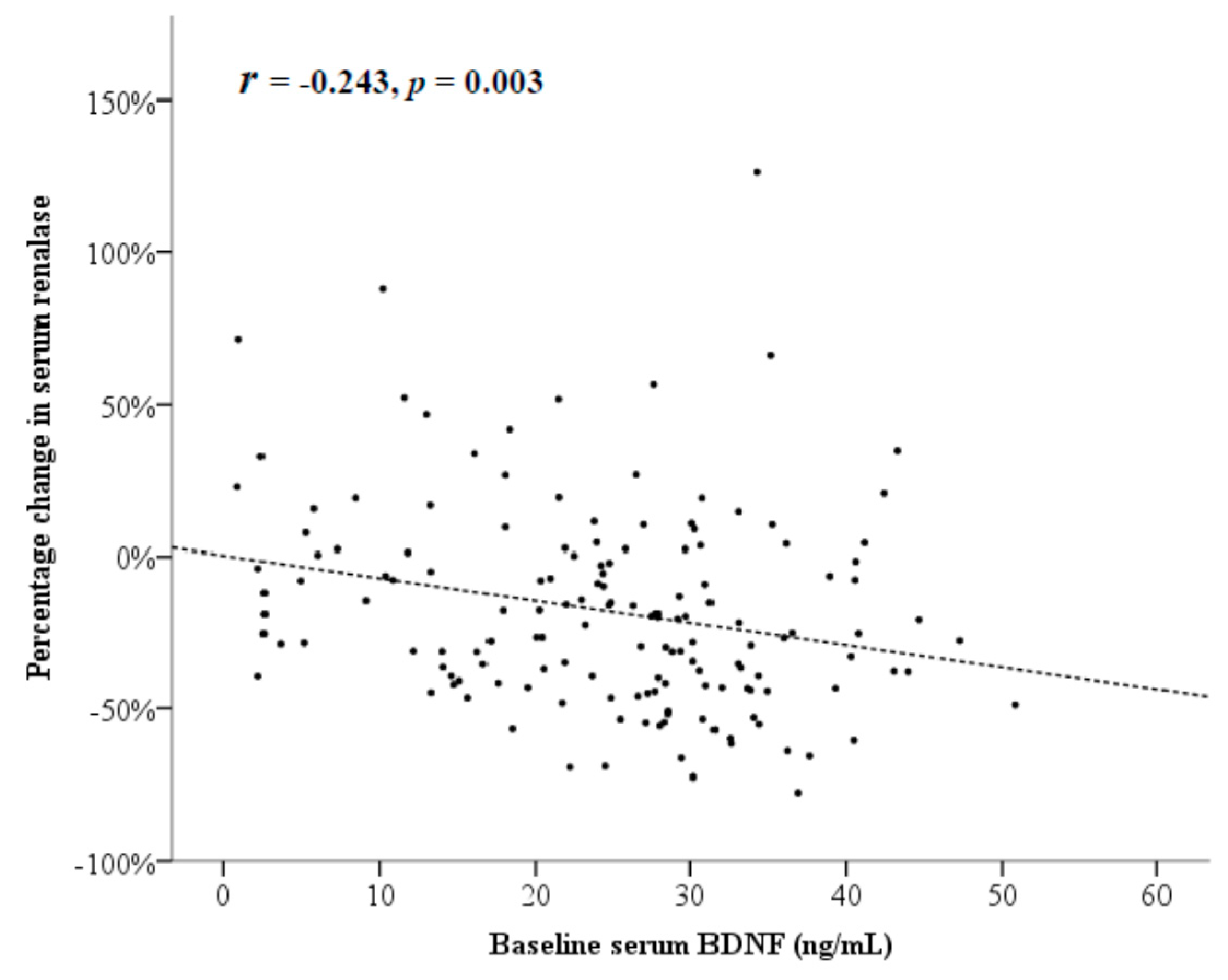
3.1. Assessments before and after PCI
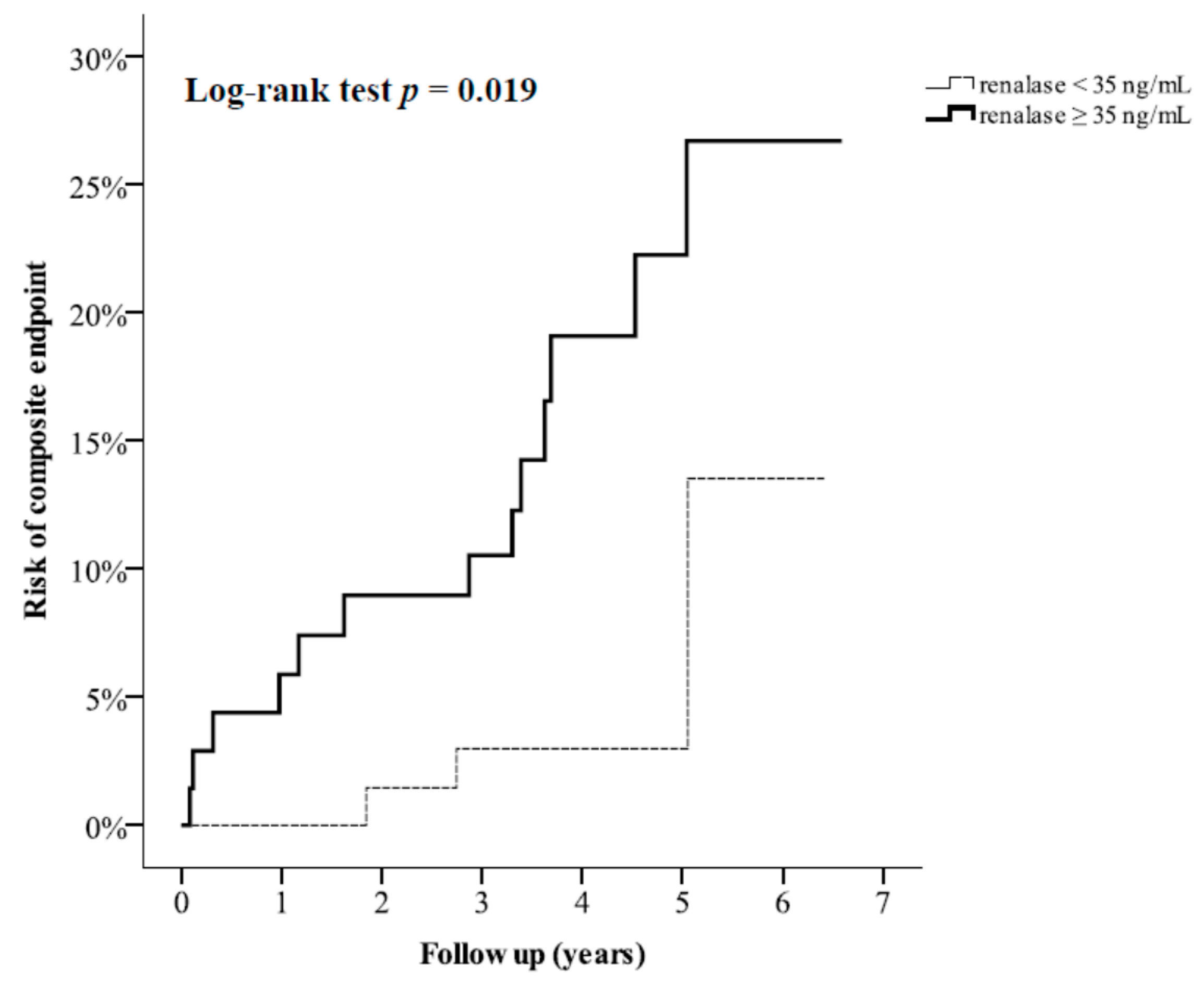
3.2. Assessments for Longitudicnal Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Rosengart, T.K.; Sweet, J.; Finnin, E.B.; Wolfe, P.; Cashy, J.; Hahn, E.; Marymont, J.; Sanborn, T. Neurocognitive functioning in patients undergoing coronary artery bypass graft surgery or percutaneous coronary intervention: Evidence of impairment before intervention compared with normal controls. Ann. Thorac. Surg. 2005, 80, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Duan, Z.; Zhang, Y.; Zeng, Z.; Pan, F. Comment on “Inflammasome activation of IL-18 results in endothelial progenitor cell dysfunction in systemic lupus erythematosus”. J. Immunol. 2012, 189, 499. [Google Scholar] [CrossRef] [PubMed]
- So, E.S. Cardiovascular disease risk factors associated with depression among Korean adults with coronary artery disease and cerebrovascular disease. Asia Pac. Psychiatry 2015, 7, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Zellweger, M.J.; Osterwalder, R.H.; Langewitz, W.; Pfisterer, M.E. Coronary artery disease and depression. Eur. Heart J. 2004, 25, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Kronmal, R.A.; Newman, A.B.; Bild, D.E.; Mittelmark, M.B.; Polak, J.F.; Robbins, J.A.; Gardin, J.M. Risk factors for 5-year mortality in older adults: The Cardiovascular Health Study. JAMA 1998, 279, 585–592. [Google Scholar] [CrossRef] [PubMed]
- May, H.T.; Horne, B.D.; Knight, S.; Knowlton, K.U.; Bair, T.L.; Lappe, D.L.; Le, V.T.; Muhlestein, J.B. The association of depression at any time to the risk of death following coronary artery disease diagnosis. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, L.; Mack, W.J.; Chui, H.C.; Heflin, L.; Mungas, D.; Reed, B.; DeCarli, C.; Weiner, M.W.; Kramer, J.H. Coronary artery disease is associated with cognitive decline independent of changes on magnetic resonance imaging in cognitively normal elderly adults. J. Am. Geriatr. Soc. 2012, 60, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Leibrock, J.; Lottspeich, F.; Hohn, A.; Hofer, M.; Hengerer, B.; Masiakowski, P.; Thoenen, H.; Barde, Y.A. Molecular cloning and expression of brain-derived neurotrophic factor. Nature 1989, 341, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Alam, A.; San, C.Y.; Eguchi, S.; Chen, Q.; Lian, Q.; Ma, D. Molecular mechanisms of brain-derived neurotrophic factor in neuro-protection: Recent developments. Brain Res. 2017, 1665, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Lee, W.J.; Tsai, I.C.; Liang, K.W.; Lin, S.Y.; Wan, C.J.; Fu, C.P.; Sheu, W.H. Brain-derived neurotrophic factor not associated with metabolic syndrome but inversely correlated with vascular cell adhesion molecule-1 in men without diabetes. Clin. Chim. Acta 2012, 413, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.T.; Wang, J.S.; Lee, W.J.; Lin, S.Y.; Fu, C.P.; Liang, K.W.; Hsu, C.Y.; Sheu, W.H. The synergistic effect of vascular cell adhesion molecule-1 and coronary artery disease on brain-derived neurotrophic factor. Clin. Chim. Acta 2017, 466, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Swardfager, W.; Herrmann, N.; Marzolini, S.; Saleem, M.; Shammi, P.; Oh, P.I.; Albert, P.R.; Daigle, M.; Kiss, A.; Lanctot, K.L. Brain derived neurotrophic factor, cardiopulmonary fitness and cognition in patients with coronary artery disease. Brain Behav. Immun. 2011, 25, 1264–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlmann, S.L.; Tschorn, M.; Arolt, V.; Beer, K.; Brandt, J.; Grosse, L.; Haverkamp, W.; Muller-Nordhorn, J.; Rieckmann, N.; Waltenberger, J.; et al. Serum brain-derived neurotrophic factor and stability of depressive symptoms in coronary heart disease patients: A prospective study. Psychoneuroendocrinology 2017, 77, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Liu, Y.; Zhang, Y.; Chen, Z.Y. Association of plasma brain-derived neurotrophic factor and cardiovascular risk factors and prognosis in angina pectoris. Biochem. Biophys. Res. Commun. 2011, 415, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Pursnani, S.; Korley, F.; Gopaul, R.; Kanade, P.; Chandra, N.; Shaw, R.E.; Bangalore, S. Percutaneous coronary intervention versus optimal medical therapy in stable coronary artery disease: A systematic review and meta-analysis of randomized clinical trials. Circ. Cardiovasc. Interv. 2012, 5, 476–490. [Google Scholar] [CrossRef] [PubMed]
- Harold, J.G.; Bass, T.A.; Bashore, T.M.; Brindis, R.G.; Brush, J.E., Jr.; Burke, J.A.; Dehmer, G.J.; Deychak, Y.A.; Jneid, H.; Jollis, J.G.; et al. ACCF/AHA/SCAI 2013 update of the clinical competence statement on coronary artery interventional procedures: A report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training (Writing Committee to Revise the 2007 Clinical Competence Statement on Cardiac Interventional Procedures). J. Am. Coll. Cardiol. 2013, 62, 357–396. [Google Scholar] [PubMed]
- Gu, G.; Zhou, Y.; Zhang, Y.; Cui, W. Increased prevalence of anxiety and depression symptoms in patients with coronary artery disease before and after percutaneous coronary intervention treatment. BMC Psychiatry 2016, 16, 259. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P. Study of Anxiety/Depression in Patients with Coronary Heart Disease after Percutaneous Coronary Intervention. Cell Biochem. Biophys. 2015, 72, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Desir, G.V.; Wang, L.; Peixoto, A.J. Human renalase: A review of its biology, function, and implications for hypertension. J. Am. Soc. Hypertens. 2012, 6, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.H.; Cha, R.H.; Kang, S.W.; Park, C.W.; Cha, D.R.; Kim, S.G.; Yoon, S.A.; Kim, S.; Han, S.Y.; Park, J.H.; et al. Circulating renalase predicts all-cause mortality and renal outcomes in patients with advanced chronic kidney disease. Korean J. Intern. Med. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Dobrzycki, S. Renalase, kidney and cardiovascular disease: Are they related or just coincidentally associated? Adv. Med. Sci. 2015, 60, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Musialowska, D.; Malyszko, J. Renalase—A new marker or just a bystander in cardiovascular disease: Clinical and experimental data. Kardiol. Pol. 2016, 74, 937–942. [Google Scholar] [PubMed]
- Ronco, C.; Haapio, M.; House, A.A.; Anavekar, N.; Bellomo, R. Cardiorenal syndrome. J. Am. Coll. Cardiol. 2008, 52, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Wybraniec, M.T.; Bozentowicz-Wikarek, M.; Chudek, J.; Mizia-Stec, K. Urinary renalase concentration in patients with preserved kidney function undergoing coronary angiography. Nephrology 2018, 23, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.J.; Jiang, X.; Zhou, W.; Wang, Y.; Gao, L.; Wang, Y.; Li, G.T.; Hong, T.; Huo, Y.; Jing, Z.C.; et al. Connective tissue disease-associated pulmonary arterial hypertension in Chinese patients. Eur. Respir. J. 2014, 44, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Wang, L.; Deng, D.; Zhang, Q.; Liu, W. Renalase Protects against Renal Fibrosis by Inhibiting the Activation of the ERK Signaling Pathways. Int. J. Mol. Sci. 2017, 18, 855. [Google Scholar] [Green Version]
- Lee, H.T.; Kim, J.Y.; Kim, M.; Wang, P.; Tang, L.; Baroni, S.; D’Agati, V.D.; Desir, G.V. Renalase protects against ischemic AKI. J. Am. Soc. Nephrol. 2013, 24, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Zhao, Q.; Li, J.; Xing, T.; Wang, F.; Wang, N. Renalase protects against contrast-induced nephropathy in Sprague-Dawley rats. PLoS ONE 2015, 10, e0116583. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, D.; Cvetkovic, T.; Stojanovic, M.; Bojanic, V.; Stefanovic, N.; Stojanovic, I. The assessment of renalase: Searching for the best predictor of early renal dysfunction by multivariate modeling in stable renal transplant recipients. Ann. Transplant. 2015, 20, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Hennebry, S.C.; Eikelis, N.; Socratous, F.; Desir, G.; Lambert, G.; Schlaich, M. Renalase, a novel soluble FAD-dependent protein, is synthesized in the brain and peripheral nerves. Mol. Psychiatry 2010, 15, 234–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paredes, D.; Granholm, A.C.; Bickford, P.C. Effects of NGF and BDNF on baseline glutamate and dopamine release in the hippocampal formation of the adult rat. Brain Res. 2007, 1141, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quelhas-Santos, J.; Serrao, M.P.; Soares-Silva, I.; Fernandes-Cerqueira, C.; Simoes-Silva, L.; Pinho, M.J.; Remiao, F.; Sampaio-Maia, B.; Desir, G.V.; Pestana, M. Renalase regulates peripheral and central dopaminergic activities. Am. J. Physiol. Renal. Physiol. 2015, 308, F84–F91. [Google Scholar] [CrossRef] [PubMed]
- Kaess, B.M.; Preis, S.R.; Lieb, W.; Beiser, A.S.; Yang, Q.; Chen, T.C.; Hengstenberg, C.; Erdmann, J.; Schunkert, H.; Seshadri, S.; et al. Circulating brain-derived neurotrophic factor concentrations and the risk of cardiovascular disease in the community. J. Am. Heart Assoc. 2015, 4, e001544. [Google Scholar] [CrossRef] [PubMed]
- Devapalasundarum, A.N.; Silbert, B.S.; Evered, L.A.; Scott, D.A.; MacIsaac, A.I.; Maruff, P.T. Cognitive function in patients undergoing coronary angiography. Heart Asia 2010, 2, 75–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejiri, J.; Inoue, N.; Kobayashi, S.; Shiraki, R.; Otsui, K.; Honjo, T.; Takahashi, M.; Ohashi, Y.; Ichikawa, S.; Terashima, M.; et al. Possible role of brain-derived neurotrophic factor in the pathogenesis of coronary artery disease. Circulation 2005, 112, 2114–2120. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before * | After * | Change # | p† | ||
|---|---|---|---|---|---|
| Age (years) | 60 ± 12 | ||||
| Male, n (%) | 136 (89.5%) | ||||
| Current smoker, n (%) | 47 (30.9%) | ||||
| BMI (kg/m2) | 26.8 ± 4.0 | 26.5 ± 3.9 | −0.3 | (−0.5, −0.1) | <0.001 |
| Systolic BP (mmHg) | 128 ± 19 | 129 ± 18 | 0.2 | (−2.9, 3.4) | 0.877 |
| Diastolic BP (mmHg) | 78 ± 14 | 75 ± 10 | −3.2 | (−5.4, −1.0) | 0.005 |
| Fasting glucose (mmol/L) | 5.6 ± 1.1 | 5.4 ± 0.9 | −0.2 | (−0.3, 0.0) | 0.108 |
| Total cholesterol (mmol/L) | 4.1 ± 1.1 | 4.1 ± 0.9 | −0.1 | (−8.7, 4.3) | 0.506 |
| HDL cholesterol (mmol/L) | 1.0 ± 0.3 | 1.2 ± 0.2 | 0.2 | (5.0, 7.5) | <0.001 |
| Triglyceride (mmol/L) | 1.4 ± 0.9 | 1.5 ± 0.8 | 0.04 | (−6.5, 13.3) | 0.498 |
| eGFR (mL/min/1.73 m2) | 84.3 ± 22.5 | 77.0 ± 20.4 | −7.3 | (−9.7, −4.9) | <0.001 |
| BDNF (ng/mL) | 24.7 ± 11.0 | 23.5 ± 8.3 | −1.1 | (−2.8, 0.5) | 0.175 |
| Renalase (ng/mL) | 47.5 ± 17.3 | 35.9 ± 11.3 | −11.7 | (−14.3, −9.0) | <0.001 |
| Antihypertensive agent use | |||||
| ACE inhibitor or ARB, n (%) | 74 (48.7%) | 108 (71.1%) | 34.0 | (45.9%) | <0.001 |
| α-blocker, n (%) | 12 (7.9%) | 6 (3.9%) | −6.0 | (−50.0%) | 0.070 |
| β-blocker, n (%) | 31 (20.4%) | 46 (30.3%) | 15.0 | (48.4%) | 0.009 |
| Calcium channel blocker, n (%) | 73 (48.0%) | 73 (48.0%) | 0.0 | (0.0%) | 0.999 |
| Diuretics, n (%) | 23 (15.1%) | 25 (16.4%) | 2.0 | (8.7%) | 0.754 |
| Antiplatelet agent, n (%) | 125 (82.2%) | 148 (97.4%) | 23.0 | (18.4%) | <0.001 |
| Statins, n (%) | 79 (52.0%) | 115 (75.7%) | 36.0 | (45.6%) | <0.001 |
| r | p | |
|---|---|---|
| ΔBMI (kg/m2) | −0.103 | 0.209 |
| ΔDiastolic BP (mmHg) | 0.099 | 0.225 |
| ΔHDL cholesterol (mmol/L) | 0.110 | 0.176 |
| ΔGFR (mL/min/1.73 m2) | −0.011 | 0.896 |
| Renalase Reduction (n = 76) | Reference (n = 76) | p * | p# | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years) | 60 ± 11 | 60 ± 12 | 0.812 | |
| Male, n (%) | 68 (89.5%) | 68 (89.5%) | 1.000 | |
| Current smoker, n (%) | 20 (26.3%) | 27 (35.5%) | 0.292 | |
| Anthropometric data | ||||
| BMI (kg/m2) | ||||
| Before (mean ± SD) | 27.1 ± 3.8 | 26.6 ± 4.2 | 0.530 | |
| After (mean ± SD) | 26.8 ± 3.6 | 26.2 ± 4.1 | ||
| Change (mean (95% CI)) | −0.2 (−0.5, 0.1) | −0.4 (−0.6, 0.2) | 0.353 | |
| Systolic BP (mmHg) | ||||
| Before (mean ± SD) | 128 ± 16 | 129 ± 21 | 0.745 | |
| After (mean ± SD) | 128 ± 17 | 129 ± 19 | ||
| Change (mean (95% CI)) | 1 (−3, 5) | 0 (−5, 5) | 0.774 | |
| Diastolic BP (mmHg) | ||||
| Before (mean ± SD) | 79 ± 13 | 76 ± 15 | 0.138 | |
| After (mean ± SD) | 75 ± 10 | 74 ± 10 | ||
| Change (mean (95% CI)) | −4 (−7, −1) | −2 (−5, 1) | 0.286 | |
| Biochemistry data | ||||
| Fasting glucose (mmol/L) | ||||
| Before (mean ± SD) | 5.6 ± 1.3 | 5.6 ± 1.0 | 0.969 | |
| After (mean ± SD) | 5.4 ± 0.8 | 5.4 ± 1.0 | ||
| Change (mean (95% CI)) | −0.1 (−0.4, 0.1) | −0.2 (−0.5, 0.1) | 0.787 | |
| Total cholesterol (mmol/L) | ||||
| Before (mean ± SD) | 4.1 ± 1.1 | 4.1 ± 1.1 | 0.789 | |
| After (mean ± SD) | 4.0 ± 0.9 | 4.1 ± 0.9 | ||
| Change (mean (95% CI)) | −0.1 (−0.4, 0.1) | 0.0 (−0.2, 0.3) | 0.283 | |
| HDL cholesterol (mmol/L) | ||||
| Before (mean ± SD) | 1.0 ± 0.3 | 1.0 ± 0.3 | 0.789 | |
| After (mean ± SD) | 1.1 ± 0.2 | 1.2 ± 0.2 | ||
| Change (mean (95% CI)) | 0.2 (0.1, 0.2) | 0.2 (0.1, 0.2) | 0.573 | |
| Triglyceride (mmol/L) | ||||
| Before (mean ± SD) | 1.5 ± 1.1 | 1.3 ± 0.8 | 0.157 | |
| After (mean ± SD) | 1.5 ± 0.9 | 1.4 ± 0.8 | ||
| Change (mean (95% CI)) | 0.0 (−0.2, 0.2) | 0.1 (0.0, 0.2) | 0.305 | |
| eGFR (mL/min/1.73m2) | ||||
| Before (mean ± SD) | 87.0 ± 20.3 | 81.6 ± 24.3 | 0.140 | |
| After (mean ± SD) | 78.8 ± 17.0 | 75.2 ± 23.4 | ||
| Change (mean (95% CI)) | −8.2 (−11.8, −4.5) | −6.4 (−9.5, 3.4) | 0.467 | |
| BDNF (ng/mL) | ||||
| Before (mean ± SD) | 27.0 ± 10.1 | 22.4 ± 11.3 | 0.009 | |
| After (mean ± SD) | 22.7 ± 8.1 | 24.3 ± 8.5 | ||
| Change (mean (95% CI)) | −4.2 (−6.3, −2.2) | 2.0 (−0.5, 4.5) | <0.001 |
| Univariate Linear Regression Analysis | Multivariate Linear Regression Analyses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| B # | 95% CI | p | B # | 95% CI | p | B # | 95% CI | p | |
| Age (every 10 years) | 0.511 | (−4.093, 5.115) | 0.827 | −0.356 | (−5.106, 4.395) | 0.883 | −0.323 | (−5.756, 5.110) | 0.907 |
| Male (yes/no) | −5.977 | (−23.303, 11.350) | 0.497 | −11.310 | (−28.982, 6.363) | 0.208 | −11.842 | (−30.897, 7.212) | 0.221 |
| Current smoker (yes/no) | 2.284 | (−9.233, 13.801) | 0.696 | 8.144 | (−3.881, 20.168) | 0.183 | 8.868 | (−3.757, 21.494) | 0.167 |
| BMI (kg/m2) | −0.259 | (−1.596, 1.079) | 0.703 | −0.059 | (−1.631, 1.514) | 0.941 | |||
| Systolic BP (mmHg) | 0.121 | (−0.165, 0.407) | 0.404 | 0.117 | (−0.185, 0.418) | 0.446 | |||
| Diastolic BP (mmHg) | −0.210 | (−0.598, 0.178) | 0.287 | ||||||
| eGFR (mL/min/1.73m2) | −0.068 | (−0.305, 0.170) | 0.574 | 0.041 | (−0.220, 0.302) | 0.758 | |||
| Fasting glucose (mmol/L) | 2.025 | (−2.627, 6.678) | 0.391 | 2.128 | (−2.701, 6.957) | 0.385 | |||
| Total cholesterol (mmol/L) | −0.087 | (−5.117, 4.943) | 0.973 | 0.430 | (−5.683, 6.543) | 0.890 | |||
| Triglyceride (mmol/L) | −2.091 | (−7.777, 3.595) | 0.469 | 2.375 | (−23.369, 28.119) | 0.856 | |||
| HDL cholesterol (mmol/L) | 1.600 | (−19.207, 22.406) | 0.879 | −2.728 | (−9.590, 4.134) | 0.433 | |||
| BDNF (ng/mL) | −0.736 | (−1.209, −0.263) | 0.003 | −0.851 | (−1.345, −0.357) | 0.001 | −0.845 | (−1.371, −0.319) | 0.002 |
| ACE inhibitor or ARB used | 3.040 | (−7.604, 13.683) | 0.573 | ||||||
| α-blocker used | −5.087 | (−24.819, 14.645) | 0.611 | ||||||
| β-blocker used | 3.429 | (−9.776, 16.635) | 0.609 | ||||||
| Calcium channel blocker used | −2.190 | (−12.843, 8.464) | 0.685 | ||||||
| Diuretics used | 2.626 | (−12.229, 17.481) | 0.727 | ||||||
| Antiplatelet agent used | −6.749 | (−20.875, 7.377) | 0.347 | ||||||
| Statins used | 1.927 | (−8.728, 12.582) | 0.721 | ||||||
| Univariate Model | Multivariate Model | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Crude | Model 1 | Model 2 | |||||||
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Serum renalase ≥ 35 ng/mL (yes/no) | 4.031 | (1.141, 14.236) | 0.030 | 3.674 | (1.041, 12.972) | 0.043 | 5.636 | (1.444, 21.998) | 0.013 |
| Age ≥ 60 years (yes/no) | 3.927 | (1.262, 12.218) | 0.018 | 3.720 | (1.168, 11.851) | 0.026 | 5.284 | (1.556, 17.946) | 0.008 |
| Gender (male/female) | 0.755 | (0.171, 3.331) | 0.711 | 1.163 | (0.258, 5.253) | 0.844 | 1.112 | (0.200, 6.192) | 0.903 |
| Using statins after PCI (yes/no) | 0.910 | (0.290, 2.856) | 0.872 | 1.223 | (0.334, 4.486) | 0.761 | |||
| Multiple coronary artery disease (yes/no) | 1.263 | (0.457, 3.493) | 0.653 | 1.406 | (0.490, 4.034) | 0.526 | |||
| Total cholesterol (increase in every 1 mmol/L) | 1.048 | (0.626, 1.754) | 0.860 | 1.157 | (0.627, 2.135) | 0.641 | |||
| eGFR (increase in every 15 mL/min/1.73m2) | 0.982 | (0.669, 1.442) | 0.928 | 1.470 | (0.967, 2.234) | 0.071 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.-T.; Sheu, W.H.-H. Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention. J. Clin. Med. 2018, 7, 437. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110437
Lee I-T, Sheu WH-H. Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention. Journal of Clinical Medicine. 2018; 7(11):437. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110437
Chicago/Turabian StyleLee, I-Te, and Wayne Huey-Herng Sheu. 2018. "Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention" Journal of Clinical Medicine 7, no. 11: 437. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110437